Abstract
Pseudomonas aeruginosa infections are challenging to treat due to multi-drug resistance (MDR) and the complexity of the patients affected by these serious infections. As new antibiotic therapies come on the market, limited data exist about the effectiveness of such treatments in clinical practice. In this comparative effectiveness study of ceftolozane/tazobactam versus aminoglycoside- or polymyxin-based therapies among hospitalized patients with positive MDR P. aeruginosa cultures, we identified 57 patients treated with ceftolozane/tazobactam compared with 155 patients treated with aminoglycoside- or polymyxin-based regimens. Patients treated with ceftolozane/tazobactam were younger (mean age 67.5 vs. 71.1, p = 0.03) and had a higher comorbidity burden prior to hospitalization (median Charlson 5 vs. 3, p = 0.01) as well as higher rates of spinal cord injury (38.6% vs. 21.9%, p = 0.02) and P. aeruginosa-positive bone/joint cultures (12.3% vs. 0.7%, p < 0.0001). Inpatient mortality was significantly lower in the ceftolozane/tazobactam group compared with aminoglycosides or polymyxins (15.8% vs. 27.7%, adjusted odds ratio 0.39, 95% confidence interval 0.16–0.93). There were no significant differences observed for the other outcomes assessed. In hospitalized patients with MDR P. aeruginosa, inpatient mortality was 61% lower among patients treated with ceftolozane/tazobactam compared to those treated with aminoglycoside- or polymyxin-based regimens.
1. Introduction
Pseudomonas aeruginosa infections are challenging to treat due to multi-drug resistance (MDR) and the complexity of the patients affected by these serious infections [1]. As new antibiotic therapies come on the market, limited data exist on the effectiveness of such treatments in clinical practice among varied clinical populations [2]. Aminoglycosides and polymyxins have been used to treat MDR P. aeruginosa infections but present significant toxicity profiles, including nephrotoxicity, ototoxicity, and neurotoxicity [3,4,5]. Additionally, these agents are associated with suboptimal pharmacokinetics, narrow therapeutic index, and inferior efficacy [4,5,6,7]. Historically, aminoglycosides and polymyxins have been used to treat resistant P. aeruginosa infections. Still, clinical data defining optimal dosing and combination regimens of these agents are lacking [2,8].
P. aeruginosa resistance to aminoglycosides and polymyxins generally remains low (<4% of MDR isolates). Therefore, the benefit–risk profile of these antibiotics pushes the scale toward benefits outweighing risks in MDR and extensively resistant infections [9]. Alternatively, novel anti-pseudomonal antibiotics may be preferred if they result in at least similar rates of positive clinical outcomes without the safety concerns. To date, there have only been select comparative effectiveness studies comparing ceftolozane/tazobactam-based regimens, a novel cephalosporin/beta-lactamase inhibitor combination, with aminoglycoside or polymyxin-based regimens, in patients with MDR P. aeruginosa infections [7,10]. Just one study in the United States has been conducted, including 100 ceftolozane/tazobactam treated patients and 100 aminoglycoside or polymyxin-treated patients from 6 hospitals in Michigan and Ohio [7]. This study found that acute kidney injury was significantly lower in the ceftolozane/tazobactam group (adjusted odds ratio [aOR] 0.08; 95% confidence interval [CI], 0.03–0.22), while no difference was observed in inpatient mortality (aOR 0.62, 95% CI 0.30–1.28). We, therefore, conducted a comparative effectiveness study of ceftolozane/tazobactam versus aminoglycosides or polymyxins in another clinical population, patients treated in Veterans Affairs (VA) hospitals nationally, to assess the real-world benefit–risk profile of ceftolozane/tazobactam compared with aminoglycosides or polymyxins for the treatment of MDR P. aeruginosa infections.
2. Results
We identified 23,176 hospitalized patients with positive P. aeruginosa cultures between January 2015 and April 2018 from 62 medical centers. After applying the inclusion/exclusion criteria shown in (Figure 1), we identified 212 patients with a MDR P. aeruginosa infection, of which 26.9% (n = 57) were treated with ceftolozane/tazobactam, and 73.1% (n = 155) were treated with aminoglycoside- or polymyxin-based regimens. Of the 155 patients in the aminoglycoside or polymyxin treatment group, 132 received aminoglycoside-based therapy (48 tobramycin, 50 amikacin, and 34 gentamicin) and 23 received polymyxin-based therapy (0 colistin, 23 polymyxin B).
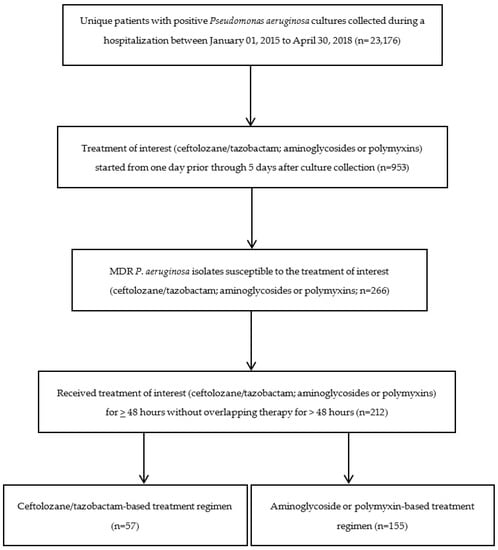
Figure 1.
Flow chart for the study of cohort identification.
Baseline demographics and clinical characteristics are presented in Table 1. Patients treated with ceftolozane/tazobactam-based regimens were younger (mean age 67.5 vs. 71.1, p = 0.03) and less likely to be of Hispanic or Latino ethnicity (1.8% vs. 22.6%, p < 0.001) than patients treated with aminoglycoside- or polymyxin-based regimens. Those treated with ceftolozane/tazobactam also had a higher comorbidity burden (median Charlson 5 vs. 3, p = 0.01) as well as higher rates of spinal cord injury (38.6% vs. 21.9%, p = 0.02) and positive P. aeruginosa cultures in the 30 days before admission (54.4% vs. 38.7%, p = 0.04) than those treated with aminoglycoside- or polymyxin-based regimens. Patients treated with ceftolozane/tazobactam were more likely to be admitted from a nursing home (12.3% vs. 3.2%, p = 0.02) and to have had a previous nursing home stay (5.3% vs. 0%, p = 0.02). There were also significant differences in the P. aeruginosa culture source. A bone/joint source of MDR P. aeruginosa was more common in those treated with ceftolozane/tazobactam (12.3% vs. 0.7%, p < 0.001), and a urine source was less common (22.8% vs. 51.6%, p < 0.001).

Table 1.
Baseline demographics and clinical characteristics of hospitalized patients with positive MDR Pseudomonas aeruginosa infections with ceftolozane/tazobactam or aminoglycoside or polymyxin treatment regimens.
Concomitant treatments were similar between treatment groups, except for meropenem treatment (Table 2). Patients treated with ceftolozane/tazobactam-based regimens were less likely to be treated with concomitant meropenem (15.8% vs. 30.3%, p = 0.03) than those treated with aminoglycoside- or polymyxin-based regimens. Patients treated with ceftolozane/tazobactam were more likely to be treated with meropenem (24.6% vs. 11.6%, p = 0.02) and piperacillin/tazobactam (35.1% vs. 16.8%, p = 0.004) in the 30 days before the treatment of interest than those treated with aminoglycoside- or polymyxin-based regimens. The median time to initiation of the treatment of interest from MDR P. aeruginosa culture collection was three days for both groups.
Table 2.
Treatment characteristics of hospitalized patients with positive MDR Pseudomonas aeruginosa infections with ceftolozane/tazobactam or aminoglycoside or polymyxin treatment regimens.
The overall inpatient mortality rate was 24.5% (52/212). After controlling for confounders, inpatient mortality was significantly lower in patients treated with ceftolozane/tazobactam-based regimens than with aminoglycoside or polymyxin-based regimens (15.8% vs. 27.7%, aOR 0.39, 95% CI 0.16–0.93; Table 3). No significant differences were observed for any of the other clinical outcomes assessed, including acute kidney injury (16.7% vs. 12.4%, aOR 0.86, 95% CI 0.32–2.33).
Table 3.
Comparative effectiveness of ceftolozane/tazobactam compared with aminoglycoside or polymyxin treatment regimens among hospitalized patients with positive MDR Pseudomonas aeruginosa infections.
3. Discussion
In hospitalized patients with MDR P. aeruginosa infections, we found a significantly lower risk of in-hospital mortality among patients treated with ceftolozane/tazobactam-based regimens compared with those treated with aminoglycoside- or polymyxin-based regimens in the national VA Healthcare system. We did not observe differences in 30-day readmission, persistent positive culture, microbiological clearance, or acute kidney injury.
Our national study population had important similarities and differences from the previous comparative effectiveness study conducted in the United States [7]. Our study population was older (mean age 70 years), more male (99%), and more white (69%) than previous work (mean age 59 years, 68% male, and 58% white). In both studies, most patients presented from home (37% of our study vs. 39% previous work), and chronic pulmonary disease, diabetes, and congestive heart failure were common comorbidities. However, the median Charlson Comorbidity Index was higher in our study (4) than in previous work (3) [7]. Most patients in the previous study were admitted to the ICU (69%), and the most common infection type was ventilator-associated pneumonia (52%), with 46% of patients with sepsis. A total of 59% of our patients received intensive care during admission, with only 3.8% and 24% of our patients being diagnosed with pneumonia and sepsis, respectively. Based on culture data, only 36% of our patients had a pseudomonal respiratory tract infection. Patients with pneumonia generally have worse outcomes, and pneumonia is an independent risk factor for death in patients with pseudomonal infections [11,12]. Therefore, patients in previous work may have been more severely ill, leading to differences in the study findings. Interestingly, however, inpatient mortality rates were similar in both studies (25% of our study vs. 23% in previous work) [7].
Additionally, there was higher concomitant antibiotic therapy in both treatment groups in our study compared to previous work, with 96% in the ceftolozane/tazobactam and 94% in the aminoglycoside- or polymyxin-based treatment group having received concomitant antibiotic therapy in our study, as compared to 15% in the ceftolozane/tazobactam and 72% in the aminoglycoside or polymyxin treatment group in previous work [7]. Importantly, we assessed differences between the treatment groups in concomitant therapy from the index date (initiation of ceftolozane/tazobactam or aminoglycosides/polymyxins) through 15 days after the index date, while previous work only considered combination therapy with secondary agents also targeting P. aeruginosa for >48 h. Moreover, unlike our study, the previous study did not consider differences in treatments leading up to the index date, including previous antibiotics for past infections and empiric therapy for the treatment of the MDR P. aeruginosa infection. These important differences in treatment may have impacted the therapy chosen (ceftolozane/tazobactam vs. aminoglycoside or polymyxin-based regimens) and clinical outcomes.
We found no difference in clinical outcomes assessed except inpatient mortality. In previous work, receipt of ceftolozane/tazobactam was associated with increased clinical cure (aOR 2.63; 95% confidence interval [CI], 1.31–5.30) and decreased acute kidney injury (AKI, aOR, 0.08; 95% CI, 0.03–0.22) [7]. We did not assess clinical cure. Clinical cure is a subjective clinical outcome defined as improvement in symptoms. However, improvement in symptoms can occur from administering non-antibiotic medications (e.g., fever reducing, anti-inflammatory, steroids). Further, clinical cure may be defined differently between clinicians and investigators [7,13]. Another small, matched case-control study which included 48 patients from 9 medical centers in Italy with nosocomial pneumonia or bloodstream infection due to MDR or extensively drug-resistant P. aeruginosa found no difference in clinical cure (13% vs. 18%, p = 0.11) and decreased acute kidney injury (0 vs. 8%, p = 0.04) among those treated with ceftolozane/tazobactam versus colistin- or aminoglycoside-based regimens [10]. We did not find any difference in acute kidney injury in our study (aOR, 0.86; 95% CI, 0.32–2.33).
In both the American comparative effectiveness study and the Italian case-control study, similar survival rates were observed among those treated with ceftolozane/tazobactam versus aminoglycoside- or polymyxin-based regimens [7,10]. However, the previous study of patients in the United States may have detected a difference had they had a larger sample size (at least 250 per group) assuming a crude incidence of in-hospital mortality of 20% vs. 25% and an aOR of 0.62. Previous work among patients in Italian medical centers was also likely underpowered to detect a survival benefit [10]. We observed a benefit in in-hospital survival with ceftolozane/tazobactam. Consistent with our findings, a single-center case-control study among 57 patients with hematologic malignancy and P. aeruginosa infection, 50.9% due to MDR and 29.8% to extensively drug-resistant strains, demonstrated a survival benefit associated with ceftolozane/tazobactam [14]. In this single-center case-control study, the 30-day mortality rate was lower among patients treated with ceftolozane/tazobactam versus standard of care antibiotics (5.3% vs. 28.9%; p = 0.045) [14].
Among those with known MDR P. aeruginosa infections, our results and previous work suggest that treatment with ceftolozane/tazobactam may better meet antimicrobial stewardship goals to optimize outcomes and minimize unintended consequences of aminoglycoside- or polymyxin-based treatment, when the isolates are ceftolozane/tazobactam-susceptible [15]. Our results build on previous findings that in patients with serious infections due to MDR P. aeruginosa, ceftolozane/tazobactam has been associated with higher rates of clinical cure and lower rates of nephrotoxicity than aminoglycoside- or polymyxin-based treatment, and ceftolozane/tazobactam may also be associated with an inpatient survival benefit [7,10]. As such, our results support previous studies which have concluded that ceftolozane/tazobactam may be preferred over aminoglycoside- or polymyxin-based treatment for MDR P. aeruginosa infections, especially in patients who may be at higher risk for aminoglycoside or nephrotoxicity, including those who are older and those with underlying comorbidities and illness [3,15]. Moreover, early treatment with ceftolozane/tazobactam may be prudent once susceptibly is known, as previous work has found that starting ceftolozane/tazobactam less than four days after the positive culture is associated with higher clinical and microbiological cure rates [12].
The main limitation to this work is that we were unable to distinguish between actual MDR P. aeruginosa infection and colonization. Only 23.6% of patients had a primary diagnosis of septicemia during admission, and the percentage with primary diagnoses of other infections assessed was only ~<5%. However, when diagnoses were considered anytime during admission, 82% had a diagnosis of an unspecified bacterial infection, 65% had septicemia, and 55% had pneumonia. However, all patients were treated with at least 48 h of ceftolozane/tazobactam, aminoglycosides, or polymyxins, and all MDR P. aeruginosa isolates were susceptible to the treatment of interest.
Another limitation is that we did not assess the dosages or blood levels of study medications and cannot determine whether study drugs were appropriately dosed. Dosing strategies for aminoglycosides and polymyxins vary and optimal dosing targets are debated, resulting in potential overdosing or underdosing with aminoglycosides and polymyxins, as opposed to ceftolozane/tazobactam, which is generally dosed at 1.5 or 3 g every 8 h with normal renal function [7,16]. We also did not capture alternative routes of administration of the study drugs, such as via nebulization.
We used a broad definition of previous and concomitant concurrent antibiotic treatments to control for all antibiotics used in addition to the treatment of interest. However, since we assessed all antibiotic exposures, it is possible that some of the antibiotic exposures were not solely for the treatment of the MDR P. aeruginosa infection. Ceftazidime/avibactam is another novel cephalosporin-beta-lactamase inhibitor therapy used for MDR P. aeruginosa infections that was approved in 2018; however, we did not include patients treated with ceftazidime/avibactam in our study. Due to their approvals after our study time frame, we also did not evaluate other more recently approved antibiotics, such as plazomicin, cefiderocol, and imipenem-cilastatin-relebactam [2].
Channeling bias may have influenced our study findings, as rates of acute kidney injury did not vary between the treatment groups. Patients at higher risk for acute kidney injury may have been preferentially treated with ceftolozane/tazobactam. The generalizability of this study may be limited to older male patients as this study was conducted among patients admitted to VA hospitals. Another limitation is that we assessed all-cause mortality and cannot rule out the impact of underlying conditions on mortality in our older, more clinically complex study population.
4. Materials and Methods
This comparative effectiveness analysis included hospitalized VA patients with positive P. aeruginosa cultures between January 2015 and April 2018. Figure 1 presents a flow chart for the study of cohort identification. Multi-drug resistance was defined as any isolate that tested either intermediate (I) or resistant (R) to at least one antibiotic in at least three of these categories: extended-spectrum cephalosporins (cefepime, ceftazidime), fluoroquinolones (ciprofloxacin, levofloxacin), aminoglycosides (amikacin, gentamicin, tobramycin), carbapenems (imipenem, meropenem, doripenem), and piperacillin (piperacillin, piperacillin/tazobactam). We then included patients (1) treated with ceftolozane/tazobactam or aminoglycosides or polymyxins for ≥48 h without overlapping ceftolozane/tazobactam and aminoglycoside or polymyxin therapy for >48 h, (2) with MDR P. aeruginosa isolates susceptible to the treatment of interest (ceftolozane/tazobactam; or aminoglycoside or polymyxin-based regimens), and (3) treatment initiated one day prior through 5 days after culture collection. The index date was defined as the start date of the treatment of interest.
We assessed the following objective clinical outcomes: inpatient mortality, 30-day readmission from discharge, persistent positive culture (defined as at least one subsequent positive culture after starting the treatment of interest, with and having received at least seven days of any antibiotic therapy), microbiological clearance (defined as a negative follow-up culture among those with follow-up cultures), and acute kidney injury (defined as a serum creatinine increase of 1.5 times the baseline serum creatinine).
We assessed several covariates, including demographics, clinical characteristics, current medical problems, medical history, infection diagnoses, culture source, resistance of the MDR P. aeruginosa isolate, and concomitant antibiotic treatment (Table 1). All antibiotic therapies received from the admission date until the index date were also evaluated. Concomitant treatments were defined as any antibiotic received from the index date through 15 days after initiation of the treatment of interest.
Baseline characteristics of patients in the ceftolozane/tazobactam and aminoglycoside- or polymyxin-based treatment groups were compared using the chi-square, Fisher’s exact test, t-test, or non-parametric Wilcoxon test, as appropriate. Confounding was assessed by controlling for variables significantly associated with the treatment of interest and the clinical outcome. Variables were included in the initial model if the univariate likelihood ratio p-value was ≤0.10 and were retained in the final model if the p-value was <0.05. aOR and 95% confidence intervals (CI) were calculated using automatic stepwise logistic regression. Different models were developed for each clinical outcome, each controlling for identified confounders of the specific exposure–outcome relationship.
5. Conclusions
In hospitalized patients with MDR P. aeruginosa, the risk of inpatient mortality was 61% lower among patients treated with ceftolozane/tazobactam compared with those treated with aminoglycoside or polymyxin-based regimens. Readmission, persistent positive cultures, microbiological clearance, and acute kidney injury did not differ between the treatment groups. Ceftolozane/tazobactam may be a treatment alternative to aminoglycosides or polymyxins for MDR P. aeruginosa infections, as it may have a more favorable safety profile and may be associated with improved clinical outcomes.
Author Contributions
Conception and design of the study: A.R.C., L.A.P., K.L.L. Data generation: A.R.C., E.C.P., V.L. Analysis and/or interpretation of the data: A.R.C., E.C.P., V.L., R.J.D., L.A.P., K.L.L., H.J.A., J.X.L. Preparation or critical revision of the manuscript: A.R.C., E.C.P., V.L., R.J.D., L.A.P., K.L.L., H.J.A., J.X.L. All authors have read and agreed to the published version of the manuscript.
Funding
This work, including the APC, was funded in part by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (Grant number: VEAP 6844).
Institutional Review Board Statement
This study was approved by the Institutional Review Board and Research and Development Committee of the VA Providence Healthcare System (RDC-2018-001).
Informed Consent Statement
Patient consent was waived as this was a retrospective study of existing health records.
Data Availability Statement
The study data may be made available upon reasonable request and approval by the Department of Veterans Affairs.
Acknowledgments
The views expressed are those of the authors and do not necessarily reflect the position or policy of the United States Department of Veterans Affairs. This material is based upon work supported, in part, by the Office of Research and Development, Department of Veterans Affairs.
Conflicts of Interest
A.R.C. has received research funding from AbbVie, Gilead, Merck, and Shionogi and has been a speaker/advisor for Merck. K.L.L. has received research funding or is an advisor/consultant for Merck, Pfizer Pharmaceuticals, Ocean Spray Cranberries, Inc., Nabriva Therapeutics US, Inc., Melinta Therapeutics, Inc., and Tetraphase Pharmaceuticals. L.A.P. was an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA at the time the study was conducted. R.J.D. is an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. There are no other conflicts to report.
References
- Bassetti, M.; Vena, A.; Croxatto, A.; Righi, E.; Guery, B. How to manage Pseudomonas aeruginosa infections. Drugs Context 2018, 7, 212527. [Google Scholar] [CrossRef] [PubMed]
- O'Donnell, J.N.; Bidell, M.R.; Lodise, T.P. Approach to the Treatment of Patients with Serious Multidrug-Resistant Pseudomonas aeruginosa Infections. Pharmacotherapy 2020, 40, 952–969. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.F.; Silva, C.A.; Barbieri, C.D.; Oliveira, G.M.; Zanetta, D.M.; Burdmann, E.A. Prevalence and risk factors for aminoglycoside nephrotoxicity in intensive care units. Antimicrob. Agents Chemother. 2009, 53, 2887–2891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal, L.; Gafter-Gvili, A.; Borok, S.; Fraser, A.; Leibovici, L.; Paul, M. Efficacy and safety of aminoglycoside monotherapy: Systematic review and meta-analysis of randomized controlled trials. J. Antimicrob. Chemother. 2007, 60, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliota, A.F.; Penteado, S.T.; Tonin, F.S.; Fernandez-Llimos, F.; Sanches, A.C. Nephrotoxicity prevalence in patients treated with polymyxins: A systematic review with meta-analysis of observational studies. Diagn. Microbiol. Infect. Dis. 2019, 94, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pogue, J.M.; Kaye, K.S.; Veve, M.P.; Patel, T.S.; Gerlach, A.T.; Davis, S.L.; Puzniak, L.A.; File, T.M.; Olson, S.; Dhar, S.; et al. Ceftolozane/Tazobactam vs Polymyxin or Aminoglycoside-based Regimens for the Treatment of Drug-resistant Pseudomonas aeruginosa. Clin. Infect. Dis. 2020, 71, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Horcajada, J.P.; Montero, M.; Oliver, A.; Sorlí, L.; Luque, S.; Gómez-Zorrilla, S.; Benito, N.; Grau, S. Epidemiology and Treatment of Multidrug-Resistant and Extensively Drug-Resistant Pseudomonas aeruginosa Infections. Clin. Microbiol. Rev. 2019, 32, e00031-19. [Google Scholar] [CrossRef] [PubMed]
- Karlowsky, J.A.; Lob, S.H.; Young, K.; Motyl, M.R.; Sahm, D.F. Activity of imipenem-relebactam against multidrug-resistant Pseudomonas aeruginosa from the United States—SMART 2015–2017. Diagn. Microbiol. Infect. Dis. 2019, 95, 212–215. [Google Scholar] [CrossRef]
- Vena, A.; Giacobbe, D.R.; Mussini, C.; Cattelan, A.; Bassetti, M.; Group, C.S. Clinical Efficacy of Ceftolozane-Tazobactam Versus Other Active Agents for the Treatment of Bacteremia and Nosocomial Pneumonia due to Drug-Resistant Pseudomonas aeruginosa. Clin. Infect. Dis. 2020, 71, 1799–1801. [Google Scholar] [CrossRef]
- Kang, C.I.; Kim, S.H.; Kim, H.B.; Park, S.W.; Choe, Y.J.; Oh, M.D.; Kim, E.C.; Choe, K.W. Pseudomonas aeruginosa bacteremia: Risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin. Infect. Dis. 2003, 37, 745–751. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, J.C.; Satlin, M.J.; Elabor, A.; Saraiya, N.; McCreary, E.K.; Molnar, E.; El-Beyrouty, C.; Jones, B.M.; Dixit, D.; Heil, E.L.; et al. Ceftolozane-Tazobactam for the Treatment of Multidrug-Resistant. Open Forum Infect. Dis. 2018, 5, ofy280. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.F.; de Kraker, M.E.; Sommer, H.; Weiss, E.; Bettiol, E.; Wolkewitz, M.; Nikolakopoulos, S.; Wilson, D.; Harbarth, S. Appropriate endpoints for evaluation of new antibiotic therapies for severe infections: A perspective from COMBACTE’s STAT-Net. Intensive Care Med. 2017, 43, 1002–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Cruz, A.; Alba, N.; Semiglia-Chong, M.A.; Padilla, B.; Rodríguez-Macías, G.; Kwon, M.; Cercenado, E.; Chamorro-de-Vega, E.; Machado, M.; Pérez-Lago, L.; et al. A Case-Control Study of Real-Life Experience with Ceftolozane-Tazobactam in Patients with Hematologic Malignancy and Pseudomonas aeruginosa Infection. Antimicrob. Agents Chemother. 2019, 63, e02340-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pogue, J.M.; Kaye, K.S.; Bonomo, R.A.; Perez, F. Reply to Vena et al. Clin. Infect. Dis. 2020, 71, 1801–1802. [Google Scholar] [CrossRef] [PubMed]
- Puzniak, L.; Dillon, R.; Palmer, T.; Collings, H.; Enstone, A. Real-world use of ceftolozane/tazobactam: A systematic literature review. Antimicrob. Resist. Infect. Control 2021, 10, 68. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).