
The Post-Traumatic Growth of Primary Caregivers of Patients after Liver Transplantation
Abstract
:1. Introduction
1.1. The Status of Liver Transplantation
1.2. Concepts Related to Stress, Coping Strategies, and Post-Traumatic Growth
2. Materials and Methods
- (1)
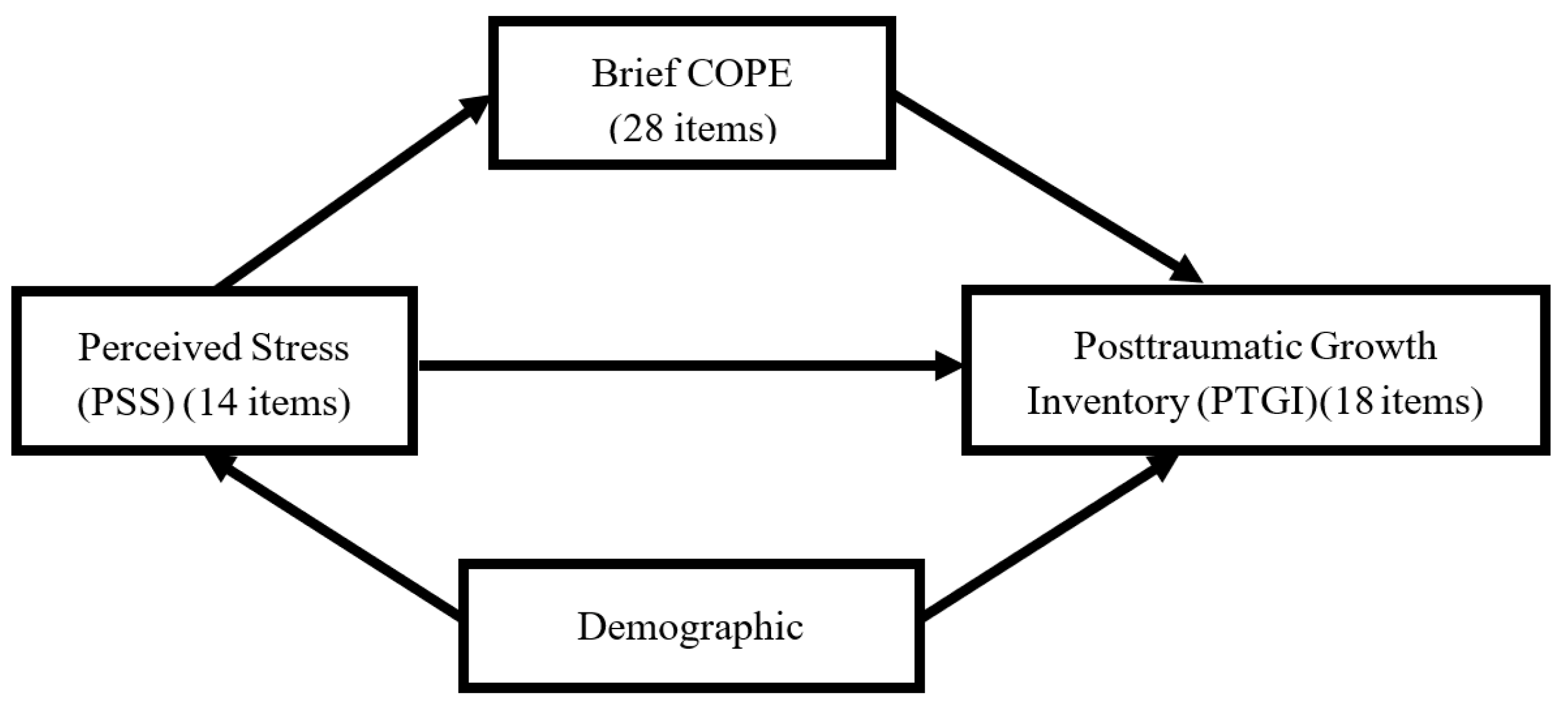
- Demographic questionnaire: It was prepared with reference to the relevant literature and included: gender, age, education level, marital status, religious beliefs, pre-transplant occupation of care, annual family income, length of care, and relationship to liver transplant recipients.
- (2)
- Perceived Stress Scale (PSS): This study used the Perceived Stress Scale developed by Cohen et al. In 2005, Dr. Li-Chuan Chu was authorized to translate it into a Chinese version and used a self-reported method to measure the degree of stress in an individual’s life in the past month. A five-point Likert scale scoring method was used with the five options “never”, “occasionally”, “sometimes”, “often”, and “always”, giving 0, 1, 2, 3, and 4 points. There were 14 questions in total, of which 7 were positive questions, and the other 7 were reverse questions. First of all, the 7 positive questions must be scored in the reverse direction on the scale, and all scores must be added together. The total score is 0–56 points. The higher the score, the higher the perceived stress intensity of the subject. The scale reliability based on Cronbach’s α value was 0.85 in other studies and 0.71 in this study, which is acceptable [28].
- (3)
- Brief Coping Strategies Scale (Brief COPE): Based on the Brief COPE adapted by Carver in 1997, strategies were divided into problem coping strategies, emotional coping strategies, and dysfunctional coping strategies. A total of 14 coping strategies were measured, including active coping, emotional support, instrumental support, positive reinterpretation, planning, acceptance, denial, substance use, self-distraction, catharsis, behavioral avoidance, humor, religion, and self-blame. Each coping strategy consisted of 2 questions, with a total of 28 questions, and its Cronbach’s α coefficient was between 0.50 and 0.90. The score was on a four-point scale, with the four options “never”, “occasionally”, “sometimes”, and “often”, giving 1, 2, 3, and 4 points, respectively. The higher the behavioral characteristics of this dimension, the better the coping has. Huei-Jia Tzeng, Chang-Chu Ho, and Ming-Chang Tsai (2010) conducted Brief COPE in Chinese culture. After obtaining the questionnaire from the original author, the content was scored and revised according to the relevance, correctness, and wording appropriateness of the research topic questionnaire. After synthesizing expert opinions, the content validity was completed. The internal consistency reliability of the scale was Cronbach’s α of 0.86, and the Cronbach’s α in this study was 0.84 [29].
- (4)
- Posttraumatic Growth Inventory: The questionnaire was developed by Tedeschi and Calhoun in 1996, and Ho et al. (2004) translated it into the Chinese version. The internal consistency reliability based on Cronbach’s α of the Chinese version was 0.86, with a total of 4 subscales: self, spirituality, life direction, and interpersonal. It is based on a six-point scale with “no change at all” “, “Very small change”, “Small change”, “Medium change”, “Obvious change”, and “Very large change”, giving 0, 1, 2, 3, 4, and 5. A score greater than or equal to three was considered moderate or above growth. In this study, Cronbach’s α was 0.91 [30].
3. Results
3.1. Demographic Variables of Caregivers
3.2. Analysis of Care Stress, Coping Strategies, and Post-Traumatic Growth among Primary Caregivers
3.3. Differences in Primary Caregiver Demographic Variables and Post-Traumatic Growth
3.4. The Mediating Effect of Coping Strategies on Perceived Stress and Post-Traumatic Growth
3.5. Factors Affecting the Post-Traumatic Growth of the Primary Caregivers of Liver Transplant Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Welfare, Executive Yuan. 2020 Year Statistics on Cause of Death. Available online: https://www.mohw.gov.tw/cp-5256-63399-2.html (accessed on 1 June 2022).
- Global Health Estimates; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/data/global-health-estimates (accessed on 27 July 2022).
- GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef]
- Finkenstedt, A.; Nachbaur, K.; Zoller, H.; Joannidis, M.; Pratschke, J.; Graziadei, I.W.; Vogel, W. Acute-on-chronic liver failure: Excellent outcomes after liver transplantation but high mortality on the wait list. Liver Transplant. 2013, 19, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; McMaster, P.; O’Grady, J.G.; Castaing, D.; Klempnauer, J.L.; Jamieson, N.; Muhlbacher, F. Evolution of liver transplantation in Europe: Report of the European Liver Transplant Registry. Liver Transplant. 2003, 9, 1231–1243. [Google Scholar] [CrossRef] [PubMed]
- Humar, A.; Ganesh, S.; Jorgensen, D.; Tevar, A.; Ganoza, A.; Molinari, M.; Hughes, C. Adult living donor versus deceased donor liver transplant (LDLT versus DDLT) at a single center: Time to change our paradigm for liver transplant. Ann. Surg. 2019, 270, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare, Central Health Insurance Agency. Organ Transplant Survival Rate. Available online: https://www.nhi.gov.tw/News_Content.aspx?n=FC05EB85BD57C709&sms=587F1A3D9A03E2AD&s=78A05FFEA39BA610 (accessed on 1 May 2022).
- Braun, M.; Mikulincer, M.; Rydall, A.; Walsh, A.; Rodin, G. Hidden morbidity in cancer: Spouse caregivers. J. Clin. Oncol. 2007, 25, 4829–4834. [Google Scholar] [CrossRef]
- Cohen, M.; Katz, D.; Baruch, Y. Stress among the family caregivers of liver transplant recipients. Prog. Transplant. 2007, 17, 48–53. [Google Scholar] [CrossRef]
- Northouse, L.L.; Mood, D.W.; Montie, J.E.; Sandler, H.M.; Forman, J.D.; Hussain, M.; Pienta, K.J.; Smith, D.C.; Sanda, M.G.; Kershaw, T. Living with prostate cancer: Patients’ and spouses’ psychosocial status and quality of life. J. Clin. Oncol. 2007, 25, 4171–4177. [Google Scholar] [CrossRef]
- Lin, I.F.; Fee, H.R.; Wu, H.S. Negative and positive caregiving experiences: A closer look at the intersection of gender and relationship. Fam. Relat. 2012, 61, 343–358. [Google Scholar] [CrossRef]
- Vitaliano, P.P.; Zhang, J.; Scanlan, J.M. Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol. Bull. 2003, 129, 946. [Google Scholar] [CrossRef]
- Goetzinger, A.M.; Blumenthal, J.A.; O’Hayer, C.V.; Babyak, M.A.; Hoffman, B.M.; Ong, L.; Davis, R.D.; Smith, S.R.; Rogers, J.G.; Milano, C.A.; et al. Stress and coping in caregivers of patients awaiting solid organ transplantation. Clin. Transplant. 2012, 26, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Folkman, S. Stress, coping, and hope. Psycho-Oncology 2010, 19, 901–908. [Google Scholar] [CrossRef]
- Kim, Y.; Carver, C.S.; Deci, E.L.; Kasser, T. Adult attachment and psychological well-being in cancer caregivers: The mediational role of spouses’ motives for caregiving. Health Psychol. 2008, 27, S144–S154. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. J. Trauma. Stress 1996, 9, 455–471. [Google Scholar] [CrossRef]
- Pillai, V.G.; Chen, C.L. Living donor liver transplantation in Taiwan—challenges beyond surgery. Hepatobiliary Surg. Nutr. 2016, 5, 145. [Google Scholar]
- Taiwan Organ Sharing Registry and Patient Autonomy Promotion Center. Available online: https://www.torsc.org.tw/docList.jsp?uid=158&pid=9&rn=-897379992 (accessed on 11 November 2021).
- Broelsch, C.E.; Testa, G.; Alexandrou, A.; Malago, M. Living related liver transplantation: Medical and social aspects of a controversial therapy. Gut 2002, 50, 143–145. [Google Scholar] [CrossRef]
- Chen, C.L.; Concejero, A.; Wang, C.C.; Wang, S.H.; Lin, C.C.; Liu, Y.W.; Yong, C.C.; Yang, C.H.; Lin, T.S.; Chiang, Y.C.; et al. Living donor liver transplantation for biliary atresia: A single center experience with the first 100 cases. Am. J. Transplant. 2006, 6, 2672–2679. [Google Scholar] [CrossRef]
- Starzl, T.E.; Iwatsuki, S.; Van Thiel, D.H.; Carlton Gartner, J.; Zitelli, B.J.; Jeffrey Malatack, J.; Schade, R.R.; Shaw, B.W., Jr.; Hakala, T.R.; Rosenthal, J.T.; et al. Evolution of liver transplantation. Hepatology 1982, 2, 614S–636S. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Couto, A.M.; Caldas, C.P.; Castro, E.A.B. Family caregiver of older adults and cultural care in nursing care. Rev. Bras. Enferm. 2018, 71, 959–966. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef]
- Coolidge, F.L.; Segal, D.L.; Hook, J.N.; Stewart, S. Personality disorders and coping among anxious older adults. J. Anxiety Disord. 2000, 14, 157–172. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. Post traumatic growth: Conceptual foundations and empirical evidence. Psychol. Inquiry. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Lindstrom, C.M.; Cann, A.; Calhoun, L.G.; Tedeschi, R.G. The relationship of core belief challenge, rumination, disclosure, and sociocultural elements to posttraumatic growth. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 50. [Google Scholar] [CrossRef]
- Chu, L.; Kao, H.S.R. The Moderation of Meditation Experience and Emotional Intelligence on the Relationship between Perceived Stress and Negative Mental Health. Chin. J. Psychol. 2005, 47, 157–179. [Google Scholar] [CrossRef]
- Tzeng, H.-J.; Ho, C.-C.; Tsai, M.-C. The Relationships of Coping Behaviors with Bereavement, Attachment Styles, and Anticipatory Mourning Reactions among Families of Terminal Cancer Patients. J. Ment. Health 2010, 23, 563–585. [Google Scholar] [CrossRef]
- Ho, S.M.; Chan, C.L.; Ho, R.T. Posttraumatic growth in Chinese cancer survivors. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2004, 13, 377–389. [Google Scholar] [CrossRef]
- Nouzari, R.; Najafi, S.S.; Momennasab, M. Post-Traumatic Growth among Family Caregivers of Cancer Patients and Its Association with Social Support and Hope. Int. J. Community Based Nurs. Midwifery 2019, 7, 319. [Google Scholar] [CrossRef]
- Akbar, Z.; Witruk, E. Coping mediates the relationship between gender and posttraumatic growth. Procedia-Soc. Behav. Sci. 2016, 217, 1036–1043. [Google Scholar] [CrossRef]
- Zwahlen, D.; Hagenbuch, N.; Carley, M.I.; Jenewein, J.; Buchi, S. Posttraumatic growth in cancer patients and partners—Effects of role, gender and the dyad on couples’ posttraumatic growth experience. Psycho-Oncology 2010, 19, 12–20. [Google Scholar] [CrossRef]
- Hsieh, Y.-L. The Representation and Reality in Life Experience of Married Women. J. Contemp. Soc. Work 2014, 6, 1–49. Available online: https://reurl.cc/kd8EpG (accessed on 1 March 2022).
- National Alliance for Caregiving and AARP. Caregiving in the U.S. 2020—AARP Research Report. Available online: https://www.caregiving.org/wp-content/uploads/2021/01/full-report-caregiving-in-the-united-states-01-21 (accessed on 22 June 2021).
- Nguyen, D.L.; Chao, D.; Ma, G.; Morgan, T. Quality of life and factors predictive of burden among primary caregivers of chronic liver disease patients. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2015, 28, 124. [Google Scholar]
- Hsh, W.-C.; Lin, J.-H.; Lin, M.-H.; Hsh, H.-C.; Shih, W.-M. Quality of Life of Primary Caregivers of Liver Cirrhosis Patients and Related Factors. J. Nurs. 2019, 66, 60–69. [Google Scholar] [CrossRef]
- Liu, Y.Z.; Wang, Y.X.; Jiang, C.L. Inflammation: The common pathway of stress-related diseases. Front. Hum. Neurosci. 2017, 11, 316. [Google Scholar] [CrossRef] [PubMed]
- Pinyopornpanish, M.; Pinyopornpanish, K.; Soontornpun, A.; Tanprawate, S.; Nadsasarn, A.; Wongpakaran, N.; Wongpakaran, T. Perceived stress and depressive symptoms not neuropsychiatric symptoms predict caregiver burden in Alzheimer’s disease: A cross-sectional study. BMC Geriatr. 2021, 21, 180. [Google Scholar] [CrossRef] [PubMed]
- Ott, C.H.; Sanders, S.; Kelber, S.T. Grief and personal growth experience of spouses and adult-child caregivers of individuals with Alzheimer’s disease and related dementias. Gerontologist 2007, 47, 798–809. [Google Scholar] [CrossRef]
- Hamama, L.; Sharon, M. Posttraumatic growth and subjective well-being among caregivers of chronic patients: A preliminary study. J. Happiness Stud. 2013, 14, 1717–1737. [Google Scholar] [CrossRef]
- Lin, I.F.; Wu, H.S. Patterns of coping among family caregivers of frail older adults. Res. Aging 2014, 5, 603–624. [Google Scholar] [CrossRef]
- Yuan, Q.; Wang, P.; Tan, T.H.; Devi, F.; Poremski, D.; Magadi, H.; Subramaniam, M. Coping patterns among primary informal dementia caregivers in Singapore and its impact on caregivers—Implications of a latent class analysis. Gerontologist 2020, 5, 680–692. [Google Scholar] [CrossRef]

{kind=link}
| Item | n | % | Mean | SD | t/F | Scheffe |
|---|---|---|---|---|---|---|
| Sex | 5.03 *** | |||||
| Male | 26 | 31.0 | 32.04 | 14.38 | ||
| Female | 58 | 69.0 | 46.48 | 11.06 | ||
| Age | 45.32 | 13.02 | −1.55 | |||
| 20–49 | 48 | 57.1 | 40.00 | 13.83 | ||
| ≥50 | 36 | 42.9 | 44.69 | 13.57 | ||
| Education | 0.78 | |||||
| ≤High school | 42 | 50.0 | 43.19 | 13.41 | ||
| ≥College | 42 | 50.0 | 40.83 | 14.32 | ||
| Marriage | −1.43 | |||||
| Single | 21 | 25.0 | 38.29 | 13.06 | ||
| Married | 63 | 75.0 | 43.25 | 13.96 | ||
| Religion | 0.30 | |||||
| Yes | 61 | 72.6 | 42.30 | 14.54 | ||
| No | 23 | 27.4 | 41.26 | 12.04 | ||
| Caregiver | 5.40 ** | ③ > ①,② | ||||
| ① Spouse | 39 | 46.4 | 44.85 | 12.345 | ||
| ② Children | 22 | 26.2 | 32.82 | 15.083 | ||
| ③ Parents | 12 | 14.3 | 48.33 | 9.365 | ||
| ④ Others | 11 | 13.1 | 43.45 | 12.972 | ||
| Occupation before caring | −0.58 | |||||
| Yes | 57 | 67.9 | 41.40 | 13.86 | ||
| No | 27 | 32.1 | 43.30 | 13.967 | ||
| Household income | 2.08 | |||||
| ≤USD 21,000 | 35 | 41.7 | 39.77 | 15.564 | ||
| ≥USD 21,000 < 28,000 | 32 | 38.1 | 41.34 | 14.086 | ||
| ③ ≥ 28,000 | 17 | 20.2 | 47.88 | 6.744 | ||
| Chronic disease | −2.01 | |||||
| Yes | 25 | 29.8 | 37.44 | 14.73 | ||
| No | 59 | 70.2 | 43.95 | 13.09 | ||
| Caring time | 5.71 | 5.68 | −1.01 | |||
| 0–12 months | 70 | 83.3 | 41.33 | 13.77 | ||
| ≥12 months | 14 | 16.7 | 45.43 | 14.19 | ||
| Organ source | 0.01 | |||||
| Relatives | 55 | 65.5 | 42.02 | 13.79 | ||
| Cadaveric | 29 | 34.5 | 42.00 | 14.17 |
| Item | Range | Mean | SD | Standardized Score a | Order |
|---|---|---|---|---|---|
| Perception stress | 0–56 | 27.27 | 6.63 | ||
| Coping strategies | |||||
| Problem-oriented | 6–24 | 20.51 | 3.34 | 85.46 | 1 |
| Emotion-oriented | 10–40 | 31.02 | 4.96 | 77.55 | 2 |
| Dysfunctional | 12–48 | 23.07 | 4.99 | 48.06 | 3 |
| Post-traumatic growth | 0–75 | 42.01 | 13.84 | ||
| Self | 0–35 | 19.70 | 6.57 | 56.29 | 3 |
| Interpersonal | 0–15 | 8.83 | 3.21 | 58.87 | 2 |
| Life direction | 0–10 | 5.98 | 2.54 | 59.80 | 1 |
| Spirituality | 0–15 | 7.50 | 3.61 | 50.00 | 4 |
| Item | Female | Caregiver- Children | Perceived Stress | Problem- Oriented Coping | Emotion- Oriented Coping | Dysfunctional Coping |
|---|---|---|---|---|---|---|
| Post-traumatic growth | 0.485 * | −0.218 * | 0.338 ** | 0.369 ** | 0.449 ** | 0.041 |
| Self | 0.438 ** | −0.254 * | 0.365 ** | 0.362 ** | 0.384 ** | 0.056 |
| Interpersonal | 0.433 ** | −0.148 | 0.261 ** | 0.315 ** | 0.431 ** | 0.011 |
| Life direction | 0.300 ** | −0.240 * | 0.282 ** | 0.274 * | 0.262 * | −0.066 |
| Spirituality | 0.467 ** | −0.073 | 0.198 | 0.281 ** | 0.454 ** | 0.092 |
| Item | Effect | Standardized Estimate | Bootstrapping 95% CI | Z |
|---|---|---|---|---|
| Total indirect effect | 0.30 | 0.19 | [−0.02, 0.70] | |
| Problem-oriented | −0.01 | 0.20 | [−0.37, 0.42] | 2.16 |
| Emotion-oriented | 0.35 | 0.15 | [0.08, 0.65] | 3.35 *** |
| Dysfunctional-oriented | −0.04 | 0.06 | [−0.17, 0.06] | 0.10 |
| Model | Variables | R2 | Adjusted R2 | F | B | S.E. | β | t |
|---|---|---|---|---|---|---|---|---|
| 1 | Gender | 0.24 | 0.23 | 25.29 | 14.44 | 2.87 | 0.49 | 5.03 *** |
| 2 | Perceived stress | 0.32 | 0.30 | 18.68 | 0.59 | 0.19 | 0.29 | 3.08 ** |
| 3 | Caregiver-children | 0.36 | 0.34 | 15.21 | −7.34 | 3.00 | −0.24 | −2.44 * |
| 4 | Emotion-oriented coping | 0.41 | 0.38 | 13.71 | 0.72 | 0.29 | 0.26 | 2.50 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Lee, W.-C.; Kao, Y.-Y.; Chen, L.-C.; Ho, L.-H.; Shih, W.-M. The Post-Traumatic Growth of Primary Caregivers of Patients after Liver Transplantation. Healthcare 2022, 10, 1617. https://doi.org/10.3390/healthcare10091617
Chen Y-H, Lee W-C, Kao Y-Y, Chen L-C, Ho L-H, Shih W-M. The Post-Traumatic Growth of Primary Caregivers of Patients after Liver Transplantation. Healthcare. 2022; 10(9):1617. https://doi.org/10.3390/healthcare10091617
Chicago/Turabian StyleChen, Ya-Hui, Wei-Chen Lee, Yu-Yi Kao, Li-Chen Chen, Lun-Hui Ho, and Whei-Mei Shih. 2022. "The Post-Traumatic Growth of Primary Caregivers of Patients after Liver Transplantation" Healthcare 10, no. 9: 1617. https://doi.org/10.3390/healthcare10091617
APA StyleChen, Y.-H., Lee, W.-C., Kao, Y.-Y., Chen, L.-C., Ho, L.-H., & Shih, W.-M. (2022). The Post-Traumatic Growth of Primary Caregivers of Patients after Liver Transplantation. Healthcare, 10(9), 1617. https://doi.org/10.3390/healthcare10091617