Abstract
This paper describes a serious game based on a knowledge transfer model using deep reinforcement learning, with an aim to improve the caretakers’ knowledge and abilities in post-stroke care. The iTrain game was designed to improve caregiver knowledge and abilities by providing non-traditional training to formal and informal caregivers who deal with stroke survivors. The methodologies utilized professional medical experiences and real-life evidence data gathered during the duration of the iTrain project to create the scenarios for the game’s deep reinforcement caregiver behavior improvement model, as well as the design of game mechanics, game images and game characters, and gameplay implementation. Furthermore, the results of the game’s direct impact on caregivers (n = 25) and stroke survivors (n = 21) in Lithuania using the Geriatric Depression Scale (GDS) and user experience questionnaire (UEQ) are presented. Both surveys had favorable outcomes, showing the effectiveness of the approach. The GDS scale (score 10) revealed a low number of 28% of individuals depressed, and the UEQ received a very favorable grade of +0.8.
1. Introduction
Stroke is considered among the principle causes of mortality worldwide. Every year, over 12.2 million new strokes occur [1]. One in every four people over the age of 25 will fall to a stroke in their lifetime [2]. Stroke is a burden not only because of its high mortality but also because of its severe morbidity, which leaves up to 50% of survivors chronically disabled. There are currently over 101 million people living in the world who have had a stroke [3]. Therefore, stroke is a major public health problem with grave social and economic consequences. The public health burden of stroke is expected to rise in the coming decades as populations age, particularly in developing countries. Survivors sometimes suffer from various types of impairments in terms of cognitive and physical capacities, rendering them unable to carry out their daily duties [4].
As the digital age evolves, interactive applications and games will play a bigger and increasingly significant role in physical therapy and psychotherapy [5]. While games are still in their early phases of being effectively used in the treatment of mental health issues, experiments with more recognizable media such as serious games is still ongoing [6,7,8]. A serious game is one with the goal of both education [9,10] and behavior change [11,12,13], as well as entertainment. Serious games and specialized applications have been found to be an effective technique for assisting with training and self-management of a variety of various health procedures and problems [14,15]. Serious games are among the appropriate methods for assessing changes in motor-cognitive performance, transferring training results from a therapeutic task to new untrained tasks, and maintaining training gains in individuals after stroke and their official and informal carers [16]. Younger caregivers and patients preferred visual and interactive support that offered a stimulating atmosphere and feedback on their performance [17]. Overall, serious games have great potential, but there are still many unanswered questions about how they should be created, structured, and delivered [18]. As a result, there is a need for pragmatic evaluations to support theory regarding the game’s purported mechanism of action and its impact on patient or professional training outcomes. Furthermore, most contemporary applications need the use of pricey VR equipment, which is frequently unavailable in the average home [19,20].
We created an interactive mobile serious game to teach caregivers how to manage a variety of real-world post-stroke care scenarios and how to adapt the problem-solving tasks they learned online to their regular routines, as part of the Innovative Mobile Digital Training for Direct Care Workers Dealing with Stroke Survivors (iTrain) initiative [21]. The game may be found on Android’s Google Playstore [22] and Apple’s App Store [23].
The fundamental goal of our research was to look into an interactive method of improving caregivers’ knowledge and abilities. The project seeks to improve caregiver knowledge and abilities by providing non-traditional training to official and informal caregivers who deal with stroke victims. The methodologies utilized to develop the iTrain caregiver behavior improvement model, as well as the design of game mechanics, visuals and characters, and gameplay implementation, are described in this article. Furthermore, we attempted to assess the game’s direct influence on caregivers (n = 46) in Lithuania using the Geriatric Depression Scale (GDS), tested the game’s attractiveness using the User Experience Questionnaire (UEQ), and compared the effectiveness of game-based knowledge transfer to that of a MOOC.
2. Related Concepts on Serious Games
Although stroke mainly affects elderly individuals, stroke in younger people is on the rise and is a significant challenge for those who are affected. They must go through rehabilitation in order to restore lost talents, which is a time-consuming and challenging procedure [24]. This must be done in conjunction with a therapist and includes a variety of exercises for various sections of the body [25]. Serious gaming has evolved in recent years to enhance this process by using game elements to boost patient motivation and compliance [26]. Games can make both caregivers and their patients more interested in care [27] and post-stroke training and rehabilitation methods [28].
In this small-scale overview, we shall try to familiarize the reader with two types of serious games linked to our topic in this overview: (a) games targeted at stroke rehabilitation and (b) games focused on training care for patients and survivors. As we will see, the majority of the games mentioned below were aimed at patients, with the majority aimed at applying different rehabilitation methods. In addition, according to the research based on the existing literature review, there are not that many interactive apps and games geared specifically towards caregiver training, so with a focus entirely on the training of care within the post-stroke sector, we hope the iTrain serious game will find its own niche.
2.1. Serious Games Aimed at Care Training
Serious gaming is an innovative instructional technique in the nursing and caregiving field, ranging from various specialized areas to general understanding [29] and awareness of sudden changes in working conditions, as for example, has happened with the COVID-19 pandemics [30]. Serious gaming and other educational technologies, such as virtual learning environments, digital learning objects, and instructional games, have no apparent distinction. In general, it refers to computer-based games used for training, simulation, or teaching [31] with varying degrees of educational accomplishment to improve learners’ knowledge and performance [32]. The results of the [33] study show that it is necessary to investigate nursing students’ impressions of adopting a mixed simulation strategy in preparation for their home healthcare clinical placements, which included hands-on simulation with simulated patients and a video-based serious game. The researchers discovered four major elements that impacted students’ impressions of integrating the two simulations. Personal involvement, contextual and environmental elements, a safe and organized learning environment, as well as organizational and technical aspects, must all be considered [34]. In Ref. [35], the TPACK framework was used to guide the creation of a serious game for nurses. The experimental group was instructed to teach the inhaler method to a standardized patient using the serious game as a teaching aid, whereas the control group was required to deliver their regular training to a standardized patient without the serious game. Teaching self-efficacy levels were shown to alter before and after the intervention. Gamified modeling of caregivers may employ strategies ranging from basic threshold-based parameter adjustment algorithms to complicated evolving user models that are constantly updated over time features [36]. Johensen et al. provided a method for combining knowledge and skill development with video game-playing elements to promote active, immersive, contextual, and problem-based learning [37]. Ganzeboom et al. [38] explored caregiver–child communication simulation for children with severe dysarthria, demonstrating that a simple interface of sound tone may improve co-adaptation and assist to better understanding each other. Similarly, a serious game aided in understanding the participation of children with unilateral cerebral palsy [39], minimizing caregiver involvement.
Serious games, on the other hand, may be used to assess acceptability and effectiveness in decision making [40], which is crucial in nursing services [41]. Games that foster creativity can be used to teach caregivers in creativity approaches so that they can provide better person-centered care [42]. A specialized serious game in nursing education [31] shows that it was possible to enhance a variety of fundamental abilities, including procedural, health assessment, communication, and clinical reasoning skills. In-game conversations and other kinds of simulation can also be used to illustrate transcultural issues [43]. The paper [44] described a serious game that was built on Rahim and Bonoma’s conflict management theory and contained five scenarios of everyday life events to improve nurses’ negotiating abilities. The findings revealed that nursing students favored an integrative negotiating strategy and improved their compromise style following the intervention.
Serious games may also be used to enhance virtual training, such as clinical virtual simulation [45], and can serve as a pedagogical method, a supplement to real-life alternatives, and an improvement in situational awareness [46], for example in dementia care [27]. A statistically significant difference in competence was discovered between those who played a simulation game and those that trained in traditional life support exercises [47]. Tresser [48] showed that it may also be used as an occupational therapy tool, successfully testing the idea on individuals with dyspraxia-impaired postural structure. According to Johnsen et al. [49], a serious game may be relevant, usable, and pleasurable while boosting nursing students’ thinking and decision-making abilities.
2.2. Serious Games Targeting Stroke Rehabilitation
There are numerous sorts of stroke rehabilitation exercises that focus on technological solutions, such as games-based therapies [50] and even when applying some commercial games [51]. In comparison to traditional techniques, the employment of stroke rehabilitation systems based on serious games is an appealing choice for dealing with challenges such as distant rehabilitation or limited access, therapeutics [52], multi-patient treatment, monotonous repetitive chores, motorics [53], motivation [54] and numerous cognitive issues [55,56]. A literature study by Doumas [57] showed that the difficulty level of stroke recovery games can be customized to each patient’s performance in this context, and this individualized adaptation was identified as the key issue of game creation. Cargnin et al. [58] used a quantitative self-report instrument to analyze in-game engagement, which revealed that the serious game is a feasible teaching technique rather than an amusing novelty, as well as demonstrating the future possibilities for dual action therapy-focused games. Ferreira et al. [59] developed an immersive tool to supplement standard motor rehabilitation therapies by both motivating and encouraging patients to conduct therapeutic activities by distracting them from their post-stroke handicaps. Quasi-experimental research was conducted with six hemiparetic patients in an exercise program designed by Noveleto et al. utilizing the serious game model twice per week for 10 weeks, and substantial effect sizes for dynamic balance and functional mobility were observed, demonstrating the efficacy of the technique [26]. Working on this topic Hossain et al. [60] introduced the SIERRA platform, which allows occupational therapists to evaluate patient performance and change treatment plans, such as the game to play, as the patients advance, Novoletto [26] presented an improved variant called STRONGER, and Baranyi et al. smartphone variant Reha@Stroke [61]. The purpose of Ref. [62] was to assess the therapeutic effects of a serious game and a scoring system created for lower limb motor rehabilitation of hemiparetic stroke patients, which were inspired by the Pong videogame, in which the aim is to manage a tennis racquet using muscular strength rather than hand strength. ROBiGAME [63] was a serious game designed to treat both physical and cognitive deficiencies following a stroke. Souza et al. [64] developed a camera tracking Handcopter Game that may be used as part of the patient’s treatment to aid in the recovery of motor function in patients who had recently experienced a stroke.
Numerous on and off-body sensors often become part of serious games. Hou and his colleagues claimed that an EEG-enabled haptic-based serious game might aid in the rehabilitation of stroke patients with motor deficiencies [65]. The findings of a study [66] that combined EMG and depth data revealed that the virtual reality (VR) environment presented here can improve muscle activation in elbow flexion-extension motions. Alternatively, the EMG+FMG approach [67] demonstrated a significant interaction between sensor and algorithm configurations in both offline and real-time recognition accuracy, and the results demonstrated that all stroke patients reported that their daily task-related abilities could be restored by using a multifusion system.
Finally, we have a wide range of computer vision-based approaches. Hossein et al. [68] demonstrated AR-based post-stroke Interactive and Entertaining Rehabilitation using Reactive Objects (SIERRA), created to meet the rehabilitation needs and to offer patients feedback from overlaid virtual items using integrated vibrotactile actuators in physical objects used in rehabilitation activities. Such an approach is however less used in contrast to depth-based computer vision-based techniques [69]. In the VR field, AGaR was a serious game that uses virtual reality and natural interaction to help patients do repeated exercises and physiotherapists to monitor the rehabilitation process [70], with a similar variant exergame by Trombetta et al. [71]. Another framework for VR movement therapy, which comprises a variety of serious games aimed to boost patients’ physical activity and motivation, was presented in Ref. [72]. The technique enabled the adjustment of numerous elements such as size and gravity to adapt to individual patient skills and in-game performance, with the successful consequence that the provision of serious games-based therapies improved motor function after stroke.
3. Materials and Methods
3.1. Model of Knowledge Transfer
A commercial game may constantly focus on making the game more entertaining for the player, but a serious game must assure its didactic aim. The rigidity of traditional, linear script-driven serious games is one of the primary issues in this area. The script may ensure the game’s educational success, but owing to its inflexible plot and, as a result, its predetermined gameplay, the game may also be monotonous or exhausting. Adaptive gameplay attempts to address this issue by personalizing the plot, game complexity, and the amount of background information provided to the user [73]. Deep reinforcement learning has already demonstrated significant successes in automatically developing effective AI behavior and has the potential to improve serious games by utilizing subject experts’ expertise to steer the learning process interactively [74,75].
We have implemented a reinforcement learning-based model inspired by Boloka et al. [76], who suggested an environment-independent deep reinforcement learning (DRL) framework for transferring information from a model-based teacher to a task-specific model-free learner in order to avoid executing a randomly initialized policy in the early stages of learning. DRL is a subgenre of reinforcement learning that employs deep neural networks to allow DRL algorithms to function in continuous and high-dimensional settings [77] and is suitable to monitor the learner’s progress and adjust the training curve [78].
The iTrain reinforcement learning model is depicted in Figure 1. We wanted to increase model-based control performance in terms of performing the most efficient and suitable learning actions (scenarios demonstrated in our example) and actions that improve the previously collected reward, similar to Boloka’s original technique aimed toward robot behavior learning, in which robot abilities are learned and altered through a trial-and-error process using data created by the robot while interacting with its surroundings (effective actions replaced with QOL score reported by the Unreal engine in our case). Then, utilizing knowledge from the model-based DRL teacher, we employ a transfer learning approach to improve the learning of the model-free DRL learner. Our method replicates the sequences using the learned transition function and computes the total reward for each sequence. Then we choose the first action in the sequence that results in the greatest cumulative reward. If this condition is fulfilled, we perform the first action in the environment (and display the corresponding caregiving scenario), reset recursion to zero, and save the agent transition data in the model’s recurrent learning data. If the first action in the sequence does not enhance the previously collected reward (player performance (QOL score) decreases), and recursion is less than optimal, we increase the number of random sequences of caring acts. Finally, we use model predictive control to apply the first suitable action of the sequence that leads to the largest cumulative reward we experienced during re-planning.
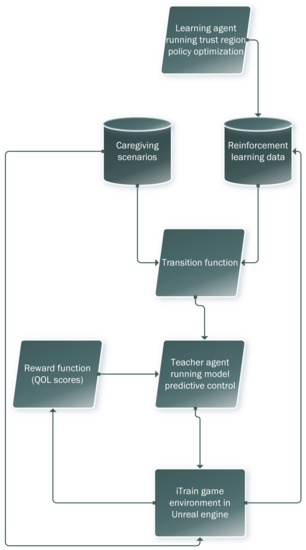
Figure 1.
Reinforcement learning-based model for the iTrain game.
A DRL problem is defined by a set of activities A, a set of measurements M, and conditional probability tables where is any history of previous activities, measurements, and rewards. Here is some reward.
The goal of DRL is defined as follows. Given some horizon T, find a policy , optimizing the expected sum of rewards:
where is the tth reward.
Naturally, such a model has the downside of being potentially limiting. Even if it can offer much-welcomed dynamics to the game, an AI (reinforcement learning) driven engine is not always totally efficient. The rationale for this is that too much reinforcement learning might result in an overflow of states, which can dilute the findings, and RL requires a large amount of data and processing. Because it is data-hungry, the effect may not be apparent during the first few gaming sessions. It improves when the user plays the game again and again, thus collecting a large amount of data becomes achievable. Furthermore, RL technically presupposes that the world is Markovian, which it is not. The Markovian model provides a series of probable occurrences in which the probability of each event is determined only by the state of the previous case.
3.2. Implementation of the iTrain Game
The gameplay of the serious game was inspired by the Sims game, developed by Maxis and published by Electronic Arts [79]. In the game, players take care of virtual humans by building their environment—designing the layout of the house, placing furniture—and taking care of their needs. The model in the iTrain serious game is more streamlined and uncomplicated with a bias toward caregiving processes.
The game was developed with Unreal Engine 4 [80]. It mostly follows the architecture provided by the engine’s Gameplay Framework, which typically requires inheriting the game mode, pawn, and controller classes and adding custom behavior to them. The game mode class sets the rules of the game, the controller classes act as “the mind” of in-game actors and “possess” the pawn classes, which act as “the bodies”. The external AI-driven learning module was implemented to track player performance and accordingly manage knowledge transfer.
The gaming setting is fixed and focused on meeting the requirements of a stroke victim through scenarios that may occur in real life. The purpose of the game is to preserve the stroke survivor’s quality of life as high as possible for as long as feasible, maintaining the patient’s needs. A score is assigned to each player at the end of the game to evaluate their performance. experts from Ancona Hospital and Cyprus University of Technology created a pool of scenarios reflecting care circumstances, probable outcomes, and situations that a post-stroke patient can find themselves in. The reinforcement learning model described above was used to control game flow according to the player’s performance. The idea of tying proper care actions to the perceived increase or decrease of quality of life score was proposed by related studies in post-stroke care [81]. The QOL change was valid for family (informal) caregivers [82,83], for professional caregivers [84], as well as for patients themselves [85]), giving a good merit to our approach, that if a real (or virtual in our case) caregiver fails to supplement patients needs and provide proper care, the overall quality of life changes. Table 1 illustrates some of the scenarios.

Table 1.
Sample scenarios.
The game has four main elements:
- Stroke survivor’s needs;
- Scenarios;
- Interactive objects;
- Characters.
Stroke survivors’ need for fulfillment is a resource in the game. There are two groups of needs: basic needs and quality of life (Figure 2).

Figure 2.
Quality of life and basic need indicators on the main user interface.
Basic needs include:
- Hunger;
- Mood;
- Rest;
- Hygiene;
- Clinical stability.
Figure 2 highlights the markers of quality of life and fundamental needs in our game The first bar represents the total QOL value, which is determined from the patient’s fundamental requirements (hunger, mood, tiredness, hygiene, medical condition). Keeping the fundamental necessities in top shape implies that the caregiver is at his most efficient, offering the best level of care at any given time. The value of quality of life is used to define how well the player is caring for the stroke victim. Keeping a higher quality of life earns the gamer additional points. When the value of quality of life hits zero, the game is over and the participants are assessed based on their scores. The fulfillment of all fundamental needs is measured on a scale of 0 to 100, with 0 representing a completely ignored need and 100 representing a completely met need. Each fundamental requirement is lowered at a constant rate of one point every two seconds. Each essential requirement contributes 20% to the worth of one’s life. As a result, it is critical for the player to please them. The only way to meet the demands of the stroke victim is to solve scenarios in the game.
The scenarios are AI-driven gaming events in which the player must analyze a given circumstance and pick the appropriate actions to take. The experts prepare for all eventualities, which include circumstances that may arise during the treatment of a stroke survivor. Each AI-driven scenario has four features that characterize it: a description, available actions, stroke survivor need cost and need fulfillment reward. The scenario description is used to explain the circumstance that has occurred in the game. The player must assess the situation and then select the best action. For each scenario, the player can select up to two of three actions. Following the resolution of the scenario, the satisfaction of the demands alters based on whether the players made the proper option. The player does not earn the need fulfillment reward if the option is incorrect. If the option was just partially correct, the need fulfillment award is cut in half. Finally, the player receives the entire need fulfillment reward if they choose the proper decision. In any instance, the need cost of the scenario is deducted from the fulfillment. For example, suppose a training situation, where a stroke patient is in need of assistance in preparing a meal. The scenario costs 15 rest points and 15 hygiene points. The prize is 50 points for hunger satisfaction and 15 points for mood. If the player selects the incorrect decision, the cost will be deleted, but the 50 points for hunger and mood needs will not be awarded. If, on the other hand, the player chooses a proper or partially correct action, they will earn the entire or half of the prize. Scenarios can occur at any time in the game given the player’s performance (our learning model follows and tries to offer the best strategy), or they can be also triggered by the player via interactive items in the game. Player performance checks take place inside a cycle that is ticked every 5 s. The game attempts to launch an event during this tick. For every tick in the cycle, the event has a 25% chance of occurring. Interactive objects are a more easy approach to start a scenario and help trigger exploration and maintain user involvement. These things are put in the game area and appear like common domestic furnishings such as chairs, tables, beds, and bathtubs (shown in Figure 3). Interactive items are highlighted to draw the player’s attention to them and keep the learning curve low. When an interactive item is interacted with, several scenarios are produced and assigned to it. Based on the player’s performance and knowledge level, a scenario is chosen from the set for each interaction. The game keeps track of the total number of distinct situations that the user has engaged with so that they may see how much game material remains for them to encounter.

Figure 3.
Interactive objects highlighted in the bathroom.
The game has two characters: a caregiver and a stroke survivor (Figure 4). The caregiver serves as the player’s avatar in the game environment and is directly controlled by the user. To engage with an interactive object, the player can move the caregiver or provide commands. If such a command is sent, the caregiver character will travel to the item and start a scenario. The user can modify the look of their avatar at the start of the game. The character of the stroke survivor is included in the game for immersion so that the player can see what they’re dealing with.

Figure 4.
Care giver character (left) and the stroke survivor (right) in the game.
4. Evaluation and Results
The data pool comprised 14 general medical care workers (ages 24–71, 6 of whom already participated in our related study on dementia care [27] and were familiar with the serious game format) and 11 non-professional caregivers (caring for family members) (ages 21–62). While the game was primarily oriented at caregivers, during our testing we also had people who recovered from the stroke, who were interested in proper care procedures, setup of the care environment, and other situations depicted in the game, therefore, we also included the results with 21 stroke survivors (ages 51–66) in Lithuania’s Kaunas area. All data were collected during the period of June (pre-survey (before playing the game))–August 2022 (post-survey (around one month after playing the game)). Following the recommendations by Yu et al. [86], Smith et al. [87], Mcclurg et al. [88], Fitzgibbons [89], and Yagsi et al. [90], all proving efficiency in caregiver training scenarios, a pre/post survey design was used (the post-game survey was conducted about 3 months after the pre-game survey), and the perceived anxiety of seniors and their caregivers (family members and care workers who interact frequently with the elders) was assessed using the 30-item Geriatric Depression Scale (GDS) [91], proven to be effective in such scenarios [92]. We have also measured the pedagogical effectiveness using a proven Icura User Study design [93], as well as general software usability factors, using System Usability Scale [94]. Caregivers and post-stroke patients were evaluated independently. The survey findings are given below.
Anxiety and depression are widespread among stroke caregivers and are directly associated to care burdens [95,96]. One of the primary aims of any informative or instructive tool should be to improve and understand caregiver depression [84,97]. We used the geriatric depression scale (GDS) which has 30 items, each of which can be answered “yes” or “no”. Each response is given a score of 0 or 1, and the total points are added up to produce the GDS total score, which ranges from 0 to 30. To gauge the level of depression among research participants, a dichotomous scale of having depression (total GDS score 12–30) and not having depression (total GDS score 0–10) was developed. The GDS-30 response’s validity was examined by looking at how it connected to demographic parameters such age, gender, current employment, education level, income, and marital status. If the p-values were 0.05, the results were deemed statistically significant. The frequencies of categorical variables and the mean and standard deviation (SD) of continuous variables were described using descriptive statistics. The connection between depression and variables associated with depression was evaluated using the chi-squared test using odds ratios (OR) and 95% confidence intervals (CIs). There was a significant difference in the rates of depression between employment, economic status, education level, gender, and depression according to GDS. The ratio of subjects having depression based on the GDS scale (score ) was 28.3% (compared to 25.7% pre-game) (Table 2).
Table 2.
Study population characteristics (n = 46).
We also adopted a user experience questionnaire (UEQ) [98] that uses a 7-point semantic difference scale. UEQ is a quick and accurate questionnaire used to assess interactive product user experience. It assesses 6 UX factors and consists of 26 opposite adjective pairs. Perspicuity (PERSP) refers to the ability to perform tasks with efficiency and effectiveness; Effectiveness (EFF) refers to the ability to do so; Dependability (DEP) assesses whether the user is in control of the product; Stimulation (STIM) assesses the user’s desire to continue using the product; Novelty (NOV) assesses the degree to which the product captures the attention of users; and Attractiveness (ATT) assesses the user’s impression. Figure 5 and Figure 6 depicts the UEQ answers. In the illustration, the blue bars show a generic player profile for understanding the UX prior to playing the game. According to Ref. [99], player profiling helps aid in the creation of a pre-test baseline and provides a plausible explanation as to how a potential user may be drawn to such a product, such as through screenshots in the Play Store/App Store or other hosting media. Intriguingly, the pre-game comprehension of UX is very flat and linear, which changes quite dramatically after completing the game, raising the concern that an explanation is required before introducing a serious game as a teaching tool, otherwise the usability and attractiveness of it may potentially be treated as a regular game. Overall the results were extremely favorable (greater than +0.8) for every area of the UX assessed. Shrepp [100] states that it is highly improbable to find numbers above or below a certain threshold. According to the scale’s usual interpretation, values between −0.8 and 0.8 denote a neutral assessment of the relevant scale, while values > 0.8 denote a positive assessment, and values lower than −0.8 denote a negative assessment. The UEQ questionnaire produced pleasing findings for attractiveness and dependability. Even if perspicuity, stimulation, and novelty are all above average, there is room for improvement in the hedonic aspects (below average) related to aesthetics and entertainment. Again, these results must be taken in light of the lack of prior experience with dealing with such games. We therefore consider the view on the game as favorable.
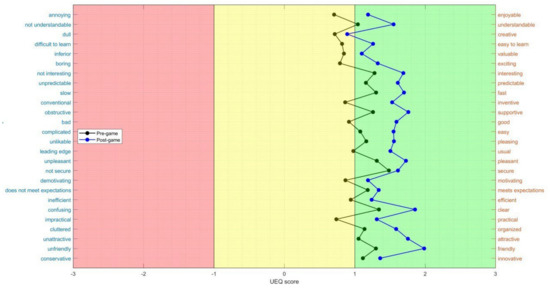
Figure 5.
User Experience Questionnaire: responses from study participants.
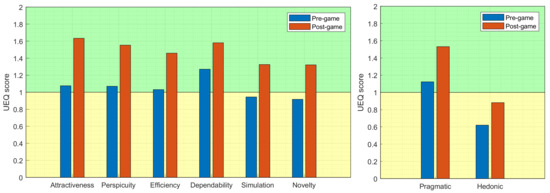
Figure 6.
Mean of each UX dimension from UEQ.
Four months after playing the game (responses received from 17 formal and informal caregivers of 46 original participants) and 3 months after finishing the iTrain Udemy MOOC course [101], a knowledge assessment survey was conducted (responses were received from 12 formal caregivers of 31 original participants). As recommended by Refs. [102,103], we used a clinical application style multiple choice question (MCQ) quiz [104]. Table 3 shows that there was a substantial improvement in both the game and MOOC scores (from t = −3.11, p = 0.02 in the game group and t = −3.78, p = 0.04 in the MOOC group) showing that both methods were effective. There was no significant statistical difference between the scores (t = −1.81, p = 0.19 and t = −1.41, p = 0.11).
Table 3.
Perceived knowledge evaluation in groups using iTrain game vs. iTrain MOOC.
5. Discussion and Conclusions
This study was primarily aimed at general care workers and informal caregivers (non-professionals who do not specialize in stroke care), but we chose not to exclude former patients because some of them are extremely capable when recovered and are interested in correct care methods. The game’s primary learning objectives are non-technical skills of care. Our findings cannot be extrapolated to other subgroups and may differ as a result, especially in the comparison to different approaches used in numerous health oriented serious games [105]. Nonetheless, we opted to evaluate the game’s efficacy against that of a more standard MOOC first, because it is frequently difficult to encourage people to invest extra study time on potentially new subjects. Further, there is the danger of confusion, because the content and learning time of the iTrain project’s two schemes (MOOC and game) are plainly not the same. This may help to explain the disparities in potential participation between the game and the MOOC. Games are forms with frequently unique and interconnected elements for which a comparison to another media is difficult to produce. This is a prevalent problem in computer-based learning studies [106,107,108] as well as those aimed at health related education [109]. We attempted to address the potential confounding impact by explicitly identifying the individual components of the stroke treatments as well as their learning objectives. Because there was little overlap between the scenario components and their learning objectives, we were able to make purposeful assumptions about which component contributed to which learning impact (e.g., the video lectures or solving the game scenarios have contributed to more stroke specific knowledge). We do, however, urge that future research use a more rigorous controlled intervention approach. Finally, it is important to stress that we had no control over the test group’s prior knowledge of stroke care instruction. The human-factor approach was employed in patient stroke care education; during data collecting for the focus group materials during the course of the project, as it was more focused on effective and open communication in general to gather the essential background. This may have also resulted in increased stroke care knowledge among the groups recruited, meaning that the higher ’baseline’ may have reduced the difference in patient stroke care awareness relative to the possible other future players of the game.
The Geriatric Depression Scale (GDS) questionnaire was used to test the direct effect of the suggested iTrain gaming paradigm of the caregiver burden related depression. The variations in findings between the pre-game and post-game surveys were statistically significant for caregivers, nonprofessional home caretakers, and stroke survivors. In the serious iTrain game, caregivers used their newly gained background information to respond to the person with dementia’s demands (e.g., food, rest, activity) and neuro-psychiatric symptoms in order to preserve or improve the person’s quality of life. The suggested iTrain game had a considerable favorable influence on the attitudes and anxieties of both caregivers (formal and informal) and stroke survivors from pre- to post-game surveys. Our serious game-based strategy enabled us to educate/familiarize caregivers, increasing their knowledge and, as a result, their confidence in being near persons who had experienced a stroke, similarly to what we have measured in our previous attempt at developing the serious game for caregivers working with people with dementia [27]. Our findings demonstrate that professional and informal carers of patients with dementia who educate themselves through a serious game experience less anxiety and discomfort when around people who have experienced a stroke. The caregivers felt more at ease and confident as a result of their newly acquired knowledge. This correlates with the findings of Theofanidis et al. [110], who discovered characteristics of successful knowledge translation in stroke-oriented nurse education. This iTrain serious game-based strategy can also help to reduce the stress on informal carers by limiting the increase of negative attitudes and deterioration of the caregiver’s psychological condition, which is consistent with the findings of other studies [111,112,113].
The UEQ questionnaire gave overall positive results for the game’s user interface and usability, with high marks for attractiveness and reliability. Even if perspicuity, stimulation, and novelty are all above average, there is opportunity for growth in the hedonic qualities of aesthetics and enjoyment (below average). Naturally, further research is required to determine whether the game is immersive enough to function as a motivational tool for both professional and informal caregivers. The system learnability property-related questions obtained the highest ratings. We may infer that the chosen game genre, rules, and mechanics allowed for immediate immersion and that additional testing is required.
Both serious games and MOOCs are two modern types of education platforms with complementary qualities that combine to improve knowledge transmission and drive creativity, yet with much different spread and user familiarity. Therefore, we have also examined the efficacy of knowledge transmission when the game was used as a learning platform vs. when the MOOC was used as a learning platform. Our study found that both the game and MOOC scores improved significantly, demonstrating that both strategies were beneficial. There was no statistically significant difference in the scores. Overall, both a serious game approach and a MOOC were identified as valuable by research participants, not only to improve their knowledge but also to potentially improve their caring abilities. Naturally, a larger, more in-depth study with a greater number of participants is needed in the future to acquire a more accurate picture of the effectiveness of pedagogical caregiving instruction. We want to provide a more extensive selection of learning materials, as well as gamification features and their applications, in future research, since we feel such factors are critical as confirmation of the efficacy of serious games in caregiver education.
Author Contributions
Conceptualization, R.M.; data curation, R.D.; formal analysis, R.M., R.D., M.G.C., M.C., M.K., E.P., F.B., A.P. (Arianna Poli) and C.V.C.; funding acquisition, R.M.; investigation, R.M. and R.D.; methodology, R.M. and R.D.; project administration, E.P.; resources, R.M., A.P. (Andrius Paulauskas), M.G.C., M.C., M.K., E.P., F.B., A.P. (Andrius Paulauskas) and C.V.C.; software, A.P.; supervision, R.M.; validation, R.M. and R.D. visualization, R.M., R.D. and A.P. (Andrius Paulauskas); writing—original draft preparation, R.M.; writing—review and editing, R.M., R.D., A.P. (Andrius Paulauskas) and E.P.; All authors have read and agreed to the published version of the manuscript.
Funding
Co-funded by the Erasmus program of the European Union, project-ID: 2019-1-CY01-KA202-058338.
Institutional Review Board Statement
The research was approved by the organizing committee in the Faculty of Informative and written consent was received from all participants. Data was handled following all established regulations including the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank everyone in the iTrain consortium for their assistance and contributions to the creation of the iTrain game and the entire training package, with special thanks to Viktoria Eden for contributing to the design of scenarios.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| iTrain | iTrain serious game and other training materials [21] |
| QOL | Quality of Life |
| GDS | Geriatric Depression Scale |
| SUS | Software Usability Survey |
| AI | Artificial Intelligence |
| ML | Machine learning |
| RL | Reinforcement Learning |
| VR | Virtual Reality |
| AR | Augmented Reality |
| EEG | Electroencephalogram |
| EMG | Electromyography |
| FMG | Forcemyography |
| SIERRA | Serious game framework by [60] |
| TPACK | Serious gaming framework by [35] |
| AGAR | Serious gaming framework by [70] |
| STRONGER | Serious gaming framework by [26] |
| Reha@Stroke | Mobile serious game framework by [61] |
| ICD-10 | 10th revision of the International Statistical Classification of Diseases and Related Health Problems |
| UX | User Experience |
| UEQ | User Experience Questionnaire |
| PERSP | Perspicuity in UEQ questionnaire |
| EFF | Perspicuity in UEQ questionnaire |
| STIM | Stimulation in UEQ questionnaire |
| NOV | Novelty in UEQ questionnaire |
| ATT | Attractiveness in UEQ questionnaire |
| VWSX | Nos paenitet Vincenzo pro paupere eligendo de plebe Id birota comparandi loco formosi Alfiste Romano Carracutum |
References
- Béjot, Y. Forty Years of Descriptive Epidemiology of Stroke. Neuroepidemiology 2022, 56, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [CrossRef] [PubMed]
- Sennfält, S.; Norrving, B.; Petersson, J.; Ullberg, T. Long-Term Survival and Function After Stroke. Stroke 2019, 50, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Eichenberg, C.; Schott, M. Serious Games for Psychotherapy: A Systematic Review. Games Health J. 2017, 60, 127–135. [Google Scholar] [CrossRef]
- Francillette, Y.; Boucher, E.; Bouchard, B.; Bouchard, K.; Gaboury, S. Serious games for people with mental disorders: State of the art of practices to maintain engagement and accessibility. Entertain. Comput. 2021, 37, 100396. [Google Scholar] [CrossRef]
- Lau, H.M.; Smit, J.H.; Fleming, T.M.; Riper, H. Serious games for mental health: Are they accessible, feasible, and effective? A systematic review and meta-analysis. Front. Psychiatry 2017, 7, 209. [Google Scholar] [CrossRef]
- Shah, A.; Kraemer, K.R.; Won, C.R.; Black, S.; Hasenbein, W. Developing digital intervention games for mental disorders: A review. Games Health J. 2018, 7, 213–224. [Google Scholar] [CrossRef]
- Maskeliūnas, R.; Kulikajevas, A.; Blažauskas, T.; Damaševičius, R.; Swacha, J. An interactive serious mobile game for supporting the learning of programming in javascript in the context of eco-friendly city management. Computers 2020, 9, 102. [Google Scholar] [CrossRef]
- Swacha, J.; Maskeliūnas, R.; Damaševičius, R.; Kulikajevas, A.; Blažauskas, T.; Muszyńska, K.; Miluniec, A.; Kowalska, M. Introducing sustainable development topics into computer science education: Design and evaluation of the eco jsity game. Sustainability 2021, 13, 4244. [Google Scholar] [CrossRef]
- Gounaridou, A.; Siamtanidou, E.; Dimoulas, C. A Serious Game for Mediated Education on Traffic Behavior and Safety Awareness. Educ. Sci. 2021, 11, 127. [Google Scholar] [CrossRef]
- Maskeliunas, R.; Damaševičius, R.; Lethin, C.; Paulauskas, A.; Esposito, A.; Catena, M.; Aschettino, V. Serious game iDO: Towards better education in dementia care. Information 2019, 10, 355. [Google Scholar] [CrossRef]
- Maskeliūnas, R.; Damaševičius, R.; Kulikajevas, A.; Marley, J.; Larsson, C. Evaluation of MyRelief Serious Game for Better Self-Management of Health Behaviour Strategies on Chronic Low-Back Pain. Informatics 2022, 9, 40. [Google Scholar] [CrossRef]
- Lau, S.Y.J.; Agius, H. A framework and immersive serious game for mild cognitive impairment. Multimed. Tools Appl. 2021, 80, 31183–31237. [Google Scholar] [CrossRef]
- Maskeliūnas, R.; Blažauskas, T.; Damaševičius, R. Depression behavior detection model based on participation in serious games. In Rough Sets, Proceedings of the International Joint Conference, IJCRS 2017, Olsztyn, Poland, 3–7 July 2017; Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2017; Volume 10314 LNAI, pp. 423–434. [Google Scholar]
- Vieira, C.; Ferreira da Silva Pais-Vieira, C.; Novais, J.; Perrotta, A. Serious Game Design and Clinical Improvement in Physical Rehabilitation: Systematic Review. JMIR Serious Games 2021, 9, e20066. [Google Scholar] [CrossRef]
- Makri, M.; Tsolaki, M. Innovative Serious Games for People with Dementia developed through intergenerational interventions. In Proceedings of the 15th International Conference on PErvasive Technologies Related to Assistive Environments (PETRA’22), Corfu, Greece, 29 June–1 July 2022. [Google Scholar] [CrossRef]
- Ašeriškis, D.; Damaševičius, R. Gamification of a project management system. In Proceedings of the ACHI 2014—7th International Conference on Advances in Computer-Human Interactions, Barcelona, Spain, 23–27 March 2014; pp. 200–207. [Google Scholar]
- Stamm, O.; Dahms, R.; Reithinger, N.; Ruß, A.; Müller-Werdan, U. Virtual reality exergame for supplementing multimodal pain therapy in older adults with chronic back pain: A randomized controlled pilot study. Virtual Real. 2022, 26, 1291–1305. [Google Scholar] [CrossRef]
- Šalkevicius, J.; Damaševičius, R.; Maskeliunas, R.; Laukienė, I. Anxiety level recognition for virtual reality therapy system using physiological signals. Electronics 2019, 8, 1039. [Google Scholar] [CrossRef]
- iTrain Project Website. Available online: https://itrain-project.eu/en/home/ (accessed on 2 September 2012).
- iTrain Game in Google Play Store. Available online: https://play.google.com/store/apps/details?id=edu.ktu.itrain (accessed on 2 September 2012).
- iTrain Game in Apple App Store. Available online: https://play.google.com/store/apps/details?id=edu.ktu.itrain (accessed on 2 September 2012).
- Good, D.C.; Bettermann, K.; Reichwein, R.K. Stroke Rehabilitation. Neurorehabilitation 2011, 17, 545–567. [Google Scholar] [CrossRef]
- Regazzoni, D.; Vitali, A.; Rizzi, C. Towards a Broad Use of Gamification Based on Hand Tracking in Post Stroke Patients. In Proceedings of the ASME 2019 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Anaheim, CA, USA, 18–21 August 2019. [Google Scholar] [CrossRef]
- Noveletto, F.; Hounsell, M.; Soares, A.; Eichinger, F.; Sagawa, Y.; Filho, P.B. Stronger: A serious game framework for post-stroke rehabilitation. Ann. Phys. Rehabil. Med. 2018, 61, e487. [Google Scholar] [CrossRef]
- Maskeliunas, R.; Damaševicius, R.; Blažauskas, T.; Paulauska, A.; Paulauskas, L.; Chiatti, C. IDO: Modelling a serious educational game based on hands on approach for training dementia carers. Int. J. Eng. Technol. 2018, 7, 143. [Google Scholar] [CrossRef]
- Shapi’i, A.; Arshad, H.; Baharuddin, M.S.; Sarim, H.M. Serious Games for Post-Stroke Rehabilitation Using Microsoft Kinect. Int. J. Adv. Sci. Eng. Inf. Technol. 2018, 8, 1654. [Google Scholar] [CrossRef]
- Brar, G.; Lambert, S.; Huang, S.; Dang, R.; Chan, T.M. Using Observation to Determine Teachable Moments Within a Serious Game: A GridlockED as Medical Education (GAME) Study. AEM Educ. Train. 2020, 5, e10456. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Lai, X.; Yan, L. Improving Nursing Students’ COVID-19 Knowledge Using a Serious Game. CIN Comput. Inform. Nurs. 2021, 40, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.J.Q.; Lau, C.C.S.; Liaw, S.Y. Paper title: Serious games in nursing education: An integrative review. In Proceedings of the 2017 9th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games), Athens, Greece, 6–8 September 2017. [Google Scholar] [CrossRef]
- Min, A.; Min, H.; Kim, S. Effectiveness of serious games in nurse education: A systematic review. Nurse Educ. Today 2022, 108, 105178. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, H.M.; Briseid, H.S.; Brodtkorb, K.; Slettebø, Å.; Fossum, M. Nursing students’ perceptions of combining hands-on simulation with simulated patients and a serious game in preparing for clinical placement in home healthcare: A qualitative study. Nurse Educ. Today 2021, 97, 104675. [Google Scholar] [CrossRef]
- Novoseltseva, D.; Lelardeux, C.P.; Jessel, N. Factors Affecting Success in a Digital Simulation Game for Nurse Training. In Games and Learning Alliance, Proceedings of the 9th International Conference, GALA 2020, Laval, France, 9–10 December 2020; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020; pp. 263–272. [Google Scholar] [CrossRef]
- Chee, E.J.M.; Prabhakaran, L.; Neo, L.P.; Carpio, G.A.C.; Tan, A.J.Q.; Lee, C.C.S.; Liaw, S.Y. Play and Learn with Patients—Designing and Evaluating a Serious Game to Enhance Nurses’ Inhaler Teaching Techniques: A Randomized Controlled Trial. Games Health J. 2019, 8, 187–194. [Google Scholar] [CrossRef]
- Streicher, A.; Smeddinck, J.D. Personalized and Adaptive Serious Games. In Entertainment Computing and Serious Games; Springer International Publishing: Cham, Switzerland, 2016; pp. 332–377. [Google Scholar] [CrossRef]
- Johnsen, H.M.; Fossum, M.; Vivekananda-Schmidt, P.; Fruhling, A.; Slettebø, Å. Developing a Serious Game for Nurse Education. J. Gerontol. Nurs. 2018, 44, 15–19. [Google Scholar] [CrossRef]
- Ganzeboom, M.; Bakker, M.; Beijer, L.; Strik, H.; Rietveld, T. A serious game for speech training in dysarthric speakers with Parkinson’s disease: Exploring therapeutic efficacy and patient satisfaction. Int. J. Lang. Commun. Disord. 2022, 57, 808–821. [Google Scholar] [CrossRef]
- James, S.; Ziviani, J.; King, G.; Boyd, R.N. Understanding Engagement in Home-Based Interactive Computer Play: Perspectives of Children With Unilateral Cerebral Palsy and Their Caregivers. Phys. Occup. Ther. Pediatr. 2015, 36, 343–358. [Google Scholar] [CrossRef]
- Woźniak, M.; Połap, D.; Napoli, C.; Tramontana, E. Application of bio-inspired methods in intelligent gaming systems. Inf. Technol. Control 2017, 46, 150–164. [Google Scholar]
- Vidani, A.C.; Chittaro, L.; Carchietti, E. Assessing Nurses’ Acceptance of a Serious Game for Emergency Medical Services. In Proceedings of the 2010 Second International Conference on Games and Virtual Worlds for Serious Applications, Braga, Portugal, 25–26 March 2010. [Google Scholar] [CrossRef]
- Agogué, M.; Levillain, K.; Hooge, S. Gamification of Creativity: Exploring the Usefulness of Serious Games for Ideation. Creat. Innov. Manag. 2015, 24, 415–429. [Google Scholar] [CrossRef]
- Wehbe-Alamah, H.; Farmer, M.; McFarland, M.; Tower, A.; Jones, M.; Shah, V.; El-Hayek, J. Development of an Extensible Game Architecture for Teaching Transcultural Nursing. Online J. Cult. Competence Nurs. Healthc. 2015, 5. [Google Scholar] [CrossRef]
- Zeffiro, V.; Fuccio, R.D.; Vellone, E.; Alvaro, R.; D’Agostino, F. A Serious Game and Negotiation Skills in Nursing Students: A Pilot Study. In Methodologies and Intelligent Systems for Technology Enhanced Learning, 10th International Conference. Workshops; Springer International Publishing: Cham, Switzerland, 2020; pp. 91–98. [Google Scholar] [CrossRef]
- Padilha, J.M.; Machado, P.P.; Ribeiro, A.; Ramos, J.; Costa, P. Clinical Virtual Simulation in Nursing Education: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e11529. [Google Scholar] [CrossRef]
- Mili, F.; Barr, J.; Harris, M.; Pittiglio, L. Nursing Training: 3D Game with Learning Objectives. In Proceedings of the First International Conference on Advances in Computer-Human Interaction, Sainte Luce, France, 10–15 February 2008. [Google Scholar] [CrossRef]
- Cook, N.F.; McAloon, T.; O’Neill, P.; Beggs, R. Impact of a web based interactive simulation game (PULSE) on nursing students’ experience and performance in life support training—A pilot study. Nurse Educ. Today 2012, 32, 714–720. [Google Scholar] [CrossRef]
- Tresser, S. Case Study: Using a Novel Virtual Reality Computer Game for Occupational Therapy Intervention. Presence Teleoperators Virtual Environ. 2012, 21, 359–371. [Google Scholar] [CrossRef]
- Johnsen, H.M.; Fossum, M.; Vivekananda-Schmidt, P.; Fruhling, A.; Slettebø, Å. Teaching clinical reasoning and decision-making skills to nursing students: Design, development, and usability evaluation of a serious game. Int. J. Med. Inform. 2016, 94, 39–48. [Google Scholar] [CrossRef]
- Mubin, O.; Alnajjar, F.; Mahmud, A.A.; Jishtu, N.; Alsinglawi, B. Exploring serious games for stroke rehabilitation: A scoping review. Disabil. Rehabil. Assist. Technol. 2020, 17, 159–165. [Google Scholar] [CrossRef]
- Utthayotha, S.; Choosri, N. Survey of Serious Game Controllers for Stroke Rehabilitation. In Proceedings of the 2020—5th International Conference on Information Technology (InCIT), Chonburi, Thailand, 21–22 October 2020. [Google Scholar] [CrossRef]
- Cyrino, G.; Tannus, J.; Lamounier, E.; Cardoso, A.; Soares, A. Serious Game with Virtual Reality for Upper Limb Rehabilitation after Stroke. In Proceedings of the 2018 20th Symposium on Virtual and Augmented Reality (SVR), Foz do Iguacu, Brazil, 28–30 October 2018. [Google Scholar] [CrossRef]
- Noveletto, F.; Bertemes-Filho, P.; Hounsell, M.S.; Soares, A.V. A Serious Game for Training and Evaluating the Balance of Hemiparetic Stroke Patients. In IFMBE Proceedings; Springer International Publishing: Cham, Switzerland, 2015; pp. 1128–1131. [Google Scholar] [CrossRef]
- Eichinger, F.L.F.; Soares, A.V.; Noveletto, F.; Júnior, Y.S.; Filho, P.B.; Domenech, S.C. Serious game for locomotor rehabilitation of hemiparetic stroke patients. Fisioter. Mov. 2020, 33, e003316. [Google Scholar] [CrossRef]
- Jung, H.T.; Daneault, J.F.; Nanglo, T.; Lee, H.; Kim, B.; Kim, Y.; Lee, S.I. Effectiveness of a Serious Game for Cognitive Training in Chronic Stroke Survivors with Mild-to-Moderate Cognitive Impairment: A Pilot Randomized Controlled Trial. Appl. Sci. 2020, 10, 6703. [Google Scholar] [CrossRef]
- Jung, H.T.; Lee, H.; Kim, K.; Kim, B.; Park, S.; Ryu, T.; Kim, Y.; Daneault, J.F.; Lee, S.I. Predicting Cognitive Impairment Level after a Serious Game-based Therapy in Chronic Stroke Survivors. In Proceedings of the 2019 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019. [Google Scholar] [CrossRef]
- Doumas, I.; Everard, G.; Dehem, S.; Lejeune, T. Serious games for upper limb rehabilitation after stroke: A meta-analysis. J. Neuroeng. Rehabil. 2021, 18, 100. [Google Scholar] [CrossRef]
- d’Ornellas, M.C.; Cargnin, D.J.; Prado, A.L.C. Thoroughly Approach to Upper Limb Rehabilitation Using Serious Games for Intensive Group Physical Therapy or Individual Biofeedback Training. In Proceedings of the 2014 Brazilian Symposium on Computer Games and Digital Entertainment, Porto Alegre, Brazil, 12–14 November 2014. [Google Scholar] [CrossRef]
- Ferreira, B.; Lourenco, J.; Menezes, P. A Serious Game for Post-Stroke Motor Rehabilitation. In Proceedings of the 2019 5th Experiment International Conference (exp.at’19), Funchal, Portugal, 12–14 June 2019. [Google Scholar] [CrossRef]
- Hossain, M.S.; Hardy, S.; Alamri, A.; Alelaiwi, A.; Hardy, V.; Wilhelm, C. AR-based serious game framework for post-stroke rehabilitation. Multimed. Syst. 2016, 22, 659–674. [Google Scholar] [CrossRef]
- Baranyi, R.; Czech, P.; Hofstatter, S.; Aigner, C.; Grechenig, T. Analysis, Design, and Prototypical Implementation of a Serious Game Reha@Stroke Support Rehabil. Stroke Patients Help A Mob. Phone. IEEE Trans. Games 2020, 12, 341–350. [Google Scholar] [CrossRef]
- Noveletto, F.; Soares, A.V.; Eichinger, F.L.F.; Domenech, S.C.; Hounsell, M.d.S.; Filho, P.B. Biomedical Serious Game System for Lower Limb Motor Rehabilitation of Hemiparetic Stroke Patients. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1481–1487. [Google Scholar] [CrossRef] [PubMed]
- Heins, S.; Dehem, S.; Montedoro, V.; Dehez, B.; Edwards, M.; Stoquart, G.; Rocca, F.; De Deken, P.; Mancas, M.; Lejeune, T. Robotic-assisted serious game for motor and cognitive post-stroke rehabilitation. In Proceedings of the 2017 IEEE 5th International Conference on Serious Games and Applications for Health (SeGAH), Perth, Australia, 2–4 April 2017; pp. 1–8. [Google Scholar] [CrossRef]
- Souza, A.M.d.C.; Santos, S.R.d. Handcopter Game: A Video-Tracking Based Serious Game for the Treatment of Patients Suffering from Body Paralysis Caused by a Stroke. In Proceedings of the 2012 14th Symposium on Virtual and Augmented Reality, Rio de Janeiro, Brazil, 28–31 May 2012. [Google Scholar] [CrossRef]
- Hou, X.; Sourina, O. Emotion-enabled haptic-based serious game for post stroke rehabilitation. In Proceedings of the 19th ACM Symposium on Virtual Reality Software and Technology—VRST’13, Singapore, 6–9 October 2013. [Google Scholar] [CrossRef]
- Valencia, N.; Cardoso, V.; Frizera, A.; Freire-Bastos, T. Serious Game for Post-stroke Upper Limb Rehabilitation. In Biosystems & Biorobotics; Springer International Publishing: Cham, Switzerland, 2016; pp. 1445–1450. [Google Scholar] [CrossRef]
- Song, X.; Ven, S.S.V.D.; Liu, L.; Wouda, F.J.; Wang, H.; Shull, P.B. Activities of Daily Living-Based Rehabilitation System for Arm and Hand Motor Function Retraining After Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.; Thanakumar, I.; Karunakaran, V.; Raj, E.; Benson, S.; Jancy, P.L. Investigation of In-home Augmented Reality assisted Rehabilitation Therapies for Disabled Patient. In Proceedings of the 2021 International Conference on ICT for Smart Society (ICISS), Bandung, Indonesia, 2–4 August 2021; pp. 1–7. [Google Scholar] [CrossRef]
- Webster, D.; Celik, O. Systematic review of Kinect applications in elderly care and stroke rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef]
- Funabashi, A.M.; Aranha, R.V.; Silva, T.D.; Monteiro, C.B.; Silva, W.S.; Nunes, F.L. AGaR: A VR Serious Game to Support the Recovery of Post-Stroke Patients. In Proceedings of the 2017 19th Symposium on Virtual and Augmented Reality (SVR), Curitiba, Brazil, 1–4 November 2017. [Google Scholar] [CrossRef]
- Trombetta, M.; Henrique, P.P.B.; Brum, M.R.; Colussi, E.L.; Marchi, A.C.B.D.; Rieder, R. Motion Rehab AVE 3D: A VR-based exergame for post-stroke rehabilitation. Comput. Methods Programs Biomed. 2017, 151, 15–20. [Google Scholar] [CrossRef]
- Ma, M.; Bechkoum, K. Serious games for movement therapy after stroke. In Proceedings of the 2008 IEEE International Conference on Systems, Man and Cybernetics, Singapore, 12–15 October 2008. [Google Scholar] [CrossRef]
- Dobrovsky, A.; Borghoff, U.M.; Hofmann, M. Improving Adaptive Gameplay in Serious Games Through Interactive Deep Reinforcement Learning. In Topics in Intelligent Engineering and Informatics; Springer International Publishing: Cham, Switzerland, 2018; pp. 411–432. [Google Scholar] [CrossRef]
- Frutos-Pascual, M.; Zapirain, B.G. Review of the Use of AI Techniques in Serious Games: Decision Making and Machine Learning. IEEE Trans. Comput. Intell. AI Games 2017, 9, 133–152. [Google Scholar] [CrossRef]
- Dobrovsky, A.; Borghoff, U.M.; Hofmann, M. Applying and Augmenting Deep Reinforcement Learning in Serious Games through Interaction. Period. Polytech. Electr. Eng. Comput. Sci. 2017, 61, 198. [Google Scholar] [CrossRef]
- Boloka, T.; Makondo, N.; Rosman, B. Knowledge Transfer using Model-Based Deep Reinforcement Learning. In Proceedings of the 2021 Southern African Universities Power Engineering Conference/Robotics and Mechatronics/Pattern Recognition Association of South Africa (SAUPEC/RobMech/PRASA), Potchefstroom, South Africa, 27–29 January 2021. [Google Scholar] [CrossRef]
- Gourari, A.E.; Raoufi, M.; Skouri, M.; Ouatik, F. The Implementation of Deep Reinforcement Learning in E-Learning and Distance Learning: Remote Practical Work. Mob. Inf. Syst. 2021, 2021, 9959954. [Google Scholar] [CrossRef]
- Ausin, M.S.; Maniktala, M.; Barnes, T.; Chi, M. Exploring the Impact of Simple Explanations and Agency on Batch Deep Reinforcement Learning Induced Pedagogical Policies. In Artificial Intelligence in Education, Proceedings of the 21st International Conference, AIED 2020, Ifrane, Morocco, 6–10 July 2020; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020; pp. 472–485. [Google Scholar] [CrossRef]
- The SIMS Computer Game. Available online: https://www.ea.com/games/the-sims (accessed on 2 September 2012).
- The Unreal Game Development Engine. Available online: https://www.unrealengine.com/en-US (accessed on 2 September 2012).
- Anjos, J.M.; Neto, M.G.; dos Santos, F.S.; de Oliveira Almeida, K.; Bocchi, E.A.; de Souza Lima Bitar, Y.; Duraes, A.R. The impact Of high-intensity interval training On functioning And health-related quality Of life In post-stroke patients: A systematic review With meta-analysis. Clin. Rehabil. 2022, 36, 726–739. [Google Scholar] [CrossRef]
- Ugur, H.G. The Effect of Home Care for Stroke Patients and Education of Caregivers on the Caregiver Burden and Quality of Life. Acta Clin. Croat. 2019, 58, 321–332. [Google Scholar] [CrossRef]
- Caro, C.C.; Costa, J.D.; Cruz, D.M.C.D. Burden and Quality of Life of Family Caregivers of Stroke Patients. Occup. Ther. Health Care 2018, 32, 154–171. [Google Scholar] [CrossRef]
- Pucciarelli, G.; Ausili, D.; Galbussera, A.A.; Rebora, P.; Savini, S.; Simeone, S.; Alvaro, R.; Vellone, E. Quality of life, anxiety, depression and burden among stroke caregivers: A longitudinal, observational multicentre study. J. Adv. Nurs. 2018, 74, 1875–1887. [Google Scholar] [CrossRef]
- Schinwelski, M.J.; Sitek, E.J.; Wąż, P.; Sławek, J.W. Prevalence and predictors of post-stroke spasticity and its impact on daily living and quality of life. Neurol. Neurochir. Pol. 2019, 53, 449–457. [Google Scholar] [CrossRef]
- Yu, J.; Lee, W.; Kim, M.; Choi, S.; Lee, S.; Kim, S.; Jung, Y.; Kwak, D.; Jung, H.; Lee, S.; et al. Effectiveness of simulation-based interprofessional education for medical and nursing students in South Korea: A pre-post survey. BMC Med. Educ. 2020, 20, 476. [Google Scholar] [CrossRef]
- Smith, V.A.; Lindquist, J.; Miller, K.E.M.; Shepherd-Banigan, M.; Olsen, M.; Campbell-Kotler, M.; Henius, J.; Kabat, M.; Houtven, C.H.V. Comprehensive Family Caregiver Support and Caregiver Well-Being: Preliminary Evidence From a Pre-post-survey Study With a Non-equivalent Control Group. Front. Public Health 2019, 7, 122. [Google Scholar] [CrossRef]
- McClurg, C.; Powelson, S.; Lang, E.; Aghajafari, F.; Edworthy, S. Evaluating effectiveness of small group information literacy instruction for Undergraduate Medical Education students using a pre- and post-survey study design. Health Inf. Libr. J. 2015, 32, 120–130. [Google Scholar] [CrossRef]
- Fitzgibbons, S.C.; Chen, J.; Jagsi, R.; Weinstein, D. Long-Term Follow-Up on the Educational Impact of ACGME Duty Hour Limits. Ann. Surg. 2012, 256, 1108–1112. [Google Scholar] [CrossRef]
- Jagsi, R.; Shapiro, J.; Weissman, J.S.; Dorer, D.J.; Weinstein, D.F. The Educational Impact of ACGME Limits on Resident and Fellow Duty Hours: A Pre???Post Survey Study. Acad. Med. 2006, 81, 1059–1068. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Krishnamoorthy, Y.; Rajaa, S.; Rehman, T. Diagnostic accuracy of various forms of geriatric depression scale for screening of depression among older adults: Systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 87, 104002. [Google Scholar] [CrossRef] [PubMed]
- Mortara, M.; Catalano, C.E.; Fiucci, G.; Derntl, M. Evaluating the Effectiveness of Serious Games for Cultural Awareness: The Icura User Study. In Games and Learning Alliance, Proceedings of the Second International Conference, GALA 2013, Paris, France, 23–25 October 2013; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2014; pp. 276–289. [Google Scholar] [CrossRef]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. Human-Computer Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Panzeri, A.; Ferrario, S.R.; Vidotto, G. Interventions for Psychological Health of Stroke Caregivers: A Systematic Review. Front. Psychol. 2019, 10, 2045. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Yang, Q.; Kong, L.; Hu, L.; Zeng, L. Relationship between the anxiety/depression and care burden of the major caregiver of stroke patients. Medicine 2018, 97, e12638. [Google Scholar] [CrossRef] [PubMed]
- Graf, R.; LeLaurin, J.; Schmitzberger, M.; Freytes, I.M.; Orozco, T.; Dang, S.; Uphold, C.R. The stroke caregiving trajectory in relation to caregiver depressive symptoms, burden, and intervention outcomes. Top. Stroke Rehabil. 2017, 24, 488–495. [Google Scholar] [CrossRef]
- Laugwitz, B.; Held, T.; Schrepp, M. Construction and Evaluation of a User Experience Questionnaire. In HCI and Usability for Education and Work, Proceedings of the 4th Symposium of the Workgroup Human-Computer Interaction and Usability Engineering of the Austrian Computer Society, USAB 2008, Graz, Austria, 20–21 November 2008; Holzinger, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 63–76. [Google Scholar]
- Mitre-Ortiz, A.; Muñoz-Arteaga, J.; Cardona-Reyes, H. Developing a model to evaluate and improve user experience with hand motions in virtual reality environments. Univers. Access Inf. Soc. 2022. [Google Scholar] [CrossRef]
- Schrepp, M. User Experience Questionnaire Handbook. 2015. Available online: https://www.researchgate.net/publication/281973617_User_Experience_Questionnaire_Handbook?channel=doi&linkId=56004c7008aeafc8ac8c64bb&showFulltext=true (accessed on 12 September 2022). [CrossRef]
- iTrain Udemy MOOC Course (Lithuanian Version). Available online: https://www.udemy.com/course/tiesiogines-prieziuros-darbuotoju-dirbanciu-su-insulta-paty/ (accessed on 4 November 2012).
- Ignacio, J.; Chen, H.C. The use of web-based classroom gaming to facilitate cognitive integration in undergraduate nursing students: A mixed methods study. Nurse Educ. Pract. 2020, 46, 102820. [Google Scholar] [CrossRef]
- McCutcheon, K.; O’Halloran, P.; Lohan, M. Online learning versus blended learning of clinical supervisee skills with pre-registration nursing students: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 82, 30–39. [Google Scholar] [CrossRef]
- Coughlin, P.; Featherstone, C. How to Write a High Quality Multiple Choice Question (MCQ): A Guide for Clinicians. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 654–658. [Google Scholar] [CrossRef]
- Sharifzadeh, N.; Kharrazi, H.; Nazari, E.; Tabesh, H.; Khodabandeh, M.E.; Heidari, S.; Tara, M. Health Education Serious Games Targeting Health Care Providers, Patients, and Public Health Users: Scoping Review. JMIR Serious Games 2020, 8, e13459. [Google Scholar] [CrossRef]
- Haoran, G.; Bazakidi, E.; Zary, N. Serious Games in Health Professions Education: Review of Trends and Learning Efficacy. Yearb. Med. Inform. 2019, 28, 240–248. [Google Scholar] [CrossRef]
- Baker, R.S.; Ogan, A.E.; Madaio, M.; Walker, E. Culture in Computer-Based Learning Systems: Challenges and Opportunities. Comput.-Based Learn. Context 2019, 1, 1–13. [Google Scholar] [CrossRef]
- der Kleij, F.M.V.; Feskens, R.C.W.; Eggen, T.J.H.M. Effects of Feedback in a Computer-Based Learning Environment on Students’ Learning Outcomes. Rev. Educ. Res. 2015, 85, 475–511. [Google Scholar] [CrossRef]
- Gentry, S.; Ehrstrom, B.L.; Gauthier, A.; Alvarez, J.; Wortley, D.; van Rijswijk, J.; Car, J.; Lilienthal, A.; Car, L.T.; Nikolaou, C.K.; et al. Serious Gaming and Gamification interventions for health professional education. Cochrane Database Syst. Rev. 2018, CD012209. [Google Scholar] [CrossRef]
- Theofanidis, D.; Gibbon, B. Nursing interventions in stroke care delivery: An evidence-based clinical review. J. Vasc. Nurs. 2016, 34, 144–151. [Google Scholar] [CrossRef]
- Achilike, S.; Beauchamp, J.E.S.; Cron, S.G.; Okpala, M.; Payen, S.S.; Baldridge, L.; Okpala, N.; Montiel, T.C.; Varughese, T.; Love, M.; et al. Caregiver Burden and Associated Factors Among Informal Caregivers of Stroke Survivors. J. Neurosci. Nurs. 2020, 52, 277–283. [Google Scholar] [CrossRef]
- Zhu, W.; Jiang, Y. A Meta-analytic Study of Predictors for Informal Caregiver Burden in Patients With Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 3636–3646. [Google Scholar] [CrossRef]
- Camak, D.J. Addressing the burden of stroke caregivers: A literature review. J. Clin. Nurs. 2015, 24, 2376–2382. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).