
Metalloproteinases and Hypertrophic Cardiomyopathy: A Systematic Review
 ,
,  ,
,  , ,
, ,  , , , and
, , , and 
Abstract
1. Introduction
2. Material and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Subject of Interest
2.4. Information Sources
2.5. Study Selection and Data Items
2.6. Risk of Bias in Individual Studies
3. Results
3.1. Included Studies
3.2. Excluded Studies
3.3. Main Findings
3.4. Risk of Bias and Study Quality
4. Discussion
4.1. Matrix Metalloproteinases and Their Role in Cardiac Tissue
4.2. Cardiac Fibrosis and Matrix Metalloproteinases
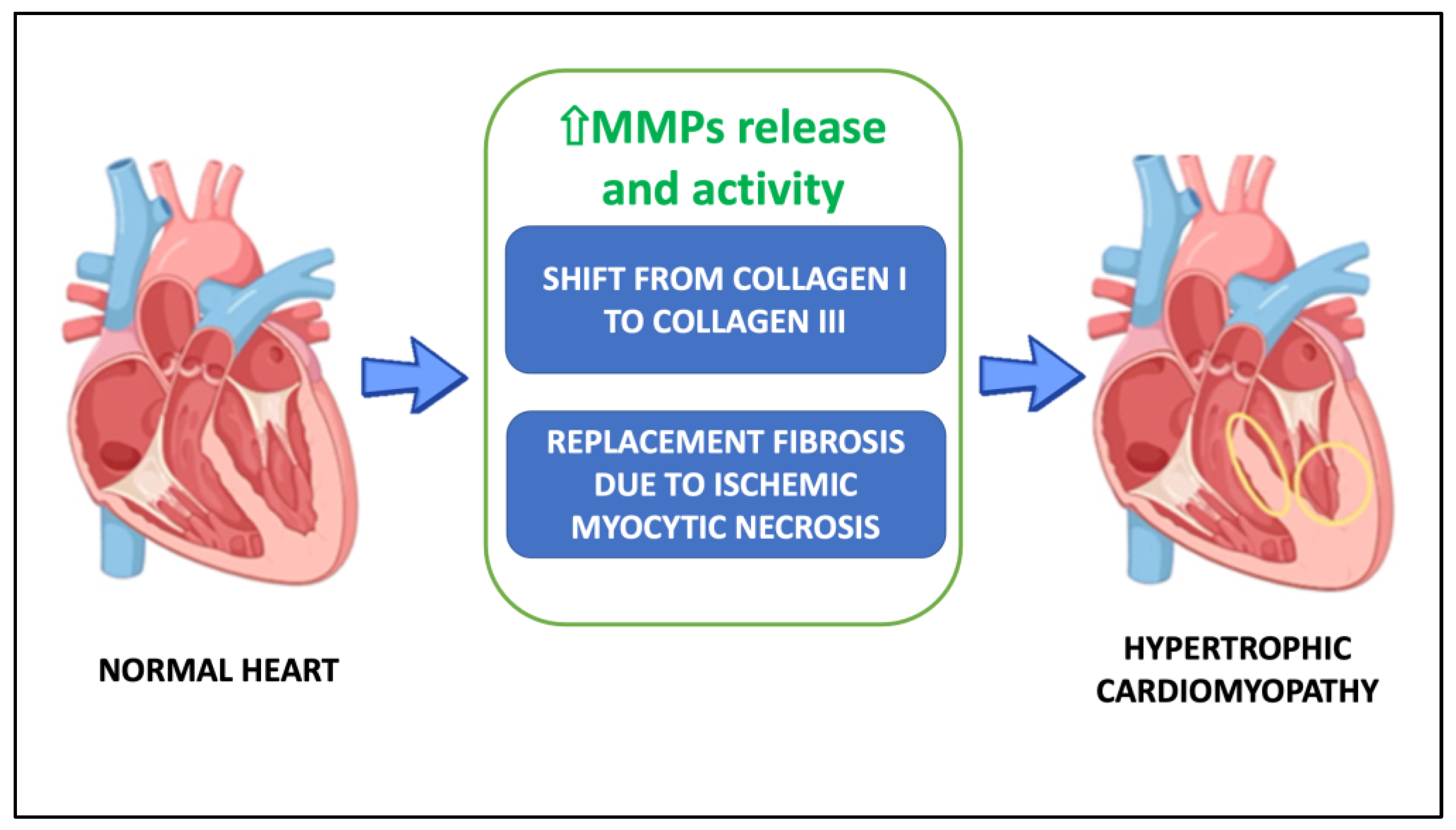
4.2.1. The Collagen Switch Hypothesis
4.2.2. The Ischemic Myocytic Necrosis Hypothesis
4.3. Matrix Metalloproteinases in the Treatment for Hypertrophic Cardiomyopathy
4.4. Strengths and Limitations
4.5. Clinical Importance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Czimbalmos, C.; Csecs, I.; Toth, A.; Kiss, O.; Suhai, F.I.; Sydo, N.; Dohy, Z.; Apor, A.; Merkely, B.; Vago, H. The demanding grey zone: Sport indices by cardiac magnetic resonance imaging differentiate hypertrophic cardiomyopathy from athlete’s heart. PLoS ONE 2019, 14, e0211624. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients with Hypertrophic Cardiomyopathy: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2020, 76, 3022–3055. [Google Scholar] [CrossRef] [PubMed]
- Aljeaid, D.; Sanchez, A.I.; Wakefield, E.; Chadwell, S.E.; Moore, N.; Prada, C.E.; Zhang, W. Prevalence of pathogenic and likely pathogenic variants in the RASopathy genes in patients who have had panel testing for cardiomyopathy. Am. J. Med. Genet. Part A 2019, 179, 608–614. [Google Scholar] [CrossRef]
- Song, C.; Wang, S.; Guo, Y.; Zheng, X.; Lu, J.; Fang, X.; Wang, S.; Huang, X. Preoperative NT-proBNP Predicts Midterm Outcome After Septal Myectomy. J. Am. Hear. Assoc. 2019, 8, e011075. [Google Scholar] [CrossRef] [PubMed]
- Borer, J.S.; Atar, D.; Marciniak, T.; Kim, M.H.; Serebruany, V. Atrial Fibrillation and Stroke in Patients with Hypertrophic Cardiomyopathy: Important New Insights. Thromb. Haemost. 2019, 119, 355–357. [Google Scholar] [CrossRef]
- Tejado, B.S.M.; Jou, C. Histopathology in HCM. Glob. Cardiol. Sci. Pr. 2018, 2018, 20. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.Y.; López, B.; Coelho-Filho, O.R.; Lakdawala, N.K.; Cirino, A.L.; Jarolim, P.; Kwong, R.; González, A.; Colan, S.D.; Seidman, J.; et al. Myocardial Fibrosis as an Early Manifestation of Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2010, 363, 552–563. [Google Scholar] [CrossRef]
- Tyagi, S.C.; Kumar, S.G.; Banks, J.; Fortson, W. Co-expression of tissue inhibitor and matrix metalloproteinase in myocardium. J. Mol. Cell. Cardiol. 1995, 27, 2177–2189. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]. The Cochrane Collaboration 2011. Available online: www.handbook.cochrane.org (accessed on 1 November 2022).
- Bradham, W.S.; Gunasinghe, H.; Holder, J.R.; Multani, M.; Killip, D.; Anderson, M.; Meyer, D.; Spencer, W.H., 3rd; Torre-Amione, G.; Spinale, F.G. Release of matrix metalloproteinases following alcohol septal ablation in hypertrophic obstructive cardiomyopathy. J. Am. Coll. Cardiol. 2002, 40, 2165–2173. [Google Scholar] [CrossRef]
- Lombardi, R.; Betocchi, S.; Losi, M.A.; Tocchetti, C.G.; Aversa, M.; Miranda, M.; D’Alessandro, G.; Cacace, A.; Ciampi, Q.; Chiariello, M. Myocardial Collagen Turnover in Hypertrophic Cardiomyopathy. Circulation 2003, 108, 1455–1460. [Google Scholar] [CrossRef]
- Fassbach, M.; Schwartzkopff, B. Elevated serum markers for collagen synthesis in patients with hypertrophic cardiomyopathy and diastolic dysfunction. Z. Kardiol. 2005, 94, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Noji, Y.; Shimizu, M.; Ino, H.; Higashikata, T.; Yamaguchi, M.; Nohara, A.; Horita, T.; Shimizu, K.; Ito, Y.; Matsuda, T.; et al. Increased Circulating Matrix Metalloproteinase-2 in Patients with Hypertrophic Cardiomyopathy with Systolic Dysfunction. Circ. J. 2004, 68, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Stroud, R.E.; Deschamps, A.M.; Lowry, A.S.; Hardin, A.E.; Mukherjee, R.; Lindsey, M.L.; Ramamoorthy, S.; Zile, M.R.; Spencer, W.H.; Spinale, F.G. Plasma Monitoring of the Myocardial Specific Tissue Inhibitor of Metalloproteinase-4 after Alcohol Septal Ablation in Hypertrophic Obstructive Cardiomyopathy. J. Card. Fail. 2005, 11, 124–130. [Google Scholar] [CrossRef]
- Roldán, V.; Marín, F.; Gimeno, J.R.; Ruiz-Espejo, F.; González, J.; Feliu, E.; García-Honrubia, A.; Saura, D.; de la Morena, G.; Valdés, M.; et al. Matrix metalloproteinases and tissue remodeling in hypertrophic cardiomyopathy. Am. Hear. J. 2008, 156, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Saura, D.; Marín, F.; Climent, V.; González, J.; Roldán, V.; Hernández-Romero, D.; Oliva, M.J.; Sabater, M.; de la Morena, G.; Lip, G.Y.H.; et al. Left atrial remodelling in hypertrophic cardiomyopathy: Relation with exercise capacity and biochemical markers of tissue strain and remodelling. Int. J. Clin. Pr. 2009, 63, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Kitaoka, H.; Kubo, T.; Okawa, M.; Hayato, K.; Yamasaki, N.; Matsumura, Y.; Doi, Y.L. Impact of Metalloproteinases on Left Ventricular Remodeling and Heart Failure Events in Patients with Hypertrophic Cardiomyopathy. Circ. J. 2010, 74, 1191–1196. [Google Scholar] [CrossRef]
- Kitaoka, H.; Kubo, T.; Okawa, M.; Takenaka, N.; Baba, Y.; Yamasaki, N.; Matsumura, Y.; Furuno, T.; Doi, Y.L. Plasma metalloproteinase levels and left ventricular remodeling in hypertrophic cardiomyopathy in patients with an identical mutation. J. Cardiol. 2011, 58, 261–265. [Google Scholar] [CrossRef]
- Zachariah, J.P.; Colan, S.D.; Lang, P.; Triedman, J.K.; Alexander, M.E.; Walsh, E.P.; Berul, C.I.; Cecchin, F. Circulating Matrix Metalloproteinases in Adolescents with Hypertrophic Cardiomyopathy and Ventricular Arrhythmia. Circ. Hear. Fail. 2012, 5, 462–466. [Google Scholar] [CrossRef]
- Fucikova, A.; Lenco, J.; Tambor, V.; Rehulkova, H.; Pudil, R.; Stulik, J. Plasma concentration of fibronectin is decreased in patients with hypertrophic cardiomyopathy. Clin. Chim. Acta 2016, 463, 62–66. [Google Scholar] [CrossRef]
- Münch, J.; Avanesov, M.; Bannas, P.; Säring, D.; Krämer, E.; Mearini, G.; Carrier, L.; Suling, A.; Lund, G.; Patten, M. Serum Matrix Metalloproteinases as Quantitative Biomarkers for Myocardial Fibrosis and Sudden Cardiac Death Risk Stratification in Patients with Hypertrophic Cardiomyopathy. J. Card. Fail. 2016, 22, 845–850. [Google Scholar] [CrossRef]
- Fernlund, E.; Gyllenhammar, T.; Jablonowski, R.; Carlsson, M.; Larsson, A.; Ärnlöv, J.; Liuba, P. Serum Biomarkers of Myocardial Remodeling and Coronary Dysfunction in Early Stages of Hypertrophic Cardiomyopathy in the Young. Pediatr. Cardiol. 2017, 38, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Qiao, S.; Song, Y.; Liu, Y.; Tang, Y.; Deng, L.; Yuan, J.; Hu, F.; Yang, W. Procollagen type I carboxy-terminal propeptide (PICP) and MMP-2 are potential biomarkers of myocardial fibrosis in patients with hypertrophic cardiomyopathy. Cardiovasc. Pathol. 2019, 43, 107150. [Google Scholar] [CrossRef] [PubMed]
- Qian, D.; Zhou, X.; Liu, H.; Cao, L. Clinical value of 2D speckle tracking imaging in evaluating the effect of percutaneous intramyocardial septal radiofrequency ablation in patients with hypertrophic obstructive cardiomyopathy. J. Clin. Ultrasound 2021, 49, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Bi, X.; Yang, C.; Song, Y.; Yuan, J.; Cui, J.; Hu, F.; Qiao, S. Matrix Metalloproteinases Increase Because of Hypoperfusion in Obstructive Hypertrophic Cardiomyopathy. Ann. Thorac. Surg. 2020, 111, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Masutomo, K.; Makino, N.; Fushiki, M.S.M.S. Effects of losartan on the collagen degradative enzymes in hypertrophic and congestive types of cardiomyopathic hamsters. Mol. Cell. Biochem. 2001, 224, 19–27. [Google Scholar] [CrossRef]
- Chiu, Y.-T.; Cheng, C.-C.; Lin, N.-N.; Hung, Y.-W.; Chen, Y.-T.; Hsu, S.-L.; Chi, C.-S.; Fu, Y.-C. High-dose Norepinephrine Induces Disruption of Myocardial Extracellular Matrix and Left Ventricular Dilatation and Dysfunction in a Novel Feline Model. J. Chin. Med. Assoc. 2006, 69, 343–350. [Google Scholar] [CrossRef]
- Kitz, S.; Fonfara, S.; Hahn, S.; Hetzel, U.; Kipar, A. Feline Hypertrophic Cardiomyopathy: The Consequence of Cardiomyocyte-Initiated and Macrophage-Driven Remodeling Processes? Veter. Pathol. 2019, 56, 565–575. [Google Scholar] [CrossRef]
- Lim, W.-W.; Neo, M.; Thanigaimani, S.; Kuklik, P.; Ganesan, A.; Lau, D.; Tsoutsman, T.; Kalman, J.; Semsarian, C.; Saint, D.; et al. Electrophysiological and Structural Remodeling of the Atria in a Mouse Model of Troponin-I Mutation Linked Hypertrophic Cardiomyopathy: Implications for Atrial Fibrillation. Int. J. Mol. Sci. 2021, 22, 6941. [Google Scholar] [CrossRef]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef]
- Nielsen, S.H.; Mouton, A.J.; DeLeon-Pennell, K.; Genovese, F.; Karsdal, M.; Lindsey, M.L. Understanding cardiac extracellular matrix remodeling to develop biomarkers of myocardial infarction outcomes. Matrix Biol. 2019, 75–76, 43–57. [Google Scholar] [CrossRef]
- Rienks, M.; Papageorgiou, A.-P.; Frangogiannis, N.G.; Heymans, S. Myocardial Extracellular Matrix: An Ever-Changing and Diverse Entity. Circ. Res. 2014, 114, 872–888. [Google Scholar] [CrossRef] [PubMed]
- Nikolov, A.; Popovski, N. Extracellular Matrix in Heart Disease: Focus on Circulating Collagen Type I and III Derived Peptides as Biomarkers of Myocardial Fibrosis and Their Potential in the Prognosis of Heart Failure: A Concise Review. Metabolites 2022, 12, 297. [Google Scholar] [CrossRef] [PubMed]
- Mundhenke, M.; Schwartzkopff, B.; Stark, P.; Schulte, H.D.; Strauer, B.E. Myocardial Collagen Type I and Impaired Left Ventricular Function under Exercise in Hypertrophic Cardiomyopathy. Thorac. Cardiovasc. Surg. 2002, 50, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Schwartzkopff, B.; Fassbach, M.; Pelzer, B.; Brehm, M.; Strauer, B.E. Elevated serum markers of collagen degradation in patients with mild to moderate dilated cardiomyopathy. Eur. J. Hear. Fail. 2002, 4, 439–444. [Google Scholar] [CrossRef]
- Maron, B.J.; Wolfson, J.K.; Epstein, S.E.; Roberts, W.C. Intramural (“small vessel”) coronary artery disease in hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 1986, 8, 545–557. [Google Scholar] [CrossRef]
- van Berlo, J.; Maillet, M.; Molkentin, J.D. Signaling effectors underlying pathologic growth and remodeling of the heart. J. Clin. Investig. 2013, 123, 37–45. [Google Scholar] [CrossRef]
- Beauloye, C.; Bertrand, L.; Horman, S.; Hue, L. AMPK activation, a preventive therapeutic target in the transition from cardiac injury to heart failure. Cardiovasc. Res. 2011, 90, 224–233. [Google Scholar] [CrossRef]


{kind=link}
| Study, Year [Ref.] | Study Design | N° of Patients | Population | Control Group | MMP | Other Factos | Outcomes | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Bradham, 2002 [10] | Prospective observational NRCT | 51 | Patient with HOCM submitted to alcohol septal ablation (51 pts) | - | MMP-2, MMP-8, MMP-9, MMP-13, TIMP-1 | CK CK-MB1 |
|
|
| Lombardi, 2003 [11] | Prospective observational NRCT | 50 | Patient with HOCM (36 pts) | Healthy subjects (14 pts) | MMP-1, MMP-2, MMP-9, TIMP-1 | ICTP, PICP, PINP |
|
|
| Fassbach, 2004 [12] | Prospective observational NRCT | 64 | Patient with HOCM (26 pts) | Healthy subjects (38 pts) | MMP-1, TIMP-1 | ICTP, PICP |
|
|
| Noji, 2004 [13] | Prospective observational NRCT | 78 | Patient with HOCM (28 pts) | Healthy subjects (50 pts) | MMP-2, MMP-3, MMP-9, TIMP-1, TIMP-2 | - |
|
|
| Stroud, 2005 [14] | Prospective observational NRCT | 34 | Patient with HOCM submitted to alcohol septal ablation (18 pts) | Healthy subjects (16 pts) | TIMP-4 | - |
|
|
| Roldàn, 2008 [15] | Prospective observational NRCT | 125 | Patient with HOCM (67 pts) | Healthy subjects (58 pts) | MMP-1, MMP-2, MMP-9, TIMP-1 | NT-proBNP |
|
|
| Saura, 2009 [16] | Prospective observational NRCT | 73 | Patient with HOCM (73 pts) | - | MMP-2, TIMP-1 | NT-pro-BNP, C-reactive protein |
|
|
| Kitaoka, 2010 [17] | Retrospective observational NRCT | 41 | Patient with HOCM (41 pts) | - | MMP-2, MMP-9, TIMP-1 | BNP |
|
|
| Kitaoka, 2011 [18] | Prospective observational NRCT | 16 * | Patient with HOCM (16 pts) | - | MMP-2, MMP-9, TIMP-1 | BNP |
|
|
| Zachariah, 2012 [19] | Prospective observational NRCT | 45 | Patient with HOCM (45 pts) | - | MMP-1, MMP-2, MMP-3, MMP-9, TIMP-1, TIMP-2, TIMP-3, TIMP-4 | - |
|
|
| Fucikova, 2016 [20] | Prospective observational NRCT | 30 | Patient with HOCM (17 pts) | Healthy subjects (17 pts) | MMP-2, MMP-9, TIMP-1, TIMP-2 | BNP, fibronectin |
|
|
| Munch, 2016 [21] | Retrospective observational NRCT | 54 | Patient with HOCM (54 pts) | - | MMP-1, MMP-2, MMP-3, MMP-9, TIMP-1 | - |
|
|
| Fernlund, 2017 [22] | Prospective observational NRCT | 105 | Patient with HOCM (39 pts) | Healthy subjects (66 pts) | MMP-9 | - |
|
|
| Yang, 2019 [23] | Prospective observational NRCT | 52 | Patient with HOCM submitted to surgical myectomy (52 pts) | - | MMP-2, MMP-9, TIMP-1 | - |
|
|
| Qian, 2020 [24] | Prospective observational NRCT | 30 | Patient with HOCM submitted to percutaneous intramyocardial septal radiofrequency ablation (30 pts) | - | MMP-2 | - |
|
|
| Bi, 2021 [25] | Prospective observational NRCT | 55 | Patient with HOCM submitted to surgical myectomy (55 pts) | - | MMP-2, MMP-9, TIMP-1 | - |
|
|
| Subgroup | MMP | Nomenclature | Mass (kDa) | Substrate | References |
|---|---|---|---|---|---|
| Interstitial collagenase | MMP-1 | Fibroblast collagenase | 52 | Collagens I, II, III, VI, VIII and X, gelatin, aggrecan, MMP-2, MMP-9 | [11,12,15,19,21] |
| MMP-8 | Neutrophil collagenase or Collagenase 2 | 75 | Collagens I, II, III, V, VII, VIII and X, gelatin, aggrecan | [10] | |
| MMP-13 | Collagenase 3 | 54 | Collagens I, II, III and IV, gelatin, aggrecan | [10] | |
| Gelatinases | MMP-2 | Gelatinase A | 72 | Gelatin, collagen types I, IV, V, VII, X, XI and XIV, elastin, fibronectin, aggrecan | [10,11,13,15,16,17,18,19,20,21,23,24,25] |
| MMP-9 | Gelatinase B | 92 | Gelatin, collagen types IV, V, VII, and X, elastin | [10,11,13,15,17,18,19,20,21,22,23,25] | |
| Stromelysins | MMP-3 | Stromelysin 1 | 57 | Collagens III, IV, IX and X, gelatin, aggrecan, MMP-1, MMP-7, MMP-8, MMP-9 and MMP-13, laminin, fibronectin, non-helical collagen | [13,19,21] |
| Glycoproteins | TIMP-1 | - | 28 | all MMPs except MMP-14 | [10,11,12,13,15,16,17,18,19,20,21,23,25] |
| TIMP-2 | - | 21 | all MMPs | [13,19,20] | |
| TIMP-3 | - | 24 | all MMPs | [19] | |
| TIMP-4 | - | 23 | all MMPs | [14,19] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serraino, G.F.; Jiritano, F.; Costa, D.; Ielapi, N.; Napolitano, D.; Mastroroberto, P.; Bracale, U.M.; Andreucci, M.; Serra, R. Metalloproteinases and Hypertrophic Cardiomyopathy: A Systematic Review. Biomolecules 2023, 13, 665. https://doi.org/10.3390/biom13040665
Serraino GF, Jiritano F, Costa D, Ielapi N, Napolitano D, Mastroroberto P, Bracale UM, Andreucci M, Serra R. Metalloproteinases and Hypertrophic Cardiomyopathy: A Systematic Review. Biomolecules. 2023; 13(4):665. https://doi.org/10.3390/biom13040665
Chicago/Turabian StyleSerraino, Giuseppe Filiberto, Federica Jiritano, Davide Costa, Nicola Ielapi, Desirèe Napolitano, Pasquale Mastroroberto, Umberto Marcello Bracale, Michele Andreucci, and Raffaele Serra. 2023. "Metalloproteinases and Hypertrophic Cardiomyopathy: A Systematic Review" Biomolecules 13, no. 4: 665. https://doi.org/10.3390/biom13040665
APA StyleSerraino, G. F., Jiritano, F., Costa, D., Ielapi, N., Napolitano, D., Mastroroberto, P., Bracale, U. M., Andreucci, M., & Serra, R. (2023). Metalloproteinases and Hypertrophic Cardiomyopathy: A Systematic Review. Biomolecules, 13(4), 665. https://doi.org/10.3390/biom13040665