
Sequential and Combined Efficacious Management of Auricular Keloid: A Novel Treatment Protocol Employing Ablative CO2 and Dye Laser Therapy—An Advanced Single-Center Clinical Investigation

 ,
, 

 and
and
Abstract
1. Introduction
1.1. Auricular Keloids
1.2. Traditional Treatment Methods
1.3. Ablative Combined Laser Therapy with CO2 and Dye as an Innovative Approach
2. Materials and Methods
2.1. Study Design and Patient Selection
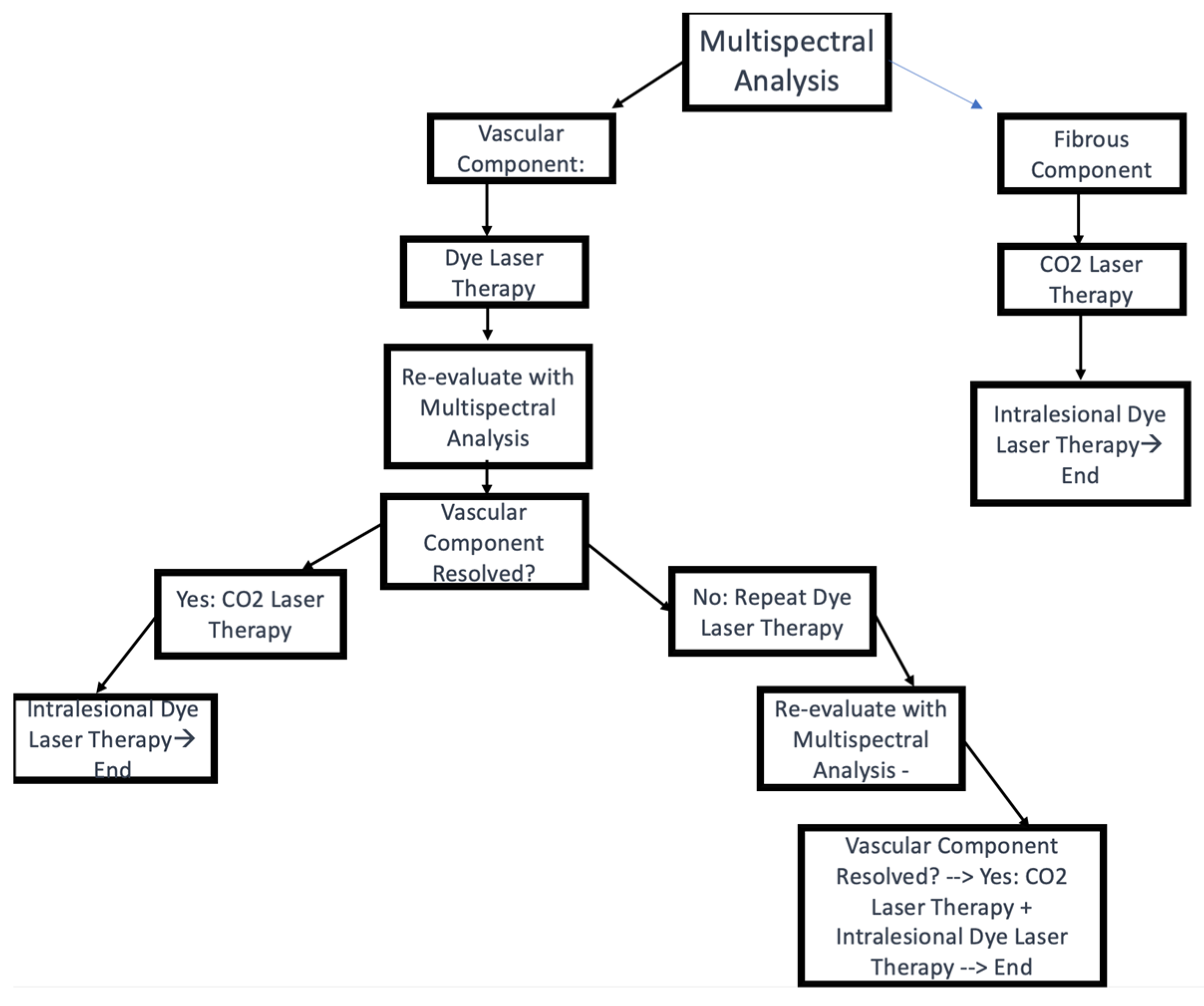
2.2. Treatment Protocol
2.2.1. Dye Laser Therapy
2.2.2. Ablative CO2 Laser Therapy
2.2.3. Follow-Up and Additional Treatments
2.2.4. Multispectral Analysis
2.2.5. Vancouver Scar Scale (VSS)
2.2.6. Patient and Observer Scar Assessment Scale
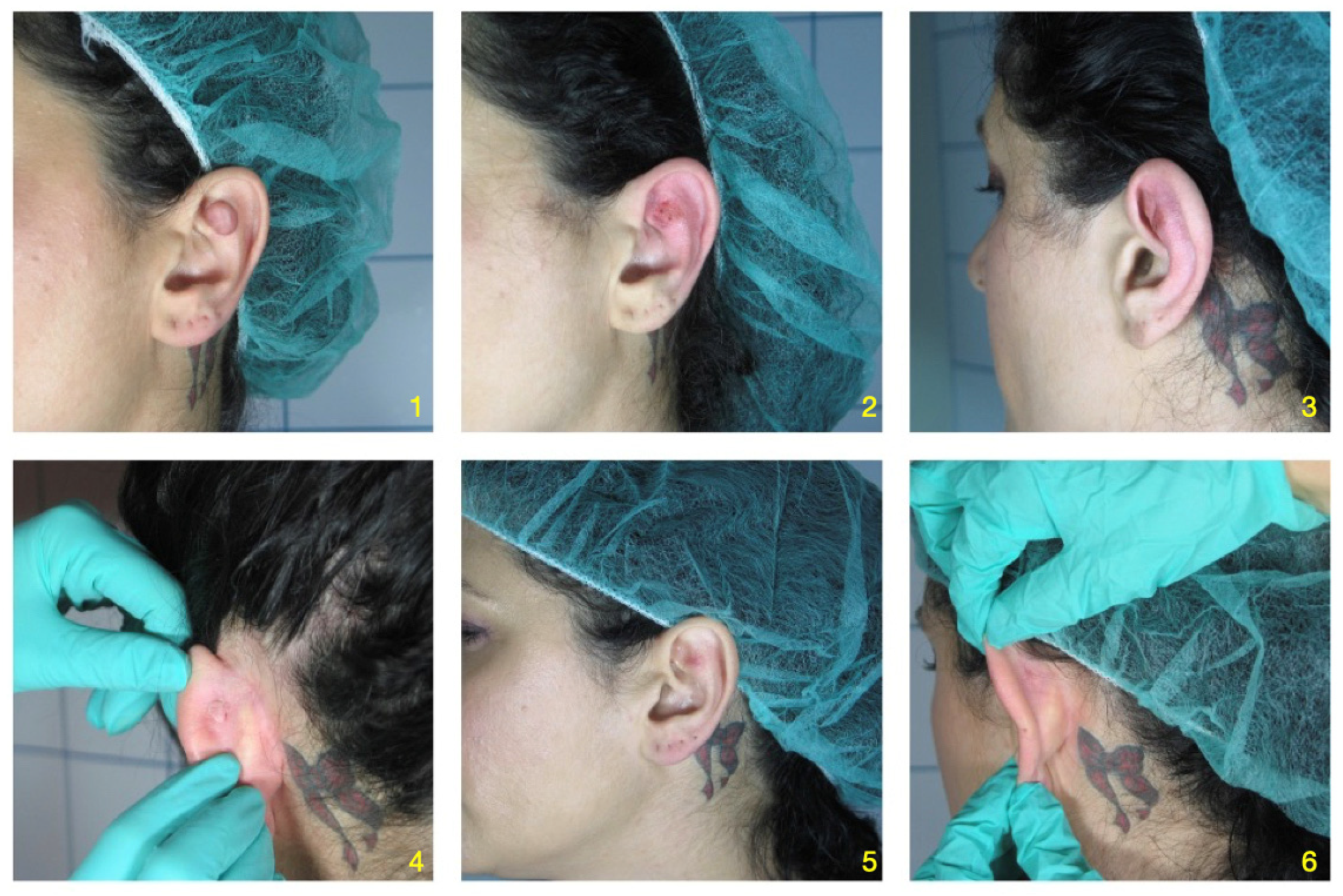
- Clinical Case n 1:
- Clinical case n 2:
3. Results
3.1. Changes in VSS and POSAS Scores
3.2. Scar Improvement
3.2.1. Chromaticity
3.2.2. Texture
3.2.3. Pliability
3.3. Complete Elimination of Ear Keloids
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Shanina, N.A.; Patrushev, A.V.; Zorman, A. Histological and immunohistochemical changes in facial skin treated with combined ablative and non-ablative laser therapy. J. Cosmet. Dermatol. 2021, 20, 3509–3516. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhou, S.; Xia, Z.; Peng, Z.; Yang, R. Fractional CO2 Laser Combined with 595-nm PDL Inhibiting Hypertrophic Scars via Measuring BMP-7 and Fas Expression in Rabbit Models. 2020. Available online: https://www.researchsquare.com/article/rs-120537/v1 (accessed on 13 June 2023).
- Liu, K.; Wu, X.L.; Wang, P.H. Advances in therapy of auricular keloid. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2016, 51, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Bock, O.; Schmid-Ott, G.; Malewski, P.; Mrowietz, U. Quality of life of patients with keloid and hypertrophic scarring. Arch. Dermatol. Res. 2006, 297, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Mustoe, T.A.; Cooter, R.D.; Gold, M.H.; Hobbs, F.D.R.; Ramelet, A.-A.; Shakespeare, P.G.; Stella, M.; Téot, L.; Wood, F.M.; Ziegler, U.E. International clinical recommendations on scar management. Plast. Reconstr. Surg. 2002, 110, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Berman, B.; Bieley, H.C. Adjunct therapies to surgical management of keloids. Dermatol. Surg. 1996, 22, 126–130. [Google Scholar] [CrossRef]
- van de Kar, A.L.; Corion, L.U.M.; Smeulders, M.J.C.; Draaijers, L.J.; van der Horst, C.M.A.M.; van Zuijlen, P.P.M. Reliable and feasible evaluation of linear scars by the Patient and Observer Scar Assessment Scale. Plast. Reconstr. Surg. 2005, 116, 514–522. [Google Scholar] [CrossRef]
- Alster, T.S.; West, T.B. Effect of topical vitamin C on postoperative carbon dioxide laser resurfacing erythema. Dermatol. Surg. 1998, 24, 331–334. [Google Scholar] [CrossRef]
- O’Brien, L.; Jones, D.J. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database Syst. Rev. 2013, 2013, CD003826. [Google Scholar] [CrossRef]
- Manuskiatti, W.; Fitzpatrick, R.E.; Goldman, M.P. Energy density and numbers of treatment affect response of keloidal and hypertrophic sternotomy scars to the 585-nm flashlamp-pumped pulsed-dye laser. J. Am. Acad. Dermatol. 2001, 45, 557–565. [Google Scholar] [CrossRef]
- Alster, T.S.; Williams, C.M. Treatment of keloid sternotomy scars with 585 nm flashlamp-pumped pulsed-dye laser. Lancet 1995, 345, 1198–1200. [Google Scholar] [CrossRef]
- Ross, E.; Naseef, G.S.; McKinlay, J.R.; Barnette, D.J.; Skrobal, M.; Grevelink, J.; Anderson, R. Comparison of carbon dioxide laser, erbium:YAG laser, dermabrasion, and dermatome: A study of thermal damage, wound contraction, and wound healing in a live pig model: Implications for skin resurfacing. J. Am. Acad. Dermatol. 2000, 42 Pt 1, 92–105. [Google Scholar] [CrossRef]
- Berman, B.; Flores, F. The treatment of hypertrophic scars and keloids. Eur. J. Dermatol. 1998, 8, 591–595. [Google Scholar] [PubMed]
- Ilișanu, M.A.; Moldoveanu, F.; Moldoveanu, A. Multispectral Imaging for Skin Diseases Assessment-State of the Art and Perspectives. Sensors 2023, 23, 3888. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Akaishi, S.; Kuribayashi, S.; Miyashita, T. Keloids and Hypertrophic Scars Can Now Be Cured Completely: Recent Progress in Our Understanding of the Pathogenesis of Keloids and Hypertrophic Scars and the Most Promising Current Therapeutic Strategy. J. Nippon. Med. Sch. Nippon. Ika Daigaku Zasshi 2016, 83, 46–53. [Google Scholar] [CrossRef]
- Gold, M.H.; McGuire, M.; Mustoe, T.A.; Pusic, A.; Sachdev, M.; Waibel, J.; Murcia, C. Updated international clinical recommendations on scar management: Part 2—Algorithms for scar prevention and treatment. Dermatol. Surg. 2014, 40, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Al-Attar, A.; Mess, S.; Thomassen, J.M.; Kauffman, C.L.; Davison, S.P. Keloid pathogenesis and treatment. Plast. Reconstr. Surg. 2006, 117, 286–300. [Google Scholar] [CrossRef]
- Layton, A.M.; Yip, J.; Cunliffe, W.J. A comparison of intralesional triamcinolone and cryosurgery in the treatment of acne keloids. Br. J. Dermatol. 1994, 130, 498–501. [Google Scholar] [CrossRef]
- Tanzi, E.L.; Alster, T.S. Side effects and complications of variable-pulsed erbium:yttrium-aluminum-garnet laser skin resurfacing: Extended experience with 50 patients. Plast. Reconstr. Surg. 2003, 111, 1524–1529; discussion 1530–1532. [Google Scholar] [CrossRef]
- Scrimali, L.; Lomeo, G.; Tamburino, S.; Catalani, A.; Perrotta, R. Laser CO2 versus radiotherapy in treatment of keloid scars. J. Cosmet. Laser Ther. Off. Publ. Eur. Soc. Laser Dermatol. 2012, 14, 94–97. [Google Scholar] [CrossRef]
- Liu, A.; Moy, R.L.; Ross, E.V.; Hamzavi, I.; Ozog, D.M. Pulsed dye laser and pulsed dye laser-mediated photodynamic therapy in the treatment of dermatologic disorders. Dermatol. Surg. 2012, 38, 351–366. [Google Scholar] [CrossRef]
- Bouzari, N.; Davis, S.C.; Nouri, K. Laser treatment of keloids and hypertrophic scars. Int. J. Dermatol. 2007, 46, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-R.; Wu, W.-S.; Jeng, S.-F.; Huang, H.-C.; Yang, K.D.; Sacks, J.M.; Wang, F.-S. Activation of ERK and p38 kinase mediated keloid fibroblast apoptosis after flashlamp pulsed-dye laser treatment. Lasers Surg. Med. 2005, 36, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Vrijman, C.; van Drooge, A.; Limpens, J.; Bos, J.; van der Veen, J.; Spuls, P.; Wolkerstorfer, A. Laser and intense pulsed light therapy for the treatment of hypertrophic scars: A systematic review. Br. J. Dermatol. 2011, 165, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Cannarozzo, G.; Silvestri, M.; Tamburi, F.; Sicilia, C.; Del Duca, E.; Scali, E.; Bennardo, L.; Nisticò, S.P. A new 675-nm laser device in the treatment of acne scars: An observational study. Lasers Med. Sci. 2021, 36, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Nouri, K.; Jimenez, G.P.; Harrison-Balestra, C.; Elgart, G.W. 585-nm pulsed dye laser in the treatment of surgical scars starting on the suture removal day. Dermatol. Surg. 2003, 29, 65–73; discussion 73. [Google Scholar] [CrossRef]
- Tawfic, S.O.; El-Tawdy, A.; Shalaby, S.; Foad, A.; Shaker, O.; Sayed, S.S.; Metwally, D. Evaluation of Fractional CO2 Versus Long Pulsed Nd:YAG Lasers in Treatment of Hypertrophic Scars and Keloids: A Randomized Clinical Trial. Lasers Surg. Med. 2020, 52, 959–965. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Pre-Treatment VSS | Post-Treatment VSS |
|---|---|---|
| 1 | 9 | 3 |
| 2 | 8 | 3 |
| 3 | 10 | 4 |
| 4 | 7 | 2 |
| 5 | 8 | 3 |
| 6 | 9 | 3 |
| 7 | 8 | 3 |
| 8 | 9 | 4 |
| 9 | 7 | 2 |
| 10 | 8 | 3 |
| 11 | 9 | 3 |
| 12 | 8 | 3 |
| 13 | 9 | 4 |
| 14 | 7 | 2 |
| 15 | 8 | 3 |
| Pre-Treatment | Post-Treatment | |
|---|---|---|
| Patient Scar Assessment | ||
| 1. Pain | 50 ± 12 | 1.3 ± 0.5 |
| 2. Itching | 4.2 ± 1.1 | 1.5 ± 0.6 |
| 3. Color | 8.0 ± 1.4 | 2.9 ± 0.8 |
| 4. Stiffness | 7.8 ± 1.5 | 3.0 ± 0.9 |
| 5. Thickness | 8.2 ± 1.6 | 3.2 ± 1.0 |
| 6. Irregularity | 7.6 ± 1.3 | 2.9 ± 0.7 |
| Observer Scar Assessment | ||
| 1. Vascularity | 6.8 ± 1.1 | 2.8 ± 0.7 |
| 2. Pigmentation | 7.0 ± 1.2 | 3.1 ± 0.8 |
| 3. Pliability | 8.2 ± 1.4 | 2.7± 0.9 |
| 4. Thickness | 7.8 ± 0.5 | 3.0 ± 1.0 |
| 5. Relief | 7.6 ± 1.3 | 2.9 ± 0.8 |
| 6. Surface area | 7.4 ± 1.4 | 3.0 ± 0.7 |
| Total POSAS | 42.6 ± 6.2 | 16.2 ± 5.1 |
| VSS Component | Pre-Treatment Mean | Pre-Treatment SD | Post-Treatment Mean | Post-Treatment SD | t-Value | p-Value |
|---|---|---|---|---|---|---|
| Total VSS | 8.4 | 1.3 | 3.1 | 1.0 | 15.92 | <0.001 |
| Measure | Pre-Treatment POSAS | Post-Treatment POSAS |
|---|---|---|
| Mean | 42.6 | 16.2 |
| Standard Deviation | 6.2 | 5.1 |
| t-value | 12.34 | 12.34 |
| p-value | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amato, S.; Nisticò, S.P.; Pellacani, G.; Guida, S.; Rossi, A.; Longo, C.; Berardesca, E.; Cannarozzo, G. Sequential and Combined Efficacious Management of Auricular Keloid: A Novel Treatment Protocol Employing Ablative CO2 and Dye Laser Therapy—An Advanced Single-Center Clinical Investigation. Cosmetics 2023, 10, 126. https://doi.org/10.3390/cosmetics10050126
Amato S, Nisticò SP, Pellacani G, Guida S, Rossi A, Longo C, Berardesca E, Cannarozzo G. Sequential and Combined Efficacious Management of Auricular Keloid: A Novel Treatment Protocol Employing Ablative CO2 and Dye Laser Therapy—An Advanced Single-Center Clinical Investigation. Cosmetics. 2023; 10(5):126. https://doi.org/10.3390/cosmetics10050126
Chicago/Turabian StyleAmato, Simone, Steven Paul Nisticò, Giovanni Pellacani, Stefania Guida, Anthony Rossi, Caterina Longo, Enzo Berardesca, and Giovanni Cannarozzo. 2023. "Sequential and Combined Efficacious Management of Auricular Keloid: A Novel Treatment Protocol Employing Ablative CO2 and Dye Laser Therapy—An Advanced Single-Center Clinical Investigation" Cosmetics 10, no. 5: 126. https://doi.org/10.3390/cosmetics10050126
APA StyleAmato, S., Nisticò, S. P., Pellacani, G., Guida, S., Rossi, A., Longo, C., Berardesca, E., & Cannarozzo, G. (2023). Sequential and Combined Efficacious Management of Auricular Keloid: A Novel Treatment Protocol Employing Ablative CO2 and Dye Laser Therapy—An Advanced Single-Center Clinical Investigation. Cosmetics, 10(5), 126. https://doi.org/10.3390/cosmetics10050126