
Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Data Collection
2.4. Study Aims
2.5. Statistical Analyses
3. Results
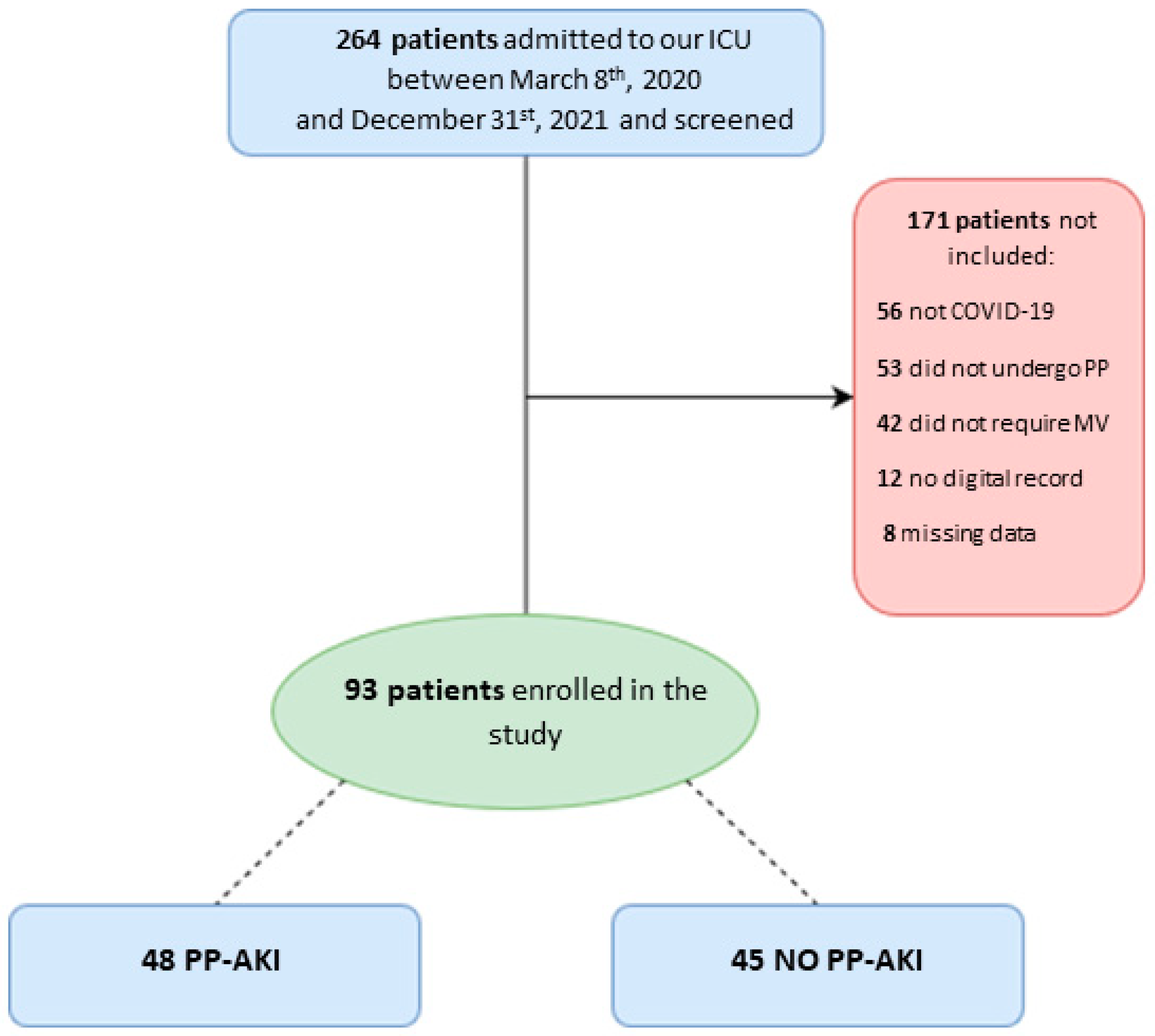
3.1. Population
3.2. Incidence and Characteristics of PP-Associated AKI
3.3. Differences between the AKI and Non-AKI Populations
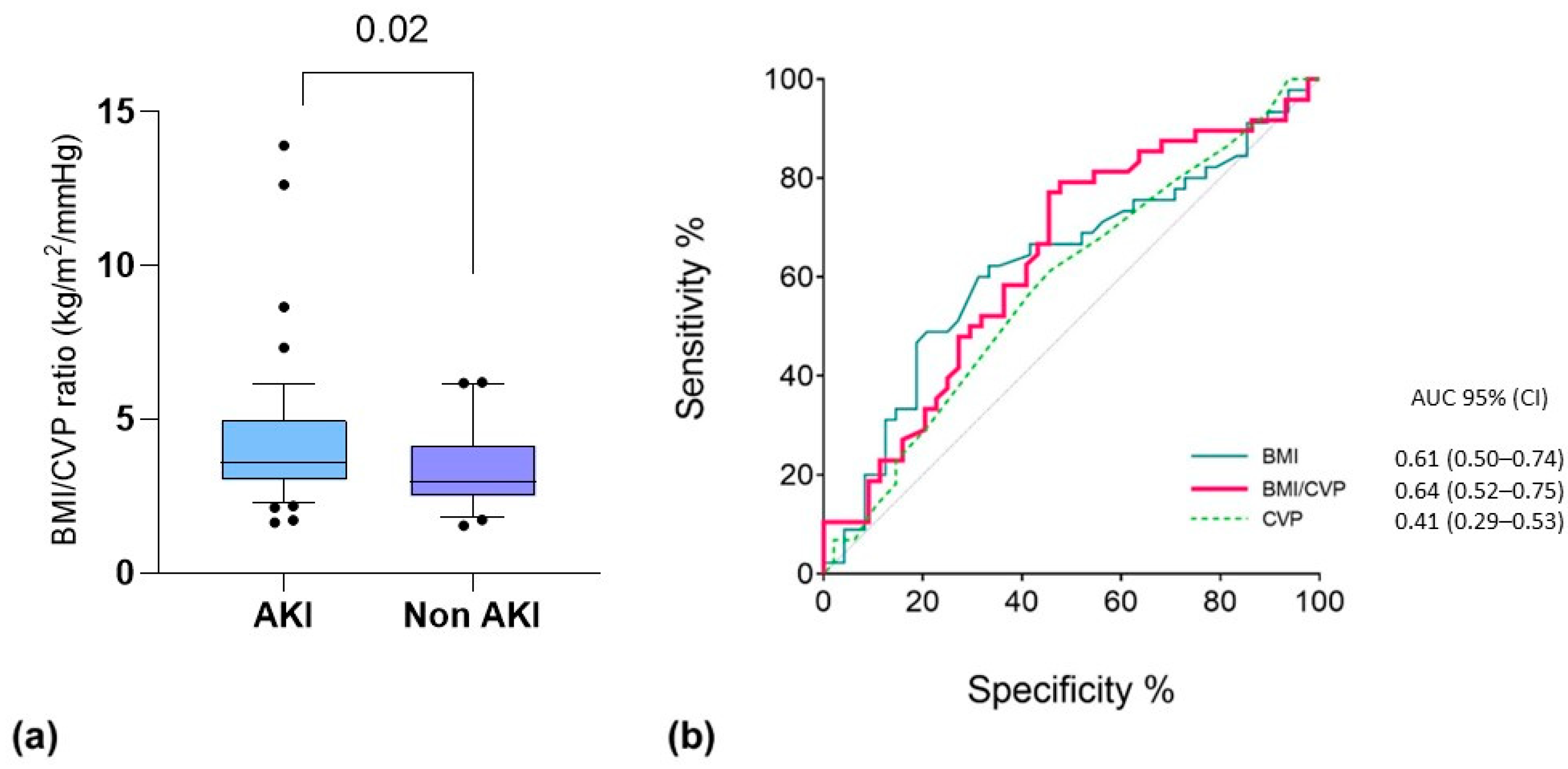
3.4. Determinants of PP-AKI
3.5. Predictors with Mortality and VFDs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostermann, M.; Lumlertgul, N.; Forni, L.G.; Hoste, E. What every Intensivist should know about COVID-19 associated acute kidney injury. J. Crit. Care 2020, 60, 91–95. [Google Scholar] [CrossRef]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Zanella, A.; Florio, G.; Antonelli, M.; Bellani, G.; Berselli, A.; Bove, T.; Cabrini, L.; Carlesso, E.; Castelli, G.P.; Cecconi, M.; et al. Time course of risk factors associated with mortality of 1260 critically ill patients with COVID-19 admitted to 24 Italian intensive care units. Intensive Care Med. 2021, 47, 995–1008. [Google Scholar] [CrossRef]
- Lumlertgul, N.; Pirondini, L.; Cooney, E.; Kok, W.; Gregson, J.; Camporota, L.; Lane, K.; Leach, R.; Ostermann, M. Acute kidney injury prevalence, progression and long-term outcomes in critically ill patients with COVID-19: A cohort study. Ann. Intensiv. Care 2021, 11, 123. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, J.; Feng, H.; Wan, F.; Zhang, Y.; Tan, L. Prone positioning in intubated and mechanically ventilated patients with SARS-CoV-2. J. Clin. Anesthesia 2021, 71, 110258. [Google Scholar] [CrossRef]
- Gleissman, H.; Forsgren, A.; Andersson, E.; Lindqvist, E.; Falck, A.L.; Cronhjort, M.; Dahlberg, M.; Günther, M. Prone positioning in mechanically ventilated patients with severe acute respiratory distress syndrome and coronavirus disease 2019. Acta Anaesthesiol. Scand. 2020, 65, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, L.; Castaldo, N.; Fantin, A.; Deana, C.; Cortegiani, A.; Longhini, F.; Forfori, F.; Cammarota, G.; Grieco, D.L.; Isola, M.; et al. Ventilatory associated barotrauma in COVID-19 patients: A multicenter observational case control study (COVI-MIX-study). Pulmonology 2022, 29, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Scaramuzzo, G.; Karbing, D.S.; Fogagnolo, A.; Mauri, T.; Spinelli, E.; Mari, M.; Turrini, C.; Montanaro, F.; Volta, C.A.; Rees, S.E.; et al. Heterogeneity of Ventilation/Perfusion Mismatch at Different Levels of PEEP and in Respiratory Mechanics Phenotypes of COVID-19 ARDS. Respir. Care 2022, 68, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Albert, R.K.; Beitler, J.; Gattinoni, L.; Jaber, S.; Marini, J.J.; Munshi, L.; Papazian, L.; Pesenti, A.; Vieillard-Baron, A.; et al. Prone position in ARDS patients: Why, when, how and for whom. Intensiv. Care Med. 2020, 46, 2385–2396. [Google Scholar] [CrossRef]
- Scholten, E.L.; Beitler, J.R.; Prisk, G.K.; Malhotra, A. Treatment of ARDS With Prone Positioning. Chest 2017, 151, 215–224. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Taccone, P.; Pesenti, A.; Latini, R.; Polli, F.; Vagginelli, F.; Mietto, C.; Caspani, L.; Raimondi, F.; Bordone, G.; Iapichino, G.; et al. Prone Positioning in Patients with Moderate and Severe Acute Respiratory Distress Syndrome: A Randomized Controlled Trial. JAMA 2009, 302, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Cour, M.; Bussy, D.; Stevic, N.; Argaud, L.; Guérin, C. Differential effects of prone position in COVID-19-related ARDS in low and high recruiters. Intensiv. Care Med. 2021, 47, 1044–1046. [Google Scholar] [CrossRef]
- Jozwiak, M.; Teboul, J.-L.; Anguel, N.; Persichini, R.; Silva, S.; Chemla, D.; Richard, C.; Monnet, X. Beneficial Hemodynamic Effects of Prone Positioning in Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2013, 188, 1428–1433. [Google Scholar] [CrossRef]
- Hering, R.; Wrigge, H.; Vorwerk, R.; Brensing, K.A.; Schröder, S.; Zinserling, J.; Hoeft, A.; Spiegel, T.V.; Putensen, C. The Effects of Prone Positioning on Intraabdominal Pressure and Cardiovascular and Renal Function in Patients with Acute Lung Injury. Obstet. Anesthesia Dig. 2001, 92, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Danziger, J.M.; Chen, K.P.; Lee, J.; Feng, M.; Mark, R.G.; Celi, L.A.; Mukamal, K.J. Obesity, Acute Kidney Injury, and Mortality in Critical Illness. Crit. Care Med. 2016, 44, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.J.D.; McAuley, D.F.; Perkins, G.D.; Barrett, N.; Blackwood, B.; Boyle, A.; Chee, N.; Connolly, B.; Dark, P.; Finney, S.; et al. Guidelines on the management of acute respiratory distress syndrome. BMJ Open Respir. Res. 2019, 6, e000420. [Google Scholar] [CrossRef]
- BMJ Open. EPIdemiology of Surgery-Associated Acute Kidney Injury (EPIS-AKI): Study Protocol for a Multicentre, Observational Trial. Available online: https://bmjopen.bmj.com/content/11/12/e055705 (accessed on 16 February 2023).
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar] [CrossRef]
- Waikar, S.S.; Bonventre, J.V. Creatinine Kinetics and the Definition of Acute Kidney Injury. J. Am. Soc. Nephrol. 2009, 20, 672–679. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; on behalf of the KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar] [PubMed]
- Kirkpatrick, A.W.; Pelosi, P.; De Waele, J.J.; Malbrain, M.L.; Ball, C.G.; Meade, M.O.; Stelfox, H.T.; Laupland, K.B. Clinical review: Intra-abdominal hypertension: Does it influence the physiology of prone ventilation? Crit. Care 2010, 14, 232. [Google Scholar] [CrossRef]
- Sun, J.; Sun, H.; Sun, Z.; Yang, X.; Zhou, S.; Wei, J. Intra-abdominal hypertension and increased acute kidney injury risk: A systematic review and meta-analysis. J. Int. Med Res. 2021, 49, 3000605211016627. [Google Scholar] [CrossRef]
- Magder, S. Understanding central venous pressure: Not a Preload Index? Curr. Opin. Crit. Care 2015, 21, 369–375. [Google Scholar] [CrossRef]
- Hamzaoui, O.; Teboul, J.-L. Central venous pressure (CVP). Intensiv. Care Med. 2022, 48, 1498–1500. [Google Scholar] [CrossRef]
- Chen, X.; Wang, X.; Honore, P.M.; Spapen, H.D.; Liu, D. Renal failure in critically ill patients, beware of applying (central venous) pressure on the kidney. Ann. Intensiv. Care 2018, 8, 91. [Google Scholar] [CrossRef]
- Li, D.-K.; Wang, X.-T.; Liu, D.-W. Association between elevated central venous pressure and outcomes in critically ill patients. Ann. Intensiv. Care 2017, 7, 83. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Zhou, Y.; Wang, P.; Qi, E.-Y.; Gu, W.-J. Elevated central venous pressure is associated with increased mortality and acute kidney injury in critically ill patients: A meta-analysis. Crit. Care 2020, 24, 80. [Google Scholar] [CrossRef]
- De Backer, D.; Aissaoui, N.; Cecconi, M.; Chew, M.S.; Denault, A.; Hajjar, L.; Hernandez, G.; Messina, A.; Myatra, S.N.; Ostermann, M.; et al. How can assessing hemodynamics help to assess volume status? Intensiv. Care Med. 2022, 48, 1482–1494. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network; Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; Deboisblanc, B.; Connors, A.F.J.; Hite, R.D.; Harabin, A.L. Comparison of Two Fluid-Management Strategies in Acute Lung Injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.; de Grooth, H.-J.; Paulus, F.; van der Ven, F.L.; Neto, A.S.; Schultz, M.J.; Tuinman, P.R.; van Akkeren, J.P.; Algera, A.G.; Algoe, C.K.; et al. Association between early cumulative fluid balance and successful liberation from invasive ventilation in COVID-19 ARDS patients—Insights from the PRoVENT-COVID study: A national, multicenter, observational cohort analysis. Crit. Care 2022, 26, 157. [Google Scholar] [CrossRef]
- De Keulenaer, B.L.; De Waele, J.J.; Powell, B.; Malbrain, M.L.N.G. What is normal intra-abdominal pressure and how is it affected by positioning, body mass and positive end-expiratory pressure? Intensiv. Care Med. 2009, 35, 969–976. [Google Scholar] [CrossRef]
- Jacobs, R.; Wise, R.D.; Myatchin, I.; Vanhonacker, D.; Minini, A.; Mekeirele, M.; Kirkpatrick, A.W.; Pereira, B.M.; Sugrue, M.; De Keulenaer, B.; et al. Fluid Management, Intra-Abdominal Hypertension and the Abdominal Compartment Syndrome: A Narrative Review. Life 2022, 12, 1390. [Google Scholar] [CrossRef] [PubMed]
- Wintjens, M.S.J.N.; van Rosmalen, F.; Hemmelder, M.H.; Hulsewe-Evers, H.P.M.G.; Kusters, Y.H.A.M.; Ubben, J.F.H.; van Renswouw, D.A.M.; Gilissen, K.M.H.; van der Horst, I.C.C.; van Mook, W.N.K.A.; et al. Prone positioning is followed by a transient decrease in glomerular filtration rate: The prospective Maastricht Intensive Care COVID cohort. J. Nephrol. 2023, 1–3. [Google Scholar] [CrossRef]
- Scaramuzzo, G.; Gamberini, L.; Tonetti, T.; Zani, G.; Ottaviani, I.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Reggiani, M.L.B.; Bertellini, E.; et al. Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: A cohort study. Ann. Intensiv. Care 2021, 11, 63. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age (years) | 67 [59–72.5] |
| Males (%) | 75/93 (81%) |
| Arterial hypertension (%) | 48/93 (52%) |
| Ischemic heart disease (%) | 7/93 (7%) |
| Asthma (%) | 8/93 (8%) |
| COPD (%) | 2/93 (2%) |
| Diabetes (%) | 14/93 (15%) |
| Previous use of diuretics (%) | 5/93 (5%) |
| Chronic kidney disease (%) | 4/93 (4%) |
| BMI (kg/cm2) | 29.4 [26.5–33.62] |
| Creatinine at ICU admission (mg/dL) | 0.89 [0.71–1.14] |
| Systolic arterial pressure (mmHg) * | 130 [120–150] |
| Diastolic arterial pressure (mmHg) * | 75 [60–80] |
| Heart rate (beats/min) * | 80 [70–90] |
| PaO2/FiO2 * | 105 [79–133] |
| Arterial lactate * (mmol/L) | 1.2 [0.9–1.5] |
| Hemoglobin (g/dL) * | 13.6 [12.4–14.45] |
| Number of PP Cycles | 2 [1–3] |
| Highest creatinine during ICU stay | 1.47 [0.965–3.19] |
| Ventilator-free days (days) | 0 [0–12] |
| ICU mortality | 54/93 (58%) |
| Hospital days before ICU (days) | 2 [1–4] |
| Days of ICU before first prone positioning | 4 [1–7] |
| Variable | |
|---|---|
| Patients developing AKI after PP | 48/93 (52%) |
| AKI diagnosed using Urine Output | 24/48 (50%) |
| AKI diagnosed using Creatinine | 10/48 (21%) |
| AKI diagnosed using both | 14/48 (29%) |
| KDIGO class 1 | 29/48 (60%) |
| KDIGO class 2 | 12/48 (25%) |
| KDIGO class 3 | 7/48 (15%) |
| Time from PP start to diagnosis (hours) | 24 [13.5–44.5] |
| Furosemide infusion before PP (yes) | 27/48 (56%) |
| Variable | No AKI (45) | AKI (48) | Total (93) |
|---|---|---|---|
| Age (years) | 68 [61–74] | 66.5 [58.5–72] | 67 [59–72] |
| BMI (kg/m2) | 27.7 [25.7–32.1] | 30.4 [27.7–33.8] | 29.4 [26.6–33.6] |
| Creatinine (mg/dL) | 0.85 [0.72–1.02] | 0.91 [0.705–1.2] | 0.89 [0.71–1.14] |
| Arterial pressure, diastolic (mmHg) | 70 [60–80] | 80 [70–82.5] | 75 [60–80] |
| Heart rate (bpm) | 80 [70–85] | 82.5 [70–97.5] | 80 [70–90] |
| PaO2/FiO2 | 107 [79–131] | 102.5 [80–133] | 105 [79–131] |
| Arterial lactates (mmol/L) | 1.1 [0.9–1.5] | 1.2 [1–1.65] | 1.2 [0.9–1.5] |
| Hemoglobin (mg/dL) | 13.3 ± 1.8 | 13.6 ± 1.7 | 13.5 ± 1.8 |
| SCr before first PP cycle (mg/dL) | 0.74 [0.61–0.89] | 0.87 [0.68–1.10] | 0.82 [0.65–0.98] |
| Last 24 h urine output (mL) | 1742 ± 555 | 1724 ± 592 | 1733 ± 570 |
| CFB from ICU entrance (mL) | 1615 [644–3770] | 413.5 [0–2015] | 1107 [0–3016] |
| CFB from ICU entrance/kg (mL/kg) | 21.4 [6.5–42.8] | 4.4 [0–24.7] | 13 [0–30.2] |
| SAPS-II score | 33 ± 6 | 34 ± 7 | 34 ± 6 |
| Hematocrit (%) | 36.4 ± 5.7 | 38.1 ± 4.8 | 37.3 ± 5.3 |
| Hemoglobin (mg/dL) | 11.9 ± 2.2 | 12.6 ± 1.7 | 12.2 ± 2 |
| Arterial lactates (mmol/L) | 1.5 [1.2–2] | 1.45 [1.1–1.9] | 1.5 [1.1–2] |
| Central venous pressure (mmHg) | 10 [7–11] | 8 [6–10] | 9 [6.5–10.5] |
| PEEP (cmH2O) | 10 [10–12] | 12 [9.5–13] | 12 [10–12] |
| CVP/PEEP ratio | 0.83 [0.615–1.1] | 0.805 [0.56–1] | 0.83 [0.575–1] |
| Tidal volume (mL) | 430 [420–480] | 450 [410–480] | 450 [420–480] |
| Duration of cycle (hours) | 41 [23–47] | 37.5 [24–46] | 39 [24–47] |
| Maximal PEEP (cmH2O) | 12 [10–12] | 12 [10–15] | 12 [10–14] |
| Maximal furosemide dose (mg/24 h) | 80 [40–100] | 80 [60–160] | 80 [60–120] |
| Worst SCr value (mg/dL) | 1.12 [0.89–2.3] | 1.84 [1.06–4.12] | 1.47 [0.97–3.18] |
| ICU Mortality | 22/45 (49%) | 32/48 (67%) | 54/93 (58%) |
| Number of PP cycles | 2 [1–2] | 2 [1–3] | 2 [1–3] |
| Days ICU (survivors) | 26 [17–44] | 24.5 [14.2–38.7] | 26 [15–40] |
| VFDs | 3 [0–12] | 0 [0–13.5] | 0 [0–12] |
| Variable | OR | 95% CI for OR | p-Value | |
|---|---|---|---|---|
| Age (in years) | 0.951 | 0.879 | 1.029 | 0.214 |
| BMI | 1.153 | 1.013 | 1.313 | 0.031 |
| Creatinine before PP | 3.346 | 0.846 | 13.234 | 0.085 |
| CVP before PP | 0.803 | 0.684 | 0.942 | 0.007 |
| CFB/kg before PP | 0.975 | 0.948 | 1.003 | 0.080 |
| SAPS before PP | 1.028 | 0.927 | 1.140 | 0.603 |
| Maximal PEEP during PP | 0.923 | 0.777 | 1.096 | 0.360 |
| Maximum serum lactate during PP | 1.128 | 0.611 | 2.084 | 0.699 |
| Previous story of CKD | 0.233 | 0.008 | 6.754 | 0.396 |
| Cycle duration (hours) | 0.975 | 0.934 | 1.017 | 0.241 |
| CFB after 48 h from supine positioning | 1.000 | 1.000 | 1.001 | 0.032 |
| Days in ICU before 1st PP cycle | 1.000 | 1.000 | 1.000 | 0.179 |
| Days in hospital before ICU | 1.000 | 1.000 | 1.000 | 0.368 |
| Constant | 1.617 | 0.887 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Rosa, R.; Grechi, B.; Ragazzi, R.; Alvisi, V.; Montanari, G.; Marangoni, E.; Volta, C.A.; Spadaro, S.; Scaramuzzo, G. Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome. Healthcare 2023, 11, 2903. https://doi.org/10.3390/healthcare11212903
La Rosa R, Grechi B, Ragazzi R, Alvisi V, Montanari G, Marangoni E, Volta CA, Spadaro S, Scaramuzzo G. Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome. Healthcare. 2023; 11(21):2903. https://doi.org/10.3390/healthcare11212903
Chicago/Turabian StyleLa Rosa, Riccardo, Benedetta Grechi, Riccardo Ragazzi, Valentina Alvisi, Giacomo Montanari, Elisabetta Marangoni, Carlo Alberto Volta, Savino Spadaro, and Gaetano Scaramuzzo. 2023. "Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome" Healthcare 11, no. 21: 2903. https://doi.org/10.3390/healthcare11212903
APA StyleLa Rosa, R., Grechi, B., Ragazzi, R., Alvisi, V., Montanari, G., Marangoni, E., Volta, C. A., Spadaro, S., & Scaramuzzo, G. (2023). Incidence and Determinants of Acute Kidney Injury after Prone Positioning in Severe COVID-19 Acute Respiratory Distress Syndrome. Healthcare, 11(21), 2903. https://doi.org/10.3390/healthcare11212903