
Microbiota Ecosystem in Recurrent Cystitis and the Immunological Microenvironment of Urothelium
 , ,
, ,
Abstract
1. Introduction
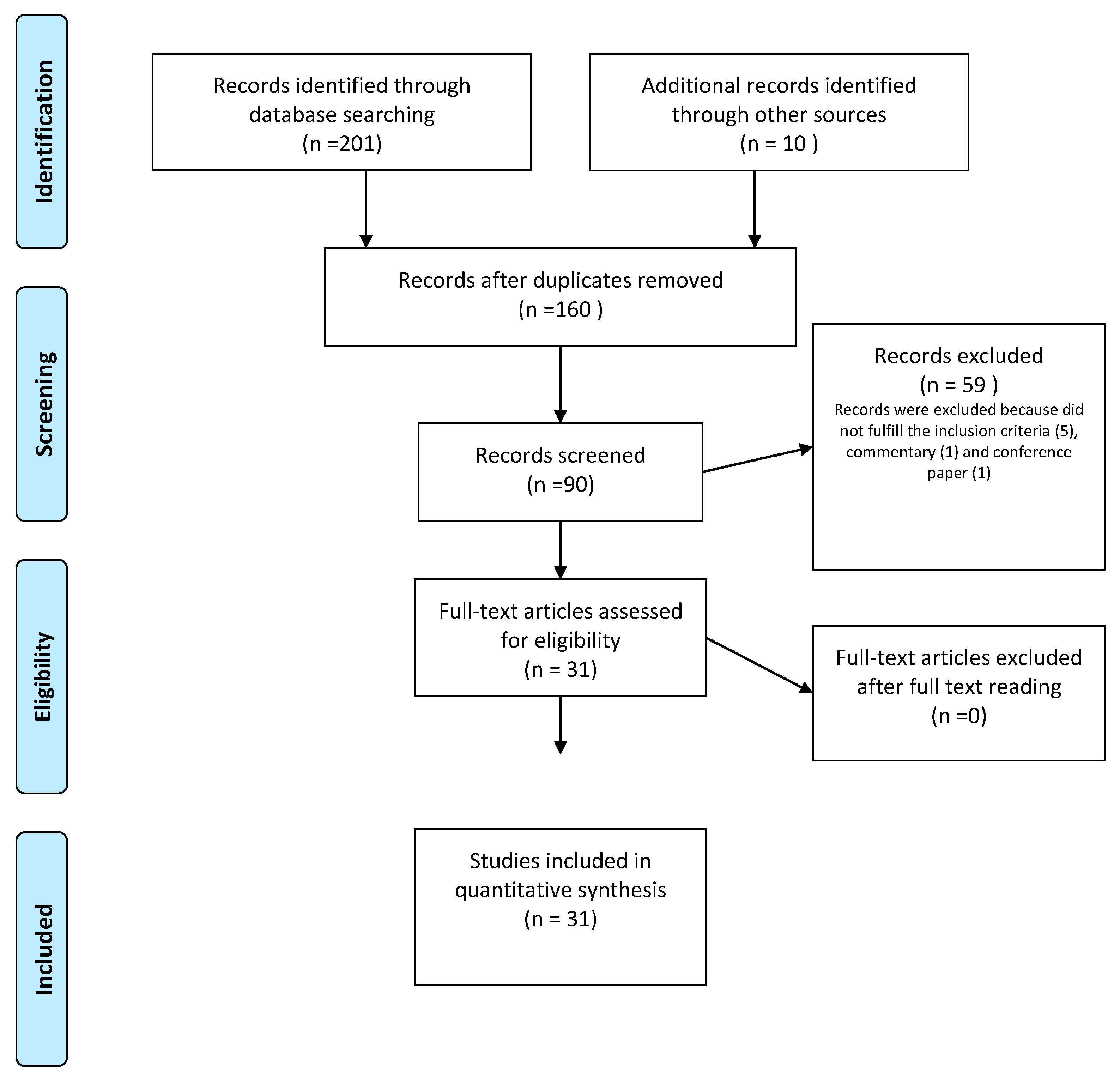
2. Materials and Methods
3. Results
3.1. Vaginal Microbiome and rUTIs
3.2. Urinary Microbiome and rUTIs
4. Discussion and Conclusions
4.1. Risk Factors for rUTIs in Women
4.2. NGS as a Better Diagnostic Tool
4.3. Pathophysiology and Immunology in rUTIs
4.4. New Perspectives of Therapy and Prevention
5. Conclusions

{kind=link}
{kind=link}
| Variables | Main Findings |
|---|---|
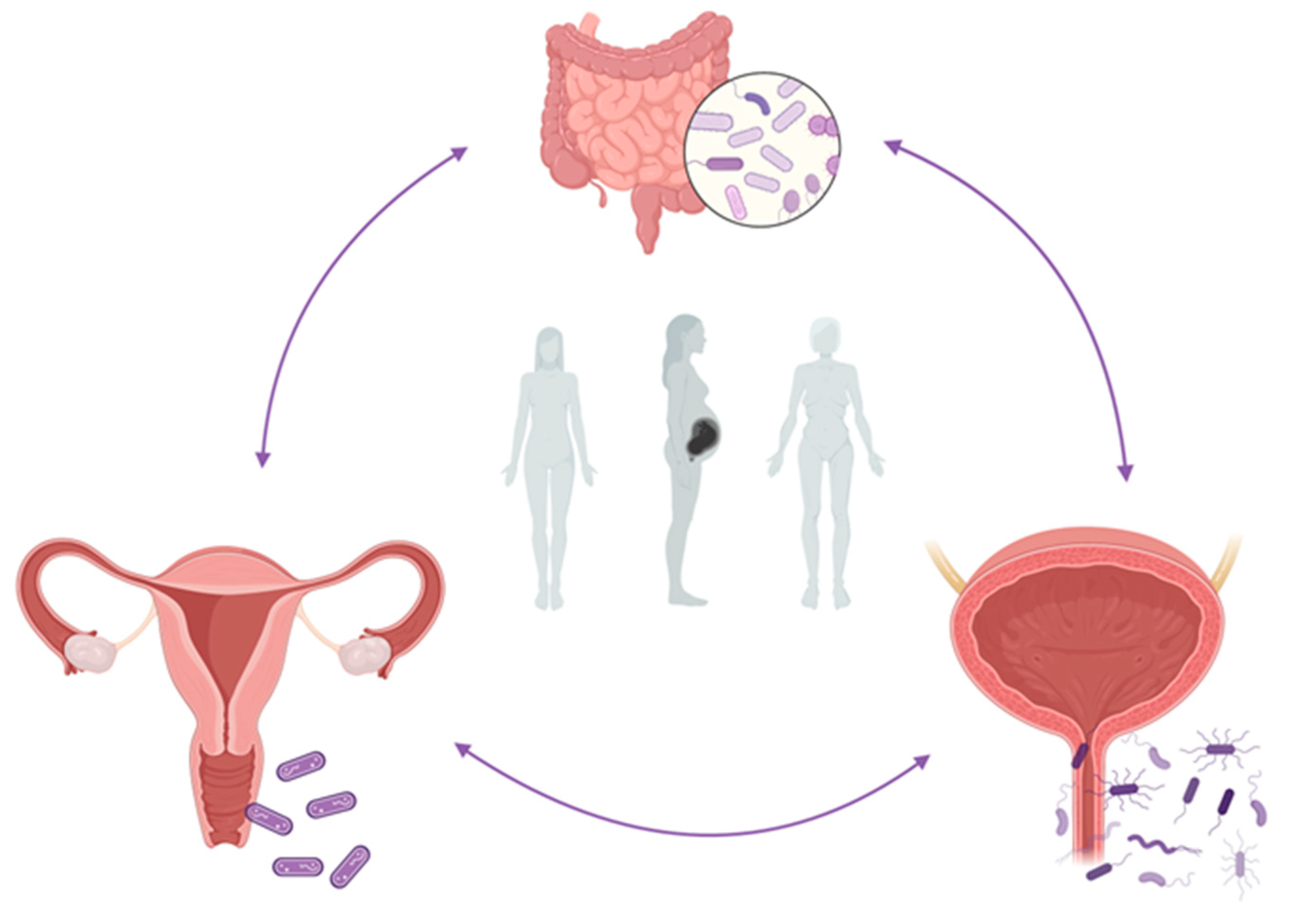
| Role of vaginal microbiome [30,37,44,59,71,72,101,131,138,142] | The vaginal microbiome is involved in rUTIs pathogenesis: if its balance is maintained, it constitutes a barrier against pathogens. However, every change, which we know as bacterial vaginosis, is an important risk factor for the development of urinary tract infections. |
| This may be a consequence of the decrease in vaginal lactobacilli, which seems to allow the growth of gram-positive bacteria, (especially Staphylococcus saprophyticus, Escherichia coli, Enterococcus faecalis, and Streptococcus agalactiae) or Gardnerella vaginalis. | |
| These vaginal bacteria may be present in the vaginal canal and colonize the urinary system, avoiding the immune response and allowing the formation of E.coli reservoirs. | |
| Role of urinary microbiome [61,77,141] | Urinary system microbiota has a key role in preserving urinary health. So, the pathophysiology of rUTI is influenced by urobiome. |
| Indeed, urinary microbiome composition differs between healthy and rUTIs subjects. Specific urine microorganisms are linked to distinct clinical features in women with rUTI. | |
| Risk factors of rUTIs and dysbiosis [10,76,77,78,79] | Risk factors for the development of symptoms include host variables, host behaviours, and bacterial features. Among these, menopause influences the urine microbiota composition following aging and the decrease in oestreogens protection. First of all, it brings altered Lactobacillus composition, increasing the risk of rUTIs. |
| Possible immunological pathways [48,66,122,130,139] | Several microscopic pathways have been identified, including the intracellular bacterial community, QIR, LPS, multimicrobial infection, and urothelial mucosal remodelling. These mechanisms allow uropathogens to persist in the bladder and survive antibiotic therapy and host immune response. Furthermore, immunological defences show some abnormalities in UTI-prone women, such as increased levels of IL-12, absence of T-cell response, less VEGF, lower level of monocyte chemotactic protein 1, the upregulation of immediate-early (IE) genes, such Nur77. |
| New perspectiver of diagnosis [82] | NGS is more sensitive than a conventional urine culture in the detection of uropathogens, highlighting an increased microbiome diversity in the recurrent cystitis group. Additional NGS tests can facilitate rapid decision-making and therapeutic advancement. |
| New perspectives of theraphy [8,32,38,55,140,144,145,152] | Following the understanding of the importance of lactobacilli and oestrogen in the pathophysiology of rUTIs, several studies demonstrated their benefits as therapies. |
| The intravaginal administration of lactobacillus and/or oestrogens is associated with a significant reduction in rUTIs, especially if they are integrated with nonantibiotic therapeutical options as well as modification of behaviour, specific diet, integration with probiotics, and d-mannos, use of local oestrogens therapy, and systemic or local immunostimulants. The administration of one or more of these approaches provides the beneficial treatment to reduce rUTI risk. |
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stamm, W.E.; Norrby, S.R. Urinary Tract Infections: Disease Panorama and Challenges. J. Infect. Dis. 2001, 183 (Suppl. 1), S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.E.; Lacy, S.S.; Hinman, F., Jr. The Urethra and its Relationship to Urinary Tract Infection. II. The Urethral Flora of the Female with Recurrent Urinary Infection. J. Urol. 1968, 99, 632–638. [Google Scholar] [CrossRef]
- Al-Badr, A.; Al-Shaikh, G. Recurrent Urinary Tract Infections Management in Women: A review. Sultan Qaboos Univ. Med. J. 2013, 13, 359–367. [Google Scholar] [CrossRef]
- Renard, J.; Ballarini, S.; Mascarenhas, T.; Zahran, M.; Quimper, E.; Choucair, J.; Iselin, C.E. Recurrent Lower Urinary Tract Infections Have a Detrimental Effect on Patient Quality of Life: A Prospective, Observational Study. Infect. Dis. Ther. 2014, 4, 125–135. [Google Scholar] [CrossRef]
- Dason, S.; Dason, J.T.; Kapoor, A. Guidelines for the diagnosis and management of recurrent urinary tract infection in women. Can. Urol. Assoc. J. 2013, 5, 316–322. [Google Scholar] [CrossRef]
- Sabih, A.; Leslie, S.W. Complicated Urinary Tract Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www-ncbi-nlm-nih-gov.offcampus.lib.washington.edu/books/NBK436013/ (accessed on 12 August 2021).
- Bonkat, G.; Pickard, R.; Bartoletti, R.; Bruyère, F.; Geerlings, S.; Wagenlehner, F.; Wullt, B.; Pradere, B.; Veeratterapillay, R. EAU Guidelines on Urological Infections; European Association of Urology: Arnhem, The Netherlands, 2018. [Google Scholar]
- Sihra, N.; Goodman, A.; Zakri, R.; Sahai, A.; Malde, S. Nonantibiotic prevention and management of recurrent urinary tract infection. Nat. Rev. Urol. 2018, 15, 750–776. [Google Scholar] [CrossRef] [PubMed]
- Boldogh, I.; Albrecht, T.; Porter, D.D. Persistent Viral Infections. In Medical Microbiology, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996; Chapter 46. Available online: https://www.ncbi.nlm.nih.gov/books/NBK8538/ (accessed on 30 January 2023).
- Foxman, B. Urinary Tract Infection Syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Foxman, B.; Gillespie, B.; Koopman, J.; Zhang, L.; Palin, K.; Tallman, P.; Marsh, J.V.; Spear, S.; Sobel, J.D.; Marty, M.J.; et al. Risk Factors for Second Urinary Tract Infection among College Women. Am. J. Epidemiol. 2000, 151, 1194–1205. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B.; Manning, S.; Tallman, P.; Bauer, R.; Zhang, L.; Koopman, J.S.; Gillespie, B.; Sobel, J.D.; Marrs, C.F. Uropathogenic Escherichia coli Are More Likely than Commensal E. coli to Be Shared between Heterosexual Sex Partners. Am. J. Epidemiol. 2002, 156, 1133–1140. [Google Scholar] [CrossRef]
- Murray, B.E.; Rensimer, E.R.; DuPont, H.L. Emergence of high-level trimethoprim resistance in fecal Escherichia coli during oral ad-ministration of trimethoprim or trimethoprim—Sulfamethoxazole. N. Engl. J. Med. 1982, 306, 130–135. [Google Scholar] [CrossRef]
- Wright, S.W.; Wrenn, K.D.; Haynes, M.L. Trimethoprim-sulfamethoxazole resistance among urinary coliform isolates. J. Gen. Intern. Med. 1999, 14, 606–609. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, J.E. The antimicrobial activity of non-antibiotics. Report from a congress on the antimicrobial effect of drugs other than antibiotics on bacteria, viruses, protozoa, and other organisms. APMIS. Suppl. 1992, 30, 7–14. [Google Scholar] [PubMed]
- Ulett, G.C.; Schembri, M.A. Bacterial pathogenesis: Remodelling recurrent infection. Nat. Microbiol. 2016, 2, 16256. [Google Scholar] [CrossRef]
- Langford, B.J.; Brown, K.A.; Diong, C.; Marchand-Austin, A.; Adomako, K.; Saedi, A.; Schwartz, K.L.; Johnstone, J.; MacFadden, D.R.; Matukas, L.M.; et al. The Benefits and Harms of Antibiotic Prophylaxis for Urinary Tract Infection in Older Adults. Clin. Infect. Dis. 2021, 73, e782–e791. [Google Scholar] [CrossRef] [PubMed]
- Gasiorek, M.; Hsieh, M.H.; Forster, C.S. Utility of DNA Next-Generation Sequencing and Expanded Quantitative Urine Culture in Diagnosis and Management of Chronic or Persistent Lower Urinary Tract Symptoms. J. Clin. Microbiol. 2019, 58, e00204-19. [Google Scholar] [CrossRef] [PubMed]
- Thomas-White, K.; Brady, M.; Wolfe, A.J.; Mueller, E.R. The Bladder Is Not Sterile: History and Current Discoveries on the Urinary Microbiome. Curr. Bladder Dysfunct. Rep. 2016, 11, 18–24. [Google Scholar] [CrossRef]
- Pohl, H.G.; Groah, S.L.; Pérez-Losada, M.; Ljungberg, I.; Sprague, B.M.; Chandal, N.; Caldovic, L.; Hsieh, M. The Urine Microbiome of Healthy Men and Women Differs by Urine Collection Method. Int. Neurourol. J. 2020, 24, 41–51. [Google Scholar] [CrossRef]
- Ley, R.E.; Peterson, D.A.; Gordon, J.I. Ecological and Evolutionary Forces Shaping Microbial Diversity in the Human Intestine. Cell 2006, 124, 837–848. [Google Scholar] [CrossRef]
- Higgins, J.; Altman, D.; Sterne, J. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, Version 5.2.0; Higgins, J.P.T., Churchill, R., Chandler, J., Cumpston, M.S., Eds.; John Wiley and Sons: Chichester, UK, 2017. [Google Scholar]
- Schünemann, H.J.; Higgins, J.P.; Vist, G.E.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H.; Cochrane GRADEing Methods Group; Cochrane Statistical Methods Group. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.2; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley and Sons: Chichester, UK, 2021. [Google Scholar]
- Czaja, C.A.; Stamm, W.E.; Stapleton, A.E.; Roberts, P.L.; Hawn, T.R.; Scholes, D.; Samadpour, M.; Hultgren, S.J.; Hooton, T.M. Prospective Cohort Study of Microbial and Inflammatory Events Immediately Preceding Escherichia coli Recurrent Urinary Tract Infection in Women. J. Infect. Dis. 2009, 200, 528–536. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4680–4687. [Google Scholar] [CrossRef]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Nikita, L.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2, 4. [Google Scholar] [CrossRef]
- Tamarelle, J.; Thiébaut, A.; de Barbeyrac, B.; Bébéar, C.; Ravel, J.; Delarocque-Astagneau, E. The vaginal microbiota and its association with human papillomavirus, Chlamydia trachomatis, Neisseria gonorrhoeae and Mycoplasma genitalium infections: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 35–47. [Google Scholar] [CrossRef]
- Borges, S.; Silva, J.; Teixeira, P. The role of lactobacilli and probiotics in maintaining vaginal health. Arch. Gynecol. Obstet. 2013, 289, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.L.; Gilbert, N.M. Roles of the vagina and the vaginal microbiota in urinary tract infection: Evidence from clinical correlations and experimental models. GMS Infect. Dis. 2020, 8, DOC02. [Google Scholar] [CrossRef] [PubMed]
- Hudson, P.L.; Hung, K.J.; Bergerat, A.; Mitchell, C. Effect of Vaginal Lactobacillus Species on Escherichia coli Growth. Urogynecology 2020, 26, 146–151. [Google Scholar] [CrossRef]
- Vagios, S.; Hesham, H.; Mitchell, C. Understanding the potential of lactobacilli in recurrent UTI prevention. Microb. Pathog. 2020, 148, 104544. [Google Scholar] [CrossRef]
- Pfau, A.; Sacks, T. The Bacterial Flora of the Vaginal Vestibule, Urethra and Vagina in Premenopausal Women with Recurrent Urinary Tract Infections. J. Urol. 1981, 126, 630–634. [Google Scholar] [CrossRef]
- Gupta, K.; Stapleton, A.; Hooton, T.M.; Roberts, P.L.; Fennell, C.L.; Stamm, W.E. Inverse Association of H2O2-Producing Lactobacilli and Vaginal Escherichia coli Colonization in Women with Recurrent Urinary Tract Infections. J. Infect. Dis. 1998, 178, 446–450. [Google Scholar] [CrossRef]
- Hooton, T.M.; Fihn, S.D.; Johnson, C.; Roberts, P.L.; Stamm, W.E. Association between bacterial vaginosis and acute cystitis in women using diaphragms. Arch. Intern. Med. 1989, 149, 1932–1936. [Google Scholar] [CrossRef]
- Hooton, T.M.; Roberts, P.L.; Stamm, W.E. Effects of Recent Sexual Activity and Use of a Diaphragm on the Vaginal Microflora. Clin. Infect. Dis. 1994, 19, 274–278. [Google Scholar] [CrossRef]
- Harmanli, O.H.; Cheng, G.Y.; Nyirjesy, P.; Chatwani, A.; Gaughan, J.P. Urinary Tract Infections in Women with Bacterial Vaginosis. Obstet. Gynecol. 2000, 95, 710–712. [Google Scholar] [CrossRef]
- Stapleton, A.E.; Au-Yeung, M.; Hooton, T.M.; Fredricks, D.N.; Roberts, P.L.; Czaja, C.A.; Yarova-Yarovaya, Y.; Fiedler, T.; Cox, M.; Stamm, W.E. Randomized, Placebo-Controlled Phase 2 Trial of a Lactobacillus crispatus Probiotic Given Intravaginally for Prevention of Recurrent Urinary Tract Infection. Clin. Infect. Dis. 2011, 52, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- Amatya, R.; Bhattarai, S.; Mandal, P.K.; Tuladhar, H.; Karki, B.M.S. Urinary tract infection in vaginitis: A condition often overlooked. Nepal. Med. Coll. J. 2013, 15, 65–67. [Google Scholar]
- Navas-Nacher, E.L.; Dardick, F.; Venegas, M.F.; Anderson, B.E.; Schaeffer, A.J.; Duncan, J.L. Relatedness of Escherichia coli Colonizing Women Longitudinally. Mol. Urol. 2001, 5, 31–36. [Google Scholar] [CrossRef]
- Muder, R.R.; Brennen, C.; Rihs, J.D.; Wagener, M.M.; Obman, A.; Stout, J.E.; Yu, V.L. Isolation of Staphylococcus aureus from the Urinary Tract: Association of Isolation with Symptomatic Urinary Tract Infection and Subsequent Staphylococcal Bacteremia. Clin. Infect. Dis. 2006, 42, 46–50. [Google Scholar] [CrossRef]
- Baraboutis, I.G.; Tsagalou, E.P.; Lepinski, J.L.; Papakonstantinou, I.; Papastamopoulos, V.; Skoutelis, A.T.; Johnson, S. Primary Staphylococcus aureus urinary tract infection: The role of undetected hematogenous seeding of the urinary tract. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1095–1101. [Google Scholar] [CrossRef]
- Gilbert, N.M.; O’Brien, V.P.; Hultgren, S.; Macones, G.; Lewis, W.G.; Lewis, A.L. Urinary Tract Infection as a Preventable Cause of Pregnancy Complications: Opportunities, Challenges, and a Global Call to Action. Glob. Adv. Health Med. 2013, 2, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Kline, K.A.; Lewis, A.L. Gram-Positive Uropathogens, Polymicrobial Urinary Tract Infection, and the Emerging Microbiota of the Urinary Tract. Microbiol. Spectr. 2016, 4, UTI-0012-2012. [Google Scholar] [CrossRef] [PubMed]
- Allsworth, J.E.; Lewis, V.A.; Peipert, J.F. Viral Sexually Transmitted Infections and Bacterial Vaginosis: 2001–2004 National Health and Nutrition Examination Survey Data. Sex. Transm. Dis. 2008, 35, 791–796. [Google Scholar] [CrossRef]
- Klein, S.; Nurjadi, D.; Horner, S.; Heeg, K.; Zimmermann, S.; Burckhardt, I. Significant increase in cultivation of Gardnerella vaginalis, Alloscardovia omnicolens, Actinotignum schaalii, and Actinomyces spp. in urine samples with total laboratory automation. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1305–1311. [Google Scholar] [CrossRef]
- Sumati, A.; Saritha, N. Association of urinary tract infection in women with bacterial vaginosis. J. Glob. Infect. Dis. 2009, 1, 151–152. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, N.M.; O’Brien, V.P.; Lewis, A.L. Transient microbiota exposures activate dormant Escherichia coli infection in the bladder and drive severe outcomes of recurrent disease. PLoS Pathog. 2017, 13, e1006238. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.; Vereecken, A.; Bosmans, E.; Dekeersmaecker, A.; Salembier, G.; Spitz, B. Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: Aerobic vaginitis. BJOG Int. J. Obstet. Gynaecol. 2002, 109, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.K.; Ulett, K.B.; Steele, M.; Benjamin, W.H., Jr.; Ulett, G.C. Prognostic value of semi-quantitative bacteruria counts in the diagnosis of group B streptococcus urinary tract infection: A 4-year retrospective study in adult patients. BMC Infect. Dis. 2012, 12, 273. [Google Scholar] [CrossRef] [PubMed]
- Gottschick, C.; Deng, Z.-L.; Vital, M.; Masur, C.; Abels, C.; Pieper, D.H.; Wagner-Döbler, I. The urinary microbiota of men and women and its changes in women during bacterial vaginosis and antibiotic treatment. Microbiome 2017, 5, 99. [Google Scholar] [CrossRef]
- Groah, S.L.; Pérez-Losada, M.; Caldovic, L.; Ljungberg, I.H.; Sprague, B.M.; Castro-Nallar, E.; Chandel, N.J.; Hsieh, M.H.; Pohl, H. Redefining Healthy Urine: A Cross-Sectional Exploratory Metagenomic Study of People with and Without Bladder Dysfunction. J. Urol. 2016, 196, 579–587. [Google Scholar] [CrossRef]
- Forster, C.S.; Pohl, H. Diagnosis of Urinary Tract Infection in the Neuropathic Bladder: Changing the Paradigm to Include the Microbiome. Top. Spinal Cord Inj. Rehabil. 2019, 25, 222–227. [Google Scholar] [CrossRef]
- Whiteside, S.A.; Razvi, H.; Dave, S.; Reid, G.; Burton, J.P. The microbiome of the urinary tract—A role beyond infection. Nat. Rev. Urol. 2015, 12, 81–90. [Google Scholar] [CrossRef]
- Atassi, F.; Ahn, D.L.P.V.; Moal, V.L.-L. Diverse Expression of Antimicrobial Activities Against Bacterial Vaginosis and Urinary Tract Infection Pathogens by Cervicovaginal Microbiota Strains of Lactobacillus gasseri and Lactobacillus crispatus. Front. Microbiol. 2019, 10, 2900. [Google Scholar] [CrossRef]
- De Seta, F.; Lonnee-Hoffmann, R.M.; Campisciano, G.; Comar, M.; Verstraelen, H.M.; Vieira-Baptista, P.; Ventolini, G.M.; Lev-Sagie, A. The Vaginal Microbiome: III. The Vaginal Microbiome in Various Urogenital Disorders. J. Low. Genit. Tract Dis. 2022, 26, 85–92. [Google Scholar] [CrossRef]
- Morand, A.; Cornu, F.; Dufour, J.-C.; Tsimaratos, M.; Lagier, J.-C.; Raoult, D. Human Bacterial Repertoire of the Urinary Tract: A Potential Paradigm Shift. J. Clin. Microbiol. 2019, 57, e00675-18. [Google Scholar] [CrossRef]
- Dubourg, G.; Morand, A.; Mekhalif, F.; Godefroy, R.; Corthier, A.; Yacouba, A.; Diakite, A.; Cornu, F.; Cresci, M.; Brahimi, S.; et al. Deciphering the Urinary Microbiota Repertoire by Culturomics Reveals Mostly Anaerobic Bacteria from the Gut. Front. Microbiol. 2020, 11, 513305. [Google Scholar] [CrossRef]
- Neugent, M.L.; Hulyalkar, N.V.; Nguyen, V.H.; Zimmern, P.E.; De Nisco, N.J. Advances in Understanding the Human Urinary Microbiome and Its Potential Role in Urinary Tract Infection. Mbio 2020, 11, e00218-20. [Google Scholar] [CrossRef]
- Bossa, L.; Kline, K.; McDougald, D.; Lee, B.B.; Rice, S.A. Urinary catheter-associated microbiota change in accordance with treatment and infection status. PLoS ONE 2017, 12, e0177633. [Google Scholar] [CrossRef] [PubMed]
- Burnett, L.A.; Hochstedler, B.R.; Weldon, K.; Wolfe, A.J.; Brubaker, L. Recurrent urinary tract infection: Association of clinical profiles with urobiome composition in women. Neurourol. Urodyn. 2021, 40, 1479–1489. [Google Scholar] [CrossRef] [PubMed]
- Elliott, T.; Reed, L.; Slack, R.; Bishop, M. Bacteriology and ultrastructure of the bladder in patients with urinary tract infections. J. Infect. 1985, 11, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Robino, L.; Scavone, P.; Araujo, L.; Algorta, G.; Zunino, P.; Pírez, M.C.; Vignoli, R. Intracellular Bacteria in the Pathogenesis of Escherichia coli Urinary Tract Infection in Children. Clin. Infect. Dis. 2014, 59, e158–e164. [Google Scholar] [CrossRef]
- Rosen, D.A.; Hooton, T.M.; Stamm, W.E.; Humphrey, P.A.; Hultgren, S.J. Detection of Intracellular Bacterial Communities in Human Urinary Tract Infection. PLoS Med. 2007, 4, e329. [Google Scholar] [CrossRef]
- Liu, S.-C.; Han, X.-M.; Shi, M.; Pang, Z.-L. Persistence of uropathogenic Escherichia Coli in the bladders of female patients with sterile urine after antibiotic therapies. J. Huazhong Univ. Sci. Technol. 2016, 36, 710–715. [Google Scholar] [CrossRef]
- De Nisco, N.J.; Neugent, M.; Mull, J.; Chen, L.; Kuprasertkul, A.; de Souza Santos, M.; Palmer, K.L.; Zimmern, P.; Orth, K. Direct detection of tissue-resident bacteria and chronic inflammation in the bladder wall of postmenopausal women with recurrent urinary tract infection. J. Mol. Biol. 2019, 431, 4368–4379. [Google Scholar] [CrossRef] [PubMed]
- Ejrnaes, K.; Sandvang, D.; Lundgren, B.; Ferry, S.; Holm, S.; Monsen, T.; Lundholm, R.; Frimodt-Moller, N. Pulsed-Field Gel Electrophoresis Typing of Escherichia coli Strains from Samples Collected before and after Pivmecillinam or Placebo Treatment of Uncomplicated Community-Acquired Urinary Tract Infection in Women. J. Clin. Microbiol. 2006, 44, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Ma, Y.; Zhao, Q.; Wang, L.; Guo, L.; Ye, L.; Zhang, Y.; Yang, J. Similarity and Divergence of Phylogenies, Antimicrobial Susceptibilities, and Virulence Factor Profiles of Escherichia coli Isolates Causing Recurrent Urinary Tract Infections That Persist or Result from Reinfection. J. Clin. Microbiol. 2012, 50, 4002–4007. [Google Scholar] [CrossRef] [PubMed]
- Skjøt-Rasmussen, L.; Olsen, S.; Jakobsen, L.; Ejrnæs, K.; Scheutz, F.; Lundgren, B.; Frimodt-Møller, N.; Hammerum, A. Escherichia coli clonal group A causing bacteraemia of urinary tract origin. Clin. Microbiol. Infect. 2013, 19, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Kõljalg, S.; Truusalu, K.; Stsepetova, J.; Pai, K.; Vainumäe, I.; Sepp, E.; Mikelsaar, M. The Escherichia coli phylogenetic group B2 with integrons prevails in childhood recurrent urinary tract infections. Apmis 2014, 122, 452–458. [Google Scholar] [CrossRef]
- Yoo, J.-J.; Song, J.S.; Bin Kim, W.; Yun, J.; Shin, H.B.; Jang, M.-A.; Ryu, C.B.; Kim, S.S.; Chung, J.C.; Kuk, J.C.; et al. Gardnerella vaginalis in Recurrent Urinary Tract Infection Is Associated with Dysbiosis of the Bladder Microbiome. J. Clin. Med. 2022, 11, 2295. [Google Scholar] [CrossRef]
- Stapleton, A.E. The Vaginal Microbiota and Urinary Tract Infection. Microbiol. Spectr. 2016, 4, 79–86. [Google Scholar] [CrossRef]
- Raz, R. Urinary Tract Infection in Postmenopausal Women. Korean J. Urol. 2011, 52, 801–808. [Google Scholar] [CrossRef]
- Muhleisen, A.L.; Herbst-Kralovetz, M.M. Menopause and the vaginal microbiome. Maturitas 2016, 91, 42–50. [Google Scholar] [CrossRef]
- Mitchell, C.M.; Waetjen, L.E. Genitourinary changes with aging. Obstet. Gynecol. Clin. N. Am. 2018, 45, 737–750. [Google Scholar] [CrossRef]
- Bhide, A.; Tailor, V.; Khullar, V. Interstitial cystitis/bladder pain syndrome and recurrent urinary tract infection and the potential role of the urinary microbiome. Post Reprod. Health 2020, 26, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Brubaker, L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric 2019, 22, 242–249. [Google Scholar] [CrossRef]
- Hugenholtz, F.; van der Veer, C.; Terpstra, M.L.; Borgdorff, H.; van Houdt, R.; Bruisten, S.; Geerlings, S.E.; van de Wijgert, J.H.H.M. Urine and vaginal microbiota compositions of postmenopausal and premenopausal women differ regardless of recurrent urinary tract infection and renal transplant status. Sci. Rep. 2022, 12, 2698. [Google Scholar] [CrossRef]
- Vaughan, M.H.; Mao, J.; Karstens, L.A.; Ma, L.; Amundsen, C.L.; Schmader, K.E.; Siddiqui, N.Y. The Urinary Microbiome in Postmenopausal Women with Recurrent Urinary Tract Infections. J. Urol. 2021, 206, 1222–1231. [Google Scholar] [CrossRef] [PubMed]
- Curtiss, N.; Balachandran, A.; Krska, L.; Peppiatt-Wildman, C.; Wildman, S.; Duckett, J. Age, menopausal status and the bladder microbiome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 126–129. [Google Scholar] [CrossRef]
- Biagi, E.; Candela, M.; Fairweather-Tait, S.; Franceschi, C.; Brigidi, P. Ageing of the human metaorganism: The microbial counterpart. Age 2011, 34, 247–267. [Google Scholar] [CrossRef]
- Yoo, J.-J.; Shin, H.B.; Song, J.S.; Kim, M.; Yun, J.; Kim, Z.; Lee, Y.M.; Lee, S.W.; Lee, K.W.; Kim, W.b.; et al. Urinary Microbiome Characteristics in Female Patients with Acute Uncomplicated Cystitis and Recurrent Cystitis. J. Clin. Med. 2021, 10, 1097. [Google Scholar] [CrossRef]
- Ansaldi, Y.; Weber, B.M.d.T. Urinary tract infections in pregnancy. Clin. Microbiol. Infect. 2022. [Google Scholar] [CrossRef] [PubMed]
- DiGiulio, D.B.; Callahan, B.J.; McMurdie, P.J.; Costello, E.K.; Lyell, D.J.; Robaczewska, A.; Sun, C.L.; Goltsman, D.S.A.; Wong, R.J.; Shaw, G.; et al. Temporal and spatial variation of the human microbiota during pregnancy. Proc. Natl. Acad. Sci. USA 2015, 112, 11060–11065. [Google Scholar] [CrossRef]
- Fettweis, J.M.; Serrano, M.G.; Brooks, J.P.; Edwards, D.J.; Girerd, P.H.; Parikh, H.I.; Huang, B.; Arodz, T.J.; Edupuganti, L.; Glascock, A.L.; et al. The vaginal microbiome and preterm birth. Nat. Med. 2019, 25, 1012–1021. [Google Scholar] [CrossRef]
- Dominguez-Bello, M.G. Gestational shaping of the maternal vaginal microbiome. Nat. Med. 2019, 25, 882–883. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M.; Gupta, K. Recurrent Urinary Tract Infection in Women; UpToDate: Waltham, MA, USA, 2016. [Google Scholar]
- Eschenbach, D.A.; Patton, D.L.; Meier, A.; Thwin, S.S.; Aura, J.; Stapleton, A.; Hooton, T.M. Effects of oral contraceptive pill use on vaginal flora and vaginal epithelium. Contraception 2000, 62, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hillier, S.L.; Hooton, T.M.; Roberts, P.L.; Stamm, W.E. Effects of Contraceptive Method on the Vaginal Microbial Flora: A Prospective Evaluation. J. Infect. Dis. 2000, 181, 595–601. [Google Scholar] [CrossRef]
- Hooton, T.M.; Hillier, S.; Johnson, C.; Roberts, P.L.; Stamm, W.E. Escherichia coli Bacteriuria and Contraceptive Method. JAMA 1991, 265, 64–69. [Google Scholar] [CrossRef]
- Hooton, T.M.; Scholes, D.; Roberts, P.L.; Stapleton, A.; Stergachis, A.; Stamm, W.E. A prospective cohort study of the association between UTI and contraceptive method. Abstr. Intersci. Conf. Antimicrob. Agents Chemother. 1994, 34, 134. [Google Scholar]
- Hooton, T.M.; Fennell, C.L.; Clark, A.M.; Stamm, W.E. Nonoxynol-9: Differential Antibacterial Activity and Enhancement of Bacterial Adherence to Vaginal Epithelial Cells. J. Infect. Dis. 1991, 164, 1216–1219. [Google Scholar] [CrossRef] [PubMed]
- Achilles, S.L.; Hillier, S.L. The complexity of contraceptives: Understanding their impact on genital immune cells and vaginal microbiota. AIDS 2013, 27 (Suppl 1), S5–S15. [Google Scholar] [CrossRef]
- Raz, R.; Stamm, W.E. A Controlled Trial of Intravaginal Estriol in Postmenopausal Women with Recurrent Urinary Tract Infections. N. Engl. J. Med. 1993, 329, 753–756. [Google Scholar] [CrossRef]
- Stapleton, A.; Latham, R.H.; Johnson, C.; Stamm, W.E. Postcoital antimicrobial prophylaxis for recurrent urinary tract infection. A randomized, double-blind, placebo-controlled trial. JAMA 1990, 264, 703–706. [Google Scholar] [CrossRef]
- Stamatiou, C.; Bovis, C.; Panagopoulos, P.; Petrakos, G.; Economou, A.; Lycoudt, A. Sex-induced cystitis--patient burden and other epidemiological features. Clin. Exp. Obstet. Gynecol. 2005, 32, 180–182. [Google Scholar]
- Hooton, T.M.; Scholes, D.; Hughes, J.P.; Winter, C.; Roberts, P.L.; Stapleton, A.E.; Stergachis, A.; Stamm, W.E. A Prospective Study of Risk Factors for Symptomatic Urinary Tract Infection in Young Women. N. Engl. J. Med. 1996, 335, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Scholes, D.; Hooton, T.M.; Roberts, P.L.; Stapleton, A.; Gupta, K.; Stamm, W.E. Risk Factors for Recurrent Urinary Tract Infection in Young Women. J. Infect. Dis. 2000, 182, 1177–1182. [Google Scholar] [CrossRef]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef]
- Cumpanas, A.A.; Bratu, O.G.; Bardan, R.; Ferician, O.C.; Cumpanas, A.D.; Horhat, F.G.; Licker, M.; Pricop, C.; Cretu, O.M. Urinary Microbiota—Are We Ready for Prime Time? A Literature Review of Study Methods’ Critical Steps in Avoiding Contamination and Minimizing Biased Results. Diagnostics 2020, 10, 343. [Google Scholar] [CrossRef] [PubMed]
- Meštrović, T.; Matijašić, M.; Perić, M.; Čipčić Paljetak, H.; Barešić, A.; Verbanac, D. The Role of Gut, Vaginal, and Urinary Microbiome in Urinary Tract Infections: From Bench to Bedside. Diagnostics 2021, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, A.J.; Brubaker, L. Urobiome updates: Advances in urinary microbiome research. Nat. Rev. Urol. 2019, 16, 73–74. [Google Scholar] [CrossRef]
- Lewis, D.A.; Brown, R.; Williams, J.; White, P.; Jacobson, S.K.; Marchesi, J.R.; Drake, M.J. The human urinary microbiome; bacterial DNA in voided urine of asymptomatic adults. Front. Cell. Infect. Microbiol. 2013, 3, 41. [Google Scholar] [CrossRef]
- Finucane, T.E. ‘Urinary tract infection’ and the microbiome. Am. J. Med. 2017, 130, e97–e98. [Google Scholar] [CrossRef]
- Ackerman, A.L.; Chai, T.C. The Bladder is Not Sterile: An Update on the Urinary Microbiome. Curr. Bladder Dysfunct. Rep. 2019, 14, 331–341. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. Female Gut and Genital Tract Microbiota-Induced Crosstalk and Differential Effects of Short-Chain Fatty Acids on Immune Sequelae. Front. Immunol. 2020, 11, 2184. [Google Scholar] [CrossRef]
- Brubaker, L.; Wolfe, A.J. The new world of the urinary microbiota in women. Am. J. Obstet. Gynecol. 2015, 213, 644–649. [Google Scholar] [CrossRef]
- Wolfe, A.J.; Toh, E.; Shibata, N.; Rong, R.; Kenton, K.; FitzGerald, M.; Mueller, E.R.; Schreckenberger, P.; Dong, Q.; Nelson, D.E.; et al. Evidence of Uncultivated Bacteria in the Adult Female Bladder. J. Clin. Microbiol. 2012, 50, 1376–1383. [Google Scholar] [CrossRef]
- Hilt, E.E.; McKinley, K.; Pearce, M.M.; Rosenfeld, A.B.; Zilliox, M.J.; Mueller, E.R.; Brubaker, L.; Gai, X.; Wolfe, A.J.; Schreckenberger, P.C. Urine Is Not Sterile: Use of Enhanced Urine Culture Techniques to Detect Resident Bacterial Flora in the Adult Female Bladder. J. Clin. Microbiol. 2014, 52, 871–876. [Google Scholar] [CrossRef]
- Price, T.K.; Dune, T.; Hilt, E.E.; Thomas-White, K.J.; Kliethermes, S.; Brincat, C.; Brubaker, L.; Wolfe, A.J.; Mueller, E.R.; Schreckenberger, P.C. The Clinical Urine Culture: Enhanced Techniques Improve Detection of Clinically Relevant Microorganisms. J. Clin. Microbiol. 2016, 54, 1216–1222. [Google Scholar] [CrossRef]
- Pearce, M.M.; Hilt, E.E.; Rosenfeld, A.B.; Zilliox, M.J.; Thomas-White, K.; Fok, C.; Kliethermes, S.; Schreckenberger, P.C.; Brubaker, L.; Gai, X.; et al. The Female Urinary Microbiome: A Comparison of Women with and without Urgency Urinary Incontinence. Mbio 2014, 5, e01283-14. [Google Scholar] [CrossRef] [PubMed]
- Khasriya, R.; Sathiananthamoorthy, S.; Ismail, S.; Kelsey, M.; Wilson, M.; Rohn, J.L.; Malone-Lee, J. Spectrum of Bacterial Colonization Associated with Urothelial Cells from Patients with Chronic Lower Urinary Tract Symptoms. J. Clin. Microbiol. 2013, 51, 2054–2062. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; Kameh, D.; Johnson, M.E.; Johansen, T.E.B.; Albala, D.; Mouraviev, V. A Head-to-Head Comparative Phase II Study of Standard Urine Culture and Sensitivity Versus DNA Next-generation Sequencing Testing for Urinary Tract Infections. Rev. Urol. 2017, 19, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, T.; Watanabe, N.; Inoue, S.; Aoki, H.; Tsuji, T.; Yamamoto, B.; Yanagi, H.; Oki, M.; Kryukov, K.; Nakagawa, S.; et al. Usefulness of next-generation DNA sequencing for the diagnosis of urinary tract infection. Drug Discov. Ther. 2020, 14, 42–49. [Google Scholar] [CrossRef]
- Bennett, J.E.; Dolin, R.; Blaser, M.J. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier Health Sciences: Philadelphia, PA, USA, 2014; Volume 2. [Google Scholar]
- Hooton, T.M. Recurrent urinary tract infection in women. Int. J. Antimicrob. Agents 2001, 17, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Brannon, J.R.; Dunigan, T.L.; Beebout, C.J.; Ross, T.; Wiebe, M.A.; Reynolds, W.S.; Hadjifrangiskou, M. Invasion of vaginal epithelial cells by uropathogenic Escherichia coli. Nat. Commun. 2020, 11, 2803. [Google Scholar] [CrossRef]
- Rosen, D.A.; Pinkner, J.S.; Jones, J.M.; Walker, J.N.; Clegg, S.; Hultgren, S.J. Utilization of an Intracellular Bacterial Community Pathway in Klebsiella pneumoniae Urinary Tract Infection and the Effects of FimK on Type 1 Pilus Expression. Infect. Immun. 2008, 76, 3337–3345. [Google Scholar] [CrossRef] [PubMed]
- Robino, L.; Scavone, P.; Araujo, L.; Algorta, G.; Zunino, P.; Vignoli, R. Detection of intracellular bacterial communities in a child with Escherichia coli recurrent urinary tract infections. Pathog. Dis. 2013, 68, 78–81. [Google Scholar] [CrossRef]
- Schilling, J.D.; Lorenz, R.G.; Hultgren, S.J. Effect of Trimethoprim-Sulfamethoxazole on Recurrent Bacteriuria and Bacterial Persistence in Mice Infected with Uropathogenic Escherichia coli. Infect. Immun. 2002, 70, 7042–7049. [Google Scholar] [CrossRef]
- Mysorekar, I.U.; Hultgren, S.J. Mechanisms of uropathogenic Escherichia coli persistence and eradication from the urinary tract. Proc. Natl. Acad. Sci. USA 2006, 103, 14170–14175. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Ahn, J.H.; Choi, W.S.; Park, H.K.; Kim, S.; Paick, S.H.; Kim, H.G. What is the Cause of Recurrent Urinary Tract Infection? Contemporary Microscopic Concepts of Pathophysiology. Int. Neurourol. J. 2021, 25, 192–201. [Google Scholar] [CrossRef]
- Simpson, B.W.; May, J.M.; Sherman, D.J.; Kahne, D.; Ruiz, N. Lipopolysaccharide transport to the cell surface: Biosynthesis and extraction from the inner membrane. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20150029. [Google Scholar] [CrossRef]
- Zhang, G.; Meredith, T.C.; Kahne, D. On the essentiality of lipopolysaccharide to Gram-negative bacteria. Curr. Opin. Microbiol. 2013, 16, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Hunstad, D.A.; Justice, S.S.; Hung, C.S.; Lauer, S.R.; Hultgren, S.J. Suppression of Bladder Epithelial Cytokine Responses by Uropathogenic Escherichia coli. Infect. Immun. 2005, 73, 3999–4006. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, H.; Kouadir, M.; Song, H.; Shi, F. Recent advances in the mechanisms of NLRP3 inflammasome activation and its inhibitors. Cell Death Dis. 2019, 10, 128. [Google Scholar] [CrossRef]
- Hughes, F.M., Jr.; Vivar, N.P.; Kennis, J.G.; Pratt-Thomas, J.D.; Lowe, D.W.; Shaner, B.E.; Nietert, P.J.; Spruill, L.S.; Purves, J.T. Inflammasomes are important mediators of cyclo¬phosphamide-induced bladder inflammation. Am. J. Physiol. Ren. Physiol. 2014, 306, F299–F308. [Google Scholar] [CrossRef]
- Jaillon, S.; Moalli, F.; Ragnarsdottir, B.; Bonavita, E.; Puthia, M.; Riva, F.; Barbati, E.; Nebuloni, M.; Krajinovic, L.C.; Markotic, A.; et al. The Humoral Pattern Recognition Molecule PTX3 Is a Key Component of Innate Immunity against Urinary Tract Infection. Immunity 2014, 40, 621–632. [Google Scholar] [CrossRef]
- Bishop, B.L.; Duncan, M.J.; Song, J.; Li, G.; Zaas, D.; Abraham, S.N. Cyclic AMP–regulated exocytosis of Escherichia coli from infected bladder epithelial cells. Nat. Med. 2007, 13, 625–630. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, V.P.; Lewis, A.L.; Gilbert, N.M. Bladder Exposure to Gardnerella Activates Host Pathways Necessary for Escherichia coli Recurrent UTI. Front. Cell. Infect. Microbiol. 2021, 11, 788229. [Google Scholar] [CrossRef]
- Yoon, K.; Lee, S.-O.; Cho, S.-D.; Kim, K.; Khan, S.; Safe, S. Activation of nuclear TR3 (NR4A1) by a diindolylmethane analog induces apoptosis and proapoptotic genes in pancreatic cancer cells and tumors. Carcinog. 2011, 32, 836–842. [Google Scholar] [CrossRef]
- Gao, H.; Chen, Z.; Fu, Y.; Yang, X.; Weng, R.; Wang, R.; Lu, J.; Pan, M.; Jin, K.; McElroy, C.; et al. Nur77 exacerbates PC12 cellular injury in vitro by aggravating mitochondrial impairment and endoplasmic reticulum stress. Sci. Rep. 2016, 6, 34403. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, A.; Cho, Y.A.; Yelent, B.; Koza-Taylor, P.H.; Li, D.; Chen, E.; Whang, M.; Kang, C.; Turi, T.G.; Winoto, A. Transcriptional activation of known and novel apoptotic pathways by Nur77 orphan steroid receptor. EMBO J. 2003, 22, 6526–6536. [Google Scholar] [CrossRef] [PubMed]
- Herring, J.A.; Elison, W.S.; Tessem, J.S. Function of Nr4a Orphan Nuclear Receptors in Proliferation, Apoptosis and Fuel Utilization Across Tissues. Cells 2019, 8, 1373. [Google Scholar] [CrossRef]
- Rodríguez-Calvo, R.; Tajes, M.; Vázquez-Carrera, M. The NR4A subfamily of nuclear receptors: Potential new therapeutic targets for the treatment of inflammatory diseases. Expert Opin. Ther. Targets 2017, 21, 291–304. [Google Scholar] [CrossRef]
- Liebmann, M.; Hucke, S.; Koch, K.; Eschborn, M.; Ghelman, J.; Chasan, A.I.; Glander, S.; Schädlich, M.; Kuhlencord, M.; Daber, N.M.; et al. Nur77 serves as a molecular brake of the metabolic switch during T cell activation to restrict autoimmunity. Proc. Natl. Acad. Sci. USA 2018, 115, E8017–E8026. [Google Scholar] [CrossRef]
- Hanna, R.N.; Carlin, L.M.; Hubbeling, H.G.; Nackiewicz, D.; Green, A.M.; Punt, J.A.; Geissmann, F.; Hedrick, C.C. The transcription factor NR4A1 (Nur77) controls bone marrow differentiation and the survival of Ly6C− monocytes. Nat. Immunol. 2011, 12, 778–785. [Google Scholar] [CrossRef]
- O’Brien, V.P.; Joens, M.S.; Lewis, A.L.; Gilbert, N.M. Recurrent Escherichia coli Urinary Tract Infection Triggered by Gardnerella vaginalis Bladder Exposure in Mice. J. Vis. Exp. 2020, 166, e61967. [Google Scholar] [CrossRef]
- Kirjavainen, P.V.; Pautler, S.; Baroja, M.L.; Anukam, K.; Crowley, K.; Carter, K.; Reid, G. Abnormal Immunological Profile and Vaginal Microbiota in Women Prone to Urinary Tract Infections. Clin. Vaccine Immunol. 2009, 16, 29–36. [Google Scholar] [CrossRef]
- Neugent, M.L.; Kumar, A.; Hulyalkar, N.V.; Lutz, K.C.; Nguyen, V.H.; Fuentes, J.L.; Zhang, C.; Nguyen, A.; Sharon, B.M.; Kuprasertkul, A.; et al. Recurrent urinary tract infection and estrogen shape the taxonomic ecology and function of the postmenopausal urogenital microbiome. Cell Rep. Med. 2022, 3, 100753. [Google Scholar] [CrossRef]
- Akgul, T.; Karakan, T. The role of probiotics in women with recurrent urinary tract infections. Turk. J. Urol. 2018, 44, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Boswell-Ruys, C.L.; Toh, S.-L.; Lee, B.S.B.; Simpson, J.M.; Clezy, K.R. Probiotics for preventing urinary tract infection in people with neuropathic bladder. Cochrane Database Syst. Rev. 2017, 9, 010723. [Google Scholar] [CrossRef]
- Goneau, L.W.; Yeoh, N.S.; MacDonald, K.W.; Cadieux, P.A.; Burton, J.P.; Razvi, H.; Reid, G. Selective Target Inactivation Rather than Global Metabolic Dormancy Causes Antibiotic Tolerance in Uropathogens. Antimicrob. Agents Chemother. 2014, 58, 2089–2097. [Google Scholar] [CrossRef]
- Uehara, S.; Monden, K.; Nomoto, K.; Seno, Y.; Kariyama, R.; Kumon, H. A pilot study evaluating the safety and effectiveness of Lactobacillus vaginal suppositories in patients with recurrent urinary tract infection. Int. J. Antimicrob. Agents 2006, 28 (Suppl. 1), 30–34. [Google Scholar] [CrossRef]
- Sadahira, T.; Wada, K.; Araki, M.; Mitsuhata, R.; Yamamoto, M.; Maruyama, Y.; Iwata, T.; Watanabe, M.; Watanabe, T.; Kariyama, R.; et al. Efficacy of Lactobacillus vaginal suppositories for the prevention of recurrent cystitis: A phase II clinical trial. Int. J. Urol. 2021, 28, 1026–1031. [Google Scholar] [CrossRef]
- Reid, G.; Charbonneau, D.; Erb, J.; Kochanowski, B.; Beuerman, D.; Poehner, R.; Bruce, A.W. Oral use of Lactobacillus rhamnosus GR-1 and L. fermentum RC-14 significantly alters vaginal flora: Randomized, placebo-controlled trial in 64 healthy women. FEMS Immunol. Med. Microbiol. 2003, 35, 131–134. [Google Scholar] [CrossRef]
- Garofalo, L.; Nakama, C.; Hanes, D.; Zwickey, H. Whole-Person, Urobiome-Centric Therapy for Uncomplicated Urinary Tract Infection. Antibiotics 2022, 11, 218. [Google Scholar] [CrossRef]
- Heinemann, C.; Reid, G. Vaginal microbial diversity among postmenopausal women with and without hormone replacement therapy. Can. J. Microbiol. 2005, 51, 777–781. [Google Scholar] [CrossRef]
- Raz, R. Hormone Replacement Therapy or Prophylaxis in Postmenopausal Women with Recurrent Urinary Tract Infection. J. Infect. Dis. 2001, 183, S74–S76. [Google Scholar] [CrossRef] [PubMed]
- Cauci, S.; Driussi, S.; De Santo, D.; Penacchioni, P.; Iannicelli, T.; Lanzafame, P.; De Seta, F.; Quadrifoglio, F.; de Aloysio, D.; Guaschino, S. Prevalence of Bacterial Vaginosis and Vaginal Flora Changes in Peri- and Postmenopausal Women. J. Clin. Microbiol. 2002, 40, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, B.C. A randomized, open, parallel-group study on the preventive effect of an estradiol-releasing vaginal ring (Estring) on recurrent urinary tract infections in postmenopausal women. Am. J. Obstet. Gynecol. 1999, 180, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Wheeler, T.L., 2nd; Snyder, T.E.; Richter, H.E. Local Effects of Vaginally Administered Estrogen Therapy: A Review. J. Pelvic Med. Surg. 2009, 15, 105–114. [Google Scholar] [CrossRef]
- Mehta, J.; Utkarsh, K.; Fuloria, S.; Singh, T.; Sekar, M.; Salaria, D.; Rolta, R.; Begum, M.Y.; Gan, S.H.; Rani, N.N.I.M.; et al. Antibacterial Potential of Bacopa monnieri (L.) Wettst. and Its Bioactive Molecules against Uropathogens—An In Silico Study to Identify Potential Lead Molecule(s) for the Development of New Drugs to Treat Urinary Tract Infections. Molecules 2022, 27, 4971. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dominoni, M.; Scatigno, A.L.; La Verde, M.; Bogliolo, S.; Melito, C.; Gritti, A.; Pasquali, M.F.; Torella, M.; Gardella, B. Microbiota Ecosystem in Recurrent Cystitis and the Immunological Microenvironment of Urothelium. Healthcare 2023, 11, 525. https://doi.org/10.3390/healthcare11040525
Dominoni M, Scatigno AL, La Verde M, Bogliolo S, Melito C, Gritti A, Pasquali MF, Torella M, Gardella B. Microbiota Ecosystem in Recurrent Cystitis and the Immunological Microenvironment of Urothelium. Healthcare. 2023; 11(4):525. https://doi.org/10.3390/healthcare11040525
Chicago/Turabian StyleDominoni, Mattia, Annachiara Licia Scatigno, Marco La Verde, Stefano Bogliolo, Chiara Melito, Andrea Gritti, Marianna Francesca Pasquali, Marco Torella, and Barbara Gardella. 2023. "Microbiota Ecosystem in Recurrent Cystitis and the Immunological Microenvironment of Urothelium" Healthcare 11, no. 4: 525. https://doi.org/10.3390/healthcare11040525
APA StyleDominoni, M., Scatigno, A. L., La Verde, M., Bogliolo, S., Melito, C., Gritti, A., Pasquali, M. F., Torella, M., & Gardella, B. (2023). Microbiota Ecosystem in Recurrent Cystitis and the Immunological Microenvironment of Urothelium. Healthcare, 11(4), 525. https://doi.org/10.3390/healthcare11040525