_Rachiotis.png)
Effects of a Comic Booklet Intervention Aimed at Preventing Second-Hand Smoke Exposure for Pregnant Women in Indonesia: A Randomised Controlled Trial

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Randomisation
2.5. Interventions
2.6. Study Tools
2.6.1. Primary Outcomes
2.6.2. Secondary Outcomes
2.7. Statistical Analysis
2.8. Ethical Approval, Research Permissions, and Clinical Trial Registration
3. Results
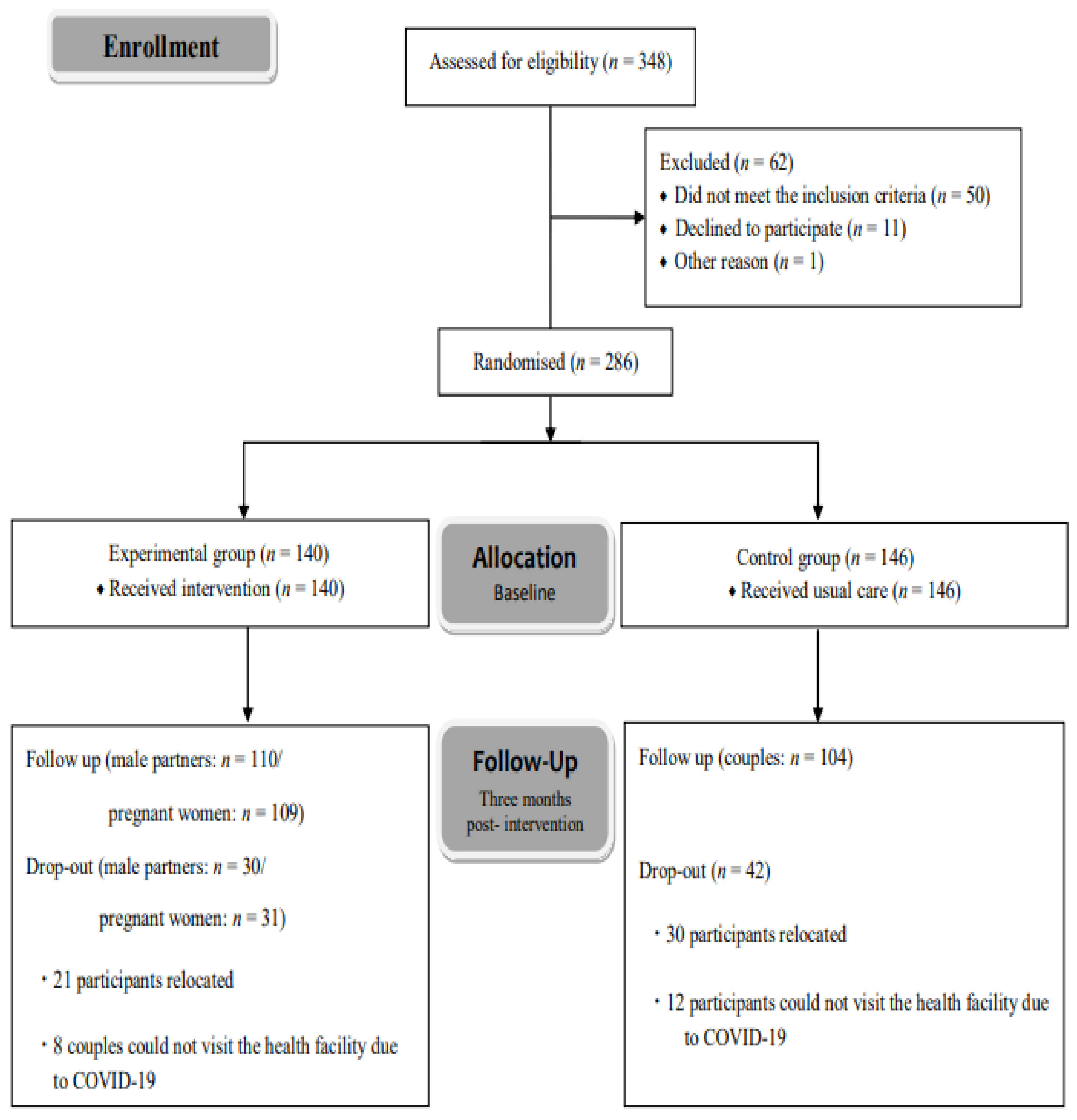
3.1. Participants
3.2. Baseline Participant Characteristics
3.3. Cronbach’s Alpha Coefficients for Each Domain
3.4. Missing Completely at Random Test Results
3.5. Primary Outcome Analyses
3.5.1. SHS Avoidance in Pregnant Women
3.5.2. Male Partners’ Smoking Behaviours
3.6. Secondary Outcome Analyses
3.6.1. Pregnant Women’s Health Beliefs and Self-Efficacy
3.6.2. Male Partners’ Health Beliefs and Self-Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cui, H.; Gong, T.-T.; Liu, C.-X.; Wu, Q.-J. Associations between passive maternal smoking during pregnancy and preterm birth: Evidence from a meta-analysis of observational studies. PLoS ONE 2016, 11, e0147848. [Google Scholar] [CrossRef]
- Abdullah, B.; Muadz, B.; Norizal, M.N.; Ismail, N.; Kornain, N.K.; Kutty, M. Pregnancy outcome and cord blood cotinine level: A cross-sectional comparative study between secondhand smokers and non-secondhand smokers. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 86–90. [Google Scholar] [CrossRef]
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic review and meta-analysis of miscarriage and maternal exposure to tobacco smoke during pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef] [PubMed]
- Pineles, B.L.; Hsu, S.; Park, E.; Samet, J.M. Systematic review and meta-analyses of perinatal death and maternal exposure to tobacco smoke during pregnancy. Am. J. Epidemiol. 2016, 184, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Xie, G.; Yang, T.; Qin, J. Congenital malformations are associated with secondhand smoke among nonsmoking women: A meta-analysis. Birth 2019, 46, 222–233. [Google Scholar] [CrossRef]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D.; Knowledge Synthesis Group. Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef] [PubMed]
- Goel, P.; Radotra, A.; Singh, I.; Aggarwal, A.; Dua, D. Effects of passive smoking on outcome in pregnancy. J. Postgrad. Med. 2004, 50, 12–16. [Google Scholar] [PubMed]
- Zeng, Y.N.; Li, Y.M. Secondhand smoke exposure and mental health in adults: A meta-analysis of cross-sectional studies. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A. Living with the past: Evolution, development, and patterns of disease. Science 2004, 305, 1733–1736. [Google Scholar] [CrossRef]
- Baker, D.J. The fetal and infant origins of adult disease. BMJ Br. Med. J. 1990, 301, 1111. [Google Scholar] [CrossRef]
- Smith, C.J.; Ryckman, K.K.; Barnabei, V.M.; Howard, B.V.; Isasi, C.R.; Sarto, G.E.; Tom, S.E.; Van Horn, L.V.; Wallace, R.B.; Robinson, J.G. The impact of birth weight on cardiovascular disease risk in the Women’s Health Initiative. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 239–245. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025, 3rd ed. Available online: https://www.who.int/publications/i/item/who-global-report-on-trends-in-prevalence-of-tobacco-use-2000-2025-third-edition (accessed on 3 February 2023).
- Andriani, H.; Rahmawati, N.D.; Ahsan, A.; Kusuma, D. Second-hand smoke exposure inside the house and adverse birth outcomes in Indonesia: Evidence from demographic and health survey 2017. medRxiv 2021. [Google Scholar] [CrossRef]
- Barraclough, S. Women and tobacco in Indonesia. Tob. Control 1999, 8, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Republic of Indonesia. There Is No Limit to the Level of Exposure to Cigarette Smoke and Cigarette Residues That Are Safe for Children. Available online: http://p2ptm.kemkes.go.id/infographic/tidak-ada-batas-kadar-pajanan-asap-rokok-dan-residu-rokok-yang-aman-untuk-anak (accessed on 3 February 2023).
- Ministry of Health Republic of Indonesia. Smoke-Free Conditions Must Be Pursued Together, Both Active and Non-Smokers. Available online: http://p2ptm.kemkes.go.id/infographic/kondisi-bebas-asap-rokok-harus-diupayakan-bersama-baik-perokok-aktif-maupun-bukan (accessed on 3 February 2023).
- Behbod, B.; Sharma, M.; Baxi, R.; Roseby, R.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2018, 1, CD001746. [Google Scholar] [CrossRef] [PubMed]
- Tong, V.T.; Dietz, P.M.; Rolle, I.V.; Kennedy, S.M.; Thomas, W.; England, L.J. Clinical interventions to reduce secondhand smoke exposure among pregnant women: A systematic review. Tob. Control 2015, 24, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, C.; Angus, K.; Cheeseman, H.; Semple, S. Reducing secondhand smoke exposure among nonsmoking pregnant women: A systematic review. Nicotine Tob. Res. 2020, 22, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Dherani, M.; Zehra, S.N.; Jackson, C.; Satyanaryana, V.; Huque, R.; Chandra, P.; Rahman, A.; Siddiqi, K. Behaviour change interventions to reduce second-hand smoke exposure at home in pregnant women—A systematic review and intervention appraisal. BMC Pregnancy Childbirth 2017, 17, 378. [Google Scholar] [CrossRef]
- Satyanarayana, V.A.; Jackson, C.; Siddiqi, K.; Chandra, P.S.; Huque, R.; Dherani, M.; Nasreen, S.; Murthy, P.; Rahman, A. A behaviour change intervention to reduce home exposure to second hand smoke during pregnancy in India and Bangladesh: A theory and evidence-based approach to development. Pilot Feasibility Stud. 2021, 7, 74. [Google Scholar] [CrossRef]
- Chi, Y.C.; Wu, C.L.; Chen, C.Y.; Lyu, S.Y.; Lo, F.E.; Morisky, D.E. Randomized trial of a secondhand smoke exposure reduction intervention among hospital-based pregnant women. Addict. Behav. 2015, 41, 117–123. [Google Scholar] [CrossRef]
- El-Mohandes, A.A.; Kiely, M.; Blake, S.M.; Gantz, M.G.; El-Khorazaty, M.N. An intervention to reduce environmental tobacco smoke exposure improves pregnancy outcomes. Pediatrics 2010, 125, 721–728. [Google Scholar] [CrossRef]
- Huang, C.M.; Wu, H.L.; Huang, S.H.; Chien, L.Y.; Guo, J.L. Transtheoretical model-based passive smoking prevention programme among pregnant women and mothers of young children. Eur. J. Public Health 2013, 23, 777–782. [Google Scholar] [CrossRef]
- Loke, A.Y.; Lam, T.H. A randomized controlled trial of the simple advice given by obstetricians in Guangzhou, China, to non-smoking pregnant women to help their husbands quit smoking. Patient Educ. Couns. 2005, 59, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Stanton, W.R.; Lowe, J.B.; Moffatt, J.; Del Mar, C.B. Randomised control trial of a smoking cessation intervention directed at men whose partners are pregnant. Prev. Med. 2004, 38, 6–9. [Google Scholar] [CrossRef]
- Kazemi, A.; Ehsanpour, S.; Nekoei-Zahraei, N.S. A randomized trial to promote health belief and to reduce environmental tobacco smoke exposure in pregnant women. Health Educ. Res. 2012, 27, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Strecher, V.J.; Rosenstock, I.M. The health belief model. In Cambridge Handbook of Psychology, Health and Medicine; Baum, A., Newman, S., Weinman, J., West, R., McManus, C., Eds.; Cambridge University Press: Cambridge, UK, 1997; pp. 113–117. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior: Theory, Research, and Practice, 5th ed.; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- World Health Organization. Recommendations for the Prevention and Management of Tobacco Use and Second-Hand Smoke Exposure in Pregnancy. Available online: https://www.who.int/publications/i/item/9789241506076 (accessed on 3 February 2023).
- Baucom, D.H.; Porter, L.S.; Kirby, J.S.; Hudepohl, J. Couple-based interventions for medical problems. Behav. Ther. 2012, 43, 61–76. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Pregnant? Don’t Smoke! Available online: https://www.cdc.gov/pregnancy/features/pregnantdontsmoke.html (accessed on 3 February 2023).
- National Health Services. Passive Smoking: Protect Your Family and Friends. Available online: https://www.nhs.uk/live-well/quit-smoking/passive-smoking-protect-your-family-and-friends/ (accessed on 3 February 2023).
- National Health Services. Stop Smoking in Pregnancy. Available online: https://www.nhs.uk/conditions/pregnancy-and-baby/smoking-pregnant/ (accessed on 3 February 2023).
- National Health Services. Secondhand (Passive) Smoke Harms Your Baby. Available online: https://www.nhs.uk/conditions/pregnancy-and-baby/smoking-pregnant/#secondhand-passive-smoke-harms-your-baby (accessed on 3 February 2023).
- Quit. Victoria. Secondhand Smoke and Your Family’s Health. Available online: https://www.quit.org.au/articles/secondhand-smoke-and-your-familys-health/ (accessed on 3 February 2023).
- ICanQuit.New South Wales Government. Smoking while Pregnant. Available online: https://www.icanquit.com.au/reasons-to-quit/smoking-and-your-family/smoking-when-pregnant (accessed on 3 February 2023).
- Moll, J.M. Doctor-patient communication in rheumatology: Studies of visual and verbal perception using educational booklets and other graphic material. Ann. Rheum. Dis. 1986, 45, 198–209. [Google Scholar] [CrossRef]
- Dworkin, M.S.; Peterson, C.E.; Gao, W.; Mayor, A.; Hunter, R.; Negron, E.; Fleury, A.; Besch, C.L. Efficacy of a food safety comic book on knowledge and self-reported behavior for persons living with AIDS. PLoS ONE. 2013, 8, e72874. [Google Scholar] [CrossRef]
- Febriani, S. Discourse on Indonesian Comics: Manifestation of National Identity in Comics Exhibition in Indonesia Circa 2005–2011. Ph.D. Thesis, Tohoku University, Sendai, Japan, 2016. [Google Scholar]
- Inaoka, K.; Octawijaya, I.H.; Wariki, W.M.V.; Ota, E. Preventing pregnant women’s exposure to secondhand smoke: Development and suitability assessment of an educational comic booklet. Health 2020, 12, 1186–1201. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Lukwago, S.N.; Bucholtz, R.D.; Clark, E.M.; Sanders-Thompson, V. Achieving cultural appropriateness in health promotion programs: Targeted and tailored approaches. Health Educ. Behav. 2003, 30, 133–146. [Google Scholar] [CrossRef]
- Doak, C.C.; Doak, L.G.; Root, J.H. Teaching Patients with Low Literact Skills. AJN Am. J. Nurs. 1996, 96, 16M. [Google Scholar] [CrossRef]
- World Health Organization Guidelines for Developing Behavioural Change Interventions in the Context of Avian Influenza. Available online: https://apps.who.int/iris/bitstream/handle/10665/205156/B3146.pdf?sequence=1&isAllowed=y (accessed on 3 February 2023).
- Lorencatto, F.; West, R.; Michie, S. Specifying evidence-based behavior change techniques to aid smoking cessation in pregnancy. Nicotine Tob. Res. 2012, 14, 1019–1026. [Google Scholar] [CrossRef]
- Michie, S.; Hyder, N.; Walia, A.; West, R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict. Behav. 2011, 36, 315–319. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Available online: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/anc-positive-pregnancy-experience/en/ (accessed on 3 February 2023).
- Rehan, V.K.; Sakurai, R.; Torday, J.S. Thirdhand smoke: A new dimension to the effects of cigarette smoke on the developing lung. Am. J. Physiol. Lung Cell Mol. Physiol. 2011, 301, L1–L8. [Google Scholar] [CrossRef]
- Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center (LA BioMed). ‘Thirdhand Smoke’ Poses Danger to Unborn Babies’ Lungs, Study Finds. Available online: https://www.sciencedaily.com/releases/2011/04/110419101231.htm (accessed on 18 November 2023).
- American Pregnancy Association. Second Hand Smoke and Pregnancy. Available online: https://americanpregnancy.org/healthy-pregnancy/pregnancy-health-wellness/second-hand-smoke-and-pregnancy/ (accessed on 18 November 2023).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Chi, Y.C.; Sha, F.; Yip, P.S.; Chen, J.L.; Chen, Y.Y. Randomized comparison of group versus individual educational interventions for pregnant women to reduce their secondhand smoke exposure. Medicine 2016, 95, e5072. [Google Scholar] [CrossRef]
- Martinelli, A.M. Development and validation of the avoidance of environmental tobacco smoke scale. J. Nurs. Meas. 1998, 6, 75–86. [Google Scholar] [CrossRef]
- Jerusalem, R.S.M. Measures in Health Psychology: A User’s Portfolio; NFER-NELSON: Windsor, UK, 1995. [Google Scholar]
- Schwarzer, R. Documentation of the General Self-Efficacy Scale. Available online: http://userpage.fu-berlin.de/%7Ehealth/faq_gse.pdf (accessed on 1 September 2018).
- Kwak, S.G.; Kim, J.H. Central limit theorem: The cornerstone of modern statistics. Korean J. Anesthesiol. 2017, 70, 144–156. [Google Scholar] [CrossRef]
- Lang, T.A.; Altman, D.G. Basic statistical reporting for articles published in biomedical journals: The “Statistical Analyses and Methods in the Published Literature” or the SAMPL Guidelines. Int. J. Nurs. Stud. 2015, 52, 5–9. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Japanese Ministry of Education & Culture, Sports, Science and Technology; Japanese Ministry of Health, Labor and Welfare. Ethical Guidelines for Medical and Health Research Involving Human Subjects. Available online: https://www.lifescience.mext.go.jp/files/pdf/n1443_01.pdf (accessed on 3 February 2023).
- Hochbaum, G.M. Public Participation in Medical Screening Programs; A Socio-Psychological Study; U.S. Departmentt. of Health, Education, and Welfare, Public Health Service, Bureau of State Services, Division of Special Health Services, Tuberculosis Program: Washington, DC, USA, 1958; pp. 7–8. [Google Scholar]
- Mayangsari, H.; Mahmood, M.A. Active smoking and exposure to passive smoking among pregnant women attending a primary health center in Temanggung, Indonesia. Indones. J. Public Health 2021, 16, 134–145. [Google Scholar] [CrossRef]
- Kaufman, M.R.; Merritt, A.P.; Rimbatmaja, R.; Cohen, J.E. ‘Excuse me, sir. Please don’t smoke here’. A qualitative study of social enforcement of smoke-free policies in Indonesia. Health Policy Plan. 2015, 30, 995–1002. [Google Scholar] [CrossRef]
- Nichter, M.; Nichter, M.; Padmawati, R.S.; Ng, N. Developing a smoke free household initiative: An Indonesian case study. Acta Obstet. Gynecol. Scand. 2010, 89, 578–581. [Google Scholar] [CrossRef]
- Trisnowati, H.; Kusuma, D.; Ahsan, A.; Kurniasih, D.E.; Padmawati, R.S. Smoke-free home initiative in Bantul, Indonesia: Development and preliminary evaluation. Tob. Prev. Cessat. 2019, 5, 40. [Google Scholar] [CrossRef]
- Sabogal, F.; Otero-Sabogal, R.; Pasick, R.J.; Jenkins, C.N.H.; Pérez-Stable, E.J. Printed health education materials for diverse communities: Suggestions learned from the field. Health Educ. Q. 1996, 23, 123–141. [Google Scholar] [CrossRef]
- Fisher, W.A.; Fisher, J.D.; Harman, J. The information-motivation-behavioral skills model: A general social psychological approach to understanding and promoting health behavior. In Social Psychological Foundations of Health and Illness; Suls, J., Wallston, K.A., Eds.; Blackwell Publishing: Malden, MA, USA, 2003; pp. 82–106. [Google Scholar]
- Chiu, H.T.; Isaac Wu, H.D.; Kuo, H.W. The relationship between self-reported tobacco exposure and cotinines in urine and blood for pregnant women. Sci. Total Environ. 2008, 406, 331–336. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | EG (n = 140) | CG (n = 146) | p-Value | ||
|---|---|---|---|---|---|
| n | Mean (SD) or (%) | n | Mean (SD) or (%) | ||
| Mean age | 135 | 27.01 (6.4) | 144 | 26.89 (6.1) | 0.87 a |
| Ethnicity Minahasan Sangir Mongondow Gorontalo Tinghoa Other | 77 24 4 16 1 15 | (55.0) (17.1) (2.9) (11.4) (0.7) (10.7) | 76 21 4 21 0 21 | (52.4) (14.5) (2.8) (14.5) (0.0) (14.5) | 0.86 c |
| Level of education Elementary school Junior high school Senior high school University/College | 8 25 85 19 | (5.8) (18.2) (62.0) (13.9) | 12 28 91 13 | (8.3) (19.4) (63.2) (9.0) | 0.55 b |
| Religion Protestant Catholic Muslim | 82 11 11 | (59.9) (8.0) (32.1) | 91 8 45 | (63.2) (5.6) (31.3) | 0.68 b |
| Occupation Housewife Working | 108 29 | (78.8) (21.2) | 114 30 | (78.6) (21.4) | 0.95 b |
| Workplace Indoor Outdoor Both | 75 13 46 | (56.0) (9.7) (34.3) | 83 12 47 | (58.5) (8.5) (33.1) | 0.89 b |
| Household earnings Over Rp.2,600,000/month Rp.2,600,000/month or less | 58 71 | (45.0) (55.0) | 66 72 | (47.8) (52.2) | 0.64 b |
| Type of household Nuclear family Joint family | 72 64 | (53.0) (47.1) | 70 71 | (49.3) (50.0) | 0.63 c |
| Married | 125 | (91.9) | 133 | (92.4) | 0.89 b |
| Mean number of gestational weeks | 130 | 15.13 (6.7) | 141 | 15.45 (6.0) | 0.68 a |
| Number of pregnancies 1 2 3, 4 or more | 43 43 33 18 | (31.4) (31.4) (24.1) (13.1) | 38 61 30 15 | (26.4) (42.4) (21.0) (10.4) | 0.30 b |
| Number of births 0 1 2 3 4 or more | 11 46 36 18 12 | (8.9) (37.4) (29.3) (14.6) (9.8) | 10 53 40 20 11 | (7.5) (39.6) (29.9) (14.9) (8.2) | 0.98 b |
| Number of children 0 1 2 3 4 or more | 20 53 34 13 7 | (15.7) (41.7) (26.8) (10.2) (5.5) | 26 58 36 9 6 | (19.3) (43.0) (26.7) (6.7) (4.4) | 0.80 b |
| Smoking status Never smoked Quit before pregnancy Quit after pregnancy | 117 6 8 | (89.3) (4.5) (6.1) | 125 5 10 | (89.3) (3.6) (7.1) | 0.87 b |
| SHS Daily Weekly Monthly Less than monthly | 106 15 1 12 | (79.1) (11.2) (0.7) (9.0) | 100 20 1 17 | (71.4) (14.3) (0.7) (12.1) | 0.51 c |
| Smoke-free home Yes No | 46 88 | (34.3) (65.7) | 47 95 | (32.9) (66.4) | 0.95 c |
| Characteristic | EG (n = 140) | CG (n = 146) | p-Value | ||
|---|---|---|---|---|---|
| n | Mean (SD) or (%) | n | Mean (SD) or (%) | ||
| Mean age | 134 | 30.03(6.9) | 143 | 30.22 (6.5) | 0.81 a |
| Ethnicity Minahasan Sangir Mongondow Gorontalo Tinghoa Other | 78 14 7 21 2 15 | (55.7) (10.0) (5.0) (15.0) (1.4) (10.7) | 78 16 3 19 0 26 | (53.4) (11.0) (2.1) (13.0) (0.0) (17.8) | 0.37 b |
| Level of education Elementary school Junior high school Senior high school University/College | 17 30 74 15 | (12.1) (21.4) (52.9) (10.7) | 14 20 99 11 | (9.6) (13.7) (67.8) (7.5) | 0.13 b |
| Religion Protestant Catholic Muslim | 77 13 47 | (55.4) (9.4) (33.8) | 89 11 44 | (61.0) (7.5) (30.1) | 0.84 b |
| Occupation Private Entrepreneur Labourer Government Farmer Other | 42 35 29 4 3 23 | (30.0) (25.0) (20.7) (2.9) (2.1) (16.4) | 49 22 29 3 8 33 | (33.6) (15.1) (19.9) (2.1) (5.5) (22.6) | 0.22 b |
| Number of cigarettes smoked/day | 131 | 10.20(6.3) | 138 | 10.75 (7.5) | 0.52 a |
| Smoking status As usual Less after pregnancy More after pregnancy | 100 30 1 | (76.3) (22.9) (0.7) | 109 28 3 | (77.9) (20.0) (2.1) | 0.64 b |
| Smoking in home Daily Weekly Monthly Less than Monthly | 116 11 0 8 | (84.7) (8.0) (0.0) (5.8) | 115 20 1 6 | (81.0) (14.1) (0.7) (4.2) | 0.18 b |
| Domains (Number of Items) | Baseline | Three Months Post-Intervention | |
|---|---|---|---|
| Primary outcomes | |||
| Pregnant women | Avoidance of environmental tobacco smoke: self-evaluation (19) | 0.69 | 0.78 |
| Pregnant women’s behaviour change: peer-evaluation (3) | 0.88 | 0.83 | |
| Male partners | Male partner’s smoking behaviour: self-evaluation (8) | 0.78 | 0.70 |
| Male partner’s smoking behaviour: peer-evaluation (8) | 0.69 | 0.70 | |
| Secondary outcomes | |||
| Pregnant women | Knowledge of SHS C (8) | 0.70 | 0.71 |
| Perceived SHS-related disease susceptibility D (2) | 0.83 | 0.83 | |
| Perceived SHS-related disease severity E (2) | 0.94 | 0.93 | |
| Perceived benefits F (4) | 0.92 | 0.86 | |
| Barriers to preventing SHS exposure G (4) | 0.67 | 0.71 | |
| Cue to action for preventing SHS exposure H (6) | 0.86 | 0.88 | |
| Self-efficacy I (10) | 0.92 | 0.91 | |
| Male partners | Knowledge of SHS C (8) | 0.73 | 0.82 |
| Perceived SHS-related disease susceptibility D (2) | 0.87 | 0.81 | |
| Perceived SHS-related disease severity E (2) | 0.90 | 0.92 | |
| Perceived benefits F (4) | 0.91 | 0.87 | |
| Barriers to preventing SHS exposure G (5) | 0.72 | 0.68 | |
| Cue to action for preventing SHS exposure H (8) | 0.82 | 0.86 | |
| Self-efficacy I (10) | 0.90 | 0.88 |
| Experimental Group | Control Group | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Baseline] | n | Mean (SD) | n | Mean (SD) | ||||
| Avoidance of environmental tobacco smoke (self-evaluation) | 140 | 50.96 (6.29) | 146 | 51.09 (6.09) | −0.13 | −0.02 | 0.87 a | −0.25, 0.21 |
| Pregnant women’s behaviour (peer-evaluation) | 140 | 9.09 (1.97) | 146 | 9.10 (1.89) | −0.01 | −0.01 | 0.95 a | −0.24, 0.23 |
| [At three months post-intervention] | ||||||||
| Avoidance of environmental tobacco smoke (self-evaluation) | 109 | 52.17 (5.20) | 103 | 51.38 (7.25) | 0.79 | 0.13 | 0.37 b | −0.15, 0.40 |
| Pregnant women’s behaviour (peer-evaluation) | 110 | 9.36 (1.45) | 104 | 9.06 (1.60) | 0.30 | 0.20 | 0.15 a | −0.07, 0.47 |
| Baseline | Three Month Post-Intervention | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Experimental Group] | n | Mean (SD) | n | Mean (SD) | ||||
| Avoidance of environmental tobacco smoke (self-evaluation) | 140 | 50.96 (6.29) | 140 | 52.22 (5.42) | −1.26 | −0.17 | 0.06 a | −0.34, −0.00 |
| Pregnant women’s behaviour(peer-evaluation) | 140 | 9.09 (1.97) | 140 | 9.35 (1.50) | −0.26 | −0.11 | 0.22 a | −0.27, 0.06 |
| [Control group] | ||||||||
| Avoidance of environmental tobacco smoke (self-evaluation) | 146 | 51.09 (6.09) | 146 | 51.75 (7.11) | −0.66 | −0.01 | 0.37 a | −0.26, 0.07 |
| Pregnant women’s behaviour (peer-evaluation) | 146 | 9.10 (1.90) | 146 | 9.09 (1.55) | 0.01 | 0.01 | 0.94 a | −0.16, 0.17 |
| Experimental Group | Control Group | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Baseline] | n | Mean (SD) | n | Mean (SD) | ||||
| Smoking behaviour (self-evaluation) | 140 | 19.36 (4.49) | 146 | 18.51 (4.19) | 0.84 | 0.19 | 0.10 a | −0.04, 0.43 |
| Male partner’s smoking behaviour (peer-evaluation) | 140 | 19.03 (3.96) | 146 | 18.20 (3.97) | 0.83 | 0.21 | 0.08 a | −0.02, 0.44 |
| [At three months post-intervention] | ||||||||
| Smoking behaviour (self-evaluation) | 110 | 20.69 (4.25) | 104 | 19.20 (4.18) | 1.49 | 0.35 | 0.01 a | 0.08, 0.62 |
| Male partner’s smoking behaviour (peer-evaluation) | 109 | 20.11 (4.71) | 103 | 18.23 (3.96) | 1.88 | 0.43 | ≤0.01 a | 0.16, 0.70 |
| Baseline | Three Months Post-Intervention | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Experimental group] | n | Mean (SD) | n | Mean (SD) | ||||
| Smoking behaviour (self-evaluation) | 140 | 19.36 (4.49) | 140 | 20.51 (4.35) | −1.15 | −0.21 | 0.01 a | −0.38, −0.05 |
| Male partner’s smoking behaviour (peer-evaluation) | 140 | 19.03 (3.96) | 140 | 20.01 (4.86) | −0.98 | −0.17 | 0.07 a | −0.34, −0.01 |
| [Control group] | ||||||||
| Smoking behaviour (self-evaluation) | 146 | 18.51 (4.20) | 146 | 19.44 (4.15) | −0.93 | −0.19 | 0.05 a | −0.35, −0.02 |
| Male partner’s smoking behaviour (peer-evaluation) | 146 | 18.20 (3.97) | 146 | 18.51 (4.36) | −0.31 | −0.01 | 0.56 a | −0.22, 0.11 |
| Experimental Group | Control Group | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Baseline] | n | Mean (SD) | n | Mean (SD) | ||||
| Knowledge of SHS C | 140 | 15.64 (0.88) | 146 | 15.55 (1.04) | 0.09 | 0.09 | 0.44 a | −14, 0.32 |
| Perceived SHS-related disease susceptibility D | 140 | 6.60 (1.13) | 146 | 6.57 (1.17) | 0.03 | 0.03 | 0.82 a | −0.20, 0.26 |
| Perceived SHS-related disease severity E | 140 | 6.68 (1.10) | 146 | 6.32 (1.21) | 0.36 | 0.31 | 0.01 a | 0.07, 0.54 |
| Perceived benefits F | 140 | 12.76 (2.64) | 146 | 12.24 (2.39) | 0.52 | 0.21 | 0.08 b | −0.03, 0.44 |
| Barriers to preventing SHS exposure G | 140 | 9.51 (2.12) | 146 | 9.86 (2.07) | −0.35 | −0.17 | 0.16 a | −0.40, 0.07 |
| Cue to action for preventing SHS exposure H | 140 | 15.83 (4.51) | 146 | 15.57 (4.71) | 0.27 | 0.06 | 0.63 a | −0.17, 0.29 |
| Self-efficacy I | 140 | 31.49 (4.19) | 146 | 30.92 (5.33) | 0.57 | 0.12 | 0.32 a | −0.11, 0.35 |
| [At three months post-intervention] | ||||||||
| Knowledge of SHS C | 109 | 15.72 (0.93) | 103 | 15.84 (0.47) | −0.12 | −0.16 | 0.25 b | −0.43, 0.11 |
| Perceived SHS-related disease susceptibility D | 109 | 6.38 (1.05) | 103 | 6.39 (1.01) | −0.02 | −0.02 | 0.90 a | −0.29, 0.25 |
| Perceived SHS-related disease severity E | 109 | 6.41 (1.02) | 103 | 6.44 (1.06) | −0.03 | −0.03 | 0.85 b | −0.30, 0.24 |
| Perceived benefits F | 109 | 12.37 (1.89) | 103 | 12.44 (1.90) | −0.06 | −0.03 | 0.81 a | −0.30, 0.24 |
| Barriers to preventing SHS exposure G | 109 | 10.31 (2.21) | 103 | 10.22 (2.07) | 0.09 | 0.04 | 0.76 a | −0.23, 0.31 |
| Cue to action for preventing SHS exposure H | 109 | 17.64 (3.72) | 103 | 16.75 (4.08) | 0.90 | 0.23 | 0.10 a | −0.04, 0.50 |
| Self-efficacy I | 109 | 31.47 (4.19) | 103 | 31.23 (4.26) | 0.24 | 0.06 | 0.69 a | −0.21, 0.33 |
| Baseline | Three Months Post-Intervention | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Experimental Group] | n | Mean (SD) | n | Mean (SD) | ||||
| Knowledge of SHS C | 140 | 15.64 (0.88) | 140 | 15.73 (0.89) | −0.09 | 0.09 | 0.31 a | −25, 0.08 |
| Perceived SHS-related disease susceptibility D | 140 | 6.60 (1.13) | 140 | 6.40 (1.09) | 0.02 | 0.15 | 0.14 a | −0.01, 0.32 |
| Perceived SHS-related disease severity E | 140 | 6.68 (1.10) | 140 | 6.44 (1.07) | 0.24 | 0.17 | 0.07 a | 0.00, 0.34 |
| Perceived benefits F | 140 | 12.76 (2.61) | 140 | 12.34 (1.99) | 0.42 | 0.15 | 0.11 a | −0.02, 0.31 |
| Barriers to preventing SHS exposure G | 140 | 9.51 (2.12) | 140 | 10.18 (2.16) | −0.67 | −0.21 | 0.01 a | −0.38, −0.05 |
| Cue to action for preventing SHS exposure H | 140 | 15.78 (4.66) | 140 | 17.38 (4.15) | −1.60 | −0.33 | ≤0.01 a | −0.49, −0.15 |
| Self-efficacy I | 140 | 31.49 (4.19) | 140 | 31.44 (4.37) | 0.05 | 0.01 | 0.93 a | −0.16, −0.18 |
| [Control group] | ||||||||
| Knowledge of SHS C | 146 | 15.55 (1.04) | 146 | 15.84 (0.62) | −0.29 | −0.26 | ≤0.01 a | −0.43, −0.10 |
| Perceived SHS-related disease susceptibility D | 146 | 6.57 (1.17) | 146 | 6.43 (1.06) | 0.14 | 0.09 | 0.31 a | −0.07, 0.25 |
| Perceived SHS-related disease severity E | 146 | 6.32 (1.21) | 146 | 6.49 (1.10) | −0.17 | −0.10 | 0.27 a | −0.27, 0.06 |
| Perceived benefits F | 146 | 12.23 (2.40) | 146 | 12.45 (2.02) | −0.22 | −0.07 | 0.38 a | −0.24, 0.09 |
| Barriers to preventing SHS exposure G | 146 | 9.86 (2.04) | 146 | 10.23 (2.15) | −0.37 | −0.14 | 0.13 a | −0.30, 0.03 |
| Cue to action for preventing SHS exposure H | 146 | 15.58 (4.69) | 146 | 16.85 (4.30) | −1.27 | −0.25 | 0.01 a | −0.42, −0.09 |
| Self-efficacy I | 146 | 30.92 (5.33) | 146 | 31.33 (4.39) | −0.41 | −0.06 | 0.49 a | −0.23, 0.10 |
| Experimental Group | Control Group | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Baseline] | n | Mean (SD) | n | Mean (SD) | ||||
| Knowledge of SHS C | 140 | 17.49 (1.11) | 146 | 17.33 (1.39) | 0.16 | 0.12 | 0.29 a | −0.11, 0.36 |
| Perceived SHS related disease susceptibility D | 140 | 6.40 (1.20) | 146 | 6.26 (1.31) | 0.14 | 0.11 | 0.35 a | −0.12, 0.34 |
| Perceived SHS-related disease severity E | 140 | 6.31 (1.06) | 146 | 6.34 (1.14) | −0.02 | −0.02 | 0.86 a | −0.25, 0.21 |
| Perceived benefits F | 140 | 12.36 (2.39) | 146 | 12.14 (2.44) | 0.22 | 0.09 | 0.44 a | −0.14, 0.32 |
| Barriers of preventing SHS exposure G | 140 | 11.54 (2.33) | 146 | 12.13 (2.59) | −0.59 | −0.24 | 0.04 a | −0.47, −0.01 |
| Cue to action for preventing SHS exposure H | 140 | 19.21 (5.61) | 146 | 18.62 (5.14) | 0.60 | 0.11 | 0.35 a | −0.12, 0.34 |
| Self-efficacy I | 140 | 31.36 (3.80) | 146 | 31.18 (4.89) | 0.18 | 0.04 | 0.73 b | −0.19, 0.27 |
| [At three months post-intervention] | ||||||||
| Knowledge of SHS C | 110 | 17.68 (0.96) | 104 | 17.66 (1.13) | 0.03 | 0.02 | 0.86 a | −0.24, 0.29 |
| Perceived SHS related disease susceptibility D | 110 | 6.37 (0.87) | 104 | 6.27 (0.87) | 0.10 | 0.12 | 0.38 a | −0.15, 0.39 |
| Perceived SHS-related disease severity E | 110 | 6.54 (1.02) | 104 | 6.32 (0.88) | 0.22 | 0.23 | 0.09 b | −0.04, 0.50 |
| Perceived benefits F | 110 | 12.11 (2.43) | 104 | 12.13 (1.71) | −0.03 | −0.01 | 0.93 b | −0.28, 0.26 |
| Barriers of preventing SHS exposure G | 110 | 12.74 (2.67) | 104 | 12.88 (1.89) | −0.15 | −0.06 | 0.64 b | −0.33, 0.20 |
| Cue to action for preventing SHS exposure H | 110 | 21.70 (5.03) | 104 | 19.84 (5.25) | 1.86 | 0.36 | 0.01 a | 0.09, 0.63 |
| Self-efficacy I | 110 | 31.49 (3.76) | 104 | 31.48 (3.77) | 0.01 | 0.00 | 0.98 a | −0.26, 0.27 |
| Baseline | Three Months Post-Intervention | MD | Cohen’s d | p-Value | 95%CI | |||
|---|---|---|---|---|---|---|---|---|
| [Experimental Group] | n | Mean (SD) | n | Mean (SD) | ||||
| Knowledge of SHS C | 140 | 17.49 (1.11) | 140 | 17.68 (1.03) | −0.19 | −0.13 | 0.15 a | −0.30, 0.04 |
| Perceived SHS related disease susceptibility D | 140 | 6.40 (1.20) | 140 | 6.36 (0.87) | 0.04 | 0.03 | 0.74 a | −0.13, 0.20 |
| Perceived SHS-related disease severity E | 140 | 6.31 (1.06) | 140 | 6.50 (1.01) | −0.19 | −0.11 | 0.15 a | −0.28, 0.06 |
| Perceived benefits F | 140 | 12.36 (2.39) | 140 | 12.20 (2.43) | 0.16 | 0.05 | 0.61 a | −0.12, 0.21 |
| Barriers of preventing SHS exposure G | 140 | 11.54 (2.33) | 140 | 12.66 (2.62) | −1.12 | −0.34 | ≤0.01 a | −0.51, −0.17 |
| Cue to action for preventing SHS exposure H | 140 | 19.21 (5.61) | 140 | 21.34 (5.23) | −2.13 | −0.36 | ≤0.01 a | −0.53, −0.19 |
| Self-efficacy I | 140 | 31.36 (3.80) | 140 | 31.53 (3.89) | −0.17 | −0.03 | 0.72 a | −0.20, 0.13 |
| [Control group] | ||||||||
| Knowledge of SHS C | 146 | 17.33 (1.40) | 146 | 17.67 (1.12) | −0.34 | −0.18 | 0.04 a | −0.35, −0.02 |
| Perceived SHS related disease susceptibility D | 146 | 6.26 (1.31) | 146 | 6.27 (0.88) | −0.01 | 0.00 | 0.96 a | −0.17, 0.16 |
| Perceived SHS-related disease severity E | 146 | 6.34 (1.14) | 146 | 6.31 (0.92) | 0.03 | 0.02 | 0.84 a | −0.14, 0.18 |
| Perceived benefits F | 146 | 12.15 (2.42) | 146 | 12.04 (1.93) | 0.11 | 0.03 | 0.70 a | −0.13, 0.20 |
| Barriers of preventing SHS exposure G | 146 | 12.14 (2.59) | 146 | 12.86 (2.10) | −0.72 | −0.23 | 0.01 a | −0.40, −0.07 |
| Cue to action for preventing SHS exposure H | 146 | 18.61 (5.14) | 146 | 19.97 (5.04) | −1.36 | −0.22 | 0.01 a | −0.39, −0.06 |
| Self-efficacy I | 146 | 31.24 (4.84) | 146 | 31.39 (3.85) | −0.15 | −0.03 | 0.80 a | −0.19, 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inaoka, K.; Octawijaya, I.H.; Mamahit, C.G.; Karundeng, J.F.; Wariki, W.M.V.; Ota, E. Effects of a Comic Booklet Intervention Aimed at Preventing Second-Hand Smoke Exposure for Pregnant Women in Indonesia: A Randomised Controlled Trial. Healthcare 2023, 11, 3061. https://doi.org/10.3390/healthcare11233061
Inaoka K, Octawijaya IH, Mamahit CG, Karundeng JF, Wariki WMV, Ota E. Effects of a Comic Booklet Intervention Aimed at Preventing Second-Hand Smoke Exposure for Pregnant Women in Indonesia: A Randomised Controlled Trial. Healthcare. 2023; 11(23):3061. https://doi.org/10.3390/healthcare11233061
Chicago/Turabian StyleInaoka, Kimiko, Ishak Halim Octawijaya, Citra Gabriella Mamahit, Jeand’arc Florentia Karundeng, Windy Mariane Virenia Wariki, and Erika Ota. 2023. "Effects of a Comic Booklet Intervention Aimed at Preventing Second-Hand Smoke Exposure for Pregnant Women in Indonesia: A Randomised Controlled Trial" Healthcare 11, no. 23: 3061. https://doi.org/10.3390/healthcare11233061
APA StyleInaoka, K., Octawijaya, I. H., Mamahit, C. G., Karundeng, J. F., Wariki, W. M. V., & Ota, E. (2023). Effects of a Comic Booklet Intervention Aimed at Preventing Second-Hand Smoke Exposure for Pregnant Women in Indonesia: A Randomised Controlled Trial. Healthcare, 11(23), 3061. https://doi.org/10.3390/healthcare11233061