
Poor Outcomes of Girdlestone Resection Arthroplasty in Injection Drug Users: A Retrospective Study

 , , ,
, , ,
Abstract
1. Introduction
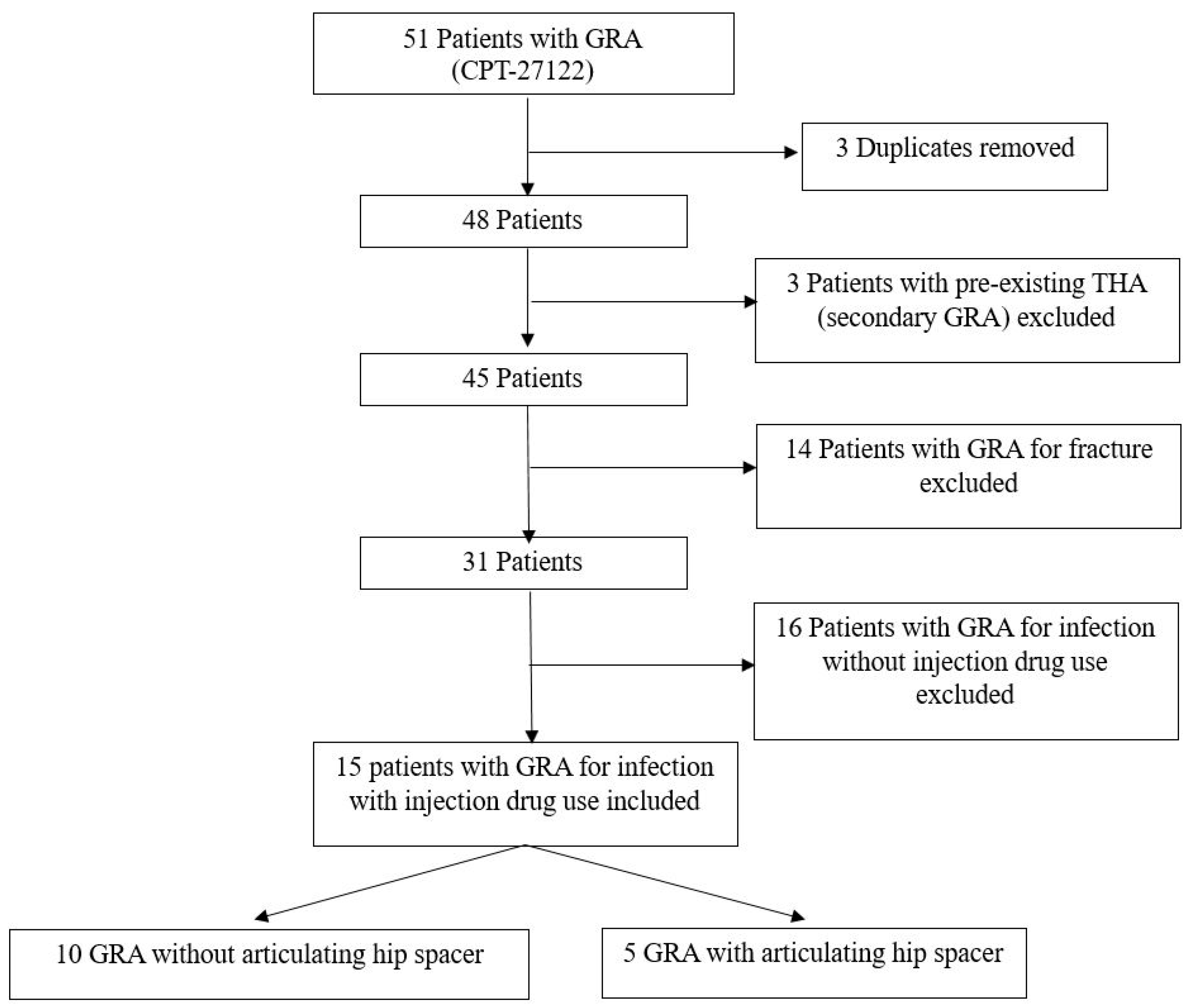
2. Results
2.1. Patient Demographics and Characteristics
2.2. Sepsis, Blood Cultures, and Mortality
2.3. Microbiology—Hip Aspirations
2.4. Microbiology—Intraoperative Cultures
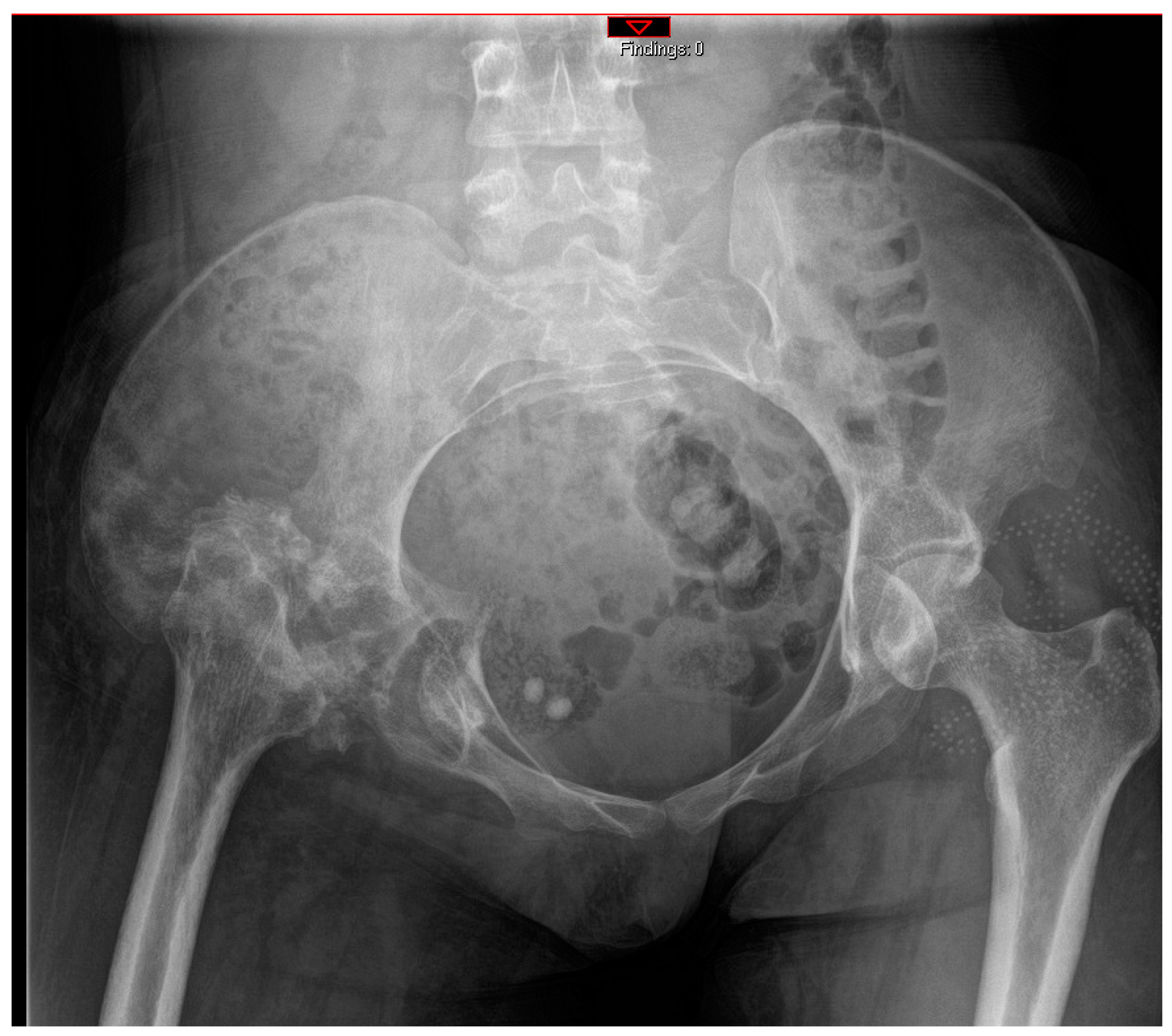
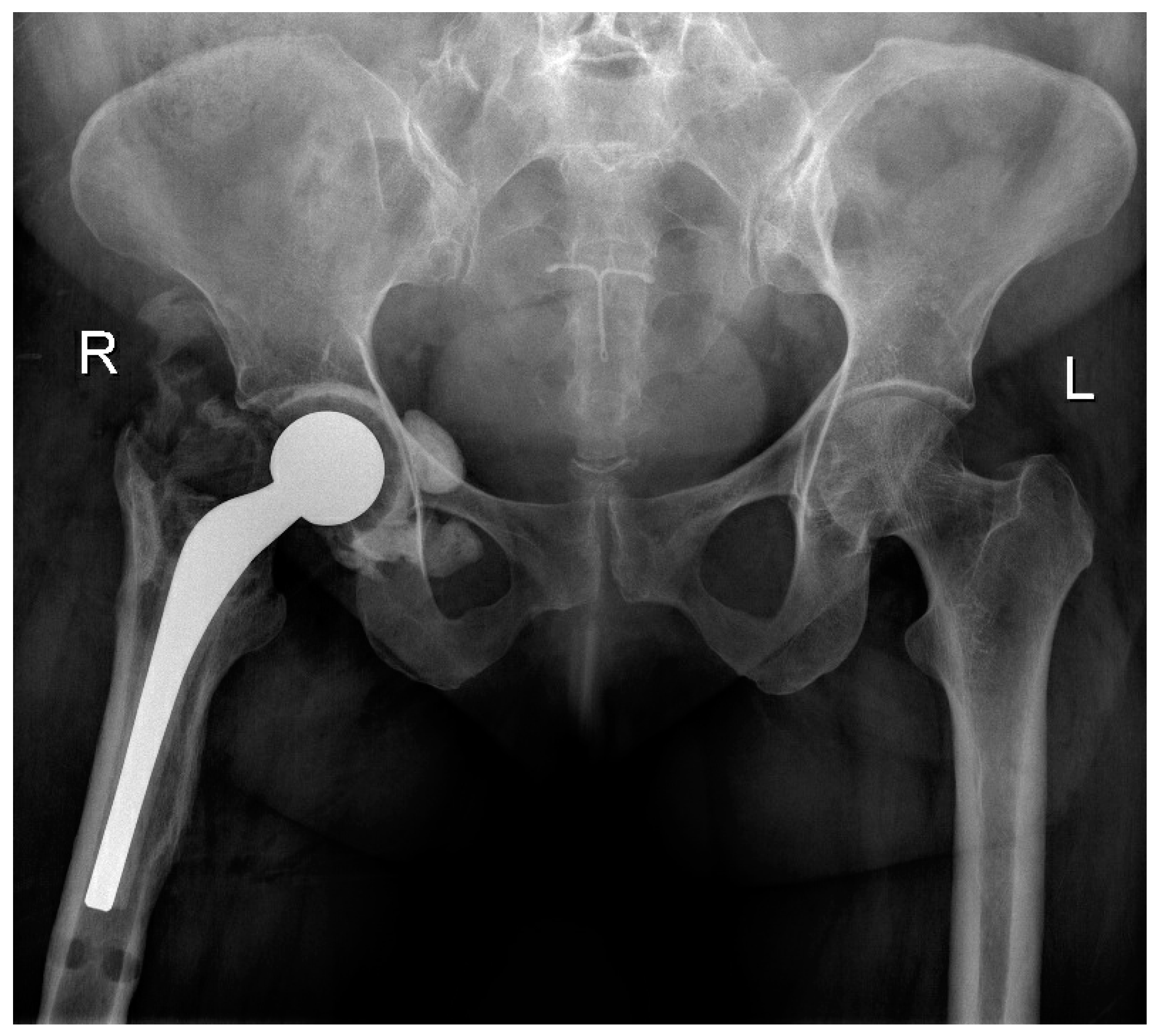
2.5. Objective Outcomes
2.6. Patient-Reported Outcome Measures
2.7. In-Hospital Psychiatric Interventions
3. Discussion
4. Limitations
5. Methods
5.1. Surgical Technique
5.2. Primary Outcomes
5.3. Secondary Outcomes
5.4. Collection of Patient-Reported Outcome Measures
5.5. Psychiatric Interventions
5.6. Statistical Analysis
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vincenten, C.M.; Gosens, T.; van Susante, J.C.; Somford, M.P. The Girdlestone situation: A historical essay. J. Bone Jt. Infect. 2019, 4, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Basu, I.; Howes, M.; Jowett, C.; Levack, B. Girdlestones excision arthroplasty: Current update. Int. J. Surg. 2011, 9, 310–313. [Google Scholar] [PubMed]
- Castellanos, J.; Flores, X.; Llusà, M.; Chiriboga, C.; Navarro, A. The Girdlestone pseudarthrosis in the treatment of infected hip replacements. Int. Orthop. 1998, 22, 178–181. [Google Scholar] [CrossRef]
- Sharma, H.; De Leeuw, J.; Rowley, D.I. Girdlestone resection arthroplasty following failed surgical procedures. Int. Orthop. 2005, 29, 92–95. [Google Scholar] [CrossRef]
- Sharma, H.; Dreghorn, C.R.; Gardner, E.R. Girdlestone resection arthroplasty of the hip: Current perspectives. Curr. Orthop. 2005, 19, 385–392. [Google Scholar] [CrossRef]
- Peterson, T.C.; Pearson, C.; Zekaj, M.; Hudson, I.; Fakhouri, G.; Vaidya, R. Septic arthritis in intravenous drug abusers: A historical comparison of habits and pathogens. J. Emerg. Med. 2014, 47, 723–728. [Google Scholar] [CrossRef]
- Condell, R.; Low, L.; Kearns, S.R.; Murphy, C.G. Girdlestone resection arthroplasty of the hip (GRA): A case series—Outdated procedure or acceptable outcome? Eur. J. Orthop. Surg. Traumatol. 2024, 34, 1711–1715. [Google Scholar] [CrossRef]
- Saldana, C.S.; Vyas, D.A.; Wurcel, A.G. Soft Tissue, Bone, and Joint Infections in People Who Inject Drugs. Infect. Dis. Clin. N. Am. 2020, 34, 495–509. [Google Scholar] [CrossRef]
- Humphrey, T.J.; Tatara, A.M.; Bedair, H.S.; Alpaugh, K.; Melnic, C.M.; Nelson, S.B. Rates and Outcomes of Periprosthetic Joint Infection in Persons Who Inject Drugs. J. Arthroplast. 2023, 38, 152–157. [Google Scholar] [CrossRef]
- Wieser, K.; Zingg, P.O.; Betz, M.; Neubauer, G.; Dora, C. Total hip replacement in patients with history of illicit injecting drug use. Arch. Orthop. Trauma Surg. 2012, 132, 1037–1044. [Google Scholar] [CrossRef]
- Hser, Y.; Evans, E.; Grella, C.; Ling, W.; Anglin, D. Long-term course of opioid addiction. Harv. Rev. Psychiatry 2015, 23, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Webb, P.; Colledge-Frisby, S.; Ireland, J.; Wheeler, A.; Ottaviano, S.; Willing, A.; Kairouz, A.; Cunningham, E.B.; Hajarizadeh, B.; et al. Epidemiology of injecting drug use, prevalence of injecting-related harm, and exposure to behavioural and environmental risks among people who inject drugs: A systematic review. Lancet Glob. Health 2023, 11, e659–e672. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, e1192–e1207. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Oh, S.; Cano, M.; Salas-Wright, C.P.; Vaughn, M.G. Trends and distinct profiles of persons who inject drugs in the United States, 2015–2019. Prev. Med. 2022, 164, 107289. [Google Scholar] [CrossRef] [PubMed]
- Bradley, H.; Hall, E.W.; Asher, A.; Furukawa, N.W.; Jones, C.M.; Shealey, J.; Buchacz, K.; Handanagic, S.; Crepaz, N.; Rosenberg, E.S. Estimated Number of People Who Inject Drugs in the United States. Clin. Infect. Dis. 2023, 76, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Ballard, W.T.; Lowry, D.A.; Brand, R.A. Resection arthroplasty of the hip. J. Arthroplast. 1995, 10, 772–779. [Google Scholar]
- Shah, N.; Parker, M.J. What is the outcome after a Girdlestone resection arthroplasty following a hip fracture? HIP Int. 2023, 33, 948–951. [Google Scholar] [CrossRef]
- Sawadogo, M.; Kafando, H.; Ouedraogo, S.; Korsaga, A.S.; Ouedraogo, S.; Tinto, S.; Ouedraogo, A.J.I.; Tall, M.; DA, S.C. Is Head and Neck Resection of the Femur (Girdlestone’s Procedure) Still Relevant? Indications and Results About 24 Cases. Open Orthop. J. 2018, 12, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Maguire, N.; Robertson, B.; Henman, P. Girdlestone procedure for avascular necrosis of the hip in an intravenous drug user. J. Surg. Case Rep. 2014, 2014, rju039. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.E.; Baxter, J.D.; Aweh, G.; O’Connell, E.; Fisher, W.H.; Barton, B.A. Risk Factors for Relapse and Higher Costs Among Medicaid Members with Opioid Dependence or Abuse: Opioid Agonists, Comorbidities, and Treatment History. J. Subst. Abus. Treat. 2015, 57, 75–80. [Google Scholar] [CrossRef]
- Nazemi, A.K.; Upfill-Brown, A.; Arshi, A.; Sekimura, T.; Zeegen, E.N.; McPherson, E.J.; Stavrakis, A.I. Analysis of perioperative outcomes in hip resection arthroplasty. Arch. Orthop. Trauma Surg. 2022, 142, 2139–2146. [Google Scholar] [CrossRef]
- National Institutes on Drug Abuse. Common Comorbidities with Substance Use Disorders Research Report; National Institute on Drug Abuse: Rockville, MD, USA, 2020.
- Li, H.; Fu, J.; Niu, E.; Chai, W.; Xu, C.; Hao, L.B.; Chen, J. The risk factors of polymicrobial periprosthetic joint infection: A single-center retrospective cohort study. BMC Musculoskelet. Disord. 2021, 22, 78. [Google Scholar] [CrossRef]
- Li, H.K.; Rombach, I.; Zambellas, R.; Walker, A.S.; McNally, M.A.; Atkins, B.L.; Lipsky, B.A.; Hughes, H.C.; Bose, D.; Kümin, M.; et al. Oral versus intravenous antibiotics for bone and joint infection. N. Engl. J. Med. 2019, 380, 425–436. [Google Scholar] [CrossRef]
- Devlin, N.J.; Brooks, R. EQ-5D and the EuroQol Group: Past, Present and Future. Appl. Health Econ. Health Policy 2017, 15, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Breivik Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Fitzpatrick, R.; Carr, A.; Murray, D. Questionnaire on the perceptions of patients about total hip replacement. J. Bone Jt. Surg. Br. Vol. 1996, 78, 185–190. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall N = 15 | No Antibiotic Spacer N = 10 | With Antibiotic Spacer N = 5 | p-Value | |
|---|---|---|---|---|
| Age (years) | 44 ± 11 | 43 ± 11 | 47.2 ± 11 | 0.459 |
| BMI | 23.1 ± 5.3 | 21.3 ± 4.7 | 26.5 ± 5.1 | 0.070 |
| Gender (female) | 9 (60%) | 6 (60%) | 3 (60%) | 1.000 |
| Active injection drug use at time of initial hospitalization | 13 (87%) | 10 (100%) | 3 (60%) | 0.095 |
| Chronic HCV infection | 9 (60%) | 5 (50%) | 4 (80%) | 0.580 |
| HIV infection | 3 (20%) | 1 (10%) | 2 (40%) | 0.242 |
| History of endocarditis | 3 (20%) | 2 (20%) | 1 (20%) | 1.000 |
| Active tobacco use | 15 (100%) | 10 (100%) | 5 (100%) | 1.000 |
| Met SIRS criteria on presentation | 4 (27%) | 3 (30%) | 1 (20%) | 1.000 |
| Stable housing | 7 (47%) | 4 (40%) | 3 (60%) | 0.608 |
| Other diagnosed psychiatric disorder, other than SUD | 6 (40%) | 6 (60%) | 0 (0%) | 0.044 |
| Paraplegic | 2 (13%) | 2 (20%) | 0 (0%) | 0.524 |
| Inpatient length of stay (days) | 9 (9–24) | 20 (11–46) | 13 (9–16) | 0.297 |
| Overall follow-up (months) | 25 ± 20 | 24 ± 22.4 | 27 ± 17 | 0.765 |
| Follow-up excluding deceased (months) | 32 ± 20 | 32 ± 24 | 31 ± 17 | 0.960 |
| Mortality | 4 (27%) | 3 (30%) | 1 (20%) | 1.000 |
| Time to mortality (days) | 78 (60–227) | 70 (50–85) | 369 [369] | 0.180 |
| Overall N = 9 | No Antibiotic Spacer N = 5 | With Antibiotic Spacer N = 4 | p-Value | |
|---|---|---|---|---|
| Conversion to THA | 4 (44%) | 1 (20%) | 3 (75%) | 0.206 |
| THA requiring revision | 3/4 (75%) | 1/4 (25%) | 2/4 (50%) | 1.000 |
| Able to ambulate at final follow-up | 7 (78%) | 3 (60%) | 4 (100%) | 0.444 |
| Active intravenous drug use at final follow-up | 3 (33%) | 2 (40%) | 1 (25%) | 1.000 |
| Resolution of infection following initial procedure and hospitalization | 3 (33%) | 0 (0%) | 3 (75%) | 0.048 |
| Completed antibiotic course as prescribed | 5 (56%) | 2 (40%) | 3 (75%) | 0.524 |
| Second admission for infection in ipsilateral hip | 6 (67%) | 5 (100%) | 1 (25%) | 0.048 |
| Complete resolution of hip infection at final follow-up | 6 (67%) | 3 (60%) | 3 (75%) | 1.000 |
| Overall N = 4 | Patient 3 (No Spacer) | Patient 4 (No Spacer) | Patient 13 (Spacer) | Patient 14 (Spacer) | |
|---|---|---|---|---|---|
| EQ-5D mobility | 3.3 ± 1.3 | 5 | 2 | 3 | 3 |
| EQ-5D self-care | 1.3 ± 0.5 | 2 | 1 | 1 | 1 |
| EQ-5D activity | 2.3 ± 1.5 | 4 | 1 | 3 | 1 |
| EQ-5D pain | 3.0 ± 1.4 | 5 | 2 | 3 | 2 |
| EQ-5D anxiety | 1.8 ± 1.0 | 3 | 1 | 1 | 2 |
| NRS least pain | 3.0 ± 2.5 | 5 | 2 | 5 | 0 |
| NRS most pain | 6.8 ± 2.5 | 8 | 8 | 8 | 3 |
| NRS average pain | 3.8 ± 3.5 | 8 | 2 | 5 | 0 |
| Oxford Hip Score | 30 ± 13 | 16 | 34 | 24 | 46 |
| Overall N = 15 | No Antibiotic Spacer N = 10 | With Antibiotic Spacer N = 5 | p-Value | |
|---|---|---|---|---|
| SUD team consult | 12 (80%) | 9 (90%) | 3 (60%) | 0.242 |
| Agreed to inpatient SUD treatment | 8 (53%) | 6 (60%) | 2 (40%) | 0.608 |
| Psychiatric consult | 8 (53%) | 8 (80%) | 0 (0%) | 0.007 |
| Peer recovery consult | 8 (53%) | 7 (70%) | 1 (20%) | 0.119 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shu, H.T.; Ghanem, D.; Covarrubias, O.; Elsabbagh, Z.; Hughes, A.J.; Sotsky, R.B.; Conway, J.D.; Ferguson, J.; Osgood, G.M.; Shafiq, B. Poor Outcomes of Girdlestone Resection Arthroplasty in Injection Drug Users: A Retrospective Study. Antibiotics 2024, 13, 782. https://doi.org/10.3390/antibiotics13080782
Shu HT, Ghanem D, Covarrubias O, Elsabbagh Z, Hughes AJ, Sotsky RB, Conway JD, Ferguson J, Osgood GM, Shafiq B. Poor Outcomes of Girdlestone Resection Arthroplasty in Injection Drug Users: A Retrospective Study. Antibiotics. 2024; 13(8):782. https://doi.org/10.3390/antibiotics13080782
Chicago/Turabian StyleShu, Henry T., Diane Ghanem, Oscar Covarrubias, Zaid Elsabbagh, Alice J. Hughes, Rachel B. Sotsky, Janet D. Conway, Jamie Ferguson, Greg M. Osgood, and Babar Shafiq. 2024. "Poor Outcomes of Girdlestone Resection Arthroplasty in Injection Drug Users: A Retrospective Study" Antibiotics 13, no. 8: 782. https://doi.org/10.3390/antibiotics13080782
APA StyleShu, H. T., Ghanem, D., Covarrubias, O., Elsabbagh, Z., Hughes, A. J., Sotsky, R. B., Conway, J. D., Ferguson, J., Osgood, G. M., & Shafiq, B. (2024). Poor Outcomes of Girdlestone Resection Arthroplasty in Injection Drug Users: A Retrospective Study. Antibiotics, 13(8), 782. https://doi.org/10.3390/antibiotics13080782