Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
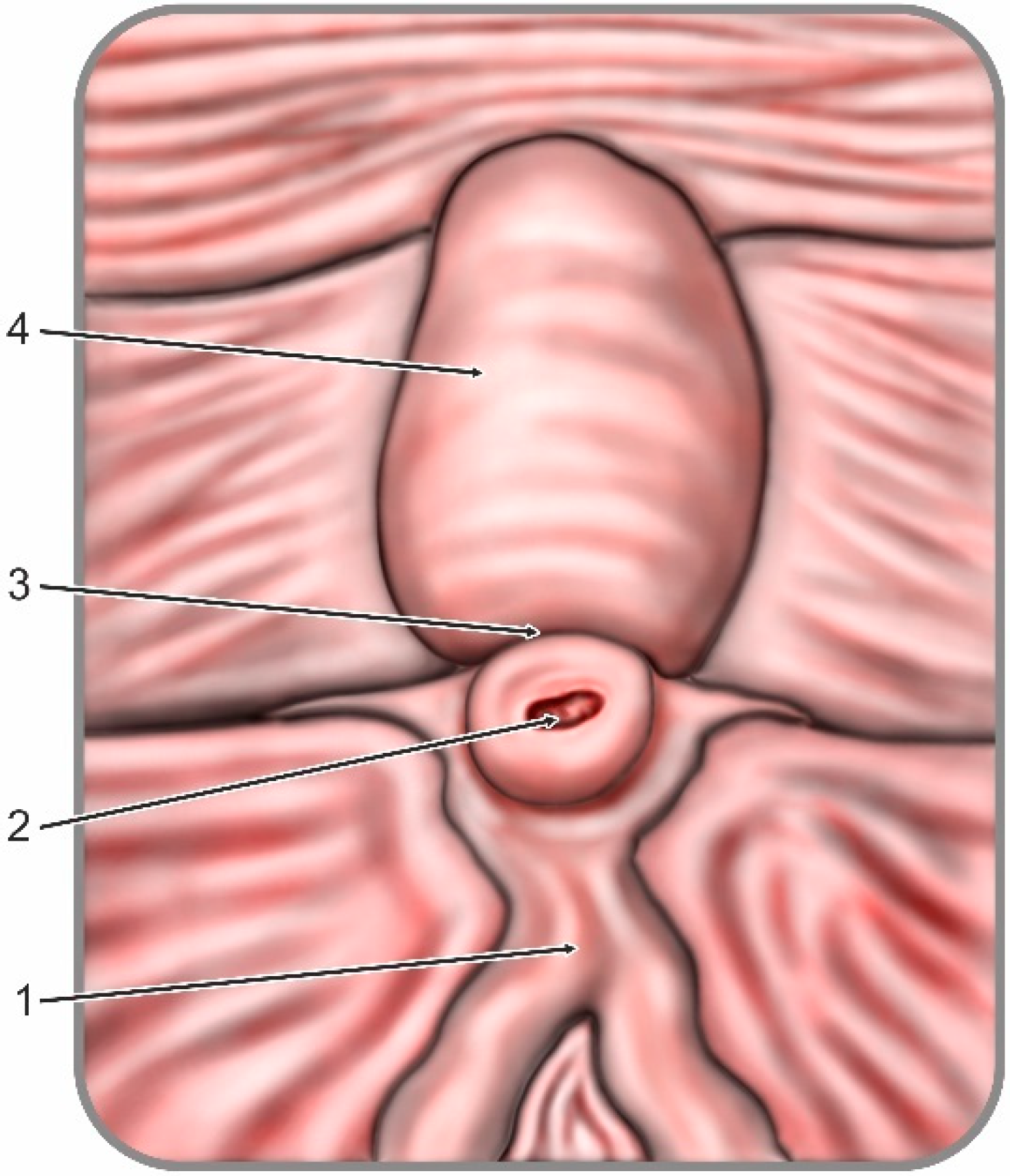
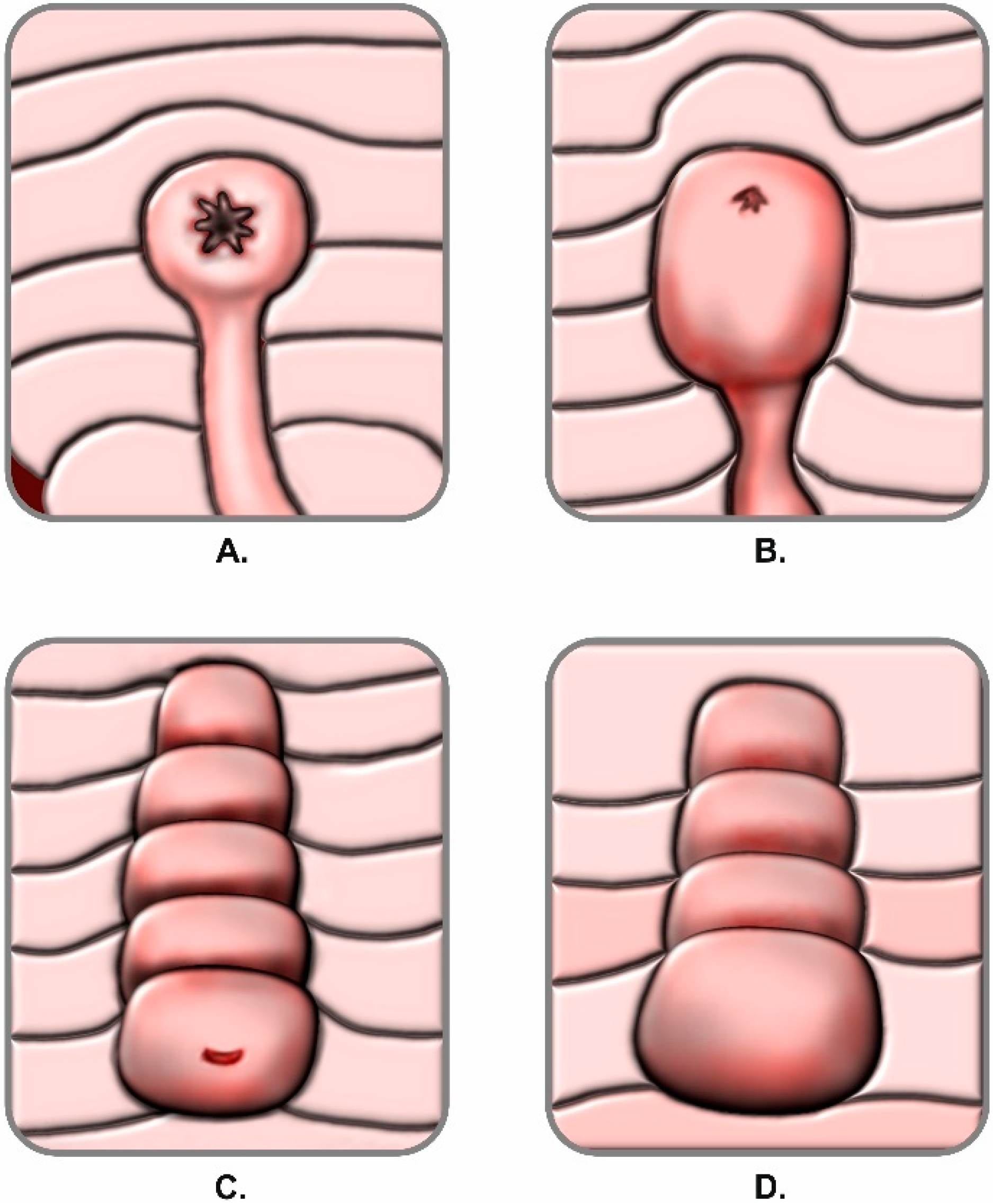
2.2. Classification of Papillary Morphology and Procedure Documentation
2.3. Prospective Evaluation
2.4. Statistical Analysis
3. Results
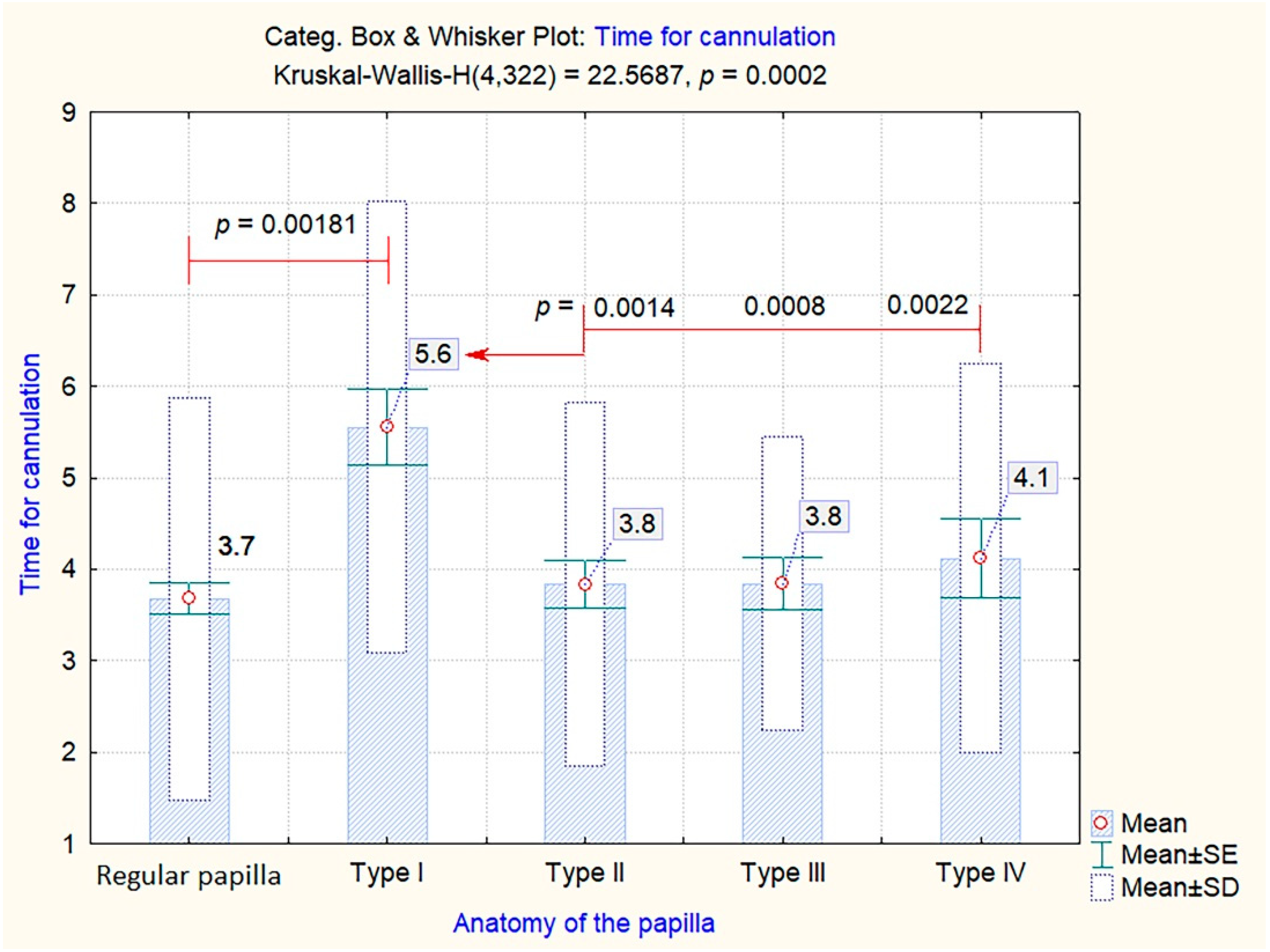
3.1. Impact of Papillary Morphology on Cannulation
3.2. Impact of Papillary Morphology on the Overall Post-ERCP Adverse Events Rate. Univariate Analysis
3.3. Multiple Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lecture, I. Hunterian Lectures. J. Anat. Physiol. 1885, 19, 292. [Google Scholar]
- Reddy, D.N.; Nabi, Z.; Lakhtakia, S. How to improve cannulation rates during endoscopic retrograde cholangiopancreatography. Gastroenterology 2017, 152, 1275–1279. [Google Scholar] [CrossRef]
- Hawes, R.H.; Devière, J. How I cannulate the bile duct. Endoscopy 2018, 41, 75–77. [Google Scholar]
- Testoni, P.A.; Mariani, A.; Aabakken, L.; Arvanitakis, M.; Bories, E.; Costamagna, G.; Devière, J.; Dinis-Ribeiro, M.; Dumonceau, J.M.; Giovannini, M.; et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy 2016, 48, 657–683. [Google Scholar] [CrossRef]
- Berry, R.; Han, J.Y.; Tabibian, J.H. Difficult biliary cannulation: Historical perspective, practical updates, and guide for the endoscopist. W J. Gastrointest. Endosc. 2019, 11, 5–20. [Google Scholar] [CrossRef]
- Freeman, M.L.; Nelson, D.B.; Sherman, S.; Haber, G.B.; Herman, M.E.; Dorsher, P.J.; Moore, J.P.; Fennerty, M.B.; Ryan, M.E.; Shaw, M.J.; et al. Complications of endoscopic biliary sphincterotomy. N. Eng. J. Med. 1996, 335, 909–919. [Google Scholar] [CrossRef]
- Cheng, C.L.; Sherman, S.; Watkins, J.L.; Barnett, J.; Freeman, M.; Geenen, J.; Ryan, M.; Parker, H.; Frakes, J.T.; Fogel, E.L.; et al. Risk factors for post-ERCP pancreatitis: A prospective multicenter study. Am. J. Gastroenterol. 2006, 101, 139–147. [Google Scholar] [CrossRef]
- Chandrasekhara, V.; Khashab, M.A.; Muthusamy, V.R.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Eloubeidi, M.A.; Fanelli, R.D.; Faulx, A.L.; Gurudu, S.R.; et al. Adverse events associated with ERCP. Gastrointest. Endosc. 2017, 85, 32–47. [Google Scholar] [CrossRef]
- Artifon, E.L.; Marson, F.P.; Gaidhane, M.; Kahaleh, M.; Otoch, J.P. Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: Is there any difference? Gastrointest. Endosc. 2015, 81, 950–959. [Google Scholar] [CrossRef]
- Horiuchi, A.; Nakayama, Y.; Kajiyama, M.; Tanaka, N. Effect of precut sphincterotomy on biliary cannulation based on the characteristics of the major duodenal papilla. Clin. Gastroenterol. Hepatol. 2007, 5, 1113–1138. [Google Scholar] [CrossRef]
- Matsushita, M.; Uchida, K.; Nishio, A.; Takakuwa, H.; Okazaki, K. Small papilla: Another risk factor for post-sphincterotomy perforation. Endoscopy 2008, 40, 875–876. [Google Scholar]
- Adler, D.G. ERCP biliary cannulation difficulty as a function of papillary subtypes: A tale of shapes and Shar-Pei dogs. Gastrointest. Endosc. 2019, 90, 964–965. [Google Scholar]
- Halttunen, J.; Meisner, S.; Aabakken, L.; Arnelo, U.; Grönroos, J.; Hauge, T.; Kleveland, P.M.; Nordblad Schmidt, P.; Saarela, A.; Swahn, F.; et al. Difficult cannulation as defined by a prospective study of the Scandinavian Association for Digestive Endoscopy (SADE) in 907 ERCPs. Scand. J. Gastroenterol. 2014, 49, 752–758. [Google Scholar] [CrossRef]
- Löhr, J.M.; Aabakken, L.; Arnelo, U.; Grönroos, J.; Halttunen, J.; Hauge, T.; Jonas, E.; Kleveland, P.M.; Nordblad Schmidt, P.; Swahn, F.; et al. How to cannulate? A survey of the Scandinavian Association for Digestive Endoscopy (SADE) in 141 endoscopists. Scand. J Gastroenterol. 2012, 47, 861–869. [Google Scholar] [CrossRef]
- Haraldsson, E.; Lundell, L.; Swahn, F.; Enochsson, L.; Löhr, J.M.; Arnelo, U. Scandinavian Association for Digestive Endoscopy (SADE) Study Group of Endoscopic Retrograde Cholangio-Pancreaticography. Endoscopic classification of the papilla of Vater. Results of an inter-and intraobserver agreement study. United Eur. Gastroenterol. J. 2017, 5, 504–510. [Google Scholar] [CrossRef]
- Haraldsson, E.; Kylänpää, L.; Grönroos, J.; Saarela, A.; Toth, E.; Qvigstad, G.; Hult, M.; Lindström, O.; Laine, S.; Karjula, H.; et al. Macroscopic appearance of the major duodenal papilla influences bile duct cannulation: A prospective multicenter study by the Scandinavian Association for Digestive Endoscopy Study Group for ERCP. Gastrointest. Endosc. 2019, 90, 957–963. [Google Scholar] [CrossRef]
- Canard, J.M.; Lennon, A.M.; Létard, J.C.; Etienne, J.; Okolo, P. Endoscopic Retrograde Cholangiopancreatography; Elsevier Churchill livingstone: Edinburgh, UK, 2011; pp. 370–465. [Google Scholar]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Lee, T.H.; Hwang, S.O.; Choi, H.J.; Jung, Y.; Cha, S.W.; Chung, I.K.; Moon, J.H.; Cho, Y.D.; Park, S.H.; Kim, S.J. Sequential algorithm analysis to facilitate selective biliary access for difficult biliary cannulation in ERCP: A prospective clinical study. BMC Gastroenterol. 2014, 14, 30. [Google Scholar] [CrossRef]
- Testoni, P.A. No treatment for asymptomatic common bile ducts stones? Endosc. Int. Open 2017, 11, E1151–E1152. [Google Scholar] [CrossRef][Green Version]
- Elmunzer, B.J. Reducing the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig. Endosc. 2017, 29, 749–757. [Google Scholar] [CrossRef]
- Tse, F.; Yuan, Y.; Moayyedi, P.; Leontiadis, G.I.; Barkun, A.N. Double-guidewire technique in difficult biliary cannulation for the prevention of post-ERCP pancreatitis: A systematic review and meta-analysis. Endoscopy 2017, 49, 15–26. [Google Scholar] [CrossRef]
- Lee, Y.S.; Cho, C.M.; Cho, K.B.; Heo, J.; Jung, M.K.; Kim, S.B.; Kim, K.H.; Kim, T.N.; Lee, D.W.; Han, J.; et al. Difficult Biliary Cannulation from the Perspective of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis: Identifying the Optimal Timing for the Rescue Cannulation Technique. Gut Liver 2020. [Google Scholar] [CrossRef]
- Dumonceau, J.M.; Andriulli, A.; Elmunzer, B.J.; Mariani, A.; Meister, T.; Deviere, J.; Marek, T.; Baron, T.H.; Hassan, C.; Testoni, P.A.; et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline–updated June 2014. Endoscopy 2014, 46, 799–815. [Google Scholar] [CrossRef]
- Dumonceau, J.M.; Kapral, C.; Aabakken, L.; Papanikolaou, I.S.; Tringali, A.; Vanbiervliet, G.; Beyna, T.; Dinis-Ribeiro, M.; Hritz, I.; Mariani, A.; et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2020, 52, 127–149. [Google Scholar] [CrossRef]
- Das, A.; Singh, P.; Sivak, M.V., Jr.; Chak, A. Pancreatic-stent placement for prevention of post-ERCP pancreatitis: A cost-effectiveness analysis. Gastrointest. Endosc. 2007, 65, 960–968. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Papilla | n (%) |
|---|---|
| Regular | 168 (52.1%) |
| Type 1 | 36 (11.1%) |
| Type 2 | 61 (18.9%) |
| Type 3 | 32 (9.9%) |
| Type 4 | 25 (7.7%) |
| Papilla | Cannulation | Total | 95% CI | ||||
|---|---|---|---|---|---|---|---|
| Standard | Difficult | Yates Chi-Square = 24.96 | |||||
| Regular | 126 | 75% | 42 | 25% | 168 | r = 0.282 | p = 0.00358 |
| Type 1 | 12 | 33.3% | 24 | 66.7% | 36 | ||
| Type 2 | 41 | 67.2% | 20 | 32.8% | 61 | ||
| Type 3 | 17 | 53.1% | 15 | 46.9% | 32 | ||
| Type 4 | 15 | 60% | 10 | 40% | 25 | ||
| Papilla (n = 322) | Overall Post-ERCP Adverse Events | Test † | p-Value * (95%CI) | |
|---|---|---|---|---|
| Absent (n = 262) | Present (n = 60) | |||
| Regular papilla | 140 (83.33%) | 28 (16.67%) | 16.087 | 0.0066 * |
| Type 1 | 26 (72.22%) | 10 (27.78%) | ||
| Type 2 | 53 (86.89%) | 8 (13.11%) | ||
| Type 3 | 29 (90.63%) | 3 (9.38%) | ||
| Type 4 | 14 (56%) | 11 (44%) | ||
| Post-ERCP pancreatitis | ||||
| Absent (n = 289) | Present (n = 33) | |||
| Regular papilla | 150 (89.29%) | 18 (10.71%) | 13.275 | 0.01001 * |
| Type 1 | 31 (86.11%) | 5 (13.89%) | ||
| Type 2 | 59 (96.72%) | 2 (3.28%) | ||
| Type 3 | 31 (96.88%) | 1 (3.13%) | ||
| Type 4 | 18 (72%) | 7 (28%) | ||
| Post-ERCP bleeding | ||||
| Absent (n = 312) | Present (n = 10) | |||
| Regular papilla | 163 (97.02%) | 5 (2.98%) | 2.9099 | 0.5730 |
| Type 1 | 36 (100%) | 0 (0%) | ||
| Type 2 | 58 (95.08%) | 3 (4.92%) | ||
| Type 3 | 31 (96.88%) | 1 (3.13%) | ||
| Type 4 | 24 (96%) | 1 (4%) | ||
| Post-ERCP infections | ||||
| Absent (n = 299) | Present (n = 23) | |||
| Regular Papilla | 160 (95.24%) | 8 (4.76%) | 9.145977 | 0.05756 |
| Type 1 | 29 (80.56%) | 7 (19.44%) | ||
| Type 2 | 57 (93.44%) | 4 (6.56%) | ||
| Type 3 | 31 (96.88%) | 1 (3.13%) | ||
| Type 4 | 22 (88%) | 3 (12%) | ||
| Papilla | Rescue Papillotomy Techniques | Total | 95% CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Needle-Knife Freehand Precut | Needle-Knife Fistulotomy | Transpancreatic Biliary Sphincterotomy | M-L Chi-Square = 32.6658 | ||||||
| Regular | 7 | 4.17% | - | - | 3 | 1.79% | 168 | r = 0.3777 | p = 0.01475 |
| Type 1 | 2 | 5.56% | - | - | 2 | 5.56% | 36 | ||
| Type 2 | 8 | 13.11% | - | - | 2 | 3.28% | 61 | ||
| Type 3 | 3 | 9.38% | 3 | 9.38% | 2 | 6.25% | 32 | ||
| Type 4 | 2 | 8% | 1 | 4% | - | - | 25 | ||
| Papilla | Prophylactic Pancreatic Stent | 95% CI | ||
|---|---|---|---|---|
| Yates-Chi-Square = 1.60275 | ||||
| Regular | 5 | 2.98% | r = 0.2119129 | p = 0.75415 |
| Type 1 | 1 | 2.78% | ||
| Type 2 | 3 | 4.92% | ||
| Type 3 | 1 | 3.13% | ||
| Type 4 | 2 | 8.00% | ||
| Multiple Regression | SE | Wald Test | P | Odd Ratio | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Overall post-ERCP adverse events | ||||||
| Papillary morphology (ref.: regular papilla) | 7.324 | 0.198 | ||||
| Type 1 | 0.515 | 0.985 | 0.321 | 0.600 | 0.219 | 1.646 |
| Type 2 | 0.546 | 1.001 | 0.317 | 0.579 | 0.199 | 1.688 |
| Type 3 | 0.458 | 2.982 | 0.084 | 0.453 | 0.185 | 1.113 |
| Type 4 | 0.507 | 0.552 | 0.458 | 1.457 | 0.540 | 3.932 |
| Constant | 0.430 | 2.270 | 0.132 | 0.523 | ||
| Duodenal diverticulum (ref.: absent diverticulum) | 1.487 | 0.685 | ||||
| Type 1 | 0.272 | 0.715 | 0.999 | 0.231 | 0.142 | 0.528. |
| Type 2 | 0.464 | 0.684 | 0.408 | 1.468 | 0.591 | 3.642 |
| Type 3 | 0.080 | 0.716 | 0.397 | 0.401 | 0.048 | 3.331 |
| Difficult cannulation | 0.299 | 11.370 | 0.001 * | 2.744 | 1.526 | 4.933 |
| Alternative access papillotomy (ref.: standard biliary sphincterotomy) | 2.472 | 0.480 | ||||
| Needle-knife freehand precut | 0.473 | 0.543 | 0.461 | 1.417 | 0.561 | 3.581 |
| Needle-knife fistulotomy | 0.079 | 0.370 | 0.543 | 1.929 | 0.233 | 15.994 |
| Transpancreatic biliary sphincterotomy | 0.834 | 1.303 | 0.254 | 0.386 | 0.075 | 1.979 |
| Altered biliary anatomy (ref.: normal anatomy) | 0.379 | 0.286 | 0.593 | 0.817 | 0.389 | 1.716 |
| Bile duct stones (ref.: absence of stones) | 0.375 | 3.107 | 0.078 | 0.516 | 0.247 | 1.077 |
| Post-ERCP pancreatitis | ||||||
| Papillary anatomy (ref.: normal papilla) | 15.453 | 0.009 * | ||||
| Type 1 | 0.921 | 1.939 | 0.164 | 3.605 | 0.593 | 21.924 |
| Type 2 | 0.283 | 0.034 | 0.854 | 0.789 | 0.064 | 9.762 |
| Type 3 | 0.055 | 0.107 | 0.744 | 0.708 | 0.089 | 5.603 |
| Type 4 | 0.889 | 7.901 | 0.005 * | 12.176 | 2.131 | 69.567 |
| Difficult cannulation | 0.438 | 5.421 | 0.020 * | 2.775 | 1.175 | 6.551 |
| Alternative access papillotomy (ref.: standard biliary sphincterotomy) | 7.804 | 0.050 * | ||||
| Needle-knife freehand precut | 0.598 | 7.610 | 0.006 * | 5.203 | 1.612 | 16.795 |
| Needle-knife fistulotomy | 0.934 | 0.000 | 0.999 | 0.000 | 0.000 | 0.001 |
| Transpancreatic biliary sphincterotomy | 0.130 | 0.000 | 0.995 | 1.007 | 0.110 | 9.219 |
| Constant | 0.744 | 29.358 | 0.000 | 0.018 | ||
| Post-ERCP bleeding | ||||||
| Difficult cannulation | 0.402 | 13.012 | <0.001 * | 4.270 | 1.940 | 5.397 |
| Pancreatic duct cannulation | 0.417 | 0.687 | 0.407 | 1.413 | 0.624 | 3.200 |
| Papillotomy (ref.: no papillotomy) | 4.577 | 0.03 1* | ||||
| Complete biliary sphincterotomy | 0.665 | 3.319 | 0.068 | 3.356 | 0.912 | 12.346 |
| Incomplete papillotomy | 0.645 | 4.573 | 0.032 * | 3.976 | 1.122 | 4.086 |
| Brush cytology: malignant | 0.735 | 6.580 | 0.010 * | 6.592 | 1.560 | 7.845 |
| Balloon sphincteroplasty | 0.630 | 4.096 | 0.043 * | 0.279 | 0.181 | 0.961 |
| Constant | 0.635 | 38.612 | <0.001 | 0.019 | ||
| Post-ERCP infections | ||||||
| Papillotomy (ref.: no papillotomy) | 4.336 | 0.114 | ||||
| Complete biliary sphincterotomy | 0.448 | 3.645 | 0.036 * | 0.425 | 0.177 | 0.823 |
| Incomplete papillotomy | 0.528 | 2.626 | 0.010 * | 0.428 | 0.151 | 0.896 |
| Indication: bile duct stones (ref.: stenoses) | 0.475 | 0.781 | 0.377 | 0.657 | 0.259 | 1.667 |
| Biliary stent insertion (ref.: absence of stents) | 0.406 | 4.956 | 0.026 * | 2.467 | 1.114 | 5.463 |
| Constant | 0.337 | 28.388 | 0.000 | 0.166 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balan, G.G.; Arya, M.; Catinean, A.; Sandru, V.; Moscalu, M.; Constantinescu, G.; Trifan, A.; Stefanescu, G.; Sfarti, C.V. Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study. J. Clin. Med. 2020, 9, 1637. https://doi.org/10.3390/jcm9061637
Balan GG, Arya M, Catinean A, Sandru V, Moscalu M, Constantinescu G, Trifan A, Stefanescu G, Sfarti CV. Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study. Journal of Clinical Medicine. 2020; 9(6):1637. https://doi.org/10.3390/jcm9061637
Chicago/Turabian StyleBalan, Gheorghe G., Mukul Arya, Adrian Catinean, Vasile Sandru, Mihaela Moscalu, Gabriel Constantinescu, Anca Trifan, Gabriela Stefanescu, and Catalin Victor Sfarti. 2020. "Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study" Journal of Clinical Medicine 9, no. 6: 1637. https://doi.org/10.3390/jcm9061637
APA StyleBalan, G. G., Arya, M., Catinean, A., Sandru, V., Moscalu, M., Constantinescu, G., Trifan, A., Stefanescu, G., & Sfarti, C. V. (2020). Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study. Journal of Clinical Medicine, 9(6), 1637. https://doi.org/10.3390/jcm9061637