
A Case of Axillary Web Syndrome Caused by Venous Blood Sampling


Abstract
:1. Introduction
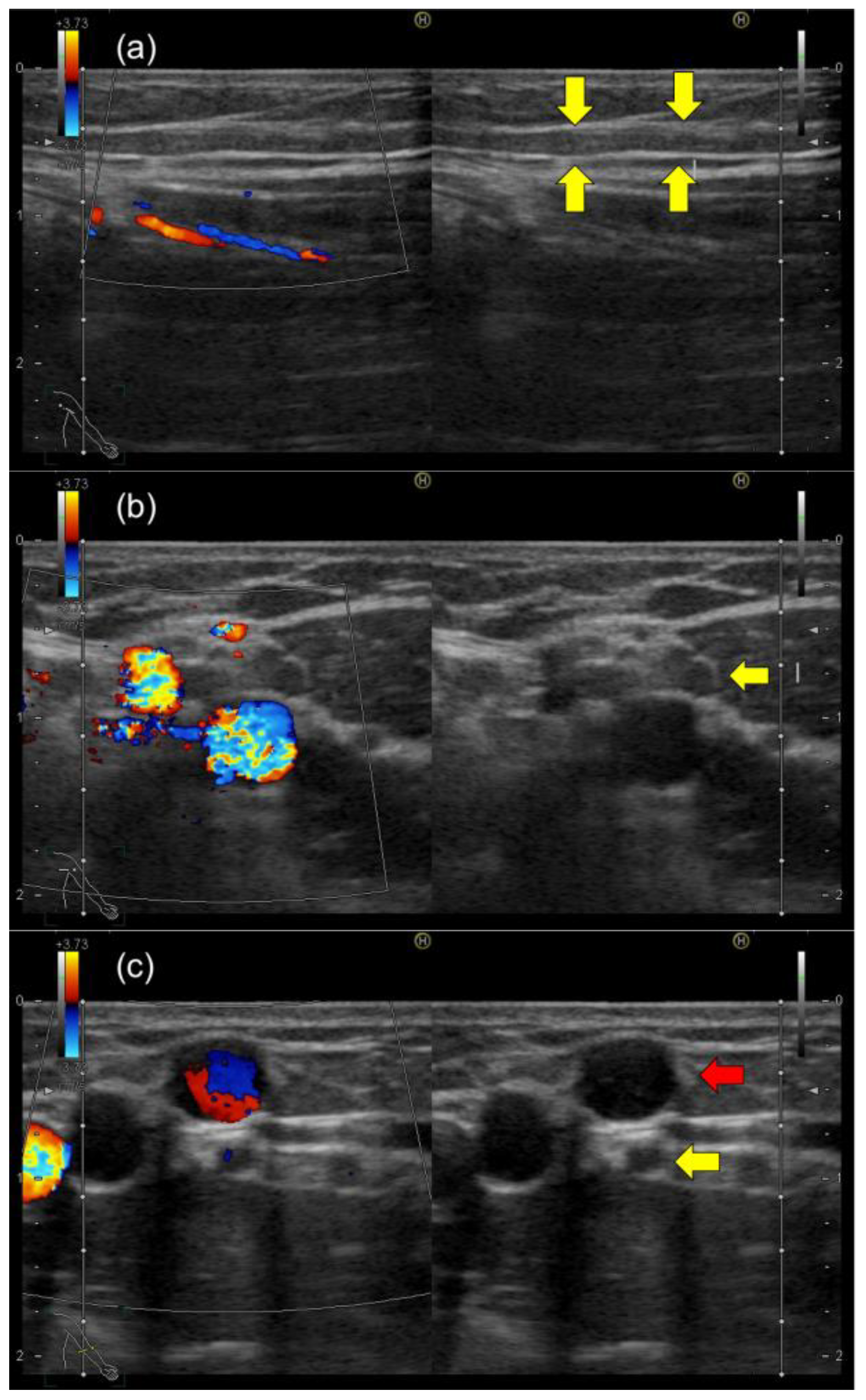
2. Case Report
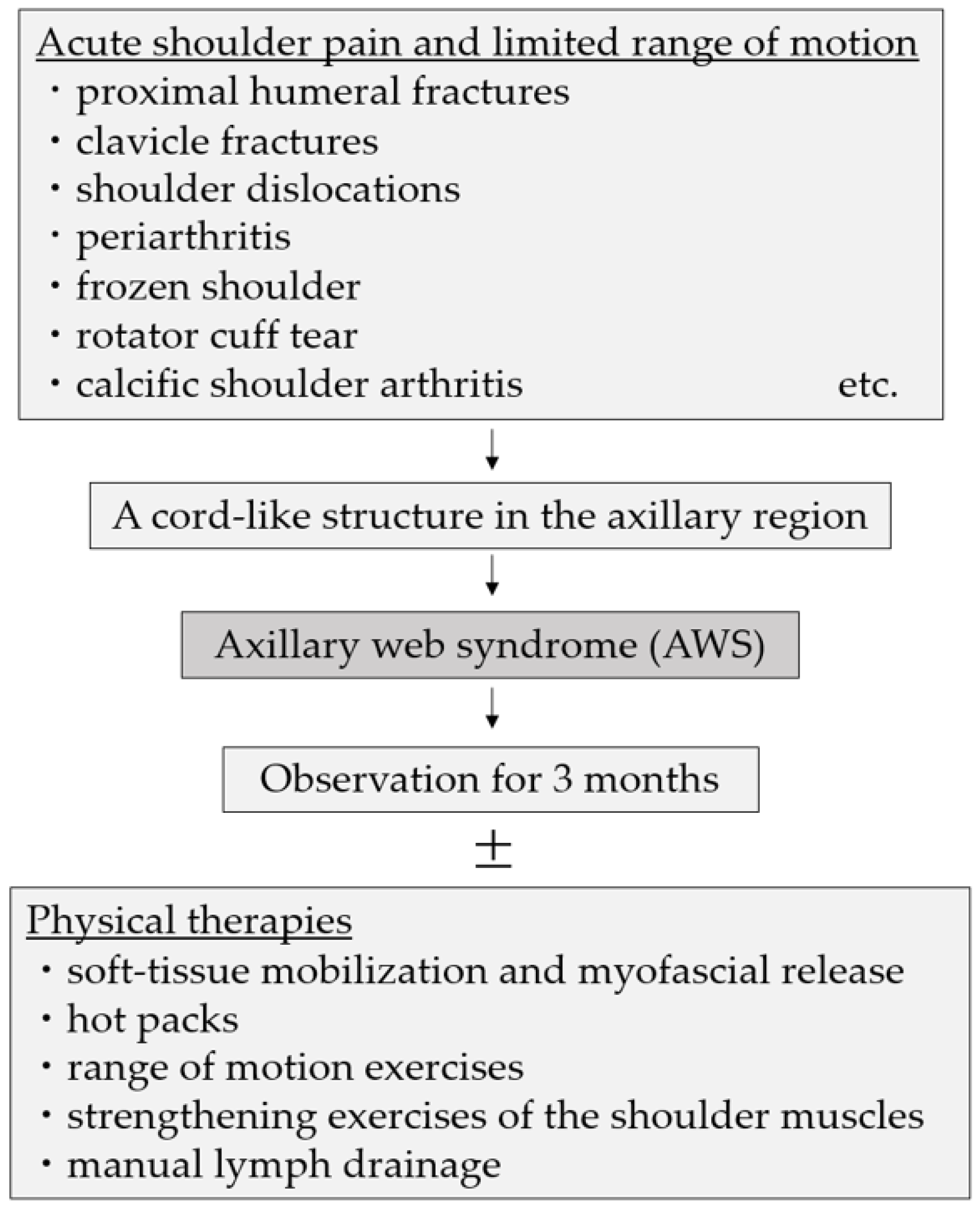
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moskovitz, A.H.; Anderson, B.O.; Yeung, R.S.; Byrd, D.R.; Lawton, T.J.; Moe, R.E. Axillary Web Syndrome after Axillary Dissection. Am. J. Surg. 2001, 181, 434–439. [Google Scholar] [CrossRef]
- Dinas, K.; Kalder, M.; Zepiridis, L.; Mavromatidis, G.; Pratilas, G. Axillary Web Syndrome: Incidence, Pathogenesis, and Management. Curr. Probl. Cancer 2019, 43, 100470. [Google Scholar] [CrossRef]
- Koehler, L.; Day, A.; Hunter, D.; Blaes, A.; Haddad, T.; Shanley, R. Five-Year Cumulative Incidence of Axillary Web Syndrome and Comparison in Upper Extremity Movement, Function, Pain, and Lymphedema in Survivors of Breast Cancer with and Without Axillary Web Syndrome. Arch. Phys. Med. Rehabil. 2022, 103, 1798–1806. [Google Scholar] [CrossRef]
- Koehler, L.A.; Hunter, D.W. Lymphspiration: The Axillary Web and Its Lymphatic Origin. Lymphology 2016, 49, 185–191. [Google Scholar]
- Torres-Lacomba, M.; Prieto-Gómez, V.; Arranz-Martín, B.; Ferrandez, J.C.; Yuste-Sánchez, M.J.; Navarro-Brazález, B.; Romay-Barrero, H. Manual Lymph Drainage with Progressive Arm Exercises for Axillary Web Syndrome After Breast Cancer Surgery: A Randomized Controlled Trial. Phys. Ther. 2022, 102, pzab314. [Google Scholar] [CrossRef]
- Roman, M.M.; Barbieux, R.; Eddy, C.; Karler, C.; Veys, I.; Zeltzer, A.; Adriaenssens, N.; Leduc, O.; Bourgeois, P. Lymphoscintigraphic Investigations for Axillary Web Syndromes. Lymphat. Res. Biol. 2022, 20, 417–424. [Google Scholar] [CrossRef]
- Johansson, K.; Chong, H.; Ciornei, C.D.; Brorson, H.; Mortimer, P.S. Axillary Web Syndrome: Evidence for Lymphatic Origin with Thrombosis. Lymphat. Res. Biol. 2020, 18, 329–332. [Google Scholar] [CrossRef]
- Leduc, O.; Fumière, E.; Banse, S.; Vandervorst, C.; Clément, A.; Parijs, T.; Wilputte, F.; Maquerlot, F.; Ezquer Echandia, M.; Tinlot, A.; et al. Identification and Description of the Axillary Web Syndrome (AWS) by Clinical Signs, MRI and US Imaging. Lymphology 2014, 47, 164–176. [Google Scholar]
- Koehler, L.A.; Hunter, D.W.; Haddad, T.C.; Blaes, A.H.; Hirsch, A.T.; Ludewig, P.M. Characterizing Axillary Web Syndrome: Ultrasonographic Efficacy. Lymphology 2014, 47, 156–163. [Google Scholar]
- Borg, M.B.; Mittino, L.; Battaglia, M.; Loro, A.; Lanzotti, L.; Invernizzi, M.; Baricich, A. Tolerability, Safety and Efficacy of a Specific Rehabilitation Treatment Protocol for Axillary Web Syndrome: An Observational Retrospective Study. Cancers 2023, 15, 426. [Google Scholar] [CrossRef]
- Lippi, L.; de Sire, A.; Losco, L.; Mezian, K.; Folli, A.; Ivanova, M.; Zattoni, L.; Moalli, S.; Ammendolia, A.; Alfano, C.; et al. Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review. J. Clin. Med. 2022, 11, 3839. [Google Scholar] [CrossRef] [PubMed]
- Agostini, F.; Attanasi, C.; Bernetti, A.; Mangone, M.; Paoloni, M.; del Monte, E.; Mammucari, M.; Maggiori, E.; Russo, D.; Di Marzo, R.; et al. Web Axillary Pain Syndrome—Literature Evidence and Novel Rehabilitative Suggestions: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 10383. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-T.; Francisco, M.D.; Yen, C.-K.; Wang, S.-Y.; Shiue, Y.-L. Vein Pattern Locating Technology for Cannulation: A Review of the Low-Cost Vein Finder Prototypes Utilizing near Infrared (NIR) Light to Improve Peripheral Subcutaneous Vein Selection for Phlebotomy. Sensors 2019, 19, 3573. [Google Scholar] [CrossRef]
- Ialongo, C.; Bernardini, S. Phlebotomy, a Bridge between Laboratory and Patient. Biochem. Med. 2016, 26, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.; Sitzia, J.; Harlow, W. Incidence and Risk of Arm Oedema Following Treatment for Breast Cancer: A Three-Year Follow-up Study. QJM 2005, 98, 343–348. [Google Scholar] [CrossRef]
- Zhang, Q.; Tan, C. Axillary Web Syndrome Following Granulomatous Inflammation after Folliculitis. Eur. J. Dermatol. 2016, 26, 314–315. [Google Scholar] [CrossRef]
- Welsh, P.; Gryfe, D. Atypical Presentation of Axillary Web Syndrome (AWS) in a Male Squash Player: A Case Report. J. Can. Chiropr. Assoc. 2016, 60, 294–298. [Google Scholar]
- Demir, Y.; Güzelküçük, Ü.; Kesikburun, S.; Yaşar, E.; Tan, A.K. A Rare Cause of Shoulder Pain: Axillary Web Syndrome. Turk. J. Phys. Med. Rehabil. 2017, 63, 178–180. [Google Scholar] [CrossRef]
- Lee, K.C.; Chang, Y.W.; Chen, C.P. Axillary Web Syndrome Following Epidermal Inclusion Cyst: A Case Report and Literature Review. Clin. Exp. Dermatol. 2019, 44, 64–66. [Google Scholar] [CrossRef]
- Puentes Gutiérrez, A.B.; García Bascones, M.; Puentes Gutiérrez, R.; Díaz Jiménez, M. [Idiopathic axillary web syndrome]. Rehabilitacion 2020, 54, 68–72. [Google Scholar] [CrossRef]
- Hunt, W.T.N.; Porter, R.; Lucke, T. Axillary Web Syndrome Induced by Physical Exertion. Clin. Exp. Dermatol. 2020, 45, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Soares, J.; Wollstein, R.; Ashmead, D. Axillary Web Syndrome Following Collagenase Injection for Dupuytren’s Contracture: A Case Report. J. Hand Surg. 2021, 46, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Malek, A.E.; Fife, C.E.; Rasmussen, J.C.; Karni, R.J.; Morrow, J.R.; Wanger, A.; Sevick-Muraca, E.M.; Ostrosky-Zeichner, L. Lymphatic Dissemination and Axillary Web Syndrome in Primary Cutaneous Tuberculosis Secondary to Needlestick Injury. Open Forum Infect. Dis. 2021, 8, ofab160. [Google Scholar] [CrossRef] [PubMed]
- Rashtak, S.; Gamble, G.L.; Gibson, L.E.; Pittelkow, M.R. From Furuncle to Axillary Web Syndrome: Shedding Light on Histopathology and Pathogenesis. Dermatology 2012, 224, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Alharazy, S.M. Occurrence of Axillary Web Syndrome without Surgical Intervention: A Case Report. J. Int. Med. Res. 2023, 51, 3000605231152384. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.N.; Burman, I.; Gale, E. Idiopathic Axillary Web Syndrome. Am. J. Med. 2023, 136, e119–e120. [Google Scholar] [CrossRef]
- Mohammed, J.; Ash, C.; Rai, J. “Patience Is a Virtue”—Post-Traumatic Axillary Web Syndrome—Resolution without Intervention. Arch. Clin. Cases 2023, 10, 18–20. [Google Scholar] [CrossRef]
- Rohit, A.; Peter, A.; Paul, A.; Anja, B.; Christian, D.; Renate, D.; Stefan, G.; Dietmar, H.; Johannes, J.; Peter, K.; et al. Prospective Observation of Clostridium Histolyticum Collagenase for the Treatment of Dupuytren’s Disease in 788 Patients: The Austrian Register. Arch. Orthop. Trauma Surg. 2019, 139, 1315–1321. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Year | Age | Sex | Origin | Time to Onset | Rehabilitation | Time to Improvement | Additional Treatment |
|---|---|---|---|---|---|---|---|---|
| Rashtak et al. [24] | 2012 | 57 | M | Furuncle | unknown | − | 5 weeks | Antimicrobial therapy for furuncle |
| Zhang et al. [16] | 2016 | 27 | F | Granulomatous Inflammation after Folliculitis | unknown | − | 3 months | Excision of the nodule |
| Welsh et al. [17] | 2016 | 38 | M | Squash (sport) | 24 h | + | 1 months | − |
| Demir et al. [18] | 2017 | 40 | M | Idiopathic | unknown | + | 1 months | − |
| Lee et al. [19] | 2019 | 63 | M | Epidermal inclusion cysts | unknown | + | 2 months | Excision of the nodule |
| Puentes et al. [20] | 2020 | 67 | F | Idiopathic | unknown | − | 4 months | − |
| Hunt et al. [21] | 2020 | 43 | M | Supporting one’s weight with one’s arms | 5 days | − | a few weeks | − |
| Soares et al. [22] | 2021 | 65 | F | Collagenase injection for Dupuytren’s contracture | 17 days | + | 2 months | − |
| Malek et al. [23] | 2021 | 42 | M | Cutaneous Tuberculosis and Lymphatic Dissemination | 7 weeks | − | 3 months | Chemotherapy for Tuberculosis |
| Alharazy et al. [25] | 2023 | 38 | M | Jumping rope | 2 days | − | 8 weeks | − |
| Siddiqui et al. [26] | 2023 | 73 | F | Idiopathic | unknown | + | 1 week | − |
| Mohammed et al. [27] | 2023 | 63 | M | Trauma | 2 weeks | − | 2 months | − |
| This report | 2023 | 31 | M | Venous Blood Sampling | 24 h | − | 3 months | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitajima, H.; Ichiseki, T.; Kaneuji, A.; Kawahara, N. A Case of Axillary Web Syndrome Caused by Venous Blood Sampling. Healthcare 2023, 11, 2390. https://doi.org/10.3390/healthcare11172390
Kitajima H, Ichiseki T, Kaneuji A, Kawahara N. A Case of Axillary Web Syndrome Caused by Venous Blood Sampling. Healthcare. 2023; 11(17):2390. https://doi.org/10.3390/healthcare11172390
Chicago/Turabian StyleKitajima, Hironori, Toru Ichiseki, Ayumi Kaneuji, and Norio Kawahara. 2023. "A Case of Axillary Web Syndrome Caused by Venous Blood Sampling" Healthcare 11, no. 17: 2390. https://doi.org/10.3390/healthcare11172390
APA StyleKitajima, H., Ichiseki, T., Kaneuji, A., & Kawahara, N. (2023). A Case of Axillary Web Syndrome Caused by Venous Blood Sampling. Healthcare, 11(17), 2390. https://doi.org/10.3390/healthcare11172390