
Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance

 , , , ,
, , , ,
Abstract
:1. Introduction
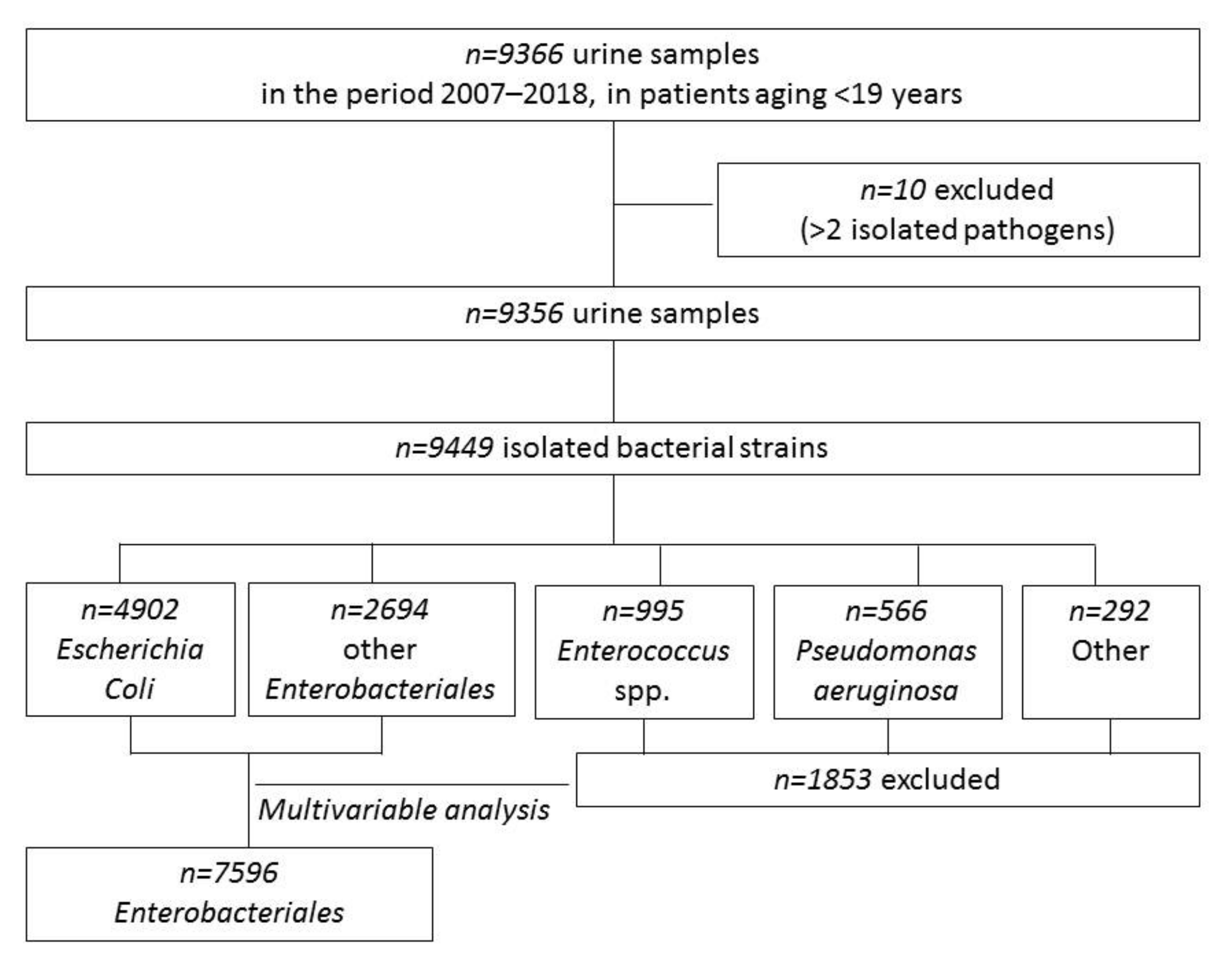
2. Materials and Methods
Statistical Analysis
3. Results
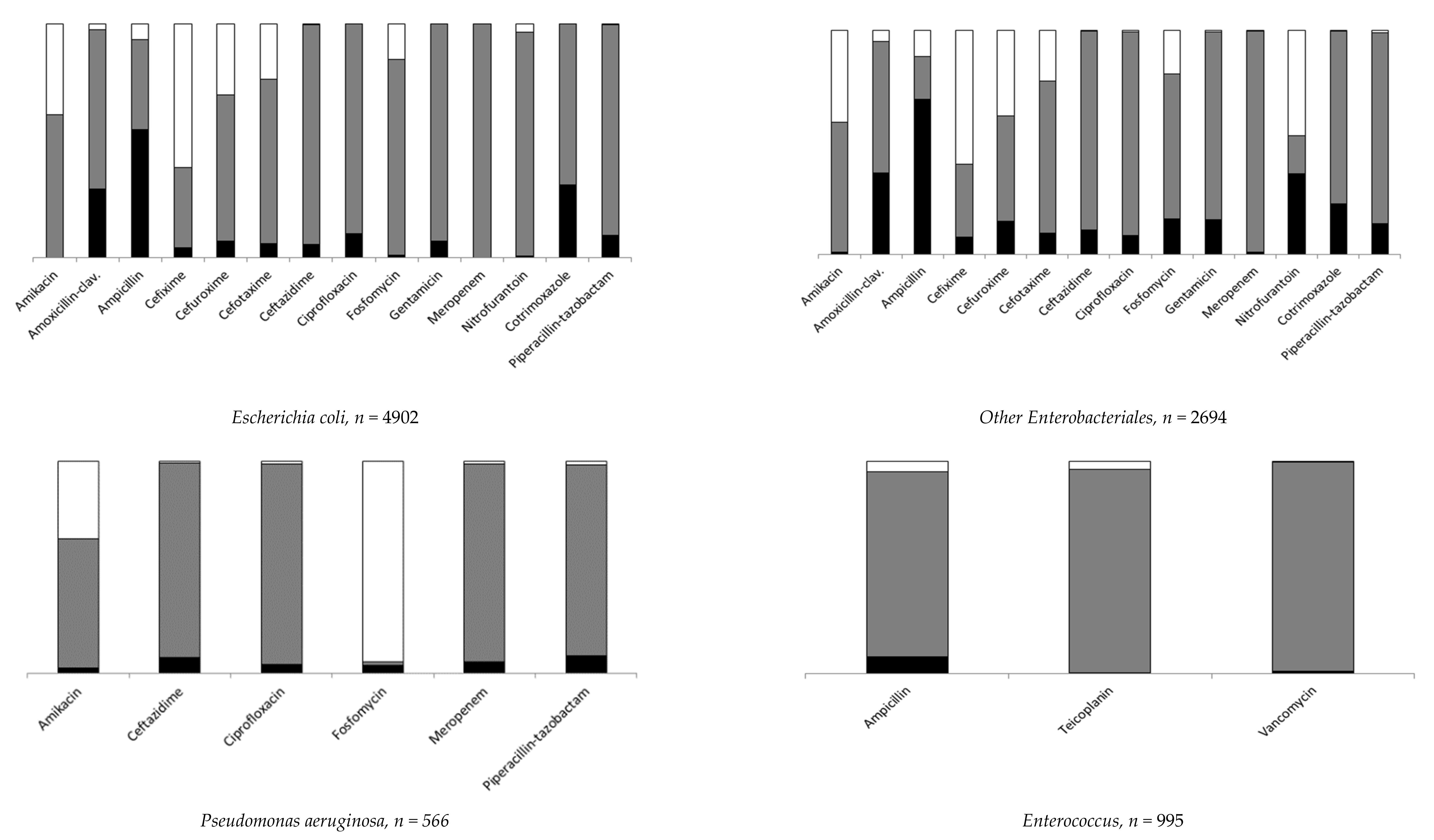
3.1. Antibiotic Resistant UTI by Pathogen
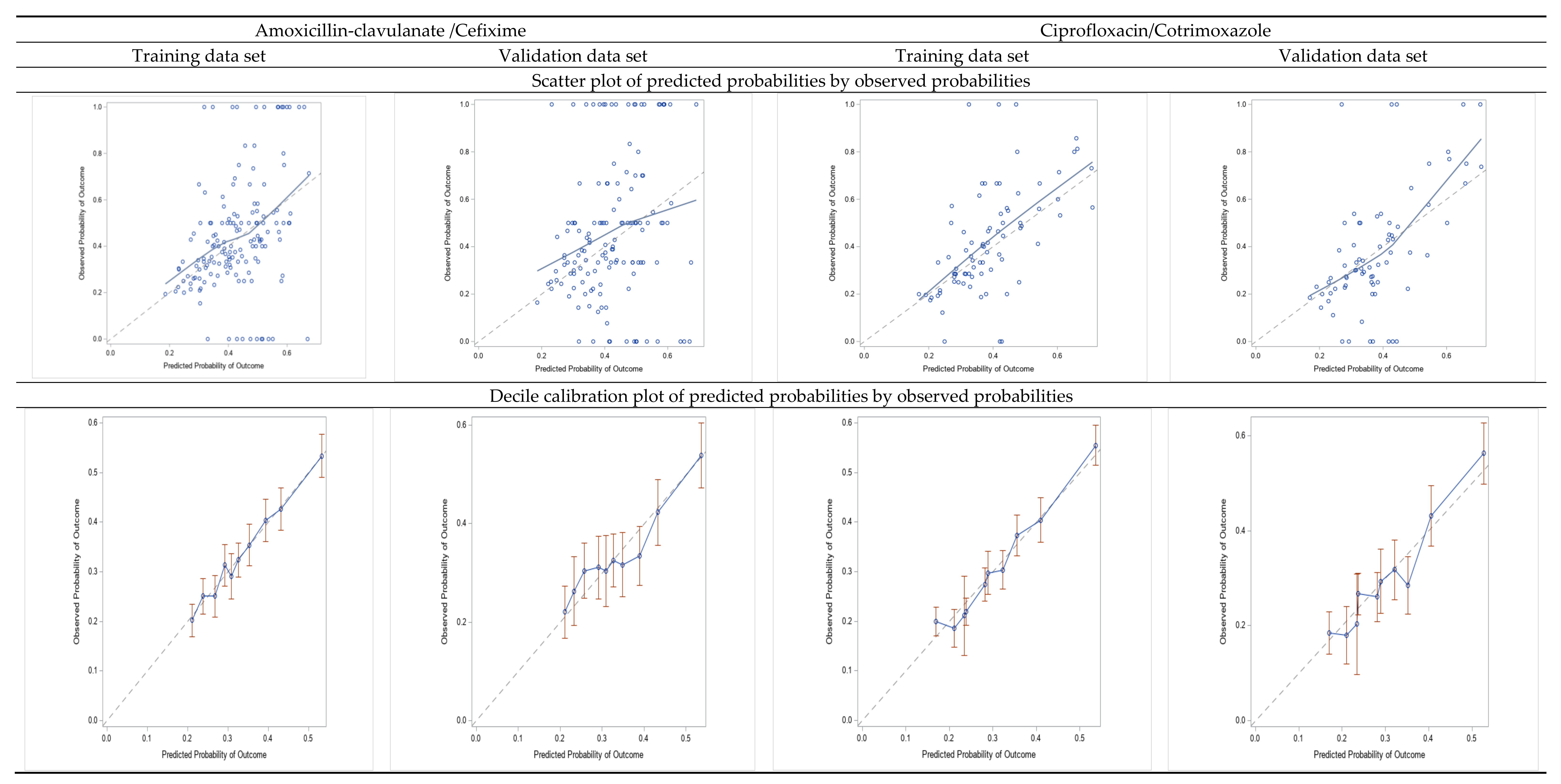
3.2. AMC/CFI and CIP/SXT Resistance Prediction Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Williams, G.J.; Hodson, E.H.; Isaacs, D.; Craig, J.C. Diagnosis and management of urinary tract infection in children. J. Paediatr. Child Health 2012, 48, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Beetz, R.; Westenfelder, M. Antimicrobial therapy of urinary tract infections in children. Int. J. Antimicrob. Agents 2011, 38, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Haralam, M.A.; Kurs-Lasky, M.; Hoberman, A. Association of Renal Scarring with Number of Febrile Urinary Tract Infections in Children. JAMA Pediatr. 2019, 173, 949–952. [Google Scholar] [CrossRef] [PubMed]
- Simões ESilva, A.C.; Oliveira, E.A.; Mak, R.H. Urinary tract infection in pediatrics: An overview. J. Pediatr. 2020, 96, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Toffolo, A.; Ammenti, A.; Montini, G. Long-term clinical consequences of urinary tract infections during childhood: A review. Acta Paediatr. 2012, 101, 1018–1031. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Mattoo, T.K.; Keren, R.; Ivanova, A.; Cui, G.; Moxey-Mims, M.; Majd, M.; Ziessman, H.A.; Hoberman, A. Early Antibiotic Treatment for Pediatric Febrile Urinary Tract Infection and Renal Scarring. JAMA Pediatr. 2016, 170, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.C.; Simpson, J.M.; Williams, G.J.; Lowe, A.; Reynolds, G.J.; McTaggart, S.J.; Hodson, E.M.; Carapetis, J.R.; Cranswick, N.E.; Smith, G.; et al. Antibiotic prophylaxis and recurrent urinary tract infection in children. N. Engl. J. Med. 2009, 361, 1748–1759, Erratum in: N. Engl. J. Med. 2010, 362, 1250. [Google Scholar] [CrossRef] [Green Version]
- RIVUR Trial Investigators; Hoberman, A.; Greenfield, S.P.; Mattoo, T.K.; Keren, R.; Mathews, R.; Pohl, H.G.; Kropp, B.P.; Skoog, S.J.; Nelson, C.P.; et al. Antimicrobial prophylaxis for children with vesicoureteral reflux. N. Engl. J. Med. 2014, 370, 2367–2376. [Google Scholar] [CrossRef] [Green Version]
- Silay, M.S.; Undre, S.; Nambiar, A.K.; Dogan, H.S.; Kocvara, R.; Nijman, R.J.M.; Stein, R.; Tekgul, S.; Radmayr, C. Role of antibiotic prophylaxis in antenatal hydronephrosis: A systematic review from the European Association of Urology/European Society for Paediatric Urology Guidelines Panel. J. Pediatr. Urol. 2017, 13, 306–315. [Google Scholar] [CrossRef]
- Barbieri, E.; Bottigliengo, D.; Tellini, M.; Minotti, C.; Marchiori, M.; Cavicchioli, P.; Gregori, D.; Giaquinto, C.; Da Dalt, L.; Donà, D. Development of a Weighted-Incidence Syndromic Combination Antibiogram (WISCA) to guide the choice of the empiric antibiotic treatment for urinary tract infection in paediatric patients: A Bayesian approach. Antimicrob. Resist. Infect. Control 2021, 10, 74. [Google Scholar] [CrossRef]
- Selekman, R.E.; Shapiro, D.J.; Boscardin, J.; Williams, G.; Craig, J.C.; Brandström, P.; Pennesi, M.; Roussey-Kesler, G.; Hari, P.; Copp, H.L. Uropathogen Resistance and Antibiotic Prophylaxis: A Meta-analysis. Pediatrics 2018, 142, e20180119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazouras, K.; Basmaci, R.; Bielicki, J.; Folgori, L.; Zaoutis, T.; Sharland, M.; Hsia, Y. Antibiotics and Cure Rates in Childhood Febrile Urinary Tract Infections in Clinical Trials: A Systematic Review and Meta-analysis. Drugs 2018, 78, 1593–1604. [Google Scholar] [CrossRef] [PubMed]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazouras, K.; Velali, K.; Tassiou, I.; Anastasiou-Katsiardani, A.; Athanasopoulou, K.; Barbouni, A.; Jackson, C.; Folgori, L.; Zaoutis, T.; Basmaci, R.; et al. Antibiotic treatment and antimicrobial resistance in children with urinary tract infections. J. Glob. Antimicrob. Resist. 2020, 20, 4–10. [Google Scholar] [CrossRef]
- Kantamalee, W.; Santanirand, P.; Saisawat, P.; Boonsathorn, S.; Techasaensiri, C.; Apiwattanakul, N. Outcomes of Empirical Antimicrobial Therapy for Pediatric Community-onset Febrile Urinary Tract Infection in the Era of Increasing Antimicrobial Resistance. Pediatr. Infect. Dis. J. 2020, 39, 121–126. [Google Scholar] [CrossRef]
- Delbet, J.D.; Lorrot, M.; Ulinski, T. An update on new antibiotic prophylaxis and treatment for urinary tract infections in children. Expert Opin Pharmacother. 2017, 18, 1619–1625. [Google Scholar] [CrossRef]
- Farrell, D.J.; Morrissey, I.; De Rubeis, D.; Robbins, M.; Felmingham, D. A UK multicentre study of the antimicrobial susceptibility of bacterial pathogens causing urinary tract infection. J. Infect. 2003, 46, 94–100. [Google Scholar] [CrossRef]
- Edlin, R.S.; Shapiro, D.J.; Hersh, A.L.; Copp, H.L. Antibiotic resistance patterns of outpatient pediatric urinary tract infections. J. Urol. 2013, 190, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Calzi, A.; Grignolo, S.; Caviglia, I.; Calevo, M.G.; Losurdo, G.; Piaggio, G.; Bandettini, R.; Castagnola, E. Resistance to oral antibiotics in 4569 Gram-negative rods isolated from urinary tract infection in children. Eur. J. Pediatr. 2016, 175, 1219–1225. [Google Scholar] [CrossRef]
- Alberici, I.; La Manna, A.; Pennesi, M.; Starc, M.; Scozzola, F.; Nicolini, G.; Toffolo, A.; Marra, G.; Chimenz, R.; Sica, F.; et al. First urinary tract infections in children: The role of the risk factors proposed by the Italian recommendations. Acta Paediatr. 2019, 108, 544–550. [Google Scholar] [CrossRef]
- Yelin, I.; Snitser, O.; Novich, G.; Katz, R.; Tal, O.; Parizade, M.; Chodick, G.; Koren, G.; Shalev, V.; Kishony, R. Personal clinical history predicts antibiotic resistance of urinary tract infections. Nat. Med. 2019, 25, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Temple-Smith, M.; Sanci, L. Urinary tract infections in children: An overview of diagnosis and management. BMJ Paediatr. Open 2019, 3, e000487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammenti, A.; Alberici, I.; Brugnara, M.; Chimenz, R.; Guarino, S.; La Manna, A.; La Scola, C.; Maringhini, S.; Marra, G.; Materassi, M.; et al. Updated Italian recommendations for the diagnosis, treatment and follow-up of the first febrile urinary tract infection in young children. Acta Paediatr. 2020, 109, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Labrosse, M.; Levy, A.; Autmizguine, J.; Gravel, J. Evaluation of a New Strategy for Clean-Catch Urine in Infants. Pediatrics 2016, 138, e20160573. [Google Scholar] [CrossRef] [Green Version]
- Urinary Tract Infection in under 16s: Diagnosis and Management; National Institute for Health and Care Excellence (NICE): London, UK, 2018.
- Esposito, S.; Maglietta, G.; Di Costanzo, M.; Ceccoli, M.; Vergine, G.; La Scola, C.; Malaventura, C.; Falcioni, A.; Iacono, A.; Crisafi, A.; et al. Retrospective 8-Year Study on the Antibiotic Resistance of Uropathogens in Children Hospitalised for Urinary Tract Infection in the Emilia-Romagna Region, Italy. Antibiotics 2021, 10, 1207. [Google Scholar] [CrossRef]
- Okarska-Napierała, M.; Wasilewska, A.; Kuchar, E. Urinary tract infection in children: Diagnosis, treatment, imaging—Comparison of current guidelines. J. Pediatr. Urol. 2017, 13, 567–573. [Google Scholar] [CrossRef]
- Shaikh, N.; Hoberman, A. Urinary Tract Infections in Infants and Children Older than One Month: Clinical Features and Diagnosis; UpToDate: Waltham, MA, USA, 2021. [Google Scholar]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Gönen, M. Analyzing Receiver Operating Characteristic Curves with SAS; SAS Institute Inc.: Cary, NC, USA, 2007. [Google Scholar]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino Sr, R.B. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Montagnani, C.; Tersigni, C.; D’Arienzo, S.; Miftode, A.; Venturini, E.; Bortone, B.; Bianchi, L.; Chiappini, E.; Forni, S.; Gemmi, F.; et al. Resistance Patterns from Urine Cultures in Children Aged 0 to 6 Years: Implications for Empirical Antibiotic Choice. Infect. Drug Resist. 2021, 14, 2341–2348. [Google Scholar] [CrossRef]
- Landi, F.; Bandettini, R.; Rotulo, G.A.; Mesini, A.; Saffioti, C.; Amoroso, L.; Pierri, F.; Guardo, D.; Castagnola, E. Resistance to Antibiotics of Uropathogen Bacteria Isolated from Urine and Blood in Pediatric Cancer Patients: A Single Center, 12-year Study. Pediatr. Infect. Dis. J. 2020, 39, 1106–1110. [Google Scholar] [CrossRef]
- Van Calster, B.; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W.; Topic Group ‘Evaluating diagnostic tests and prediction models’ of the STRATOS initiative. Calibration: The Achilles heel of predictive analytics. BMC Med. 2019, 17, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouwels, K.B.; Freeman, R.; Muller-Pebody, B.; Rooney, G.; Henderson, K.L.; Robotham, J.V.; Smieszek, T. Association between use of different antibiotics and trimethoprim resistance: Going beyond the obvious crude association. J. Antimicrob. Chemother. 2018, 73, 1700–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Martino, M.; Lallo, A.; Kirchmayer, U.; Davoli, M.; Fusco, D. Prevalence of antibiotic prescription in pediatric outpatients in Italy: The role of local health districts and primary care physicians in determining variation. A multilevel design for healthcare decision support. BMC Public Health 2017, 17, 886. [Google Scholar] [CrossRef] [PubMed]
- Youngster, I.; Avorn, J.; Belleudi, V.; Cantarutti, A.; Díez-Domingo, J.; Kirchmayer, U.; Park, B.J.; Peiró, S.; Sanfélix-Gimeno, G.; Schröder, H.; et al. Antibiotic Use in Children—A Cross-National Analysis of 6 Countries. J. Pediatr. 2017, 182, 239–244.e1. [Google Scholar] [CrossRef]
- Jackson, M.A.; Schutze, G.E.; Committee on Infectious Diseases. The Use of Systemic and Topical Fluoroquinolones. Pediatrics 2016, 138, e20162706. [Google Scholar] [CrossRef] [Green Version]
- Adefurin, A.; Sammons, H.; Jacqz-Aigrain, E.; Choonara, I. Ciprofloxacin safety in paediatrics: A systematic review. Arch. Dis. Child. 2011, 96, 874–880. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.; Goldman, J.L. Safety Concerns Surrounding Quinolone Use in Children. J. Clin. Pharmacol. 2016, 56, 1060–1075. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Age at Sampling | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–6 Months | 7 Months–2 Years | 3–7 Years | >7 Years | Total | |||||||||||
| Antibiotics | Resistant | Susceptible | Not Tested | Resistant | Susceptible | Not Tested | Resistant | Susceptible | Not Tested | Resistant | Susceptible | Not Tested | Resistant | Susceptible | Not Tested |
| Amoxicillin-clavulanate | 661 (34.8) | 1239 | 45 | 673 (31.1) | 1493 | 89 | 483 (33.6) | 955 | 60 | 592 (32.3) | 1242 | 64 | 2409 (32.8) | 4929 | 258 |
| Ciprofloxacin | 94 (4.9) | 1842 | 9 | 190 (8.5) | 2056 | 9 | 177 (11.8) | 1317 | 4 | 264 (13.9) | 1630 | 4 | 725 (9.6) | 6845 | 26 |
| Cotrimoxazole | 352 (18.2) | 1585 | 8 | 595 (26.5) | 1653 | 7 | 488 (32.6) | 1007 | 3 | 688 (36.3) | 1206 | 4 | 2123 (28.0) | 5451 | 22 |
| Cefixime | 118 (15.7) | 635 | 1192 | 117 (12.9) | 793 | 1345 | 70 (11.5) | 538 | 890 | 102 (14.4) | 604 | 1192 | 407 (13.7) | 2570 | 4619 |
| Ceftazidime | 159 (8.2) | 1780 | 6 | 172 (7.7) | 2072 | 11 | 100 (6.7) | 1393 | 5 | 137 (7.2) | 1758 | 3 | 568 (7.5) | 7003 | 25 |
| Piperacillin-tazobactam | 244 (12.6) | 1686 | 15 | 247 (11.0) | 1992 | 16 | 148 (9.9) | 1345 | 5 | 202 (10.7) | 1685 | 11 | 841 (11.1) | 6708 | 47 |
| Odds Ratio (95%CI) ^ | ||||||
|---|---|---|---|---|---|---|
| Factors | Amoxicillin-Clavulanate n = 7338 * R = 32.8% | Cefixime, n = 2977 * R = 13.7% | Ciprofloxacin, n = 7570 * R = 9.6% | Cotrimoxazole, n = 7574 * R = 28.0% | Ceftazidime, n = 7571 * R = 7.5% | Piperacillin-Tazobactam, n = 7549 * R = 11.1% |
| Sex, p-value | <0.001 | 0.302 | 0.988 | 0.341 | 0.318 | <0.001 |
| Male vs. female | 1.4 (1.2–1.6) | 1.1 (0.9–1.4) | 1.0 (0.8–1.3) | 0.9 (0.8–1.1) | 1.1 (0.9–1.4) | 1.4 (1.2–1.7) |
| Age at sampling, p-value | 0.002 | <0.001 | <0.001 | <0.001 | <0.001 | 0.0001 |
| 7 months–2 years vs. ≤6 months | 0.9 (0.8–1.1) | 0.6 (0.5–1.0) | 1.8 (1.3–2.4) | 1.5 (1.3–1.8) | 0.9 (0.7–1.2) | 0.9 (0.7–1.1) |
| 3–7 years vs. ≤6 months | 0.9 (0.8–1.1) | 0.5 (0.4–0.8) | 2.2 (1.5–3.1) | 1.8 (1.5–2.2) | 0.6 (0.4–0.9) | 0.7 (0.5–0.9) |
| >7 years vs. ≤6 months | 0.7 (0.6–0.9) | 0.5 (0.3–0.8) | 2.0 (1.3–2.8) | 1.9 (1.5–2.3) | 0.5 (0.3–0.7) | 0.6 (0.5–0.8) |
| Department of admission, p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Nephrology vs. Emergency | 2.5 (2.0–3.1) | 2.4 (1.7–3.6) | 2.2 (1.6–3.3) | 1.8 (1.5–2.3) | 4.0 (2.8–5.8) | 2.9 (2.2–3.8) |
| Surgery/Orthopedics vs. Emergency | 1.5 (1.2–1.9) | 2.3 (1.5–3.6) | 1.8 (1.2–2.6) | 1.1 (0.9–1.3) | 3.2 (2.1–4.7) | 2.0 (1.5–2.7) |
| Infectious Diseases vs. Emergency | 1.4 (1.1–1.8) | 1.4 (0.8–2.4) | 2.1 (1.3–3.1) | 1.4 (1.1–1.8) | 2.0 (1.2–3.2) | 1.3 (0.9–1.9) |
| Hematology/Oncology vs. Emergency | 2.5 (1.8–3.5) | 5.0 (2.9–8.5) | 3.9 (2.5–6.2) | 4.7 (3.2–6.8) | 7.4 (4.5–12.2) | 3.8 (2.6–5.8) |
| Neonatal Pediatric ICU vs. Emergency | 3.1 (2.3–4.3) | 2.9 (1.6–5.5) | 2.8 (1.6–4.7) | 1.4 (1.0–2.0) | 5.0 (3.2–7.9) | 3.5 (2.4–5.1) |
| Others vs. Emergency | 1.6 (1.4–1.9) | 2.2 (1.5–3.1) | 1.7 (1.2–2.3) | 1.2 (1.0–1.4) | 3.5 (2.6–4.8) | 2.1 (1.6–2.7) |
| Previous number of episodes, p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.0004 |
| 1 vs. 0 | 1.2 (1.0–1.3) | 1.3 (1.0–1.7) | 1.3 (1.1–1.6) | 1.2 (1.1–1.4) | 1.5 (1.2–1.9) | 1.4 (1.1–1.7) |
| >1 vs. 0 | 1.4 (1.2–1.7) | 1.8 (1.2–2.5) | 2.0 (1.5–2.7) | 1.5 (1.3–1.8) | 1.6 (1.1–2.1) | 1.4 (1.1–1.8) |
| Factors+A1:E28 | Odds Ratio (95%CI) 1 | β | LRT, p-Value | Points |
|---|---|---|---|---|
| Amoxicillin–clavulanate/Cefixime, n = 5147, | ||||
| Intercept = −1.1136 | ||||
| Sex | <0.001 | |||
| Male vs. female | 1.452 (1.261–1.672) | 0.3731 | 4 | |
| Age at sampling | 0.002 | |||
| 7 months–2 years vs. ≤6 months | 0.862 (0.726–1.024) | −0.148 | −2 | |
| 3–7 years vs. ≤6 months | 0.907 (0.738–1.115) | −0.097 | −1 | |
| >7 years vs. ≤6 months | 0.696 (0.560–0.864) | −0.363 | −4 | |
| Department of admission | <0.001 | |||
| Nephrology vs. Emergency | 2.287 (1.812–2.887) | 0.827 | 10 | |
| Surgery/Orthopedics vs. Emergency | 1.555 (1.220–1.981) | 0.441 | 5 | |
| Infectious Diseases vs. Emergency | 1.321 (0.981–1.780) | 0.279 | 3 | |
| Hematology/Oncology vs. Emergency | 2.428 (1.719–3.430) | 0.887 | 11 | |
| Neonatal or Pediatric ICU vs. Emergency | 3.292 (2.346–4.620) | 1.192 | 14 | |
| Others vs. Emergency | 1.635 (1.340–1.995) | 0.492 | 6 | |
| Previous number of episodes | <0.001 | |||
| 1 vs. 0 | 1.316 (1.122–1.544) | 0.275 | 3 | |
| >1 vs. 0 | 1.421 (1.158–1.743) | 0.351 | 4 | |
| AUC (95% CI) training, n = 5147; | 0.618 (0.601–0.634) | − | 0.17042 | − |
| Brier Score; | 0.214 | |||
| Spiegelhater z test, p-value; | 0.989 | |||
| Hosmer and Lemeshow test, p-value | 0.952 | |||
| AUC (95% CI) validation, n = 2204; | 0.597 (0.572–0.622); | − | − | |
| Brier Score; | 0.216; | |||
| Spiegelhater z test, p-value; | 0.988; | |||
| Hosmer and Lemeshow test, p-value | 0.469 | |||
| Range–point total | – | − | − | −4; 22 |
| Ciprofloxacin/ Cotrimoxazole, n = 5305, | ||||
| Intercept = −1.5882 | ||||
| Age at sampling | <0.001 | |||
| 7 months –2 years vs. ≤6 months | 1.505 (1.241–1.824) | 0.409 | 4 | |
| 3–7 years vs. ≤6 months | 1.925 (1.561–2.372) | 0.655 | 7 | |
| >7 years vs. ≤6 months | 1.953 (1.567–2.433) | 0.669 | 7 | |
| Department of admission | <0.001 | |||
| Nephrology vs. Emergency | 1.900 (1.494–2.416) | 0.642 | 7 | |
| Surgery/Orthopedics vs. Emergency | 1.154 (0.905–1.470) | 0.143 | 2 | |
| Infectious Diseases vs. Emergency | 1.448 (1.064–1.970) | 0.370 | 4 | |
| Hematology/Oncology vs. Emergency | 3.896 (2.585–5.872) | 1.360 | 15 | |
| Neonatal or Pediatric ICU vs. Emergency | 1.503 (1.022–2.211) | 0.408 | 4 | |
| Others vs. Emergency | 1.290 (1.050–1.583) | 0.254 | 3 | |
| Previous number of episodes | <0.001 | |||
| 1 vs. 0 | 1.261 (1.077–1.476) | 0.232 | 3 | |
| >1 vs. 0 | 1.568 (1.304–1.886) | 0.450 | 5 | |
| AUC (95% CI) training, n = 5305; | 0.640 (0.624–0.656) | − | 0.6472 2 | |
| Brier score; | 0.199 | |||
| Spiegelhater z test, p-value; | 0.949 | |||
| Hosmer and Lemeshow test, p-value | 0.189 | |||
| AUC (95% CI) validation, n = 2272; | 0.633 (0.608–0.658) | − | ||
| Brier Score; | 0.198 | |||
| Spiegelhater z test, p-value; | 0.972 | |||
| Hosmer and Lemeshow test, p-value | 0.637 | |||
| Range–point total | – | − | − | 0; 27 |
| Point Total | Amoxicillin-Clavulanate/Cefixime %Estimate of Risk | Ciprofloxacin/Cotrimoxazole %Estimate of Risk |
|---|---|---|
| −4 | 19.0 | - |
| −3 | 20.4 | - |
| −2 | 21.8 | - |
| −1 | 23.2 | - |
| 0 | 24.7 | 17.0 |
| 1 | 26.3 | 18.3 |
| 2 | 27.9 | 19.7 |
| 3 | 29.7 | 21.2 |
| 4 | 31.4 | 22.7 |
| 5 | 33.2 | 24.3 |
| 6 | 35.1 | 26.1 |
| 7 | 37.0 | 27.9 |
| 8 | 39.0 | 29.7 |
| 9 | 41.0 | 31.6 |
| 10 | 43.0 | 33.6 |
| 11 | 45.1 | 35.7 |
| 12 | 47.2 | 37.8 |
| 13 | 49.2 | 40.0 |
| 14 | 51.3 | 42.2 |
| 15 | 53.4 | 44.4 |
| 16 | 55.5 | 46.7 |
| 17 | 57.5 | 48.9 |
| 18 | 59.5 | 51.2 |
| 19 | 61.5 | 53.5 |
| 20 | 63.5 | 55.7 |
| 21 | 65.4 | 58.0 |
| 22 | 67.3 | 60.2 |
| 23 | - | 62.3 |
| 24 | - | 64.4 |
| 25 | - | 66.5 |
| 26 | - | 68.5 |
| 27 | - | 70.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagnasco, F.; Piaggio, G.; Mesini, A.; Mariani, M.; Russo, C.; Saffioti, C.; Losurdo, G.; Palmero, C.; Castagnola, E. Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance. Antibiotics 2022, 11, 720. https://doi.org/10.3390/antibiotics11060720
Bagnasco F, Piaggio G, Mesini A, Mariani M, Russo C, Saffioti C, Losurdo G, Palmero C, Castagnola E. Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance. Antibiotics. 2022; 11(6):720. https://doi.org/10.3390/antibiotics11060720
Chicago/Turabian StyleBagnasco, Francesca, Giorgio Piaggio, Alessio Mesini, Marcello Mariani, Chiara Russo, Carolina Saffioti, Giuseppe Losurdo, Candida Palmero, and Elio Castagnola. 2022. "Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance" Antibiotics 11, no. 6: 720. https://doi.org/10.3390/antibiotics11060720
APA StyleBagnasco, F., Piaggio, G., Mesini, A., Mariani, M., Russo, C., Saffioti, C., Losurdo, G., Palmero, C., & Castagnola, E. (2022). Epidemiology of Antibiotic Resistant Pathogens in Pediatric Urinary Tract Infections as a Tool to Develop a Prediction Model for Early Detection of Drug-Specific Resistance. Antibiotics, 11(6), 720. https://doi.org/10.3390/antibiotics11060720