
The Role of Antigen Carbohydrate 125 in Modulating Soluble ST2: Prognostic-Related Effects in Acute Heart Failure

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Biomarkers Assessment
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Baseline Characteristics Across CA125 and sST2 Categories
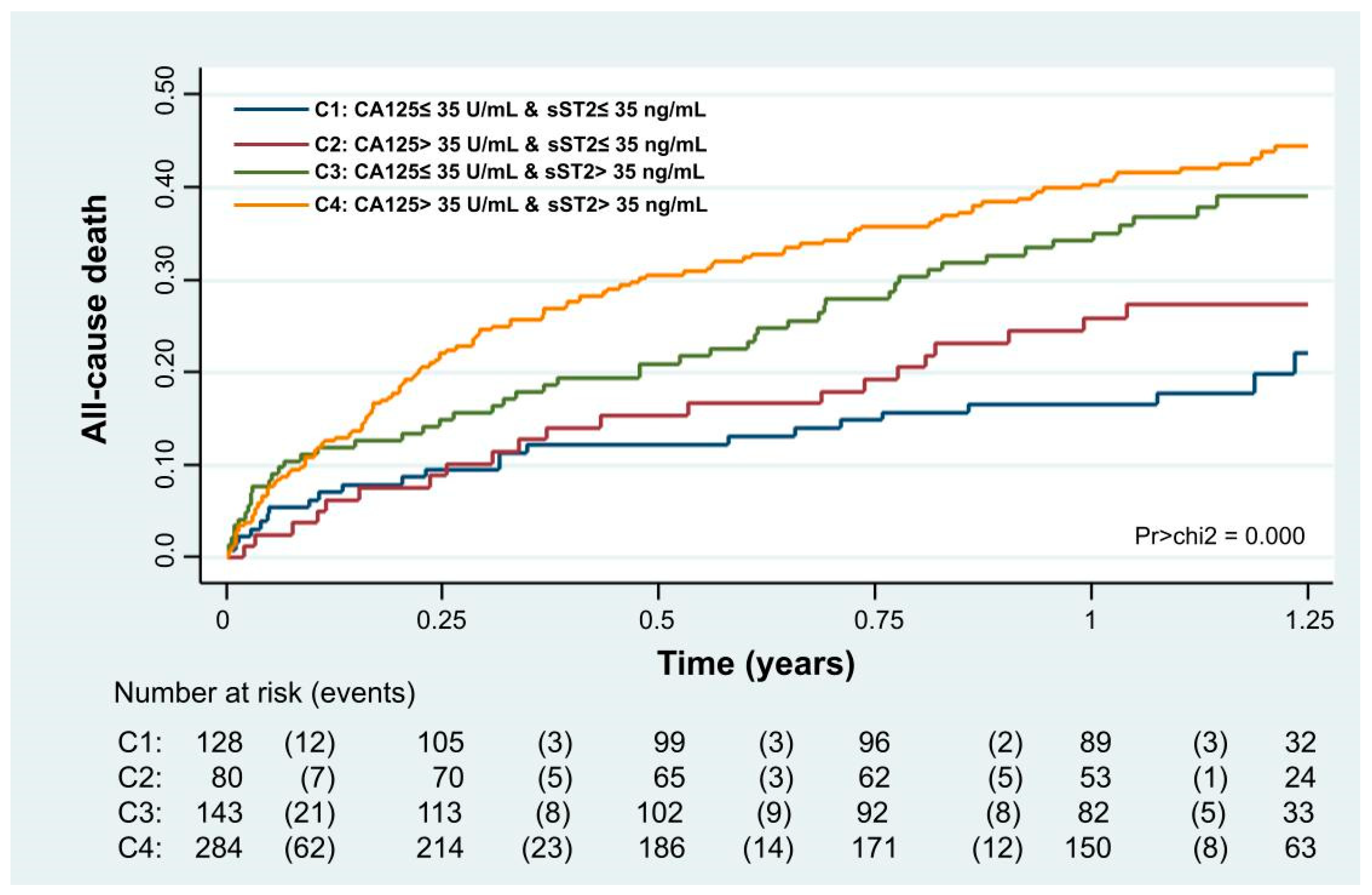
3.3. Adverse Clinical Events
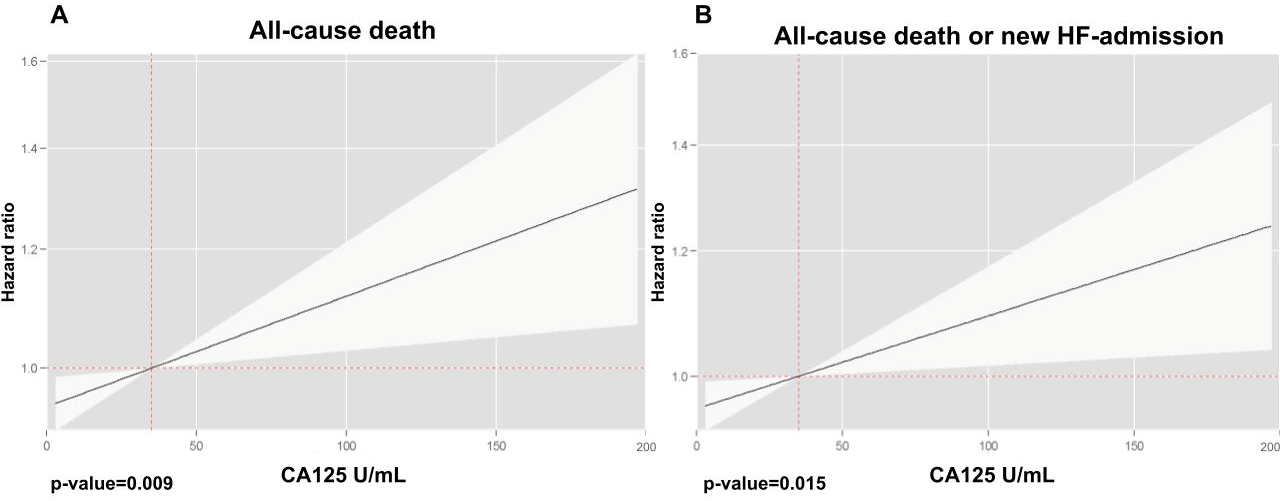
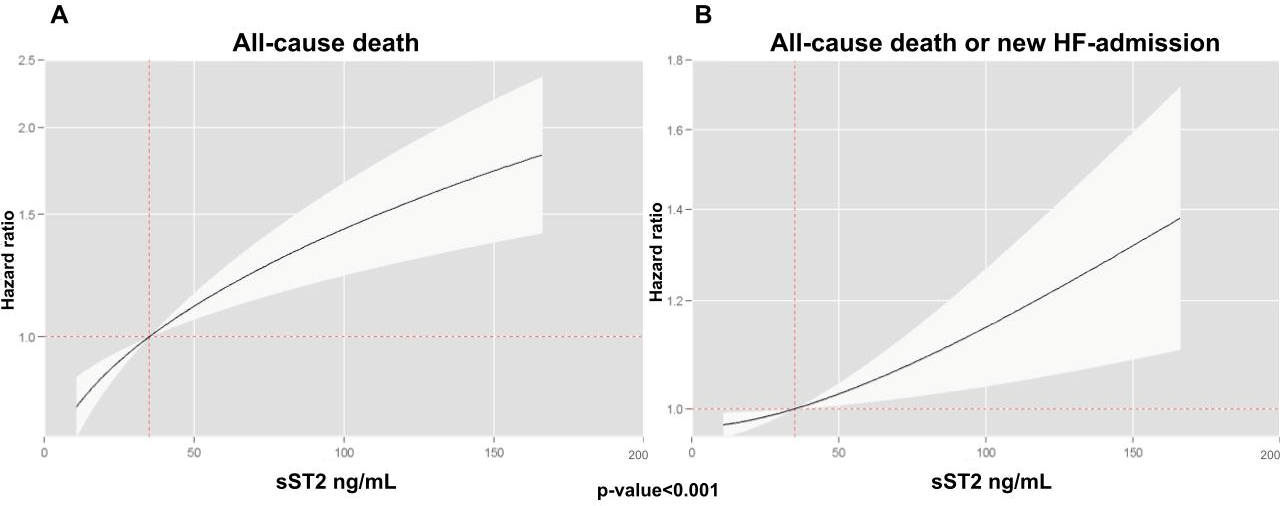
3.4. Relationship Between CA125 and sST2 as Main Terms with Adverse Clinical Events
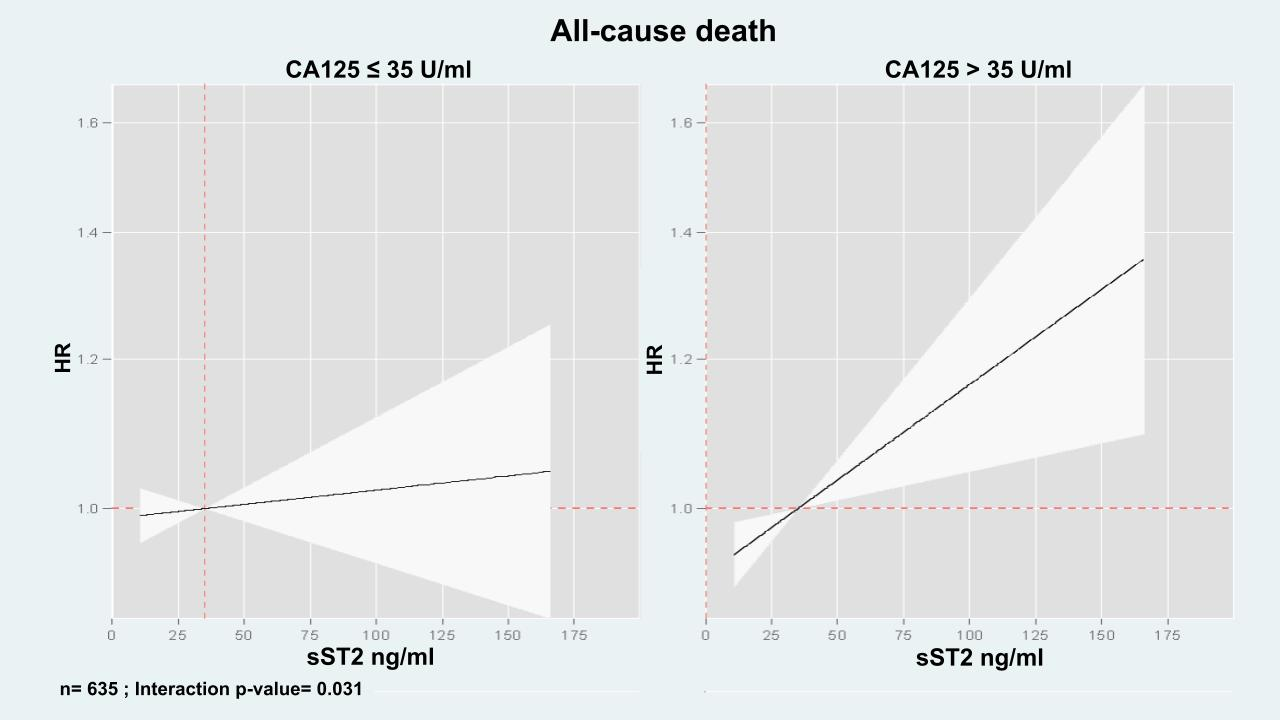
3.5. The Modifying Prognostic Role of sST2 Across CA125
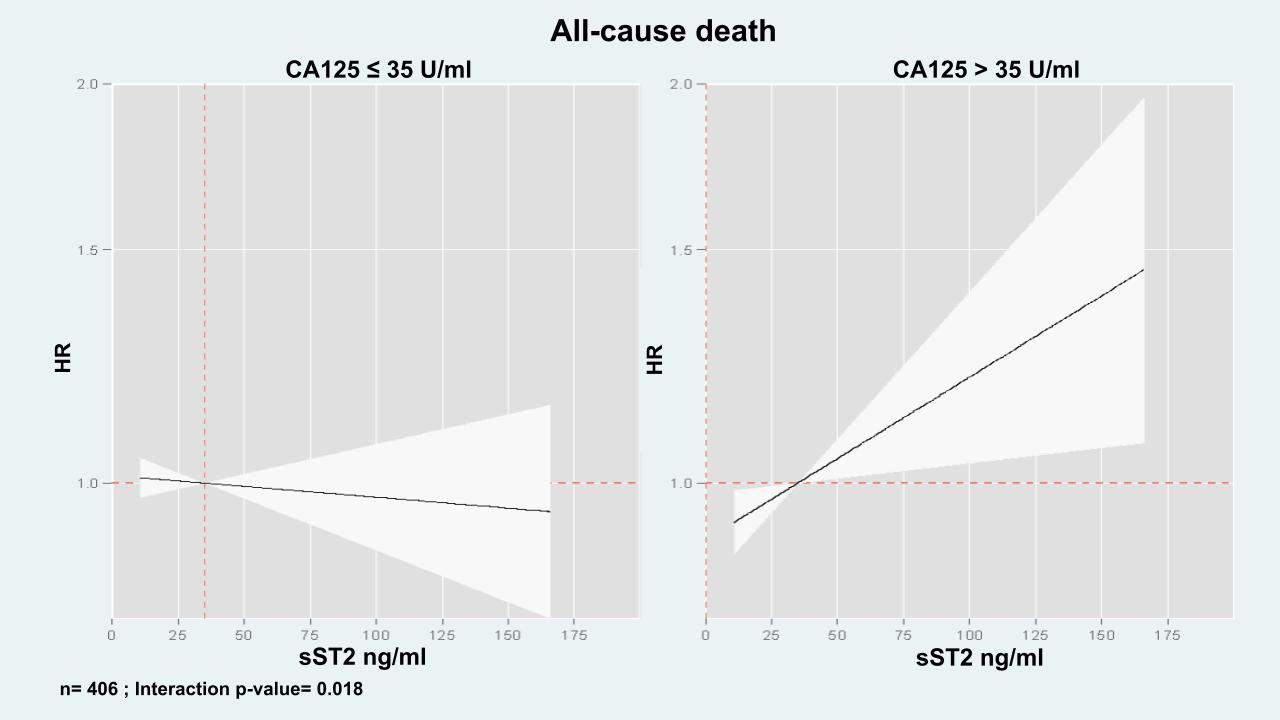
3.5.1. All Cause-Death
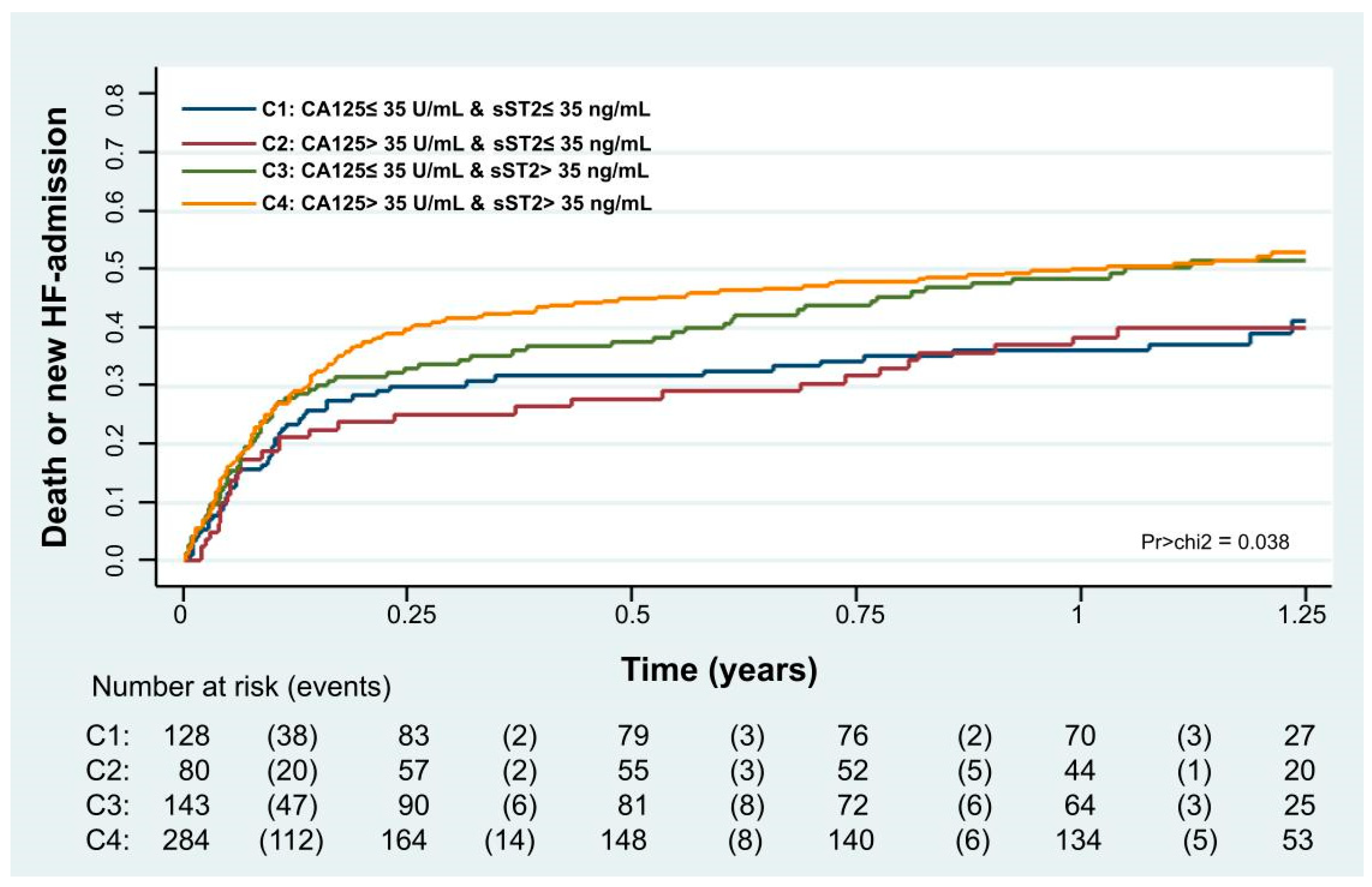
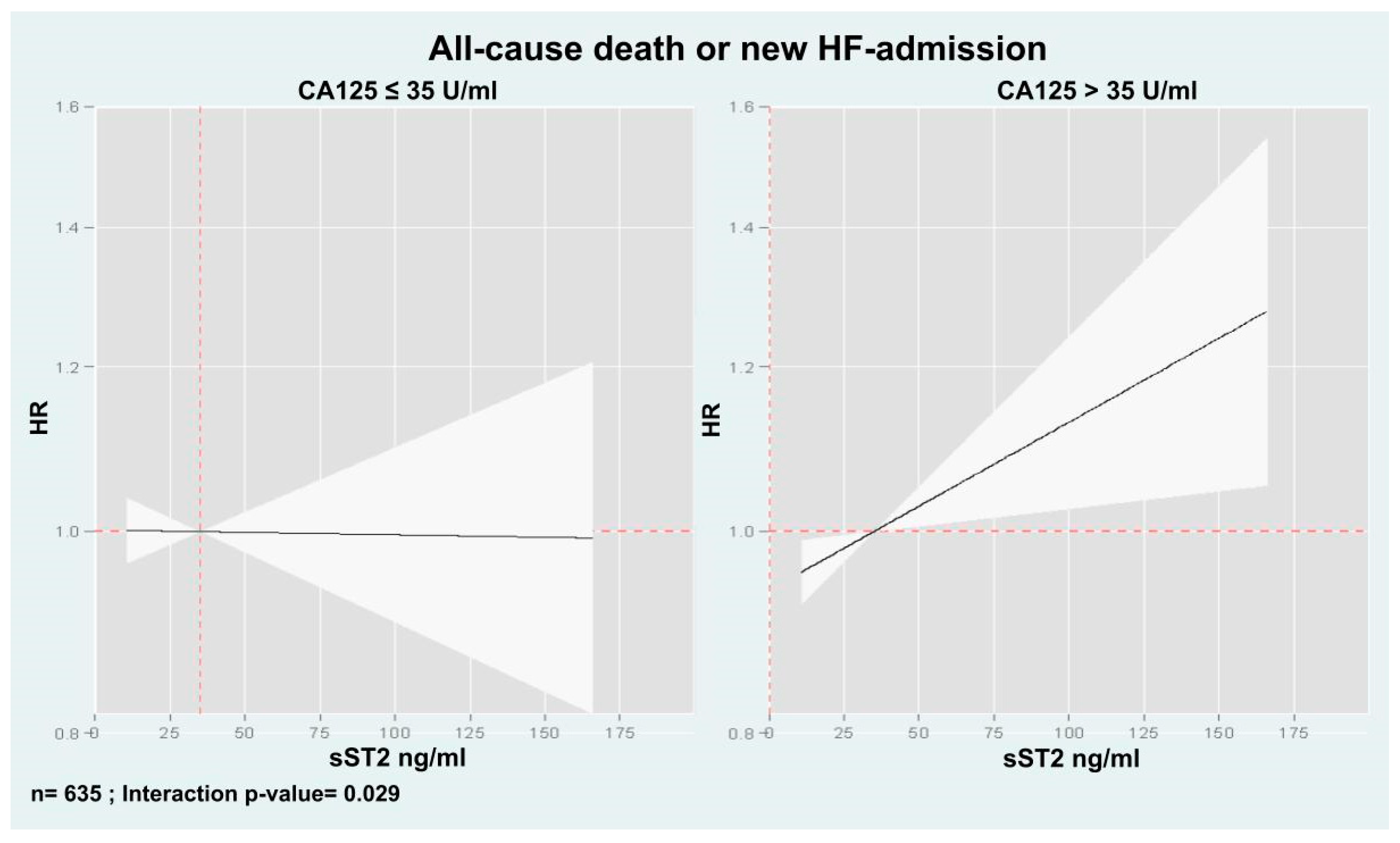
3.5.2. Combination of Death or New HF Admission
4. Discussion
4.1. Structure and Pathophysiology of MUC16 (CA125)
4.2. Relationship of CA125 with Pro-Inflammatory Pathways and sST2
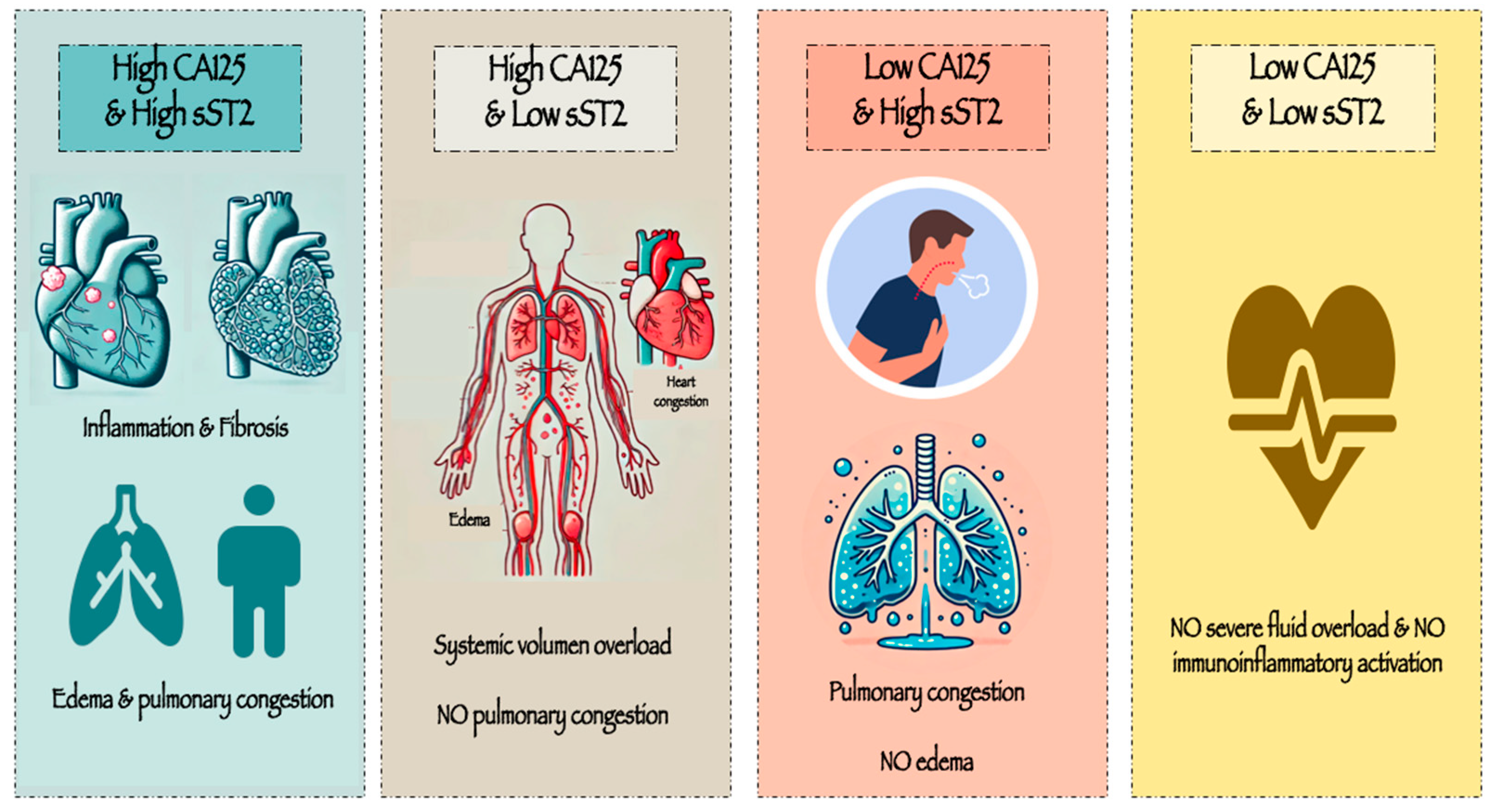
4.3. Differential Effects of sST2 Across CA125 Levels
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AHF | Acute heart failure |
| ANOVA | Analysis of variance |
| CA125 | Antigen carbohydrate 125 |
| CTD | C-terminal domain |
| CV | Cardiovascular |
| EAHFE | Epidemiology of Acute Heart Failure in Spanish Emergency Departments |
| EDs | Emergency departments |
| EMT | Epithelial-to-mesenchymal transition |
| Gal-1 | Galectin-1 |
| HF | Heart failure |
| IL-33 | Interleukin-33 |
| IQR | Interquartile range |
| JNK | c-Jun N-terminal kinase |
| LVEF | Left ventricular ejection fraction |
| MUC16 | Mucin 16 |
| NYHA | New York Heart Association |
| P-Y | Person-years |
| sST2 | Soluble Suppression of Tumorigenicity 2 |
| ST2L | Membrane-bound ST2 |
| Th0 | T-lymphocytes |
| TNF | Tumor necrosis factor |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | HR | CI | p-Value |
|---|---|---|---|
| Age, per ten-year increase | 1.20 | 1.01–1.43 | 0.046 |
| Men | 1.30 | 0.96–1.77 | 0.087 |
| Prior known HF | 1.28 | 0.93–1.53 | 0.184 |
| NYHA class prior to admission, per increase in 1 category | 1.10 | 0.94–1.27 | 0.185 |
| Atrial fibrillation | 1.23 | 0.96–1.76 | 0.159 |
| Ischemic heart disease | 1.28 | 0.93–1.78 | 0.133 |
| Barthel index, per increase of 1 point | 0.98 | 0.98–0.99 | <0.001 |
| Heart rate, per increase of 1 bpm | 1.02 | 1.01–1.04 | 0.031 |
| SBP, per increase of 10 mmHg | 0.95 | 0.89–0.99 | 0.041 |
| Hemoglobin, per increase of 1 g/dL | 0.95 | 0.89–1.01 | 0.149 |
| eGFR, per increase of 10 mL/min/1.73 m2 | 0.95 | 0.92–0.98 | 0.002 |
| Orthopnea | 1.24 | 0.93–1.56 | 0.195 |
| Crackles | 0.90 | 0.67–1.22 | 0.493 |
| Paroxysmal nocturnal dyspnea | 0.95 | 0.67–1.34 | 0.760 |
| Third heart sound | 1.99 | 0.90–4.44 | 0.092 |
| Jugular venous distension | 1.12 | 0.80–1.59 | 0.515 |
| Pleural effusion | 1.10 | 0.80–1.50 | 0.534 |
| Peripheral edemas | 0.80 | 0.59–1.10 | 0.176 |
| Variable | HR | CI | p-Value |
|---|---|---|---|
| Age, per ten-year increase | 1.18 | 1.01–1.37 | 0.038 |
| Men | 1.19 | 0.92–1.54 | 0.190 |
| Prior known HF | 1.23 | 0.94–1.61 | 0.126 |
| NYHA class prior to admission, per increase in 1 category | 1.36 | 0.95–1.87 | 0.120 |
| Atrial fibrillation | 0.91 | 0.70–1.15 | 0.430 |
| Ischemic heart disease | 1.39 | 1.05–1.83 | 0.023 |
| Barthel index, per increase of 1 point | 0.99 | 0.98–0.99 | 0.001 |
| Heart rate, per increase of 1 bpm | 1.00 | 1.00–1.01 | 0.161 |
| SBP, per increase of 10 mmHg | 0.95 | 0.91–0.99 | 0.046 |
| Hemoglobin, per increase of 1 g/dL | 0.94 | 0.89–1.00 | 0.037 |
| eGFR, per increase of 10 mL/min/1.73 m2 | 0.98 | 0.95–0.99 | 0.045 |
| Orthopnea | 1.15 | 0.88–1.49 | 0.300 |
| Crackles | 1.00 | 0.77–1.30 | 0.995 |
| Paroxysmal nocturnal dyspnea | 0.87 | 0.65–1.17 | 0.363 |
| Third heart sound | 1.19 | 0.53–2.65 | 0.675 |
| Jugular venous distension | 1.07 | 0.80–1.43 | 0.671 |
| Pleural effusion | 1.10 | 0.85–1.43 | 0.471 |
| Peripheral edemas | 0.99 | 0.76–1.30 | 0.962 |
References
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Primers 2020, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Kurmani, S.; Squire, I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr. Heart Fail. Rep. 2017, 14, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Riccardi, M.; Myhre, P.L.; Zelniker, T.A.; Metra, M.; Januzzi, J.L.; Inciardi, R.M. Soluble ST2 in Heart Failure: A Clinical Role beyond B-Type Natriuretic Peptide. J. Cardiovasc. Dev. Dis. 2023, 10, 468. [Google Scholar] [CrossRef]
- Wang, Z.; Pan, X.; Xu, H.; Wu, Y.; Jia, X.; Fang, Y.; Lu, Y.; Xu, Y.; Zhang, J.; Su, Y. Serum Soluble ST2 Is a Valuable Prognostic Biomarker in Patients With Acute Heart Failure. Front. Cardiovasc. Med. 2022, 9, 812654. [Google Scholar] [CrossRef]
- Kumric, M.; Kurir, T.T.; Bozic, J.; Glavas, D.; Saric, T.; Marcelius, B.; D’Amario, D.; Borovac, J.A. Carbohydrate Antigen 125: A Biomarker at the Crossroads of Congestion and Inflammation in Heart Failure. Card. Fail. Rev. 2021, 7, e19. [Google Scholar] [CrossRef]
- Giamougiannis, P.; Martin-Hirsch, P.L.; Martin, F.L. The evolving role of MUC16 (CA125) in the transformation of ovarian cells and the progression of neoplasia. Carcinogenesis 2021, 42, 327–343. [Google Scholar] [CrossRef]
- Núñez, J.; Rabinovich, G.A.; Sandino, J.; Mainar, L.; Palau, P.; Santas, E.; Villanueva, M.P.; Núñez, E.; Bodí, V.; Chorro, F.J.; et al. Prognostic Value of the Interaction between Galectin-3 and Antigen Carbohydrate 125 in Acute Heart Failure. PLoS ONE 2015, 10, e0122360. [Google Scholar] [CrossRef]
- Pusceddu, I.; Dieplinger, B.; Mueller, T. ST2 and the ST2/IL-33 signalling pathway-biochemistry and pathophysiology in animal models and humans. Clin. Chim. Acta 2019, 495, 493–500. [Google Scholar] [CrossRef]
- Revuelta-López, E.; de la Espriella, R.; Miñana, G.; Santas, E.; Villar, S.; Sanchis, J.; Bayés-Genís, A.; Núñez, J. The modulating effect of circulating carbohydrate antigen 125 on ST2 and long-term recurrent morbidity burden. Sci. Rep. 2025, 15, 1905. [Google Scholar] [CrossRef]
- Llorens, P.; Escoda, R.; Miró, Ò.; Herrero-Puente, P.; Martín-Sánchez, F.J.; Jacob, J.; Garrido, J.M.; Pérez-Durá, M.J.; Gil, C.; Fuentes, M.; et al. Characteristics and clinical course of patients with acute heart failure and the therapeutic measures applied in Spanish emergency departments: Based on the EAHFE registry (Epidemiology of Acute Heart Failure in Emergency Departments). Emergencias 2015, 27, 11–22. [Google Scholar]
- The ICA-SEMES Research Group; Llorens, P.; Javaloyes, P.; Martín-Sánchez, F.J.; Jacob, J.; Herrero-Puente, P.; Gil, V.; Garrido, J.M.; Salvo, E.; Fuentes, M.; et al. Time trends in characteristics, clinical course, and outcomes of 13,791 patients with acute heart failure. Clin. Res. Cardiol. 2018, 107, 897–913. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Bueno, H.; Gil, V.; Jacob, J.; Martín-Sánchez, F.J.; Llorens, P.; Puente, P.H.; Alquézar-Arbé, A.; Raposeiras-Roubín, S.; López-Díez, M.P.; et al. MEESSI-AHF risk score performance to predict multiple post-index event and post-discharge short-term outcomes. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Eiras, S.; de la Espriella, R.; Fu, X.; Iglesias-Álvarez, D.; Basdas, R.; Núñez-Caamaño, J.R.; Martínez-Cereijo, J.M.; Reija, L.; Fernández, A.L.; Sánchez-López, D.; et al. Carbohydrate antigen 125 on epicardial fat and its association with local inflammation and fibrosis-related markers. J. Transl. Med. 2024, 22, 619. [Google Scholar] [CrossRef]
- Núñez, J.; de la Espriella, R.; Miñana, G.; Santas, E.; Llácer, P.; Núñez, E.; Palau, P.; Bodí, V.; Chorro, F.J.; Sanchis, J.; et al. Antigen carbohydrate 125 as a biomarker in heart failure: A narrative review. Eur. J. Heart Fail. 2021, 23, 1445–1457. [Google Scholar] [CrossRef]
- Thériault, C.; Pinard, M.; Comamala, M.; Migneault, M.; Beaudin, J.; Matte, I.; Boivin, M.; Piché, A.; Rancourt, C. MUC16 (CA125) regulates epithelial ovarian cancer cell growth, tumorigenesis and metastasis. Gynecol. Oncol. 2011, 121, 434–443. [Google Scholar] [CrossRef]
- Marimuthu, S.; Lakshmanan, I.; Muniyan, S.; Gautam, S.K.; Nimmakayala, R.K.; Rauth, S.; Atri, P.; Shah, A.; Bhyravbhatla, N.; Mallya, K.; et al. MUC16 Promotes Liver Metastasis of Pancreatic Ductal Adenocarcinoma by Upregulating NRP2-Associated Cell Adhesion. Mol. Cancer Res. 2022, 20, 1208–1221. [Google Scholar] [CrossRef]
- Suarez-Carmona, M.; Lesage, J.; Cataldo, D.; Gilles, C. EMT and inflammation: Inseparable actors of cancer progression. Mol. Oncol. 2017, 11, 805–823. [Google Scholar] [CrossRef]
- Ballester, B.; Milara, J.; Montero, P.; Cortijo, J. MUC16 Is Overexpressed in Idiopathic Pulmonary Fibrosis and Induces Fibrotic Responses Mediated by Transforming Growth Factor-β1 Canonical Pathway. Int. J. Mol. Sci. 2021, 22, 6502. [Google Scholar] [CrossRef]
- Miñana, G.; Núñez, J.; Sanchis, J.; Bodí, V.; Núñez, E.; Llàcer, A. CA125 and immunoinflammatory activity in acute heart failure. Int. J. Cardiol. 2010, 145, 547–548. [Google Scholar] [CrossRef]
- Núñez, J.; Bayés-Genís, A.; Revuelta-López, E.; ter Maaten, J.M.; Miñana, G.; Barallat, J.; Cserkóová, A.; Bodi, V.; Fernández-Cisnal, A.; Núñez, E.; et al. Clinical Role of CA125 in Worsening Heart Failure: A BIOSTAT-CHF Study Subanalysis. JACC Heart Fail. 2020, 8, 386–397. [Google Scholar] [CrossRef]
- Huang, F.; Chen, J.; Liu, Y.; Zhang, K.; Wang, J.; Huang, H. New mechanism of elevated CA125 in heart failure: The mechanical stress and inflammatory stimuli initiate CA125 synthesis. Med. Hypotheses 2012, 79, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xiao, P.; Song, D.; Song, D.; Chen, Z.; Li, H. Growth stimulation expressed gene 2 (ST2): Clinical research and application in the cardiovascular related diseases. Front. Cardiovasc. Med. 2022, 9, 1007450. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Liu, J.; Geng, T. Predictive values of sST2 and IL-33 for heart failure in patients with acute myocardial infarction. Exp. Biol. Med. 2021, 246, 2480–2486. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Paldino, A.; Beltrami, A.P.; Padoan, L.; Iacoviello, M.; Sinagra, G.; Emdin, M.; Maisel, A.S. Cardiac Biomarkers in the Emergency Department: The Role of Soluble ST2 (sST2) in Acute Heart Failure and Acute Coronary Syndrome-There is Meat on the Bone. J. Clin. Med. 2019, 8, 270. [Google Scholar] [CrossRef]
- Homsak, E.; Gruson, D. Soluble ST2: A complex and diverse role in several diseases. Clin. Chim. Acta 2020, 507, 75–87. [Google Scholar] [CrossRef]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the diagnosis and management of heart failure. Heart Fail. Rev. 2022, 27, 625–643. [Google Scholar] [CrossRef]
- Călburean, P.-A.; Lupu, S.; Huțanu, A.; Oprica, M.; Opriș, D.R.; Stan, A.; Scurtu, A.-C.; Aniței, D.; Harpa, M.; Brînzaniuc, K.; et al. Natriuretic peptides and soluble ST2 improves echocardiographic diagnosis of elevated left ventricular filling pressures. Sci. Rep. 2024, 14, 22171. [Google Scholar] [CrossRef]
| Total Cohort (n = 635) | |
|---|---|
| Demographics and Medical History Data | |
| Age, years | 82.4 ± 10 |
| Women, n (%) | 339 (53.4) |
| Hypertension, n (%) | 534 (84.1) |
| Diabetes Mellitus, n (%) | 248 (39.1) |
| Dyslipemia, n (%) | 276 (43.5) |
| LVEF, % | 52.1 ± 13.9 |
| Ischemic heart disease, n (%) | 161 (25.4) |
| Valvular heart disease, n (%) | 189 (29.8) |
| Chronic kidney disease, n (%) | 188 (29.6) |
| Stroke, n (%) | 82 (12.9) |
| Prior history of atrial fibrillation, n (%) | 344 (54.2) |
| Prior history of HF, n (%) | 401 (63.1) |
| COPD, n (%) | 138 (21.7) |
| PAD, n (%) | 59 (9.3) |
| Barthel index | 80.6 ± 24.5 |
| MEESSI Score | −2.8 ± 1.1 |
| Dyspnea, n (%) | 602 (94.8) |
| Orthopnea, n (%) | 341 (53.7) |
| Pallor, n (%) | 75 (11.8) |
| Low output, n (%) | 97 (15.3) |
| Peripheral edema, n (%) | 435 (68.5) |
| Pleural effusion, n (%) | 191 (30.1) |
| Jugular venous distention, n (%) | 140 (22.0) |
| Paroxysmal nocturnal dyspnea, n (%) | 175 (27.6) |
| Cardiomegaly, n (%) | 311 (49.0) |
| Crackles, n (%) | 422 (66.5) |
| Third heart sound, n (%) | 13 (2.0) |
| NYHA Episode, n (%) | |
| 1 | 6 (0.9) |
| 2 | 69 (10.9) |
| 3 | 307 (48.3) |
| 4 | 253 (39.8) |
| Vital signs | |
| Heart rate, bpm | 87.9 ± 23.7 |
| SBP, mmHg | 138.2 ± 26.8 |
| DBP, mmHg | 75.8 ± 17.5 |
| Heart rate, bpm | 87.9 ± 23.7 |
| Electrocardiogram | |
| Atrial fibrillation, n (%) | 317 (49.9) |
| Laboratory | |
| Hemoglobin, g/dL 1 | 12 (10.6–13.4) |
| Hematocrit (%) | 37.3 ± 3.3 |
| Leucocyte count, 103 cells/mL | 8914.6 ± 6117.5 |
| Creatinine, mg/dL 1 | 1.2 (0.9–1.6) |
| Sodium, mEq/L | 139.3 ± 4.8 |
| NT-proBNP, pg/mL 1 | 4207 (2280–8421) |
| CRP, mg/L | 23.6 ± 201.8 |
| CA125, U/mL 1 | 44 (19–94) |
| sST2, ng/mL 1 | 49.2 (27.3–88.5) |
| CA125 > 35 U/mL, n (%) | 364 (57.3) |
| sST2 > 35 ng/mL, n (%) | 427 (67.2) |
| Chronic treatment | |
| Beta-blockers, n (%) | 277 (43.6) |
| ACEI, n (%) | 191 (30.1) |
| ARB, n (%) | 162 (25.5) |
| Aldosterone receptor blocker, n (%) | 95 (15) |
| Loop diuretics, n (%) | 419 (66) |
| Thiazides, n (%) | 96 (15.1) |
| Gategory 1 CA125 ≤ 35 and sST2 ≤ 35 (n = 128) | Category 2 CA125 > 35 and sST2 ≤ 35 (n = 80) | Category 3 CA125 ≤ 35 and sST2 > 35 (n = 143) | Category 4 CA125 > 35 and sST2 > 35 (n = 284) | p-Value | |
|---|---|---|---|---|---|
| Demographics and medical history | |||||
| Age, years | 81.9 ± 9.0 | 80.0 ± 10.9 | 84.0 ± 8.6 | 82.5 ± 10.6 | 0.029 |
| Women, n (%) | 83 (64.8) | 43 (53.8) | 59 (41.3) | 154 (54.2) | 0.002 |
| Hypertension, n (%) | 115 (89.8) | 69 (86.3) | 122 (85.3) | 228 (80.3) | 0.083 |
| Diabetes Mellitus, n (%) | 42 (32.8) | 23 (28.8) | 62 (43.4) | 121 (42.6) | 0.041 |
| Dyslipemia, n (%) | 53 (41.4) | 32 (40.0) | 70 (49.0) | 121 (42.6) | 0.485 |
| LVEF, % | 56.8 ± 13.2 | 56.5 ± 13.3 | 51.4 ± 13.9 | 49.2 ± 13.6 | <0.001 |
| Ischemic heart disease, n (%) | 30 (23.4) | 18 (22.5) | 40 (28.0) | 73 (25.7) | 0.770 |
| Valvular heart disease, n (%) | 40 (31.3) | 24 (30.0) | 36 (25.2) | 89 (31.3) | 0.590 |
| Chronic kidney disease, n (%) | 30 (23.4) | 17 (21.3) | 47 (32.9) | 94 (33.1) | 0.060 |
| Stroke, n (%) | 21 (16.4) | 5 (6.3) | 22 (15.4) | 34 (12) | 0.136 |
| Prior history of atrial fibrillation, n (%) | 73 (57.0) | 50 (62.5) | 66 (46.2) | 155 (54.6) | 0.095 |
| Prior history of HF, n (%) | 89 (69.5) | 51 (63.7) | 77 (53.8) | 184 (64.8) | 0.048 |
| COPD, n (%) | 28 (21.9) | 16 (20.0) | 35 (24.5) | 59 (20.8) | 0.819 |
| PAD, n (%) | 10 (7.8%) | 6 (7.5%) | 14 (9.8%) | 29 (10.2%) | 0.810 |
| Barthel index | 82.4 ± 23.5 | 86.6 ± 20.4 | 82.2 ± 21.4 | 77.3 ± 26.9 | 0.011 |
| Dyspnea, n (%) | 122 (95.3) | 79 (98.8) | 133 (93.0) | 268 (94.4) | 0.303 |
| Orthopnea, n (%) | 61 (47.7) | 49 (61.3) | 83 (58.0) | 148 (52.1) | 0.168 |
| Pallor, n (%) | 12 (9.4) | 6 (7.5) | 20 (14.0) | 37 (13.0) | 0.360 |
| Low output, n (%) | 13 (10.3) | 7 (8.8) | 29 (20.3) | 48 (16.9) | 0.039 |
| Peripheral edema, n (%) | 79 (61.7) | 54 (67.5) | 101 (70.6) | 201 (70.8) | 0.290 |
| Pleural effusion, n (%) | 29 (22.7) | 27 (33.8) | 34 (23.8) | 101 (35.6) | 0.014 |
| Jugular venous distention, n (%) | 20 (15.6) | 17 (21.3) | 30 (21.0) | 73 (25.7) | 0.144 |
| Paroxysmal nocturnal dyspnea, n (%) | 30 (23.4) | 29 (36.3) | 43 (30.1) | 73 (25.7) | 0.168 |
| Cardiomegaly, n (%) | 60 (46.9) | 40 (50.0) | 63 (44.1) | 148 (52.1) | 0.430 |
| Crackles, n (%) | 85 (66.4) | 52 (65.0) | 91 (63.6) | 194 (68.3) | 0.795 |
| Third heart sound, n (%) | 2 (1.6) | 2 (2.5) | 2 (1.4) | 7 (2.5) | 0.855 |
| NYHA Episode, n (%) | 0.013 | ||||
| 1 | 0 (0.0) | 0 (0.0) | 4 (2.8) | 2 (0.7) | |
| 2 | 15 (11.7) | 17 (21.3) | 10 (7.0) | 27 (9.5) | |
| 3 | 68 (53.1) | 33 (41.3) | 66 (46.2) | 140 (49.3) | |
| 4 | 45 (35.2) | 30 (37.5) | 63 (44.1) | 115 (40.5) | |
| Vital signs | |||||
| Heart rate, bpm | 87.7 ± 23.1 | 91.3 ± 24.1 | 86.5 ± 22.5 | 87.8 ± 24.4 | 0.542 |
| SBP, mmHg | 141.8 ± 26.9 | 140.2 ± 28.4 | 141.6 ± 27.3 | 134.4 ± 25.7 | 0.012 |
| DBP, mmHg | 76.1 ± 15.5 | 76.2 ± 20 | 78.6 ± 17.8 | 74.2 ± 17.3 | 0.099 |
| Electrocardiogram | |||||
| Atrial fibrillation, n (%) | 68 (53.1) | 41 (51.2) | 65 (45.5) | 143 (50.4) | 0.627 |
| Laboratory | |||||
| Hemoglobin, g/dL 1 | 12.3 (11.0–13.6) | 11.9 (10.8–13.5) | 12.0 (10.7–13.2) | 11.8 (10.2–13.4) | 0.202 |
| Hematocrit, % | 38.2 ± 6.6 | 37.6 ± 5.7 | 37.2 ± 5.8 | 36.9 ± 6.4 | 0.239 |
| Leucocyte count, 103 cells/mL | 8058.3 ± 2804.7 | 8120.2 ± 3066.0 | 10,417.3 ± 6827.7 | 8767.7 ± 7254.2 | 0.005 |
| Creatinine, mg/dL 1 | 1.1 (0.8–1.3) | 1.1 (0.8–1.4) | 1.3 (1.0–1.7) | 1.2 (0.9–1.7) | <0.001 |
| Sodium, mEq/L | 139.6 ± 4.2 | 139.6 ± 4.1 | 139.4 ± 4.3 | 139.0 ± 5.5 | 0.576 |
| NT-proBNP, pg/mL 1 | 2827.0 (1386.0–4850.0) | 4343.0 (1729.5–8207.0) | 4380.0 (2484.0–8318.0) | 5515.5 (2974.0–11,317.0) | <0.001 |
| CRP, mg/L | 15.3 ± 37.0 | 16.8 ± 39.4 | 48.4 ± 393.7 | 14.7 ± 46.2 | 0.530 |
| Chronic treatment | |||||
| Beta-blockers, n (%) | 52 (40.6) | 36 (45.0) | 55 (38.5) | 134 (47.2) | 0.315 |
| ACEI, n (%) | 36 (28.1) | 26 (32.5) | 45 (31.5) | 84 (29.6) | 0.892 |
| ARB, n (%) | 44 (34.4) | 17 (21.3) | 40 (28.0) | 61 (21.5) | 0.030 |
| Aldosterone receptor blocker, n (%) | 16 (12.5) | 12 (15.0) | 23 (16.1) | 44 (15.5) | 0.846 |
| Loop diuretics, n (%) | 83 (64.8) | 46 (57.5) | 87 (60.8) | 203 (71.5) | 0.043 |
| Thiazides, n (%) | 27 (21.1) | 15 (18.8) | 21 (14.7) | 33 (11.6) | 0.068 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martí-Martínez, A.; Núñez, J.; López-Escribano, H.; Revuelta-López, E.; Mollar, A.; Peiró, M.; Sanchis, J.; Bayés-Genís, A.; Carratala, A.; Miró, Ò.; et al. The Role of Antigen Carbohydrate 125 in Modulating Soluble ST2: Prognostic-Related Effects in Acute Heart Failure. Biomolecules 2025, 15, 602. https://doi.org/10.3390/biom15040602
Martí-Martínez A, Núñez J, López-Escribano H, Revuelta-López E, Mollar A, Peiró M, Sanchis J, Bayés-Genís A, Carratala A, Miró Ò, et al. The Role of Antigen Carbohydrate 125 in Modulating Soluble ST2: Prognostic-Related Effects in Acute Heart Failure. Biomolecules. 2025; 15(4):602. https://doi.org/10.3390/biom15040602
Chicago/Turabian StyleMartí-Martínez, Arancha, Julio Núñez, Herminio López-Escribano, Elena Revuelta-López, Anna Mollar, Marta Peiró, Juan Sanchis, Antoni Bayés-Genís, Arturo Carratala, Òscar Miró, and et al. 2025. "The Role of Antigen Carbohydrate 125 in Modulating Soluble ST2: Prognostic-Related Effects in Acute Heart Failure" Biomolecules 15, no. 4: 602. https://doi.org/10.3390/biom15040602
APA StyleMartí-Martínez, A., Núñez, J., López-Escribano, H., Revuelta-López, E., Mollar, A., Peiró, M., Sanchis, J., Bayés-Genís, A., Carratala, A., Miró, Ò., Llorens, P., & Herrero-Puente, P. (2025). The Role of Antigen Carbohydrate 125 in Modulating Soluble ST2: Prognostic-Related Effects in Acute Heart Failure. Biomolecules, 15(4), 602. https://doi.org/10.3390/biom15040602