Abstract
Since non-adherence to antibiotic therapy can cause several problems, including antimicrobial resistance (AMR) and treatment failures, the present study evaluated adherence to oral antibiotic therapy and AMR awareness among consecutively enrolled dental patients. Data concerning age, gender, socioeconomic status, education level, cohabitation, and general health were retrieved from medical records. AMR awareness was investigated through direct questions and adherence to antibiotic treatment was assessed through a modified Italian version of the Morisky medical scale-8 items. Participants’ characteristics were analyzed in relation to treatment adherence and AMR, using a Χ2 independence test (significance level of α <0.1). Dental patients generally showed a low (51.82%) adherence to oral antibiotic therapy, and medium and high adherence was reported only by 29.37% and 18.81% of participants. Treatment adherence was similar in relation to participants’ gender and age but significantly lower in subjects with only secondary school graduation and higher in participants with higher education levels. Non-cohabitants were significantly more adherent than cohabitants. AMR awareness was declared by 42.15% of males and 38.70% of females: 56.52% of dental patients aware of AMR were 18–38 years old, 35.20% were 39–59 years old, and 26.95% were aged between 60 and 80. Further studies are needed to develop adequate strategies, expanding dental patients’ knowledge of AMR, thus optimizing the benefits and reducing the risks of antibiotic administration in dental patients.
1. Introduction
The discovery and the use of antibiotics was one of the most important revolutions of the twentieth century to control and reduce infectious diseases [1].
However, excessive use and misuse of antibiotics play an important role in increasing bacterial resistance [2], leading, in turn, to an increased risk of complications and mortality and, consequently, to a more complex resolution of infectious diseases and potential treatment failure. Moreover, the overuse of antimicrobials increases healthcare costs [3,4], thereby causing a global public health problem that crosses all borders and is present worldwide [5,6].
Antimicrobial resistance (AMR) is caused by several factors, including inappropriate antibiotic prescription with overuse or misuse, and poor patient adherence to antimicrobial therapy, non-compliant with treatment recommendations [7], registering an increase in the improper use of antibiotics across Europe in recent years. Out of all antibiotics administrations, 7–10% were in an outpatient environment, with dentistry accounting for a comparatively higher amount of these prescriptions [7], as confirmed by numerous findings highlighting that dentists often do not observe antibiotics prescription guidelines, especially for prophylactic purposes in dentoalveolar surgery [8,9,10].
In addition, according to a recent global survey, non-adherence to antibiotic therapy, which determines an inappropriate use and may increase the risk of therapeutic failure, reinfection, and AMR, was estimated at around 22.3%, with a variation between 9% and 44% among countries [11]. Consequently, several measures were undertaken to improve patients’ adherence to short-term antimicrobial treatments, comprising accurate antibiotic prescriptions and written information on the importance of taking all medications [12]. To assess patients’ adherence to antibiotics, different direct and indirect methods, characterized by specific advantages and disadvantages, were developed [13,14], among which the Morisky Medication Adherence Scale (MMAS-4) is one of the most common indirect methods employed [15,16,17,18]. Based on the MMAS-4, the Morisky Medication Adherence Scale-8 (MMAS-8), which is an 8-item self-reported scale [19], was developed, and its validated Italian version [20], amended accordingly, was employed in the present study.
Considering the contributing role of patients’ adherence to antibiotic treatments in AMR [11,12] and the insufficient evidence concerning dental prescription, the study primarily aimed to assess the adherence to oral antibiotic therapy through a modified Italian version of the Morisky Medical Adherence Scale-8 items, also in relation to participants’ characteristics, and secondarily to evaluate the awareness of antimicrobial resistance among dental patients.
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
Outpatients (not hospitalized) attending the Complex Operating Unit of Odontostomatology, Head and Neck Clinical Department, between January and July 2021, who provided written informed consent and met the eligibility criteria described below, were consecutively enrolled in the study. The sample size was obtained from a previous study evaluating patients’ adherence to oral antibiotic prescription in outpatients [21,22,23].
Inclusion criteria were mentally competent subjects aged between 18 and 80 with no gender restriction, who received an antibiotics prescription compliant with the guidelines. Exclusion criteria were mentally incompetent subjects or subjects with cognitive impairments and chronic diseases causing worsening of the cognitive sphere, or those younger than 18 years of age.
2.2. Data Collection and Adherence to Antibiotic Treatment Assessment
Data concerning age, gender, socioeconomic status, education level, cohabitation, and general health were retrieved from medical and dental records.
In this study, only orally administered antibiotics were considered, being more frequently prescribed in dentistry compared to the other administration routes and characterized by higher compliance to treatment [24].
Upon completion of the oral antibiotics treatment prescribed, awareness of antibiotic resistance was investigated through direct questions asked to all participants, and adherence to the antibiotic prescription was assessed through a closed questionnaire capable of determining adherence to antibiotic therapy delivered to all enrolled subjects. The currently employed questionnaire was a validated Italian version [20] of the Morisky Medical Adherence Scale-8 items, adapted for a short-term oral antibiotic treatment; accordingly, questions 2 and 5 were properly modified. Question 2 originally asked, “People sometimes miss taking their medications for reasons other than forgetting. Over the past 2 weeks, were there any days when you did not take your medications?”It was modified as:“People sometimes miss taking their medications, but not because they forget it. Were there any days when you didn’t take antibiotics?” Question 5 originally asked,“Did you take all your medications yesterday?”It was modified to:“Did you take antibiotics on the last day of therapy?” (Table 1).

Table 1.
Administered questionnaire assessing adherence to antibiotic therapy: modified version of the Morisky Medical Adherence Scale-8 items (MMAS-8) [19].
Questionnaire items 1–7 required a yes or no answer, while item 8 provided a Likert scale answer (never, rarely, sometimes, often, always). As previously described [22], the questionnaire score was computed as follows: one point was assigned to no answers, and no points were assigned to yes answers, except for item 5, where the scores were inverted (no points were assigned to no answers, one point was assigned to yes answers). For item 8, the answers never and rarely were assigned a value of 1, while the answers sometimes, often, and always were assigned a value of 0. The total questionnaire score ranged from 0 to 8, where a score of 8 indicated complete adherence, scores of 6–7 showed medium adherence, and scores < 6 indicated a low adherence to antibiotic therapy [22].
2.3. Statistical Analysis
A descriptive statistical analysis of participants’ socio-demographic characteristics, antibiotic treatment adherence, and antimicrobial resistance awareness was conducted, to analyze and summarize collected data using Microsoft Excel software 2019 (Microsoft Corporation, Redmond, WA, USA). Socio-demographic characteristics were evaluated in relation to the level of antibiotic treatment adherence through a Χ2 independence test with a significance level of α < 0.01.
3. Results
3.1. Study Population
From January to July 2021, a total of 730 patients were examined, and 598 patients satisfied the inclusion and exclusion criteria.
Out of the 598 potentially eligible subjects, 45 did not give their consent to participate in the study, and 32 arbitrarily refused the antibiotic therapy prescribed; consequently, 521 patients were finally recruited for the study.
Socio-demographic characteristics of the enrolled subjects are summarized in Table 2.
Table 2.
Socio-demographic characteristics of the studied population.
3.2. Education Level and Cohabiting
In total,255 subjects were cohabitants, and among them, 25 (9.80%) had an elementary school license, 82 (32.16%) had secondary school graduation, 100 (39.22%) had high school graduation, and 48 (18.82%) had a university degree.
Among the 266 non-cohabitants, 8 (3.01%) had an elementary school license, 29 (10.90%) had secondary school graduation, 140 (52.63%) had high school graduation, and 89 (33.46%) possessed a university degree.
3.3. Antibiotic Therapy Adherence
Based on the Morisky Medical Adherence Scale-8 items questionnaire, the score distribution based on the reported answers is shown in Figure 1.
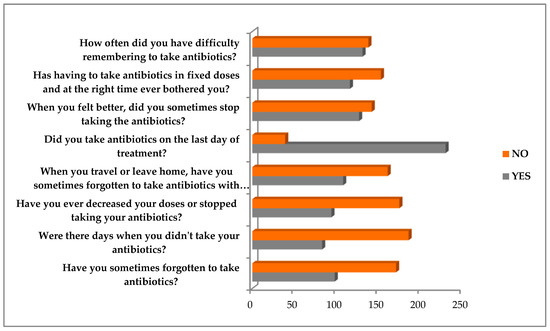
Figure 1.
Distribution of the Morisky scale score based on the questions and answers.
The overall level of adherence resulted as low in 270 (51.82%) subjects, medium in 153 (29.37%), and high in 98 (18.81%), respectively (Figure 2).
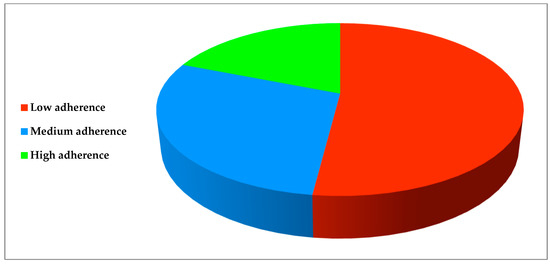
Figure 2.
Participants’ adherence to antibiotic treatment.
The Χ2 independence test (significance level of α < 0.01) revealed no statistically significant (α < 0.01) differences in the level of antibiotic treatment adherence in relation to participants’ gender and age. Conversely, a significantly lower adherence to therapy was found in subjects (n = 69) with secondary school graduation and a significantly higher adherence in those(n = 86) with high school graduation or a university degree. Non-cohabitants were significantly more adherent to antibiotic therapy when compared to cohabitants. The distribution of adherence levels based on gender, age, education level, and cohabiting is summarized in Table 3.
Table 3.
Distribution of adherence levels by gender, age, education level, and cohabiting.
3.4. Antibiotic Resistance (AMR) Awareness
Awareness of antibiotic resistance was declared by 110 males (42.15%) and 101 females (38.70%), and by 104 subjects (56.52%) between 18 and 38 years old, 69 (35.20%) between 39 and 59 years of age, and 38 (26.95%) of those aged between 60 and 80.
In relation to the education level, AMR awareness was expressed by 2 subjects(6.06%) with elementary school license, 20 (18.02%) with secondary school graduation, 93 (38.75%) with high school graduation, and 96 (70.07%) university-graduated subjects. Among the 211 subjects who declared to be aware of AMR, the level of adherence to antibiotic treatment resulted low in 66 subjects (31.28%), medium in 83 (39.34%), and high in 62 (29.38%), respectively.
Analyzing the socio-demographic characteristics of enrolled subjects in relation to the awareness of antibiotic resistance, no association (α = 0.01) was found concerning participants’ gender; conversely, a statistically significant association (α = 0.01) was found in younger compared to older subjects. A significant association was also found between subjects with higher compared to lower education levels (α = 0.01) and between those showing higher adherence to antibiotic prescription (α = 0.01) and AMR awareness.
4. Discussion
The present study primarily aimed to assess the adherence to oral antibiotic therapy through a modified Italian version of the Morisky Medical Adherence Scale-8 items, also in relation to participants’ characteristics, and secondarily to evaluate the awareness of antimicrobial resistance among dental patients, in view of the contributing role of patients’ adherence to antibiotic treatments in AMR [11,12] and of the insufficient evidence concerning oral prescription in dentistry.
Adherence to the prescribed oral antibiotic therapy resulted as low in 270 (51.82%) dental patients, medium in 153 (29.37%), and high in 98 (18.81%). Our results are in accordance with an Italian study, revealing a low adherence to antibiotic treatment in 59.9% of the study population [25], and another study conducted in Europe, reporting that 55.8% of participants did not complete the antimicrobial therapy prescribed [26]. Similarly, Llor et al. described a non-adherence of 25.2% in a Spanish sample, progressively declining over time in an additional 28.7% [27]; in a Chinese study, adherence to antibiotic therapy was observed in only 13% of patients [28].
In the present study, the level of adherence to antibiotic therapy was negatively influenced by cohabitation, in contrast with Desta et al. results [29], and positively linked to a higher education level of the participants. The last finding may be explained by the fact that currently enrolled, non-cohabiting subjects had a higher education level (52.63% with high school graduation and 33.46% with a university degree) than cohabiting ones (39.22% with high school graduation and 18.82% with a university degree).
No relation has been presently found between the level of adherence to antibiotic therapy and gender, compliant with the results of a recent meta-analysis [30]; however, conflicting results have been obtained by Manteuffel et al. [31], reporting lower adherence in the female gender.
Our results showed no significant differences in adherence to antibiotic treatment between participants in the different age groups. In contrast, Fernandes et al. identified increasing age as a factor associated with non-adherence [32], while Rolnick et al. found a greater non-adherence in younger patients [33].
Awareness of antimicrobial resistance resulted aslow in 66 dental patients (31.28%), medium in 83 (39.34%), and high in 62 (29.38%). AMR was positively associated with higher education levels and a younger age. Indeed, it appears that older age groups have a lower AMR awareness, and that the failure of antibiotic intake is mainly caused by forgetfulness in 37.24% of cases, compared to 30.71% who do not take it intentionally [34]. More generally, 36.08% of patients stopped taking or decreased the doses of their antibiotics, and 48.37% stopped taking their antibiotics in advance as their health conditions improved. Less adherence to antibiotic therapy was found associated with a lower level of education and knowledge of the issues related to the improper use of antibiotics. The results from this study agree with a recent study by Chan et al., concluding that the lack of knowledge of antibiotics, including the problem related to antimicrobial resistance, affects adherence to antibiotic therapy. Therefore, patients, unaware of the possible damage to both their health and the public health, may pay less attention to following antibiotic treatment or even intentionally decide not to adhere to it correctly [35]. Similarly, Raupach-Rosin et al. pointed out that higher education, especially a university degree, positively affects knowledge and AMR awareness [36]. However, such findings highlight the need to provide dental patients with more accurate indications on antibiotic prescription and information on antimicrobial resistance, aiming primarily to increase knowledge and comprehension of the benefits related to the correct use of antibiotics as well as of the risks deriving from their abuse and misuse, and secondarily, to improve dental patients’ overall behavior toward antibiotic intake. According to these considerations, the present study also noted a significant positive association between AMR and adherence to antibiotic therapy.
Moreover, by simplifying antibiotic administration, in compliance with guidelines for antimicrobial stewardship, dental patients could better tolerate the prescribed treatment regimen, especially considering that 51.63% of participants showed difficulty remembering to take their antibiotics [37,38,39,40,41]. Today, the adherence to antibiotic therapy has increased thanks to electronic devices with a reminder function, smartphone apps, and periodic adherence measurements [42,43,44]. Other simply modifiable adherence barriers, mainly described as worries about side effects and drug–drug interactions, and difficulties in swallowing tablets and integrating antibiotic intake into daily life, should also be carefully addressed to optimize patients’ adherence to antibiotic treatment [45]. Finally, the presented results, revealing a low level of adherence to antibiotic therapy in dental patients, are consistent with the findings from other studies employing a self-report as a method for measuring adherence [42].
The limited number of enrolled participants may represent the main limitation of the study, not allowing the generalizability of the results with a high level of accuracy. Therefore, consistent conclusions could not be drawn and presented findings definitely require validation by more comprehensive studies. However, to our knowledge, the present study is the first to evaluate the adherence to antibiotic therapy in dental patients. The Morisky scale questionnaire, currently employed, allowed a sensitive measurement of the adherence to antibiotic treatment, also reflecting dental patients’ behavior during antimicrobial intake [46]. Although self-reports have well-known intrinsic limitations due to memory bias, overestimating adherence, and stimulation of socially acceptable responses [46], assessing adherence to antibiotic therapy through questionnaires seems to have a medium–high agreement with measurements obtained through other methods [20,47,48,49].Its use, combined with additional objective assessment methods, such as electronic adherence monitoring devices, pill counts, pharmacy refill rate, or direct drug and biomarker measurement, may be indicated to improve measurements [20,44].
5. Conclusions
Presently enrolled dental patients generally showed a low (51.82%) adherence to oral antibiotic therapy, significantly higher in participants with higher education levels and in non-cohabitants. Given that adherence to antibiotic treatment is necessary to make the therapy effective and, at the same time, to reduce the impact of antimicrobial resistance on public health, interventions to expand dental patients’ knowledge of antibiotic therapy and, particularly, of antimicrobial resistance, may enhance their adherence to treatment.
Antimicrobial resistance awareness was higher in younger (56.52%)dental patients. Such findings suggest that focused interventions counteracting patients’ non-adherence, especially eliminating modifiable adherence barriers and improving AMR knowledge, should be directed to the elderly.
Further studies are needed, due to the lack of investigations on adherence to antibiotic treatment in dentistry, to assess it and to evaluate possible influencing factors to develop adequate strategies to optimize the benefits and reduce the risks of antibiotic therapies in dental patients.
Author Contributions
Conceptualization, F.D. and L.S.; Methodology, F.D.S.; Validation, F.D.S. and L.S.; Formal Analysis, F.D. and A.L.; Investigation, F.D. and F.D.S.; Data Curation, D.P. and F.D.C.; Writing—Original Draft Preparation, F.D. and F.D.S.; Writing—Review & Editing, F.D., F.D.S., F.D.C., A.L., D.P. and L.S.; Visualization, A.L. and D.P.; Supervision, F.D.C.; Project Administration, L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The present monocentric, observational, no-profit study was conducted in compliance with the ethical standards of the Declaration of Helsinki and approved by the local Ethical Committee (Protocol No. 34/2013 on 6 May 2013, confirmed by the resolution #776, 6 August 2014).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors acknowledge the help of Cristian Manfredi, formerly a dental student, in collecting part of the clinical data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guerrini, L.; Monaco, A.; Pietropaoli, D.; Ortu, E.; Giannoni, M.; Marci, M.C. Antibiotics in Dentistry: A Narrative Review of Literature and Guidelines Considering Antibiotic Resistance. Open Dent. J. 2019, 13, 383–398. [Google Scholar] [CrossRef]
- Landecker, H. Antibiotic resistance and the biology of history. Body Soc. 2016, 22, 19–52. [Google Scholar] [CrossRef] [PubMed]
- Teoh, L.; Sloan, A.J.; McCullough, M.J.; Thompson, W. Measuring Antibiotic Stewardship Programmes and Initiatives: An Umbrella Review in Primary Care Medicine and a Systematic Review of Dentistry. Antibiotics 2020, 9, 607. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, M. Report on personality and adherence to antibiotic therapy: A population-based study. BMC Psychol. 2013, 1, 24. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antimicrobial Resistance (who.int). Available online: https://www.who.int/health-topics/antimicrobial-resistance (accessed on 31 July 2022).
- Liau, I. Antibiotic resistance in severe odontogenic infections of the South Australian population: A 9-year retrospective audit. Aust. Dent. J. 2018, 63, 187–192. [Google Scholar] [CrossRef]
- Löffler, C.; Böhmer, F. The effect of interventions aiming to optimise the prescription of antibiotics in dental care-A systematic review. PLoS ONE 2017, 12, e0188061. [Google Scholar] [CrossRef]
- Preus, H.R.; Fredriksen, K.W.; Vogsland, A.E.; Sandvik, L.; Grytten, J.I. Antibiotic-prescribing habits among Norwegian dentists: A survey over 25 years (1990–2015). Eur. J. Oral Sci. 2017, 125, 280–287. [Google Scholar] [CrossRef]
- Chisci, G.; Capuano, A.; Parrini, S. Alveolar Osteitis and Third Molar Pathologies. J. OralMaxillofac. Surg. 2018, 76, 235–236. [Google Scholar] [CrossRef]
- Busa, A.; Parrini, S.; Chisci, G.; Pozzi, T.; Burgassi, S.; Capuano, A. Local versus systemic antibiotics effectiveness: A comparative study of postoperative oral disability in lower third molar surgery. J. Craniofac. Surg. 2014, 25, 708–709. [Google Scholar] [CrossRef]
- Pechère, J.C.; Hughes, D.; Kardas, P.; Cornaglia, G. Non-compliance with antibiotic therapy for acute community infections: A global survey. Int. J. Antimicrob. Agents 2007, 29, 245–253. [Google Scholar] [CrossRef]
- Haynes, R.B.; Ackloo, E.; Sahota, N.; McDonald, H.P.; Yao, X. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2008, 2, CD000011. [Google Scholar] [CrossRef] [PubMed]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B. Measurement, correlates, and health outcomes of medication adherence among seniors. Ann. Pharmacother. 2004, 38, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Morgado, M.; Rolo, S.; Macedo, A.F.; Pereira, L.; Castelo-Branco, M. Predictors of uncontrolled hypertension and antihypertensive medication nonadherence. J. Cardiovasc. Dis. Res. 2010, 1, 196–202. [Google Scholar] [PubMed]
- Marcum, Z.A.; Zheng, Y.; Perera, S.; Strotmeyer, E.; Newman, A.B.; Simonsick, E.M.; Shorr, R.I.; Bauer, D.C.; Donohue, J.M.; Hanlon, J.T.; et al. Prevalence and correlates of self-reported medication non-adherence among older adults with coronary heart disease, diabetes mellitus, and/or hypertension. Res. Soc. Adm. Pharm. 2013, 9, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Voils, C.I.; Hoyle, R.H.; Thorpe, C.T.; Maciejewski, M.L.; Yancy, W.S., Jr. Improving the measurement of self-reported medication nonadherence. J. Clin. Epidemiol. 2011, 64, 250–254. [Google Scholar] [CrossRef]
- Shalansky, S.J.; Levy, A.R.; Ignaszewski, A.P. Self-reported Morisky score for identifying nonadherence with cardiovascular medications. Ann. Pharmacother. 2004, 38, 1363–1368. [Google Scholar] [CrossRef]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens. 2008, 10, 348–354. [Google Scholar] [CrossRef]
- Fabbrini, G.; Abbruzzese, G.; Antonini, A.; Barone, P.; Antonini, A.; Tinazzi, M.; Castegnaro, G.; Rizzoli, S.; Morisky, D.E.; Lessi, P.; et al. Adherence to anti-Parkinson drug therapy in the REASON sample of Italian patients with Parkinson’s disease: The linguistic validation of the Italian version of the Morisky Medical Adherence Scale-8 items. Neurol. Sci. 2013, 34, 2015–2022. [Google Scholar] [CrossRef]
- Janežič, A.; Locatelli, I.; Kos, M. Criterion validity of 8-item Morisky Medication Adherence Scale in patients with asthma. PLoS ONE 2017, 12, e0187835. [Google Scholar] [CrossRef]
- McCullough, A.R.; Tunney, M.M.; Quittner, A.L.; Elborn, J.S.; Bradley, J.M.; Hughes, C.M. Treatment adherence and health outcomes in patients with bronchiectasis. BMC Pulm. Med. 2014, 14, 107. [Google Scholar] [CrossRef] [PubMed]
- Eells, S.J.; Nguyen, M.; Jung, J.; Macias-Gil, R.; May, L.; Miller, L.G. Relationship between Adherence to Oral Antibiotics and Postdischarge Clinical Outcomes among Patients Hospitalized with Staphylococcus aureus Skin Infections. Antimicrob. Agents Chemother. 2016, 60, 2941–2948. [Google Scholar] [CrossRef] [PubMed]
- Cunha, C.B. Oral Antibiotic Therapy for Common Infectious Diseases. Med. Clin. N. Am. 2018, 102, 947–954. [Google Scholar] [CrossRef]
- Menditto, E.; Guerriero, F.; Orlando, V.; Crola, C.; Di Somma, C.; Illario, M.; Morisky, D.E.; Colao, A. Self-Assessment of Adherence to Medication: A Case Study in Campania Region Community-Dwelling Population. J. Aging Res. 2015, 2015, 682503. [Google Scholar] [CrossRef]
- Francis, N.A.; Gillespie, D.; Nuttall, J.; Hood, K.; Little, P.; Verheij, T.; Coenen, S.; Cals, J.W.; Goossens, H.; Butler, C.C.; et al. Antibiotics for acute cough: An international observational study of patient adherence in primary care. Br. J. Gen. Pract. 2012, 62, 429–437. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Llor, C.; Hernández, S.; Bayona, C.; Moragas, A.; Sierra, N.; Hernández, M.; Miravitlles, M. A study of adherence to antibiotic treatment in ambulatory respiratory infections. Int. J. Infect. Dis. 2013, 17, 168–172. [Google Scholar] [CrossRef]
- Tong, S.; Pan, J.; Lu, S.; Tang, J. Patient compliance with antimicrobial drugs: A Chinese survey. Am. J. Infect. Control 2018, 46, e25–e29. [Google Scholar] [CrossRef]
- Desta, L.; Khedri, M.; Jernberg, T.; Andell, P.; Mohammad, M.A.; Hofman-Bang, C.; Erlinge, D.; Spaak, J.; Persson, H. Adherence to beta-blockers and long-term risk of heart failure and mortality after a myocardial infarction. ESC Heart Fail. 2021, 8, 344–355. [Google Scholar] [CrossRef]
- Biffi, A.; Rea, F.; Iannaccone, T.; Filippelli, A.; Mancia, G.; Corrao, G. Sex differences in the adherence of antihypertensive drugs: A systematic review with meta-analyses. BMJ Open 2020, 10, e036418. [Google Scholar] [CrossRef]
- Manteuffel, M.; Williams, S.; Chen, W.; Verbrugge, R.R.; Pittman, D.G.; Steinkellner, A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J. Womens Health 2014, 23, 112–119. [Google Scholar] [CrossRef]
- Fernandes, M.; Leite, A.; Basto, M.; Nobre, M.A.; Vieira, N.; Fernandes, R.; Nogueira, P.; Nicola, P.J. Non-adherence to antibiotic therapy in patients visiting community pharmacies. Int. J. Clin. Pharm. 2014, 36, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Rolnick, S.J.; Pawloski, P.A.; Hedblom, B.D.; Asche, S.E.; Bruzek, R.J. Patient characteristics associated with medication adherence. Clin. Med. Res. 2013, 11, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Zanichelli, V.; Tebano, G.; Gyssens, I.C.; Vlahović-Palčevski, V.; Monnier, A.A.; StanicBenic, M.; Harbarth, S.; Hulscher, M.; Pulcini, C.; Huttner, B.D. Patient-related determinants of antibiotic use: A systematic review. Clin. Microbiol. Infect. 2019, 25, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.H.; Fan, M.M.; Fok, C.M.; Lok, Z.L.; Ni, M.; Sin, C.F.; Wong, K.K.; Wong, S.M.; Yeung, R.; Yeung, T.T.; et al. Antibiotics nonadherence and knowledge in a community with the world’s leading prevalence of antibiotics resistance: Implications for public health intervention. Am. J. Infect. Control 2012, 40, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Raupach-Rosin, H.; Rübsamen, N.; Schütte, G.; Raschpichler, G.; Chaw., P.S.; Mikolajczyk, R. Knowledge on Antibiotic Use, Self-Reported Adherence to Antibiotic Intake, and Knowledge on Multi-Drug Resistant Pathogens—Results of a Population-Based Survey in Lower Saxony, Germany. Front. Microbiol. 2019, 10, 776. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M. Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Prev. Med. 2017, 99, 269–276. [Google Scholar] [CrossRef]
- Di Spirito, F.; Argentino, S.; Martuscelli, R.; Sbordone, L. MRONJ incidence after multiple teeth extractions in patients taking oral bisphosphonates without “drug holiday”: A retrospective chart review. Oral Implantol. 2019, 12, 105–110. [Google Scholar]
- Barone, A.; Chatelain, S.; Derchi, G.; Di Spirito, F.; Martuscelli, R.; Porzio, M.; Sbordone, L. Effectiveness of antibiotics in preventing alveolitis after erupted tooth extraction: A retrospective study. Oral Dis. 2020, 26, 967–973. [Google Scholar] [CrossRef]
- Cope, A.L.; Francis, N.A.; Wood, F.; Chestnutt, I.G. Antibiotic prescribing in UK general dental practice: A cross-sectional study. Community Dent. Oral Epidemiol. 2016, 44, 145–153. [Google Scholar] [CrossRef]
- Mainjot, A.; D’Hoore, W.; Vanheusden, A.; Van Nieuwenhuysen, J.P. Antibiotic prescribing in dental practice in Belgium. Int. Endod. J. 2009, 42, 1112–1117. [Google Scholar] [CrossRef] [PubMed]
- Di Matteo, M.R.; Giordani, P.J.; Lepper, H.S.; Croghan, T.W. Patient adherence and medical treatment outcomes: A meta-analysis. Med. Care 2002, 40, 794–811. [Google Scholar] [CrossRef]
- Demonceau, J.; Ruppar, T.; Kristanto, P.; Hughes, D.A.; Fargher, E.; Kardas, P.; de Geest, S.; Dobbels, F.; Lewek, P.; Urquhart, J.; et al. Identification and assessment of adherence-enhancing interventions in studies assessing medication adherence through electronically compiled drug dosing histories: A systematic literature review and meta-analysis. Drugs 2013, 73, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Jover, V.; Sala-González, M.; Guilabert, M.; Mira, J.J. Mobile Apps for Increasing Treatment Adherence: Systematic Review. J. Med. Int. Res. 2019, 21, e12505. [Google Scholar] [CrossRef] [PubMed]
- Haag, M.; Hersberger, K.E.; Arnet, I. Assessing Medication Adherence Barriers to Short-Term Oral Antibiotic Treatment in Primary Care-Development and Validation of a Self-Report Questionnaire (BIOTICA). Int. J. Environ. Res. Public Health 2021, 18, 7768. [Google Scholar] [CrossRef]
- Garber, M.C.; Nau, D.P.; Erickson, S.R.; Aikens, J.E.; Lawrence, J.B. The concordance of self-report with other measures of medication adherence: A summary of the literature. Med. Care 2004, 42, 649–652. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; Amato, A.; Caggiano, M.; Lo Giudice, R.; Martina, S. Attitudes towards antibiotic prescription and antimicrobial resistance awareness among italian dentists: What are the milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef]
- Hawkshead, J.; Krousel-Wood, M.A. Techniques for measuring medication adherence in hypertensive patients in out-patient settings: Advantages and limitations. Dis. Manag. Health Outcomes 2007, 15, 109–118. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).