
The “Four Principles” of Western Medical Bioethics and the Bioethics of Shīʿī Islam in Iran—Is the Claim of Universality by Both Justified?

{kind=link}
Abstract
1. Introduction
2. Results
2.1. Historical Development of Bioethics
- Western Bioethics
- Shī’ī bioethics
2.2. Normative Basis of Western Bioethics
2.3. Normative Basis of Shīʿī Bioethics
2.4. The Bioethical Challenges Exemplified via the Iranian Program of the Prevention of ß-Thalassemia Major (ßTMa)
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary
| Allele | An allele is a variant form of a gene, at the gene’s specific place on a chromosome. With the pairing of chromosomes during fertilization two genes are paired. If the two paired genes contain the same allele, the gene is homozygote, with different alleles heterozygote with respect this gene. |
| Belmont Report | The Belmont Report was commissioned by the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research (USA). The Commission, created as a result of the National Research Act of 1974, was charged with identifying the basic ethical principles that should underlie the conduct of biomedical and behavioral research involving human subjects and developing guidelines to assure that such research is conducted in accordance with those principles. For details see https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/index.html, accessed on 28 August 2021. (Department of Health and Human Services (HHS) 2021) |
| Beta-thalassemia major (ßTMa) | ßTMa is characterized by mutations on chromosome 11, encoding the ß-chain of hemoglobin A, i.e., the oxygen carrier-protein in red blood cells consisting of 2 a- and 2 ß-chains. Without functional ß-chains (ß0), i.e., a genotype of ß0/ß0, ßTMa, the most severe form of thalassemia, will occur. Intermediate forms, genotype ß0/ß+, or ß+/ß+, (ß+, partial function of the ß chain) are defined as ß-thalassemia intermedia, while those least affected are heterozygous with a genotype ß/ß+ or ß/ß0, resulting in mild anemia, i.e., ß-thalassemia minor (ßTMi). So far, 52 different mutations, with different mutations in 21% of consanguineous couples, indicate the heterogenous picture of ßTMa in Iran. These genetic variants result in different phenotypes. Predicting these phenotypes, i.e., classifying the disease into categories of severe or intermediate, requires costly genetic screening (Rahimi 2013). ßTMi requires no medical treatment, while those with ßTMa require regular blood transfusions. Regular blood transfusions lead to iron-overload necessitating chelation therapy, i.e., iron is bound to a chelating agent which then is excreted. Despite and in part related to transfusion therapy, patients with ßTMa suffer major complications of the disease, such as a reduced growth rate in children, diabetes mellitus (5.4%), heart failure (6.4%), cardiac arrhythmias (5.0%), hypothyroidism (11.6%), hypoparathyroidism, adrenal insufficiency and hypogonadism (reduced sexual function and/or infertility, 55%), thrombosis (1.1%) and HIV infection (1.8%). Antibody formation, i.e., alloimmunization prohibits further transfusion therapy. Today, therapy offers patients a life expectancy well into adulthood with integration into employment and marriage. However, ultimately the patients die of the disease mostly due to heart failure. In the United Kingdom up to the year 2000 50% of patients died before age 35 years, today 80% of the patients live longer than 40 years (Borgna-Pignatti et al. 2006; Needs et al. 2022). |
| Bonobo | Pan paniscus, i.e., a pygmy chimpanzee, one of the two species making up the genus Pan. Scientifical classification: Kingdom: Animalia, Phylum: Chordata, Class: Mammalia, Order: Primates, Suborder: Haplorhini, Infraorder: Simiiformes, Family: Hominoidae, Subfamily: Hominidae, Tribe: Homini, Genus: Pan, Species: P. paniscuis (Schwartz 1929). |
| Carrier status | A “genetic” carrier is a carrier of either an autosomal recessive disease or of a X-linked disorder or a balanced chromosomal rearrangement. Being a carrier does usually not affect the carrier’s health but could have consequences for the offspring (Borry et al. 2013). |
| Clinical | Clinical refers to the direct observation of the patient. In clinical medicine medical the physician assesses patients in order to diagnose, treat or prevent disease. |
| Communitarianism | Communitarian justice holds a just distribution to each person according to principles of fair distribution derived from concepts of the good developed in moral communities (Beauchamps and Childress 2019). |
| Cost effectiveness analysis (CEA) | A strategy on which heath care resource rationing is based. If healthcare is defined as a “health need”, health resource efficiency, i.e., the ultimate goal of CEA using health resources to minimize ill health without wasting resources, is asked for. To achieve distributive fairness parameters of healthcare metrics (for instance quality-of-life years (QUALY) as a metric for the benefit achieved) and efficiency as the costs of achieving a benefit, are balanced for a prioritization strategy. However, the inherent problems with CEA and QUALY, i.e., the aggregation problem, the priority problem, the problems of “democracy” and indirect benefit will have to be considered17 and lastly the fair vs. the best outcome problem, a tension between a utilitarian approach vs. an egalitarian concern for fairness. Added to these are the problematic interpretations of QUALY or disability-adjusted life years (DALY) as the indicators for benefit in the CEA calculations.18 CEA is used most often on an institutional level, many of its decision hidden in hospital reimbursement policies or clinical guidelines. Due to the difficult process of gaining reliable data, most healthcare budgets are due to an interplay of politics and bureaucratic pressure or the ability to pay, all highly ineffective as demonstrated by Doshmangir et al. for the Iranian system (Doshmangir et al. 2019; Doshmangir et al. 2016). |
| Declaration of Geneva | Details and new versions of the “Declaration of Geneva” are to be found https://www.wma.net/what-we-do/medical-ethics/declaration-of-geneva, accessed on 24 August 2021, (World Medical Association 1948) |
| Declaration of Helsinki | The “Declaration of Helsinki” states the ethical principles for medical research involving human subjects. For details see https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/, accessed on 8 August 2021, (World Medical Association 2013) |
| Deontology | In moral philosophy, deontological ethics is the normative ethical theory that the morality of an action should be based on whether that action itself is right or wrong under a series of rules, i.e., based on an inherent rightness of the established rules, rather than based on the consequences of this action. It is sometimes described as duty-, obligation- or rule-based ethics (Alexander and Moore 2020). Deontological ethics argues with formal criteria such as equality or impartiality (Britannica 2021). |
| Egalitarian theories | Egalitarian theories of justice hold to each person an equal measure of liberty and equal access to goods in life that every rational person values; |
| European Rare Diseases (E-RARE) and European Reference Networks (ERNs) | E-RARE, the EU’s strategic objective for rare diseases is to improve patient access to diagnosis, information and care. It assists in pooling scarce resources spread across the EU, enabling patients and professionals to share expertise and information. https://ec.europa.eu/health/non_communicable_diseases/rare_diseases_de, accessed on 27 June 2021. ERNs, Health systems in the European Union aim to provide high-quality, cost-effective care. This is particularly difficult, however, in cases of rare or low-prevalence complex diseases which affect the daily lives of around 30 million EU citizens. European Reference Networks (ERNs) are virtual networks involving healthcare providers across Europe. They aim to facilitate discussion on complex or rare diseases and conditions that require highly specialized treatment, and concentrated knowledge and resources. https://ec.europa.eu/health/ern_de, accessed on 27 June 2021. |
| fatwa | The authoritative ruling of a religious scholar on questions (masāʾel) of Islamic jurisprudence that are either dubious or obscure in nature (šobohāt) or which have newly arisen without known precedent (mostaḥdaṯāt). The query eliciting a fatwā may, however, relate to an existing ordinance (ḥokm) of Islamic law, unknown to the questioner, or to its application to a specific case or occurrence; the fatwā then functions simply as a clarification of the relevant ordinance (tabyīn-e ḥokm). Although the fatwā is typically concerned with legal matters, doctrinal considerations are necessarily involved whenever a fatwā results in takfīr, the condemnation of individuals or groups as unbelievers. The ruling provided in a fatwā is not intrinsically obligatory, for it is essentially an expression of learned opinion. In Shī’ī Islam, however, the authority to deliver a fatwā is generally restricted to the mojtahed, the jurist equipped to deduce the specific ordinances of the law (forūʿ) from its sources (oṣūl), and obedience to the mojtahed of their choice—designated as marjaʿ-e taqlīd—is incumbent on all who lack the same learned qualifications; to follow the ruling given in the fatwā of a mojtahed is therefore obligatory for those who solicit it. |
| Foundationalism | “Foundationalism is a view about the structure of justification or knowledge. The foundationalist’s thesis in short is that all knowledge or justified belief rest ultimately on a foundation of non-inferential knowledge or justified belief” (Hasan and Fumerton 2018). |
| Gene co-culture of human behavior | Tomasello refers to genetic adaptation based on the interaction of changes in both, the natural environment and cultural settings. According to Toby and Cosmides evolutionary psychology (EP) primarily explores the design of the universal, evolved psychological and neural architecture that we all share by virtue of being human. EP is usually less interested in human characteristics that vary due to genetic differences because, as these differences are unlikely to be evolved adaptations central to human nature. Of the three kinds of characteristics that are found in the design of organisms—adaptations, by-products, and noise—traits caused by genetic variants are predominantly evolutionary noise, with little adaptive significance, while complex adaptations are likely to be universal in the species” (Tooby and Cosmides 2005, p. 39; Downes 2021). “Evolution acts through genes, but it acts on the relationship between the genes and the environment. The environment is as much part of the process of evolutionary inheritance as are the “genes” and equally as “biological” and “evolved” (Tooby and Cosmides 1990, p. 20). |
| Genetic counselling | The process of genetic counselling is complex and includes (i) the interpretation of family and medical histories to assess the risk of disease occurrence/recurrence; (ii) education about inheritance, testing, management, prevention, resources and research and (iii) counselling to promote informed choices and adaptation to the risk or condition (Bittles 2012, chp. 13, p. 204). |
| Good Clinical Practice | The guidelines for Good Clinical Practice (GCP) were initiated in the USA in 1977, homogenized with Japan and the European Union (EU) in 1996 and legalized into the Medicines Act (Arzneimittelgesetz) in Germany in 2004. There all practical details for clinical studies are regimented. For details see https://ichgcp.net/de#, accessed on 15 April 2021. (Bundesministerium für Justiz und Verbraucherschutz 2021; ICH 2021; Irrgang 2015; World Medical Association 2013) |
| Healthcare resources | Seen as for instance treatment, interventions, medication, rehabilitation, health care services and service providers, etc. They are scare due to the allocation of funds of the government budget are or intrinsically scare as for instance transplantable organs. |
| Homozygous/heterozygous | Zygosity is the degree to which both copies of a chromosome or gene have the same genetic sequence, i.e., the same form of gene. With both alleles of the gene the same, the organism is homozygous at this locus. If they are different the organism is heterozygous (Cambridge Dictionary). https://dictionary.cambridge.org/dictionary/english/homozygous, accessed on 2. April 2021. |
| Human Radiation Experiments | Experiments performed in the USA exposing humans to radioactive material without informed consent. The information on these experiments was published after President Bill Clinton formed the Advisory Committee on Human Radiation Experiments (ACHRE, 1994) https://ehss.energy.gov/ohre/roadmap/achre/summary.html, accessed on 2 April 2021. |
| Ijtihād | independent legal thinking and hermeneutics |
| Intuitionalism | The classic intuitionists maintained that basic moral propositions are self-evident—that is, evident in and of themselves—and so can be known without the need of any argument. Intuition is immediate apprehension by the understanding. It is the way that we apprehend self-evident truths, general and abstract ideas, “and anything else we may discover, without making any use of any process of reasoning (Stratton-Lake 2020). |
| Istiṣlāh | istiṣlāh means seeking the common good, considerations of public good; a source of legislation that requires balancing all aspects of benefit and harm that are included in the three goals of the Sharī’a. |
| Joint intentionality | The “skill and motivation to construct with others an interdependent, plural-agent ‘we’” (Tomasello 2016, chp. 1, p. 4). This interdependence goes beyond a sense of sympathy towards kins and friends, an oxytocin-based social emotion of sympathy. Thus, joint, i.e., shared intentionality gives rise to the change from strategic cooperation to genuine morality. “This new form of interdependence meant that early human now extended their sense of sympathy beyond kin and friend to collaborative partners” (Tomasello 2016, chp. 1, p. 4). Joint intentionality presupposes cognitive, psychological skills of “common-ground understanding of the ideal way that each role has to be played for joint success. These common ground ideals may be thought of as the original socially shared normative standards” (Tomasello 2016, chp. 1, p. 4). |
| Libertarian theories | Libertarian theories of justice pertain to each person a maximum of liberty and property resulting from the exercise of liberty rights and participation in fair free market exchange (Beauchamps and Childress 2019). |
| Morality of Sympathy | Morality of sympathy describes a kin- and friendship-based prosociality found in human’s last common ancestors, based on oxytocin induced social emotion of sympathy (Tomasello 2016, p. 31). The psychological characteristics of a morality of sympathy can be described as based on cognition (individual intentionality for flexible and informed decisions, as well as understanding and predicting the intentional states of others for purposes of competition), social motivation (i) the capacity to form social relations of dominance and friendship; (ii) the capacity to have and express basic emotions and recognize these emotions in others; (iii) the capacity to communicate intentionally and (iv) the sympathy based motivation to help others instrumentally, especially kin and friends) and self-regulation (the ability to control impulses for immediate self-gratification and the ability to collaborate with others to produce new resources) (Tomasello 2016, p. 35). Most importantly this morality of sympathy still lacks any socially normative sense of fairness or justice concerning how they “ought” to treat others or how others “ought” to treat them (Tomasello 2016, p. 36). |
| Mu’tazilah theology | Originally the term meant political or religious neutralists. Later (10th century) Mu’tazilah refers to a school of speculative theology using the methods of Hellenistic philosophy to develop three distinct dogmatic points: First, the absolute uniqueness of God, concluding that the Qur’ān could not be the word of God, as God had no separable parts. The Qur’ān was therefore created and not coeternal with God. Second, due to God’s justice God desires for only the best for man, but through free will man choses between good and evil and becomes responsible for his actions. Third, due to God’s justice God must reward the good and punish the evil. These premises are accepted by Shī’ī Muslim (Britannica 2020) Mu’tazilis’ rationalist theology; Muʿtazilah a major theological school of Islam was renowned for holding reason (ʿaql) above scripture and other sources of religious knowledge and for its development of the method of dialectical theology (ʿilm al-kalām) (El Omari 2016). Mu’tazilites are the followers of the rationalist-naturalist theology that privileged human reason the ability to know moral truth (Sachedina 2009, chp. 2, p. 32). |
| Nuremberg Code | The ten articles of the Nuremberg Code, as defined by “Trials of War Criminals before the Nuremberg Military Tribunals under Control Council Law No. 10”, Vol. 2, pp. 181-182. Washington, D.C.: U.S. Government Printing Office, 1949 are indicated via the NIH website https://history.nih.gov/display/history/Nuremberg+Code, accessed on 24 August 2021 (National Institute of Health 2021). |
| Ontogeny | Ontogeny describes the development of an organism during the lifetime of an individual organism, in contrast to the evolvement of species (phylogeny). There, a causal explanation of a phenomenon relates to the interplay of genes and mechanical forces, i.e., genetics and physics (Love 2022). |
| Oxytocin | A peptide-hormone secreted from the pituitary gland, it effects, via g-protein coupled receptors, milk ejection during lactation, uterine contractions during labor and may play a role in sexual arousal. Psychologically oxytocin positively affects in-group bonding, enhancing prosocial behavior by facilitating trust and attachment between in -group members, increasing empathy during perspective taking, and conditioned reward learning. For details see reference (Jurek and Neumann 2018). |
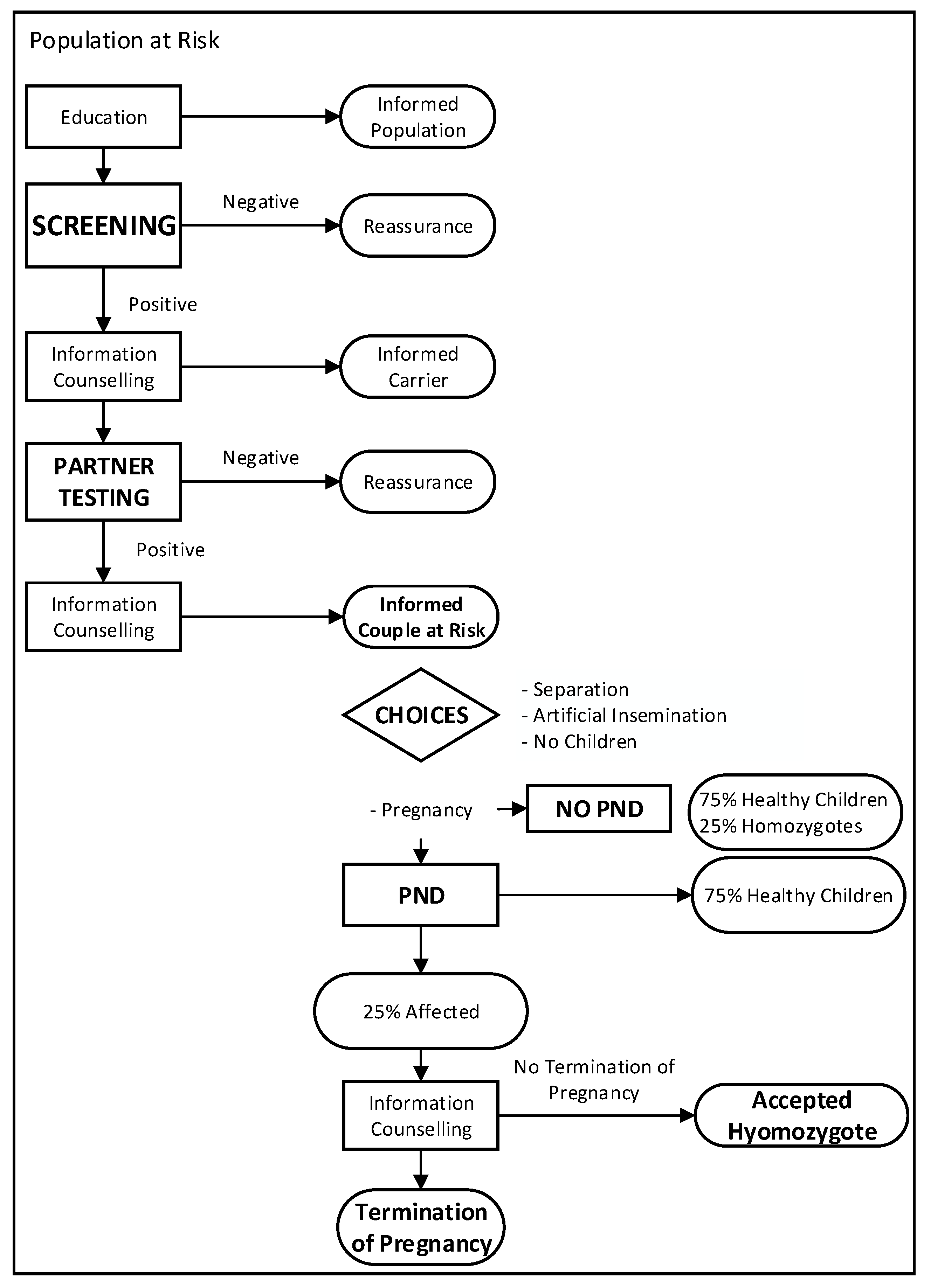
| Primary care genetic counselling network | A primary care genetic counselling network was set up as suggested by the WHO (Samavat and Modell 2004; WHO 1993, 1998) The counselling team comprises a physician and a professional (BSc.) in health studies, trained by specialists of the National Genetics Committee. Information of the public as well as target groups is organized via a national multidisciplinary educational committee, linked to corresponding provincial committees, and further down the line to primary care centers. In addition, high school students and young men in the military are educated about thalassemia. The judiciary is linked to the program through annual meetings for marriage registrars (many of whom are clergy). Laboratory services are provided by an accredited national professional laboratory network, supervised by a national reference laboratory and directorate for laboratory affairs. Laboratory staff follows national screening protocols based on international guidelines, participate in quality control, and attend regular educational courses. Data (number of couples counselled, their choice, referrals to DNA laboratories, follow-up on carrier couples and children born with thalassemia) from genetic counselling and primary care health houses are reported to the genetic offices, which report back and serve as a surveillance system. The screening process using the respective markers for thalassemia follows the flow chart provided by the WHO (see Figure 1). |
| QUALY | Quality adjusted life years are calculated as the QoL ranging from 0 (death) to 1 (perfect) multiplied with the respective life expectancy. For instance, (i) if the QoL is 0.3 and the life expectancy 5 years then the QUALY is 1.5; (ii) the British National Institute for Health and Care Excellence sees any medications with costs more than 300,000 pounds per QUALY as not cost-effective (Meissner 2010). |
| Rare Disease Policy of the EU | The EU created an operational framework in the field of rare diseases, opting for cross-border healthcare and coordination of classifications, codifications, European Reference Networks, orphan medicinal products and expert group on rare diseases, putting rare diseases in a privileged position in the health care agenda (Moliner and Waligora 2017). https://health.ec.europa.eu/non-communicable-diseases/steering-group/rare-diseases_de accessed on 27 June 2021. European Reference Networks: https://health.ec.europa.eu/european-reference-networks/overview_en, accessed on 27 June 2021. |
| Reflective equilibrium | Reflective equilibrium is the end-point of a deliberative process in which we reflect on and revise our beliefs about an area of inquiry, moral or non-moral. The inquiry might be as specific as the moral question, “What is the right thing to do in this case?” or the logical question, “Is this the correct inference to make?” Alternatively, the inquiry might be much more general, asking which theory or account of justice or right action we should accept, or which principles of inductive reasoning we should use. We can also refer to the process or method itself as the “method of reflective equilibrium” (Daniels 2020). Reflective equilibrium describes a position of reciprocal relationship between moral principles and casuistry, i.e., case-based reasoning, a process by which our considered responses to actual cases influence our moral principles, and those improved-upon principles then provide enhanced guidance for our responses to further cases. Reflective the source of the source of coherentism, with the appeal to the common morality meant to provide a foundation. Beauchamp and Childress accord foundational status to the common morality, and it is the common morality that underwrites their four principles (autonomy, non-maleficence, beneficence and justice) (Flynn 2021). |
| Relational autonomy | Relational autonomy is seen as a procedural conception of autonomous and self-reflective decisions of competent individuals, emphasizing the influence of the social environment on self-reflectiveness. Thus, instead of individual autonomy Zimmermann et al. take into account the social influence of i) relatives, as especially predictive genetic testing impinges on the interest of relatives, their right “to know” or “not to now” as this may lead to competing interests; and ii) healthcare professionals despite nondirective counselling (Zimmermann et al. 2021). |
| Second-personal agency | Second-personal agency refers to the interdependent collaborative activities structured by joint intentionality that fostered in participants a new kind of cooperative rationality … particular collaborative activities had role ideals—socially normative standards—that applied to either of them indifferently, which implied a kind of self-other equivalence. Based on the recognition of self-other equivalence, there arose a mutual respect between partners, and a sense of mutual deservingness of partners, thus creating second-personal agents (Tomasello 2016). |
| Second-personal morality | Second-personal morality can be described as the sense of mutual deservingness emerging from joint activity. Thus, second-person morality is a “dyadic morality of face to face interactions between agents collaborating, and feeling responsible to one another, as a jointly committed ‘we’” (Insern-Mas and Gomila 2022, p. 202). |
| Teleological ethics | Teleological ethics refer to normative ethical theory based on the goodness of the consequences of an action. It is based on the good, valuable and desirable. Teleological ethics argues with material or substantive criteria such as happiness or pleasure (Britannica 2021). |
| Tuskegee Study | The United States Public Health Service (USPHS) initiated a study “The Tuskegee Study of Untreated Syphilis in Negro Males” (USPHS Syphilis Study at Tuskegee) in 1933. There participants had been neither given informed consent to the study and despite the availability of penicillin since 1943, were not offered treatment. When the study details became public in 1972 the study was closed and free medical care for survivors of the study was initiated in 1973, which was later extended to the widows and children of the participants. In 1997 President Clinton issued a formal Presidential Apology (The United States Public Health Service 2021). https://www.cdc.gov/tuskegee/timeline.htm, accessed on 11 July 2021. |
| Twelfer Shi’ah | The Twelvers believe that, at the death of the Prophet Muhammad in 632 CE, the spiritual-political leadership (the imamate) of the Muslim community was ordained to pass down to ʿAlī, the Prophet’s cousin and son-in-law, and then to ʿAlī’s son Ḥusayn and thence to other Imams down to the 12th, Muḥammad ibn al-Ḥasan, who is understood to have been born circa 870 but to have gone into occultation (Arabic ghaybah; Persian ghaybat)—a state of concealment by God—soon after his father’s death circa 874. The “Hidden Imam,” as he is sometimes called, is considered to be still alive and will return when God determines it to be appropriate and safe (Newman 2019). |
| Ummah | Ummah literally means community. It is a synonym for ummat al-Islām, the Islamic community, i.e., the collective community of Islamic people. In the Qur’an the ummah typically refers to a single group that shares common religious beliefs, specifically those that are the objects of a divine plan of salvation. |
| Universal Declaration on Bioethics and Human Rights | For details see https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights (accessed on 3 May 2021). (UNESCO 2005) |
| Uṣūl al-fiqh | Islamic legal theory |
| Utilitarianism | A utilitarian approach to justice, i.e., to each person according to rules and actions that maximize social utility (Beauchamps and Childress 2019) |
| 1 | Within the framework of this paper the ‘West’ comprises the cultural sphere of influence of Europe and populations originating from Europe as the Americas and Australasia. Specifically, ‘Western’ thinking is defined by a postcolonial view where the ‘West’ (the ‘Occident’) and the ‘East’ (the ‘Orient’) are seen as opposing and mutually dependent (Said 2003). Thus, any comparison between ‘Western’ bioethical thinking and the bioethics of Shī’ī Islam will have to take into account this interdependence and the interpretation of the claim of universality of ‘Western’ bioethics as possibly Eurocentric. |
| 2 | Medical bioethics covers clinical bioethics, scientific investigations into humans and healthcare ethics. Due to our specific focus on medical bioethics, we abstain from using the additional term ‘medical’ throughout. |
| 3 | For in-depth discussion on the universality of human rights and the related religious discourse see (Auga 2020). |
| 4 | A glossary is provided as a supplementary file, covering special medical and Islamic expressions. |
| 5 | Here, different groups may diverge, creating multiple, particular moralities (PM), for instance a religious morality. For example, if prayers before all public meetings are required, this rule cannot include those in society who do not share this belief/practice. This limitation is a disadvantage inherent in PM operating in pluralistic societies. On the other hand, the advantages of a PM, retaining universal morality, is the possible richness and specificity that are lacking in universal morality. |
| 6 | Gert holds that the concept of irrationality makes it easier to grasp rationality (Gert 2006). |
| 7 | Examples for rational beliefs may be: all people are mortal, people can kill other people, cause pain, disable another; people generally do not want to have pain inflicted on them or to be disabled; and persons can deprive others of their freedom, but people generally do not want to be so deprived (Gert 2006, ibid., chp. 2, p. 88ff). |
| 8 | There bioethical rulings by Shīʿī Ayatollah Ali Sistani (Iraq) such as mandatory cardiovascular resuscitation for Muslim, but not for Non-Muslim, would not be possible due to the prohibition of religion-based discrimination (Mavani 2014). |
| 9 | For instance, religious guidance on bioethical issues may specify divine rewards or punishments to guarantee obedience (Moosapour et al. 2018). |
| 10 | ‘Independent’ reason is understood as a reasoning that is based on the prior notion that the revelation is true and as such is the major source of knowledge of the duties prescribed by the Sharī’a. |
| 11 | The concept of autosomal recessive disease is difficult to understand, for instance a 25%-risk misunderstood as the birth of one child with illness followed by three healthy children. Many Islamic societies belief that more genetic information is passed on by the father than the mother, thus the disease would only to be expected through cousin-marriage on the paternal side of the family. Being carrier of a disease and being healthy is often difficult to accept, especially from the fathers’ side of the family, preferentially redirecting the responsibility of an inherited disease exclusively on the mother. These difficulties are exacerbated by insufficient genetic knowledge of healthcare providers (Bittles 2012). |
| 12 | For instance misinterpretations of the carrier status as the presence of disease leading to discrimination in insurance/employment or relating responsibility for the disease only to the female carrier (Bittles 2012, ibid. 13, pp. 193–94). |
| 13 | Indicators of healthcare quality (life expectancy, maternal mortality rate, access to healthcare, population/physician ratio, etc.) increased substantially. By 2019 92% of the population were covered by at least one health insurance system and individual out-of-pocket payments decreased from 54% to 41%, yet still far from the goal of 30%. (Doshmangir et al. 2019). |
| 14 | Auditing peer-revied publications demonstrated for 1990: 37 medical papers, 60% with an impact factor (IF) < 1; for 2007: 3176, 70% with an IF > 1 (Azizi 2009). |
| 15 | The paper is part of medical ethics PhD thesis, with the last author Head of the Department of Medical Ethics at the Shahid Beheshti University of Medical Sciences in Teheran. |
| 16 | Abdulaziz Sachedina is a Muslim American citizen born in Tanzania, working as Professor of Islamic Studies at George Mason University, Fairfax, Virginia, and as such does not represent the Iranian religious elite. |
| 17 | An aggregation problem occurs when a low-cost and low-benefit procedure widely used will rank higher than a high-cost and high-benefit but rarely used procedure; the priority problem that impacts the equality and impartiality of healthcare, i.e., should the one with higher needs of these resources have priority? And if this is the case, how do we determine those “worst off”, the deaf or the blind? the democracy problem asks whose values will be decisive, the community who pays for the resources or some bureaucratic elites; the problem of indirect benefits, i.e., health is not an individual problem, a healthy person benefits the society by working, paying higher taxes, etc. Problems arise with the quantification of these benefits and how are these societal benefits merged with healthcare organization. |
| 18 | For instance, (i) the idea that QoL indicates an objective degree of well-being independent of the underlying disease. Yet, adaptation and adjusting processes of the disabled person may result in the “disability paradox” with a significantly less reduced QoL than estimated by a healthy person. It is a well-known phenomenon that life is the more valuable the less is left. The example indicates that QoL metric denies the fact that there is no persistent value of any resource across a population and time (Bickenbach 2021); (ii) the overall burden of a disease (effects on employment, social functioning, stigmatization, etc.) afflicts QoL-metric. As the burden of living with a disability is caused as much by the social environment as by the disease, we would have to include the problems of a failed policy to combat stigma and lack of accommodation, as healthcare by itself would not increase the overall QoL situation ibid. |
References
- Aderyani, Mohsen Rezaei, and Mehrzad Kiani. 2015. A Comparative Study of the Foundations of Medical Ethics in Secular and Islamic Thought. Journal for the Study of Religions and Ideologies 14: 27–46. [Google Scholar]
- Adib-Hajbaghery, M., M. Ahmadi, and S. Poormansouri. 2015. Health Related Quality of Life, Depression, Anxiety and Stress in Patients with Beta-Thalassemia Major. Iranian Journal of Pediatric Hematology and Oncology 5: 193. [Google Scholar] [PubMed]
- Akrami, Forouzan, Abbas Karimi, Mahmoud Abbasi, and Akbar Shahrivari. 2018. Adapting the prinicples of biomedical ethics to Islamic principles and values in the context of public health policy. Journal for the Study of Religions and Ideologies 17: 46–59. [Google Scholar]
- Alexander, L. 1949. Medical Science under Dictatorship. New England Journal of Medicine 241: 39–47. [Google Scholar] [CrossRef]
- Alexander, L., and M. Moore. 2020. Deontological Ethics. Available online: https://plato.stanford.edu/archives/win2020/entries/ethics-deontological/ (accessed on 7 June 2021).
- Alexandra, Andrew, and Seumas Miller. 2009. Ethical theory, “common morality”, and professional obligations. Theoretical Medicine and Bioethics 30: 69–80. [Google Scholar] [CrossRef]
- Ansari-Moghaddam, Alireza, Hossein Ali Adineh, Iraj Zareban, Mehdi Mohammadi, and Mahtab Maghsoodlu. 2018. The survival rate of patients with beta-thalassemia major and intermedia and its trends in recent years in Iran. Epidemiology and Health 40: 9. [Google Scholar] [CrossRef]
- Aramesh, Kiarash. 2015. A Brief History of Biomedical Research Ethics in Iran: Conflict of Paradigms. Developing World Bioethics 15: 107–12. [Google Scholar] [CrossRef]
- Arras, John D. 2009. The hedgehog and the Borg: Common morality in bioethics. Theoretical Medicine and Bioethics 30: 11–30. [Google Scholar] [CrossRef]
- Asad, Talal. 1993. Genealogies of Religion. Discipline and Reasons of Power in Christianity and Islam. Baltimore and London: The John Hopkins University Press. [Google Scholar]
- Auga, Ulrike E. 2020. Human Rights, Gender and Religion: Controversies in Political, Social, Cultural and Sexuality Discourse. In An Epistemology of Religion and Gender: Biopolitics–Performativity–Agency. London and New York: Routledge. [Google Scholar]
- Azizi, Farhad. 2009. Medical Education in the Islamic Republic of Iran: Three Decades of Success. Iranian Journal of Public Health 38: 19–26. [Google Scholar]
- Beauchamps, Tom L. 2003. Ä defense of the common morality. Kennedy Institute of Ethics Journal 13: 259–74. [Google Scholar] [CrossRef]
- Beauchamps, Tom L. 2016. Principles of Biomedical Ethics. In The Principles of Biomedical Ethics as Universal Principles; Islamic Perspectives on the Principles of Biomedical Ethics. Edited by Mohammed Ghaly. London: World Scientific Publisher, pp. 89–120. [Google Scholar]
- Beauchamp, Tom L., and James F. Childress. 2009. Principles of Biomedical Ethics, 6th ed. New York: Oxford University Press. [Google Scholar]
- Beauchamps, Tom L., and James F. Childress. 2019. Principles of Biomedical Ethics, 8th ed. New York: Oxford University Press. [Google Scholar]
- Bickenbach, Jerome. 2021. Disability and Health Care Rationing. Available online: https://plato.stanford.edu/archives/spr2021/entries/disability-care-rationing (accessed on 8 August 2021).
- Bittles, Alan H. 2012. Consanguinity in Context. Cambridge: Cambridge University Press. [Google Scholar]
- Borgna-Picatti, Caterina, Simone Rugolotto, Piero De Stefano, Antonio Piga, Felicia Di Gregorio, Maria Rita Gamberini, Vincenzo Sabato, Caterina Melevendi, Maria Domenica Cappellini, and Giuseppe Verlato. 2006. Survival and Disease Complications in Thalassaemia Major. Annals New York Academy of Sciences 850: 227–31. [Google Scholar] [CrossRef] [PubMed]
- Borry, Pascal, Marieke Teeuw, and Martina C. Cornel. 2013. Genetic Testing and Counseling in the Case of Consanguinity: Facts, Ethical and Legal Consequences. In Currents of Encounter. Studies on the Contact between Christianity and other Religions, Beliefs, and Cultures. Looking Beneath the Surface. Medical Ethics from Islamic and Western Perspectives. Edited by Hendrik M. Vroom, Petra Verdonk, Marzouk Aulad Abdellah and Martina C. Cornel. Amsterdam: Rodopi, vol. 8. [Google Scholar]
- Britannica. 2020. Muʿtazilah. Available online: https://www.britannica.com/topic/Mutazilah (accessed on 17 July 2021).
- Britannica. 2021. Normative Ethics. Available online: https://www.britannica.com/topic/normative-ethics (accessed on 29 April 2021).
- Bundesministerium für Justiz und Verbraucherschutz. 2021. Gesetz über den Verkehr mit Arzneimitteln. Available online: https://www.gesetze-im-internet.de/amg_1976/ (accessed on 19 April 2021).
- Cao, Antonio, and Yuet Wai Kan. 2013. The Prevention of Thalassemia. Cold Spring Harbor Perspectives in Medicine 3: 1–15. [Google Scholar] [CrossRef] [PubMed]
- Childress, James F. 1990. The Place of Autonomy in Bioethics. The Hastings Center Report 20: 12–17. [Google Scholar] [CrossRef] [PubMed]
- Daniels, Norman. 2020. Reflective Equilibrium. Available online: https://plato.stanford.edu/archives/sum2020/entries/reflective-equilibrium/ (accessed on 30 April 2021).
- Doshmangir, Leila, Arash Rashidian, Mehdi Jafari, Hamid Ravaghi, and Amirhossein Takian. 2016. Fail to prepare and you can prepare to fail: The experience of financing path changes in teaching hospitals in Iran. BMC Health Services Research 16: 138. [Google Scholar] [CrossRef]
- Doshmangir, Leila, Mohammad Bazyar, Reza Majdzadeh, and Amirhossein Takian. 2019. So Near, So Far: Four Decades of Health Policy Reforms in Iran, Achievements and Challenges. Archives of Iranian Medicine 22: 592–605. Available online: http://www.aimjournal.ir/Article/aim-7991 (accessed on 24 August 2021). [PubMed]
- Downes, Stephen M. 2021. Evolutionary Psychology. In The Stanford Emcyclopedia of Philosophy. Edited by Edward Nouri Zalta. Available online: https://plato.stanford.edu/archives/spr2021/entries/evolutionary-psychology/ (accessed on 24 August 2021).
- El Omari, R. 2016. The Mu’tazilite Movement(I): The origin of the Mu’tazila. Oxford: Oxford University Press. [Google Scholar]
- Esmaeilzadeh, Firooz, Azita Azarkeivan, Sara Emamgholipour, Ali Akbari Sari, Mehdi Yaseri, Batoul Ahmadi, and Mohtasham Ghaffari. 2016. Economic Burden of Thalassemia Major in Iran. Journal of Research in Health Science 16: 111–15. [Google Scholar]
- Esmaeilzadeh, Firooz, Batoul Ahmadi, Sajad Vahedi, Saeed Barzegari, and Abdolhalim Rajabi. 2021. Major Thalassemia, Screening or Treatment: An Economic Evaluation Study in Iran. International Journal of Health Policy and Management 11: 1112–19. [Google Scholar] [CrossRef]
- Flynn, Jennifer. 2021. Theory and Bioethics. Available online: https://plato.stanford.edu/archives/spr2021/entries/theory-bioethics (accessed on 19 April 2021).
- Gert, Bernard. 2006. Common Morality: Deciding What to Do. Available online: https://academic.oup.com/book/8298 (accessed on 1 June 2021).
- Gert, Bernard, Charles M. Culver, and K. Danner Clouser. 2006. Bioethics: A Systematic Approach. New York: Oxford University Press. [Google Scholar]
- Ghanei, M., P. Adibi, M. Movahedi, M. A. Kham, R. L. Ghasemi, T. Azarm, B. Zolfaghari, H. R. Jamshidi, and R. Sadri. 1997. Pre-marriage prevention of thalassaemia: Report of a 100,000 case experience in Isfahan. Public Health Genomics 111: 153–56. [Google Scholar] [CrossRef]
- Gordon, John-Stewart. 2011. Global Ethics and Principlism. Kennedy Institute of Ethics Journal 21: 251–76. [Google Scholar] [CrossRef] [PubMed]
- Hadipour Dehshal, Mahmoud, Mehdi Tabrizi Namini, Razieh Hantoushzadeh, and Sakineh Yousefi Darestani. 2019. β-Thalassemia in Iran: Things Everyone Needs to Know About This Disease. Hemoglobin 43: 166–73. [Google Scholar] [CrossRef]
- Haider, Najam. 2014. Shi’i Islam: An Introduction. Cambridge: Cambridge University Press. [Google Scholar]
- Hasan, Ali, and Richard Fumerton. 2018. Foundationalist Theories of Epistemic Justification. In The Stanford Encyclopedia of Philosophy. Edited by Edward Nouri Zalta. Stanford: Stanford University, Metaphysics Research Lab. Available online: https://plato.stanford.edu/entries/justep-foundational/ (accessed on 21 June 2021).
- Hashemieh, M., H. Timori Naghadeh, M. Tabrizi Namini, H. Neamatzadeh, and M. Hadipour Dehshal. 2015. The Iran Thalassemia Prevention Program: Success or Failure? Iranian Journal of Pediatric Hematology Oncology 5: 161–66. [Google Scholar] [PubMed]
- Hedayat, Kamyar M., Peiman Shooshtarizadeh, and Mohsin Raza. 2006. Therapeutic abortion in Islam: Contemporary views of Muslim Shiite scholars and effect of recent Iranian legislation. Journal of Medical Ethics 32: 652–57. [Google Scholar] [CrossRef] [PubMed]
- ICH (International Conference on Harmonisation of technical requirements for registration of pharmaceuticals for human use). 2021. ICH harmonised guideline integrated addendum to ICH E6(R1): Guideline for Good Clinical Practice ICH E6(R2) ICH Consensus Guideline. Available online: https://ichgcp.net/ (accessed on 19 April 2021).
- Isern-Mas, Carme, and Antoni Gomila. 2022. A second-personal approach to the Evolution of Morality. Biological Theory, 199–209. [Google Scholar] [CrossRef]
- Irrgang, Bernhard. 2015. Medizinethik für Mediziner. Stuttgart: Steiner Verlag. [Google Scholar]
- Jurek, Benjamin, and Inga D. Neumann. 2018. The Oxytocin Receptor: From Intracellular Signaling to Behavior. Physiological Reviews 98: 1805–908. [Google Scholar] [CrossRef]
- Larijani, Bagher, and Farzaneh Zahedi. 2008. Contemporary Medical Ethics: An Overview from Iran. Developing World Bioethics 8: 192–96. [Google Scholar] [CrossRef]
- Larijani, Bagher, Farzaneh Zahedi, and Hossein Malek Afzali. 2005. Medical ethics in the Islamic Republic of Iran. Eastern Mediterranean Health Journal 11: 1061–72. [Google Scholar]
- Love, Alan. 2022. Developmental Biology. In The Stanford Encyclopedia of Philosophy. Edited by Edward Nouri Zalta. Available online: https://plato.stanford.edu/archives/sum2022/entries/biology-developmental/ (accessed on 11 November 2022).
- Mavani, Hamid. 2014. Two shi’i jurisprudential methodologies to address medical and bioethical challenges: Traditional ijtihad and foundational ijtihad. Journal of Religious Ethics 42: 263–84. [Google Scholar] [CrossRef]
- Meissner, Marc. 2010. Was ist ein QUALY? Deutsches Ärzteblatt 107: A-546. Available online: https://www.aerzteblatt.de/archiv/70329/Was-ist-ein-Qaly (accessed on 17 August 2021).
- Miri, Maedehsadat, Mehdi Tabrizi Namini, Mahmoud Hadipour Dehshal, Forouzan Sadeghian Varnosfaderani, Alireza Ahmadvand, Sakineh Yousefi Darestani, and Mohsen Manshadi. 2013. Thalassemia in Iran in Last Twenty Years: The Carrier Rates and the Births Trend. Iranian Journal of Blood and Cancer 6: 11–18. [Google Scholar]
- Moliner, Antoni Montserrat, and Jaroslaw Waligora. 2017. The European Policy in the Field of Rare Disease. Advances in Experimental Medicine and Biology 1031: 561–87. [Google Scholar] [CrossRef]
- Moodi, Mitra, Mohammad-Reza Miri, and Gholam-Reza Sharifirad. 2013. The effect of instruction on knowledge and attitude of couples attending pre-marriage counseling classes. Journal of Education and Health Promotion 2: 1–5. [Google Scholar] [CrossRef] [PubMed]
- Moosapour, Hamideh, Jannat Mashayekhi, Farzaneh Zahedi, Akbar Soltani, and Bagher Larijani. 2018. General approaches to ethical reasoning in Islamic biomedical ethics discourse. Journal of Medical Ethics and History of Medicine 11: 11–21. [Google Scholar] [PubMed]
- Najmabadi, Hossein, Alireza Ghamari, Farhad Sahebjam, Roxana Kariminejad, Valeh Hadavi, Talayeh Khatibi, Ashraf Samavat, Elaheh Mehdipour, Bernadette Modell, and Mohammand Hassan Kariminejad. 2006. Fourteen-Year Experience of Prenatal Diagnosis of Thalassemia in Iran. Community Genet 9: 93–97. [Google Scholar] [CrossRef]
- National Institute of Health. 2021. The Nuremberg Code. Available online: https://history.nih.gov/display/history/Nuremberg+Code (accessed on 24 August 2021).
- Needs, T., L.-F. Gonzales-Mosquera, and D. T. Lynch. 2022. Beta Thalassemia; Treasure Island: StatPearls Publishing. Available online: https://www.ncbi.nlm.nih.gov/books/NBK531481/ (accessed on 16 May 2022).
- Neog, B. 2007. An Understanding of Common Morality. Utrecht: Utrecht University. [Google Scholar]
- Newman, Andrew J. 2019. Twelver Shi’ah. Available online: https://www.britannica.com/topic/Twelver-Shia (accessed on 9 April 2021).
- Nouri, Narges, Nayereh Nouri, Samane Tirgar, Elham Soleimani, Vida Yazdani, Farzaneh Zahedi, and Bagher Larijani. 2017. Consanguineous marriages in the genetic counseling centers of Isfahan and the ethical issues of clinical consultations. Journal of Medical Ethics and History of Medicine 10: 10. [Google Scholar]
- Palmer, Bernard. 2005. Common Morality: Deciding What to Do. The Review of Metaphysics 59: 178–80. [Google Scholar]
- Rahimi, Zohreh. 2013. Genetic Epidemiology, Hematological and Clinical Features of Hemoglobinopathies in Iran. BioMed Research International 2013: 803487. [Google Scholar] [CrossRef] [PubMed]
- Renn, Jürgen. 2020. The Evolution of Knowledge Rethinking Science for the Anthropocene. Princeton and Oxford: Princeton University Press. [Google Scholar]
- Sachedina, Abdulaziz. 2009. Islamic Biomedical Ethics Principles and Application. Available online: https://doi.org/10.1093/acprof:oso/9780195378504.001.0001 (accessed on 6 May 2021).
- Sachedina, Abdulaziz. 2015. Continuing the conversation about comparative ethics. Journal of Religious Ethics 43: 543–56. [Google Scholar] [CrossRef]
- Said, Edward W. 2003. Orientalism. Modern Classics London: Penguin Books. [Google Scholar]
- Samavat, Ashraf, and Bernadette Modell. 2004. Iranian national thalassaemia screening programme. BMJ 329: 1134–37. [Google Scholar] [CrossRef]
- Schwartz. 1929. Wilson&Reeder’s Mammals Species of the World (Online). Available online: http://www.departments.bucknell.edu/biology/resources/msw3/browse.asp?id=12100797 (accessed on 28 June 2021).
- Stratton-Lake, Peter. 2020. Intuitionism in Ethics. Available online: https://plato.stanford.edu/archives/sum2020/entries/intuitionism-ethics/ (accessed on 19 July 2021).
- Strauss, Bernard S. 2009. Genetic Counseling for Thalassemia in the Islamic Republic of Iran. Perspectives in Biology and Medicine 52: 364–76. [Google Scholar] [CrossRef]
- The United States Public Health Service. 2021. The U.S. Public Health Service Syphilis Study at Tuskegee. Available online: https://www.cdc.gov/tuskegee/timeline.htm (accessed on 11 July 2021).
- Tomasello, Michael. 2016. A Natural History of Human Morality. Cambridge: Harvard University Press. [Google Scholar]
- Tomasello, Michael. 2019. Becoming Human a Theory of Ontogeny. Cambridge: Harvard University Press. [Google Scholar]
- Tooby, John, and Leda Cosmides. 1990. On the Universality of Human Nature and the Uniqueness of the Individual: The Role of Genetics and Adaptation. Journal of Personality 58: 17–67. [Google Scholar] [CrossRef]
- Tooby, John, and Leda Cosmides. 2005. Conceptual Foundations of Evolutionary Psychology. In The Handbook of Evolutionary Psychology. Edited by D. Buss. Hoboken: John Wiley and Sons. [Google Scholar]
- UNESCO. 2005. Universal Declaration of Bioethics and Human Rights. Available online: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights (accessed on 3 May 2021).
- WHO. 1948. Constitution of the World Health Organisation. Available online: https://www.who.int/about/governance/constitution (accessed on 3 May 2021).
- WHO. 1993. Control of Hereditary Diseases: Report of a WHO Scientific Group. WHO Technical Report Series 865. Geneva: World Health Organization. Available online: https://apps.who.int/iris/handle/10665/41846 (accessed on 24 August 2021).
- WHO. 1998. Proposed International Guidelines on Ethical Issues in Medical Genetics and Genetic Services. Report of a WHO Meeting on Ethical Issues in Medical Genetics 1997. Geneva: World Health Organization. Available online: https://apps.who.int/iris/handle/10665/63910 (accessed on 3 May 2021).
- WHO. 2006. Medical genetic services in developing countries: The ethical, legal and social implications of genetic testing and screening. In Human Genetics, Chronic Diseases and Health Promotion. Geneva: World Health Organization. Available online: https://apps.who.int/iris/handle/10665/43288 (accessed on 3 May 2021).
- World Medical Association. 1948. Declaration of Geneva. Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-geneva/ (accessed on 24 August 2021).
- World Medical Association. 2013. World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 8 August 2021).
- Zimmermann, Bettina M., Insa Koné, David Shaw, and Bernice Elger. 2021. Autonomy and social influence in predictive genetic testing decision-making: A qualitative interview study. Bioethics 35: 199–206. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plöckinger, U.; Auga, U. The “Four Principles” of Western Medical Bioethics and the Bioethics of Shīʿī Islam in Iran—Is the Claim of Universality by Both Justified? Religions 2022, 13, 1118. https://doi.org/10.3390/rel13111118
Plöckinger U, Auga U. The “Four Principles” of Western Medical Bioethics and the Bioethics of Shīʿī Islam in Iran—Is the Claim of Universality by Both Justified? Religions. 2022; 13(11):1118. https://doi.org/10.3390/rel13111118
Chicago/Turabian StylePlöckinger, Ursula, and Ulrike Auga. 2022. "The “Four Principles” of Western Medical Bioethics and the Bioethics of Shīʿī Islam in Iran—Is the Claim of Universality by Both Justified?" Religions 13, no. 11: 1118. https://doi.org/10.3390/rel13111118
APA StylePlöckinger, U., & Auga, U. (2022). The “Four Principles” of Western Medical Bioethics and the Bioethics of Shīʿī Islam in Iran—Is the Claim of Universality by Both Justified? Religions, 13(11), 1118. https://doi.org/10.3390/rel13111118