The Effect of Preservation Temperature on Liver, Kidney, and Pancreas Tissue ATP in Animal and Preclinical Human Models




Abstract
1. Introduction
1.1. Current State of Abdominal Transplantation (Liver, Kidneys, and Pancreas)
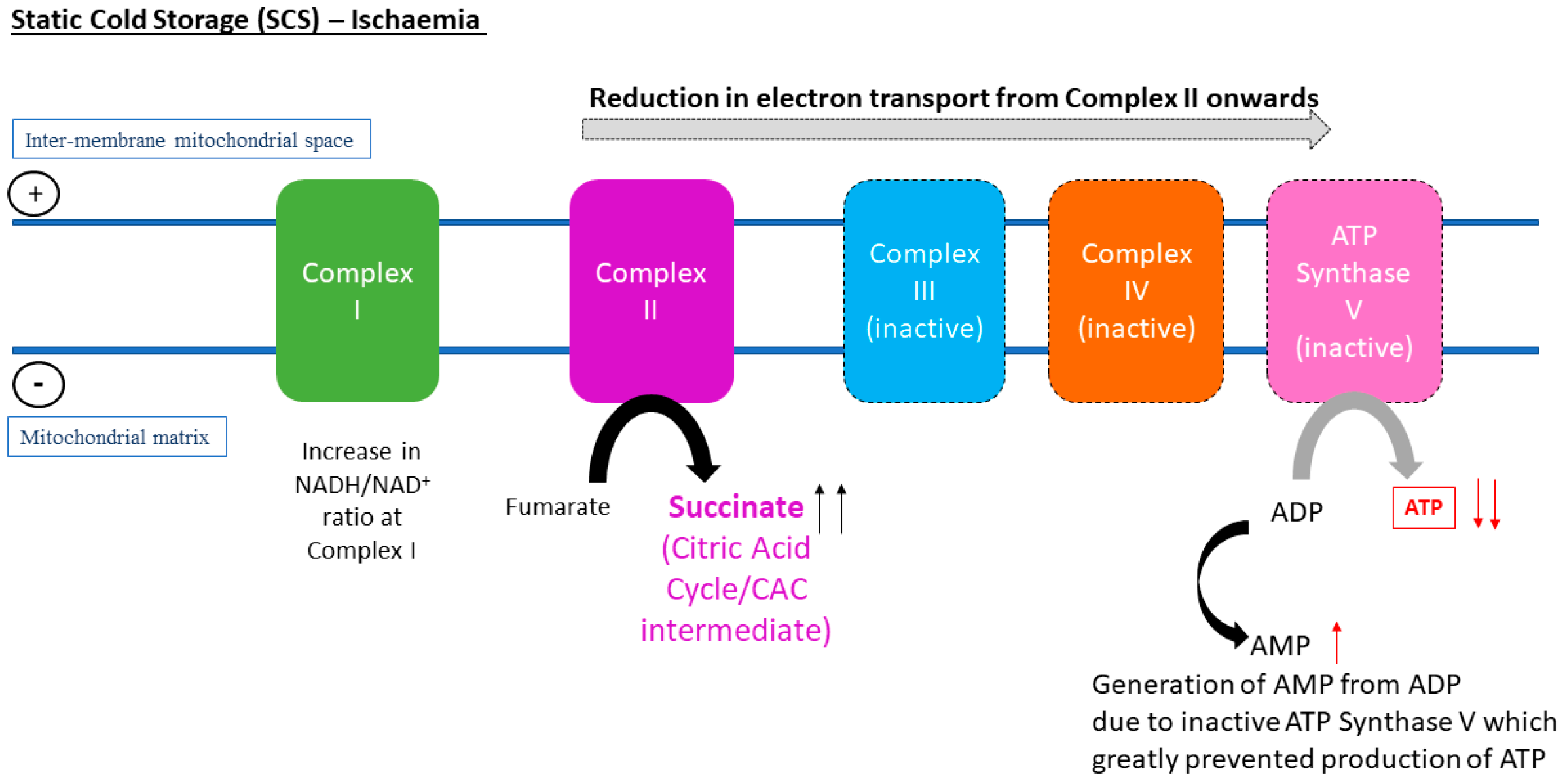
1.2. ATP Depletion and Ischaemia-Reperfusion Injury
1.3. Preservation Temperature, Metabolism, and Tissue ATP
2. Liver Preservation
2.1. Should a Combined Approach of HMP and NMP Be Adopted for Maximising Resynthesis of Liver Graft ATP?
2.2. Positive Effects of Subnormothermic Perfusion Temperatures (20–30 °C) Liver ATP Levels
2.3. Controlled Oxygenated Rewarming (COR) on Liver Tissue ATP
2.4. Novel Therapeutic Methods for Targeting IRI and Reconditioning of the Liver during HMP, SNMP, or NMP
3. Kidney Preservation
3.1. Oxygenated HMP (4 to 10 °C) Could Restore Synthesis of ATP in Kidneys
3.2. The Effects of Higher Perfusion Temperatures (>4–10 °C) on Kidney Viability are Currently Unclear
4. Pancreas Preservation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADP | Adenosine DiPhosphate |
| AMP | Adenosine MonoPhosphate |
| ALT | Alanine Aminotransferase |
| AST | Aspartate Transaminase |
| ATP | Adenosine TriPhosphate |
| BMI | Body Mass Index |
| CIT | Cold Ischaemia Time |
| COR | Controlled Oxygenated Rewarming |
| DBD | Donation after Brain Death |
| DCD | Donation after Circulatory Death |
| DGF | Delayed Graft Function |
| DHOPE | Dual Hypothermic Oxygenated Machine Perfusion |
| ECD | Extended Criteria Donor |
| GGT | Gamma-Glutamyl Transferase |
| GLDH | Glutamate Dehydrogenase |
| HMP | Hypothermic Machine Perfusion |
| HOPE | Oxygenated Hypothermic Machine Perfusion |
| IRI | Ischaemia-Reperfusion Injury |
| IFLT | Ischaemia-free liver transplantation |
| LDH | Lactate De-Hydrogenase |
| MP | Machine Perfusion |
| MPS | Machine Perfusion Solution |
| MPTP | Mitochondrial Permeability Transition Pore |
| NADH | Nicotinamide Adenine Dinucleotide |
| NMP | Normothermic Machine perfusion |
| pCO2 | Partial Carbon dioxide pressure |
| PME | Phosphomonoester |
| pO2 | Partial Oxygen Pressure |
| RCT | Randomized Controlled Trial |
| ROS | Reactive Oxygen Species |
| SCS | Static Cold Storage |
| siRNA | Small Interfering RNA |
| SNMP | Subnormothermic Machine Perfusion |
| TBARS | ThioBarbituric Acid Reactive Substances |
| TEM | Transmission Electron Microscopy |
| TNF-alpha | Tumour Necrosis Factor-Alpha |
| UW | University of Wisconsin Solution |
| VCAM-1 | Vascular Cell Adhesion Molecule 1 |
| vWF | Von Willebrand Factor |
| WIT | Warm Ischaemia Time |
References
- Bellini, M.I.; Nozdrin, M.; Yiu, J.; Papalois, V. Machine Perfusion for Abdominal Organ Preservation: A Systematic Review of Kidney and Liver Human Grafts. J. Clin. Med. 2019, 8, 1221. [Google Scholar] [CrossRef] [PubMed]
- Abramowicz, D.; Oberbauer, R.; Heemann, U.; Viklicky, O.; Peruzzi, L.; Mariat, C.; Crespo, M.; Budde, K.; Oniscu, G.C. Recent advances in kidney transplantation: A viewpoint from the Descartes advisory board. Nephrol. Dial. Transplant. 2018, 33, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Dziodzio, T.; Jara, M.; Hardt, J.; Weiss, S.; Viktor Ritschl, P.; Denecke, C.; Biebl, M.; Gerlach, U.; Reinke, P.; Pratschke, J.; et al. Effects of expanded allocation programmes and organ and recipient quality metrics on transplant-related costs in kidney transplantation—An institutional analysis. Transpl. Int. 2019. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J. An update on liver transplantation: A critical review. J. Autoimmun. 2016, 66, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Mannon, R.B. Delayed Graft Function: The AKI of Kidney Transplantation. Nephron 2018, 140, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Gruessner, R.W.; Gruessner, A.C.; Tan, M.; Kandaswamy, R.; Sutherland, D.E.R.; Humar, A. Risk Factors and Impact of Delayed Graft Function after Pancreas Transplants. Arab. Archaeol. Epigr. 2004, 4, 758–762. [Google Scholar]
- Santangelo, M.; Furian, L.; Kessaris, N.; Hadaya, K.; Kimenai, D.; Bellini, M.I. Renal Transplantation: What Has Changed in Recent Years. BioMed Res. Int. 2019, 2019, 3618104. [Google Scholar]
- Bellini, M.I.; Charalampidis, S.; Herbert, P.E.; Bonatsos, V.; Crane, J.; Muthusamy, A.; Dor, F.J.M.F.; Papalois, V. Cold Pulsatile Machine Perfusion versus Static Cold Storage in Kidney Transplantation: A Single Centre Experience. BioMed Res. Int. 2019, 2019, 7435248. [Google Scholar] [CrossRef]
- Wu, M.-Y.; Yiang, G.-T.; Liao, W.-T.; Tsai, A.P.-Y.; Cheng, Y.-L.; Cheng, P.-W.; Li, C.-Y.; Li, C.-J. Current Mechanistic Concepts in Ischemia and Reperfusion Injury. Cell. Physiol. Biochem. 2018, 46, 1650–1667. [Google Scholar] [CrossRef]
- Wang, Y.; Branicky, R.; Noë, A.; Hekimi, S. Superoxide dismutases: Dual roles in controlling ROS damage and regulating ROS signaling. J. Cell Biol. 2018, 217, 1915–1928. [Google Scholar] [CrossRef]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell biology of ischemia/reperfusion injury. Int. Rev. Cell Mol. Biol. 2012, 298, 229–317. [Google Scholar] [PubMed]
- Ishikawa, J.; Oshima, M.; Iwasaki, F.; Suzuki, R.; Park, J.; Nakao, K.; Matsuzawa-Adachi, Y.; Mizutsuki, T.; Kobayashi, A.; Abe, Y.; et al. Hypothermic temperature effects on organ survival and restoration. Sci. Rep. 2015, 5, 9563. [Google Scholar] [CrossRef] [PubMed]
- Jennings, R.B.; Sommers, H.M.; Smyth, G.A.; Flack, H.A.; Linn, H. Myocardial necrosis induced by temporary occlusion of a coronary artery in the dog. Arch. Pathol. 1960, 70, 68–78. [Google Scholar] [PubMed]
- Bellini, M.I.; D’Andrea, V. Organ preservation: Which temperature for which organ? J. Int. Med Res. 2019, 47, 2323–2325. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; Nicholson, H.F.L.; Nicholson, M.L. Oxygenated Kidney Preservation Techniques. Transplant. 2012, 93, 455–459. [Google Scholar] [CrossRef] [PubMed]
- Steichen, C.; Giraud, S.; Bon, D.; Barrou, B.; Badet, L.; Salamé, E.; Kerforne, T.; Allain, G.; Roumy, J.; Jayle, C.; et al. Barriers and Advances in Kidney Preservation. BioMed Res. Int. 2018, 2018, 9206257. [Google Scholar] [CrossRef] [PubMed]
- Boteon, Y.L.; Laing, R.W.; Schlegel, A.; Wallace, L.; Smith, A.; Attard, J.; Bhogal, R.H.; Neil, D.A.H.; Hübscher, S.; Perera, M.T.P.R.; et al. Combined Hypothermic and Normothermic Machine Perfusion Improves Functional Recovery of Extended Criteria Donor Livers. Liver Transplant. 2018, 24, 1699–1715. [Google Scholar] [CrossRef] [PubMed]
- Minor, T.; Efferz, P.; Fox, M.; Wohlschlaeger, J.; Lüer, B. Controlled Oxygenated Rewarming of Cold Stored Liver Grafts by Thermally Graduated Machine Perfusion Prior to Reperfusion. Arab. Archaeol. Epigr. 2013, 13, 1450–1460. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, C.J.; Farid, W.R.; De Jonge, J.; Metselaar, H.J.; Kazemier, G.; Van Der Laan, L.J. Biomarkers to assess graft quality during conventional and machine preservation in liver transplantation. J. Hepatol. 2014, 61, 672–684. [Google Scholar] [CrossRef] [PubMed]
- Vajdová, K.; Graf, R.; Clavien, P.-A.; Clavien, P. ATP-supplies in the cold-preserved liver: A long-neglected factor of organ viability. Hepatology 2002, 36, 1543–1552. [Google Scholar] [CrossRef]
- Westerkamp, A.C.; Karimian, N.; Matton, A.P.; Mahboub, P.; Van Rijn, R.; Wiersema-Buist, J.; De Boer, M.T.; Leuvenink, H.G.; Gouw, A.S.; Lisman, T.; et al. Oxygenated Hypothermic Machine Perfusion After Static Cold Storage Improves Hepatobiliary Function of Extended Criteria Donor Livers. Transplantation 2016, 100, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Ferrigno, A.; Rizzo, V.; Boncompagni, E.; Bianchi, A.; Gringeri, E.; Neri, D.; Richelmi, P.; Freitas, I.; Cillo, U.; Vairetti, M. Machine perfusion at 20 degrees C reduces preservation damage to livers from non-heart beating donors. Cryobiology 2011, 62, 152–158. [Google Scholar] [CrossRef]
- Berendsen, T.A.; Bruinsma, B.G.; Lee, J.; D’Andrea, V.; Liu, Q.; Izamis, M.-L.; Uygun, K.; Yarmush, M.L. A simplified subnormothermic machine perfusion system restores ischemically damaged liver grafts in a rat model of orthotopic liver transplantation. Transplant. Res. 2012, 1, 6. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bruinsma, B.G.; Berendsen, T.A.; Izamis, M.L.; Yarmush, M.L.; Uygun, K. Determination and extension of the limits to static cold storage using subnormothermic machine perfusion. Int. J. Artif. Organs 2013, 36, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, B.G.; Yeh, H.; Özer, Ş.; Martins, P.N.; Farmer, A.; Wu, W.; Saeidi, N.; Dries, S.O.D.; Berendsen, T.A.; Smith, R.N.; et al. Subnormothermic machine perfusion for ex vivo preservation and recovery of the human liver for transplantation. Am. J. Transplant. 2014, 14, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, B.G.; Sridharan, G.V.; Weeder, P.D.; Avruch, J.H.; Saeidi, N.; Özer, S.; Geerts, S.; Porte, R.J.; Heger, M.; Van Gulik, T.M.; et al. Metabolic profiling during ex vivo machine perfusion of the human liver. Sci. Rep. 2016, 6, 22415. [Google Scholar] [CrossRef]
- Ferrigno, A.; Di Pasqua, L.G.; Berardo, C.; Siciliano, V.; Rizzo, V.; Mannucci, B.; Richelmi, P.; Croce, A.C.; Vairetti, M. Liver Graft Susceptibility during Static Cold Storage and Dynamic Machine Perfusion: DCD versus Fatty Livers. Int. J. Mol. Sci. 2017, 19, 109. [Google Scholar] [CrossRef] [PubMed]
- Von Horn, C.; Baba, H.A.; Hannaert, P.; Hauet, T.; Leuvenink, H.; Paul, A.; Minor, T.; COPE Consortium Partners. Controlled oxygenated rewarming up to normothermia for pretransplant reconditioning of liver grafts. Clin. Transplant. 2017, 31, e13101. [Google Scholar] [CrossRef]
- Xu, H.; Berendsen, T.; Kim, K.; Soto-Gutierrez, A.; Bertheium, F.; Yarmush, M.L.; Hertl, M. Excorporeal normothermic machine perfusion resuscitates pig DCD livers with extended warm ischemia. J. Surg. Res. 2012, 173, e83–e88. [Google Scholar] [CrossRef]
- Maida, K.; Akamatsu, Y.; Hara, Y.; Tokodai, K.; Miyagi, S.; Kashiwadate, T.; Miyazawa, K.; Kawagishi, N.; Ohuchi, N. Short Oxygenated Warm Perfusion with Prostaglandin E1 Administration Before Cold Preservation as a Novel Resuscitation Method for Liver Grafts From Donors After Cardiac Death in a Rat In Vivo Model. Transplantation 2016, 100, 1052–1058. [Google Scholar] [CrossRef]
- Ferrigno, A.; Di Pasqua, L.G.; Bianchi, A.; Richelmi, P.; Vairetti, M. Metabolic shift in liver: Correlation between perfusion temperature and hypoxia inducible factor-1alpha. World J. Gastroenterol. 2015, 21, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Kron, P.; Graf, R.; Dutkowski, P.; Clavien, P.-A. Warm vs. cold perfusion techniques to rescue rodent liver grafts. J. Hepatol. 2014, 61, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Dutkowski, P.; Graf, R.; Clavien, P.A. Rescue of the Cold Preserved Rat Liver by Hypothermic Oxygenated Machine Perfusion. Arab. Archaeol. Epigr. 2006, 6, 903–912. [Google Scholar] [CrossRef] [PubMed]
- De Rougemont, O.; Breitenstein, S.; Leskosek, B.; Weber, A.; Graf, R.; Clavien, P.A.; Dutkowski, P. One hour hypothermic oxygenated perfusion (HOPE) protects nonviable liver allografts donated after cardiac death. Ann. Surg. 2009, 250, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, R.; Karimian, N.; Matton, A.P.M.; Burlage, L.C.; Westerkamp, A.C.; van den Berg, A.P.; de Kleine, R.H.J.; de Boer, M.T.; Lisman, T.; Porte, R.J. Dual hypothermic oxygenated machine perfusion in liver transplants donated after circulatory death. Br. J. Surg. 2017, 104, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Dutkowski, P.; Guarrera, J.V.; De Jonge, J.; Martins, P.N.; Porte, R.J.; Clavien, P.-A.; De Jonge, J. Evolving Trends in Machine Perfusion for Liver Transplantation. Gastroenterology 2019, 156, 1542–1547. [Google Scholar] [CrossRef] [PubMed]
- Czigany, Z.; Lurje, I.; Tolba, R.H.; Neumann, U.P.; Tacke, F.; Lurje, G. Machine perfusion for liver transplantation in the era of marginal organs-New kids on the block. Liver Int. 2019, 39, 228–249. [Google Scholar] [CrossRef] [PubMed]
- Berardo, C.; Di Pasqua, L.G.; Siciliano, V.; Rizzo, V.; Richelmi, P.; Ferrigno, A.; Vairetti, M. Machine Perfusion at 20 degrees C Prevents Ischemic Injury and Reduces Hypoxia-Inducible Factor-1alpha Expression During Rat Liver Preservation. Ann. Transplant. 2017, 22, 581–589. [Google Scholar] [CrossRef]
- Okamura, Y.; Hata, K.; Tanaka, H.; Hirao, H.; Kubota, T.; Inamoto, O.; Kageyama, S.; Tamaki, I.; Yermek, N.; Yoshikawa, J.; et al. Impact of Subnormothermic Machine Perfusion Preservation in Severely Steatotic Rat Livers: A Detailed Assessment in an Isolated Setting. Am. J. Transplant. 2017, 17, 1204–1215. [Google Scholar] [CrossRef]
- Yang, W.; Chen, J.; Meng, Y.; Chen, Z.; Yang, J. Novel Targets for Treating Ischemia-Reperfusion Injury in the Liver. Int. J. Mol. Sci. 2018, 19, 1302. [Google Scholar] [CrossRef]
- Karimian, N.; Yeh, H. Opportunities for Therapeutic Intervention During Machine Perfusion. Curr. Transplant. Rep. 2017, 4, 141–148. [Google Scholar] [CrossRef]
- Gillooly, A.R.; Perry, J.; Martins, P.N. First Report of siRNA Uptake (for RNA Interference) During Ex Vivo Hypothermic and Normothermic Liver Machine Perfusion. Transplantation 2019, 103, e56–e57. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Guo, Z.; Zhao, Q.; Ju, W.; Wang, D.; Wu, L.; Yang, L.; Ji, F.; Tang, Y.; Zhang, Z.; et al. The first case of ischemia-free organ transplantation in humans: A proof of concept. Am. J. Transplant. 2018, 18, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Buchs, J.B.; Lazeyras, F.; Ruttimann, R.; Nastasi, A.; Morel, P. Oxygenated hypothermic pulsatile perfusion versus cold static storage for kidneys from non heart-beating donors tested by in-line ATP resynthesis to establish a strategy of preservation. Perfusion 2011, 26, 159–165. [Google Scholar] [CrossRef]
- Lazeyras, F.; Buhler, L.; Vallée, J.-P.; Hergt, M.; Nastasi, A.; Ruttimann, R.; Morel, P.; Buchs, J.-B. Detection of ATP by “in line” 31P magnetic resonance spectroscopy during oxygenated hypothermic pulsatile perfusion of pigs’ kidneys. Magma 2012, 25, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Kay, M.D.; Hosgood, S.A.; Harper, S.J.; Bagul, A.; Waller, H.L.; Nicholson, M.L. Normothermic Versus Hypothermic Ex Vivo Flush Using a Novel Phosphate-Free Preservation Solution (AQIX) in Porcine Kidneys. J. Surg. Res. 2011, 171, 275–282. [Google Scholar] [CrossRef]
- Ravaioli, M.; Baldassare, M.; Vasuri, F.; Pasquinelli, G.; Laggetta, M.; Valente, S.; De Pace, V.; Neri, F.; Siniscalchi, A.; Zanfi, C.; et al. Strategies to Restore Adenosine Triphosphate (ATP) Level After More than 20 Hours of Cold Ischemia Time in Human Marginal Kidney Grafts. Ann. Transplant. 2018, 23, 34–44. [Google Scholar] [CrossRef]
- Kaminski, J.; Delpech, P.O.; Kaaki-Hosni, S.; Promeyrat, X.; Hauet, T.; Hannaert, P. Oxygen Consumption by Warm Ischemia-Injured Porcine Kidneys in Hypothermic Static and Machine Preservation. J. Surg. Res. 2019, 242, 78–86. [Google Scholar] [CrossRef]
- Wijermars, L.G.; Schaapherder, A.F.; De Vries, D.K.; Verschuren, L.; Wüst, R.C.; Kostidis, S.; Mayboroda, O.A.; Prins, F.; Ringers, J.; Bierau, J.; et al. Defective postreperfusion metabolic recovery directly associates with incident delayed graft function. Kidney Int. 2016, 90, 181–191. [Google Scholar] [CrossRef]
- Bhattacharjee, R.N.; Ruthirakanthan, A.; Sun, Q.; Richard-Mohamed, M.; Luke, S.; Jiang, L.; Aquil, S.; Sharma, H.; Tun-Abraham, M.E.; Alharbi, B.; et al. Subnormothermic Oxygenated Perfusion Optimally Preserves Donor Kidneys Ex Vivo. Kidney Int. Rep. 2019, 4, 1323–1333. [Google Scholar] [CrossRef]
- Krzywonos-Zawadzka, A.; Franczak, A.; Moser, M.A.J.; Olejnik, A.; Sawicki, G.; Bil-Lula, I. Pharmacological Protection of Kidney Grafts from Cold Perfusion-Induced Injury. BioMed Res. Int. 2019, 2019, 9617087. [Google Scholar] [CrossRef]
- Hamaoui, K.; Gowers, S.; Damji, S.; Rogers, M.; Leong, C.L.; Hanna, G.; Darzi, A.; Boutelle, M.; Papalois, V. Rapid sampling microdialysis as a novel tool for parenchyma assessment during static cold storage and hypothermic machine perfusion in a translational ex vivo porcine kidney model. J. Surg. Res. 2016, 200, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Sui, W.; Wang, B.; Zou, H.; Zou, G.; Luo, H. Expression of MMP-2 and TIMP-1 in Renal Tissue of Patients with Chronic Active Antibody-mediated Renal Graft Rejection. Diagn. Pathol. 2012, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.A.J.; Arcand, S.; Lin, H.-B.; Wojnarowicz, C.; Sawicka, J.; Banerjee, T.; Luo, Y.; Beck, G.R.; Luke, P.P.; Sawicki, G. Protection of the Transplant Kidney from Preservation Injury by Inhibition of Matrix Metalloproteinases. PLoS ONE 2016, 11, e0157508. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, E.; Domanski, L.; Bober, J.; Safranow, K.; Romanowski, M.; Pawlik, A.; Kwiatkowski, S.; Ciechanowski, K. Urinary Metalloproteinases-9 and -2 and Their Inhibitors TIMP-1 and TIMP-2 are Markers of Early and Long-Term Graft Function After Renal Transplantation. Kidney Blood Press. Res. 2016, 41, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Bank, J.R.; Ruhaak, R.; Soonawala, D.; Mayboroda, O.; Romijn, F.P.; van Kooten, C.; Cobbaert, C.M.; de Fijter, J.W. Urinary TIMP-2 Predicts the Presence and Duration of Delayed Graft Function in Donation After Circulatory Death Kidney Transplant Recipients. Transplantation 2019, 103, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Leemkuil, M.; Lier, G.; Engelse, M.A.; Ploeg, R.J.; De Koning, E.J.P.; Hart, N.A.T.; Krikke, C.; Leuvenink, H.G.D. Hypothermic Oxygenated Machine Perfusion of the Human Donor Pancreas. Transplant. Direct 2018, 4, e388. [Google Scholar] [CrossRef] [PubMed]
- Hamaoui, K.; Papalois, V. Machine Perfusion and the Pancreas: Will It Increase the Donor Pool? Curr. Diabetes Rep. 2019, 19, 56. [Google Scholar] [CrossRef]
- Kumar, R.; Chung, W.Y.; Runau, F.; Isherwood, J.D.; Kuan, K.G.; West, K.; Garcea, G.; Dennison, A.R. Ex vivo normothermic porcine pancreas: A physiological model for preservation and transplant study. Int. J. Surg. 2018, 54, 206–215. [Google Scholar] [CrossRef]
- Kuroda, Y.; Fujino, Y.; Morita, A.; Ku, Y.; Saitoh, Y. Correlation between high adenosine triphosphate tissue concentration and good posttransplant outcome for the canine pancreas graft after preservation by the two-layer cold storage method. Transplantation 1991, 52, 989–991. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study. | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Westerkamp [21] | 18 | - | 7 or 9 | Belzer-UW Machine Perfusion solution, pH 7.4, calcium chloride, dextrose, potassium phosphate | 2 | HMP (ex situ viability testing by NMP) | 10–12 | Human, discarded livers (DCD with advanced donor age, DBD with high BMI) | Tissue ATP, O2 consumption, vascular resistance, bile production, AST, ALT, LDH, GGT, histology | ATP Bioluminescence assay kit CLS II (Roche Diagnostics GmbH, Boehringer Mannheim, Germany) | 2 h end-ischaemic HMP preservation was shown to be effective in energy status restoration of DCD liver grafts which showed a >15-fold increase in ATP level and significantly higher bile production versus SCS group. There was no significant reduction in hepatobiliary injury markers. Thus, HMP may be more effective in restoration of energy status and function, instead of reduction of preexisting injury. Further testing in clinical liver transplant trial is suggested. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferrigno [22] | 17 | 0.5 | - | Modified University of Wisconsin –Gluconate solution (modified UW-G) with glucose, adenosine, mannitol | 6 | SNMP (graft assessed by NMP reperfusion) | 20 | Rat, DCD livers | Tissue ATP, AST, ALT, LDH, total bile production, GDH, histochemistry | ATP Bioluminescence Assay Kit CLS II (Roche Molecular Biochemicals, Milan, Italy) | An increase in ATP and bile production and a reduction in hepatic damage and GDH levels in NGBD livers were reported in SNMP group vs. SCS group. MP at 20 °C is shown to protect marginal grafts against IRI and graft recovery. A liver transplantation model is needed for further validation. |
| Berendsen [23] | 24 | 0 or 1 | - | WE with sodium bicarb and L-glutamine supplemented with insulin, penicillin, hydrocortisone and heparin | 2–3 | SNMP | 21 | Rat, DCD livers | Tissue ATP, ALT, AST, pO2, bile production, post-transplantation analysis (blood samples, jaundice, infection, body weight, histology) | ApoSENSOR ATP Luminescence Assay Kit (BioVision Inc, Milpitas, CA, USA) | This study presented a SNMP orthotopic liver transplantation model with oxygenated and supplemented cell culture medium as perfusate. In the two groups subjected to WIT (1 h), SNMP was associated with 83.3% one month survival rate vs. 0% in SCS group. After ~2.5 h of SNMP, ATP levels in WIT group were restored from about 6% of fresh controls to a level exceeding that of fresh controls. Clinical parameters were comparable amongst viable animals. SNMP may have the potential to regenerate DCD livers. |
| Bruinsma [24] | 40 | - | 0 (fresh) or 24 or 48 or 72 or 120 | WE | 3 | SNMP | 20 | Rat, livers (procurement after anesthesia) | Tissue ATP, ALT, blood gas analysis, vascular resistance, post-transplantation analysis (blood samples, AST, ALT, total bilirubin, glucose, blood urea nitrogen, albumin, body weight) | Luminescence- based cell viability assay (Biovision, Milpitas, CA) | This study assessed the limits of SNMP to restore liver tissue metabolic energy and viability in grafts subjected to different durations of SCS. ATP level decreased and vascular resistance increased with increased duration of SCS. Compared to non-perfused control groups, increase in ATP levels was reported in all SNMP groups except for 120 h. Cold storage for 72 h appeared to be the limit of SNMP to restore ATP levels to that in fresh liver samples. However, post-transplantation survival rates, ATP recovery and vascular resistance suggested that recoverability of liver viability by SNMP is limited to 48 h of SCS. ATP recovery and vascular resistance are suggested to be useful parameters for assessing the ability of MP to improve liver viability after extended cold preservation. |
| Bruinsma [25] | 7 | <1 | ~11 | WE supplemented with insulin, penicillin, streptomycin, hydrocortisone | 3 | SNMP | 21 | Human, discarded livers (5 DCD & 2 DBD) | Tissue ATP, ALT, LDH, blood gas analysis, oxygen uptake rate, bile production, ALP, phospholipids, histology | Luminescence-based cell viability assay (BioVision) | An overall 3.7-fold increase in ATP was observed post-SNMP. Clinical parameters, e.g. mean LDH, ALP, ALT, lactate and relative WIT were lower in livers with high ATP levels compared to livers with low ATP levels (not statistically significant). A significant (p = 0.02) negative correlation was observed between ATP at the end of SNMP and ALT values (which is a marker of hepatic injury). Ex vivo SNMP was shown to be effective in the maintenance of post-ischaemic liver function with improvement of hepatobiliary parameters and metabolic energy status. |
| Bruinsma [26] | 21 | 0 or <0.5 or >0.5 | - | Nutrient-rich, cell-free, and oxygenated perfusate (exact composition not stated) | 3 | SNMP | 21 | Human, discarded livers (DBD, steatotic DCD, non-steatotic DCD with extended WIT, control DCD) | Tissue ATP, ALT, liver function (with indocyanine green clearance test), oxygen uptake rate, bile production, targeted metabolomics (cofactors: ATP/ADP/AMP, NADH/NAD+, NADPH/NADP, FAD and GSH/GSSG) and untargeted metabolomics analysis, histology | Luminescence-based assay (Cell Viability Kit; Biovision) | A significant 4.12 fold increase in ATP level was observed post SNMP. The absolute ATP level at the end of SNMP was lowest in DCD (WIT > 0.5 h) group, followed by steatotic DCD group and highest in DCD (WIT < 0.5 h) group. Oxygen consumption was highest in DCD (WIT > 0.5 h) group. From transmission electron microscopy of biopsies from the three groups, mitochondrial injury score was highest in DCD (WIT > 0.5) group, with increased membrane permeability and swelling observed. Mitochondrial scores were suggested to be negatively associated with absolute ATP levels post SNMP. In this study, metabolomic analyses of livers with steatosis and prolonged WIT were conducted, suggesting that differences in metabolic factors and perfusion parameters may be closely linked to ATP recovery in livers. |
| Ferrigno [27] | 28 | 0.5 | 6 | Oxygenated Krebs-Henseleit (KH) medium with glucose, calcium chloride, with or without Ringer Lactate | 6 | SNMP, graft viability assessed by NMP reperfusion (2 h) | 20 | Rat, livers (DCD & 2 models of fatty livers: MCD diet & obese Zucker fa/fa) | Tissue ATP, ADP, AST, ALT, LDH, total bile production, bile flow, biliary enzymes, fatty acid evaluation, total lipids | Bioluminescence assay kit CLS II (Roche Molecular Biochemicals, Milan, Italy) | The effects of SNMP followed by NMP viability assessment vs. SCS on ATP/ADP ratio recovery were compared in a DCD liver model and two fatty liver models. A combined method of OW + CS was also compared to SCS and to SNMP in DCD livers. Higher ATP/ADP ratio and reduction of hepatic injury markers were reported in OW+CS group vs. SCS-only. Interestingly, comparable ATP/ADP ratios were reported in OW+CS (4 °C) and SNMP group. In the two fatty liver models, increase in ATP/ADP ratio was reported in SNMP-treated obese Zucker livers vs. SCS, but not in SNMP-treated MCD livers. The study suggested that preservation temperature and dynamic MP may not be the only modalities for graft resuscitation, but an oxygen washout prior to SCS at 4 °C might also facilitate ATP recovery in DCD livers. This is less clear in fatty livers. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Minor [18] | 12 | - | 18 | CN with low potassium, mannitol, ketoglutarate, histidine, tryptophan | 1.5 | COR, graft integrity assessed by ex vivo NMP reperfusion | Slow gradual increase of perfusate temperature from 8 to 20 °C | Porcine, livers | Tissue ATP, ADP, AMP, ALT, AST, TNF-α, lipid peroxidation (oxygen free radical induced tissue injury), vascular resistance, bile production, caspase 3, Atg6, histology | Enzymatically determined in neutralized supernatant for protein extraction with perchloric acid of freeze dried tissue samples with hexokinase & glucose-6-phosphate dehydrogenase reactions for ATP conversion. | COR, HMP and SNP were tested in this model, with SCS as control. Tissue ATP levels significantly increased in COR group and SNP group, compared to HMP group (p < 0.05). Very low tissue ATP level was detected in SCS group. Restoration of end-ischaemic tissue energetics was comparable between COR and SNP, and COR appeared to be more protective of IRI and function, with reduction in TNF-α expression, caspase-3 activation, histology injury score and increase in bile production and portal vascular perfusion resistance. |
| von Horn [28] | 18 | 0.5 | 18 | AQIX RS-I Solution (serum and animal/human protein free), stable buffer (pH 7.20–7.45) | 1.5 | COR, graft integrity assessed by ex vivo NMP reperfusion | 2 test groups: COR20 & COR35 (gradual increase up to 20 °C or 35 °C) | Rat, DCD livers | Tissue ATP, AST, ALT, blood gas analysis (pH, glucose, lactate), bile production, histology | ATP commercial test kit (Abcam, Cambridge, UK) | Tissue ATP levels in COR20 group and COR35 group were comparable (2.56 +/− 0.32 vs. 2.44 +/−0.27 μmol/g/ dw) and higher than that in SCS control group (1.79 +/− 0.07 μmol/g/ dw). No significant differences in energetic recovery, ALT release (reduced in both test groups), histopathology and increase in bile flow were observed for both test groups. Bile production was measurable in COR35 group prior to reperfusion, compared to inconsistent bile production in COR20 group. Further studies are required to differentiate whether COR35 offers greater improvement in function, viability and IRI compared to COR20. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique | Temp, °C | Model | End points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Xu [29] | 12 | 0 or 1 | 0 or 2 | Whole blood with sterile porcine plasma, hydrocortisone, insulin, penicillin, streptomycin and heparin | 4 | NMP | 39 | Porcine, DCD livers | Tissue ATP, AST, ALT, ALP, bile production, blood gas analysis, histology | ATP Colorimetric Assay Kit (K354-100; Biovision Inc., Mountain View, CA) | After being subjected to extended WIT (1h) and CIT (2h), tissue ATP levels were restored to 80% of initial starting level in NMP group. There was improvement in hepatocyte necrosis post-NMP. The restoration of ATP and mitochondrial integrity were suggested to be the underlying reason of allograft viability and functionality in the NMP group. |
| Maida [30] | 33 | 0.5 | 6 (after SOWP) | KH buffer (with or without PGE1) with glucose, sodium, potassium, tromethamine | 0.5 | SOWP before static cold storage, (with or without PGE1 addition) | 37 | Rat, DCD livers, with DBD group as positive control | Tissue ATP, ADP, ADP:ATP ratio, AST, ALT, ICAM-1, HMGB-1, histology, malondialdehyde (MDA, measures intensity of oxidative stress), survival rate post-transplantation | High-performance liquid chromatography | This study was an orthotopic rat DCD liver transplant model which evaluated the effects of SOWP with or without the addition of PGE1 (which was shown to resuscitate mitochondrial function in previous studies) on survival and graft viability. Previous studies by the same group demonstrated that SOWP prior to cold preservation was effective in preventing warm IRI of DCD rat livers. In this study, a significant increase in ATP level (p = 0.01) and reduction in ADP/ATP ratio (p = 0.02) were detected in SOWP (+PGE1) group compared to SOWP group and SCS group. 4-week survival rate was 81% in SOWP (+PGE1) group vs. 61% (SOWP group) and 100% (DBD group, control). |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferrigno [31] | 24 | - | - | Modified Krebs-Henseleit buffer with calcium chloride, NAC | 6 | - | 10 or 20 or 30 or 37 | Rat, livers | Tissue ATP, LDH, oxygen uptake, bile production, glycogen, HIF-1a | ATPlite luminescence assay kit (Perkin Elmer Inc., Waltham, MA, United States) | Tissue ATP levels in subnormothermic group (20 °C) significantly higher than that in 30 °C group and 37 °C group (p < 0.01), and also higher than that in 10 °C group (p < 0.01). However, ATP level in 10 °C group was higher than that in the normothermic groups (30 °C and 37°C). There was no increase in HIF-1a mRNA expression (which measures tissue hypoxia) in hypothermic (10 °C) group and subnormothermic (20°C) group, compared to 30 °C group (p < 0.01) and 37 °C group. A decrease in bile flow was observed in the normothermic groups, compared to 10 °C group and 20 °C group. In accordance with previous literature, bile flow may be dependant on activity of ATP-driven pumps. Thus, a decrease in tissue ATP might reflect a decrease in bile formation and flow. MP of livers at 10 °C and 20 °C was suggested to be protective of IRI and anaerobiosis, compared to normothermic temperatures. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Schlegel [32] | 25 | 0.5 or 1 | 4 | NMP (either oxygenated diluted full blood or with a leukocyte and platelet depleted blood perfusate) with bicarbonate, prostacyclin, amoxicillin, HOPE (starch-free UW) | 4 | NMP or HOPE, grafts assessed by ex-vivo normothermic reperfusion and liver transplantation | 37 °C (NMP), 4 °C (HOPE), 4 °C (SCS) | Rat, DCD livers | Tissue ATP, oxidative damage of DNA by reactive oxygen species, HMGB-1, TLR-4, IL-6, ENA 78, NSE, ICAM-1, TNF-α, AST, histology, bile production | UV spectroscopy (340 nm) with hexokinase and glucose-6-phosphate dehydrogenase | Higher ATP levels in HOPE groups (DCD with WIT = 0.5 or 1 h) compared to NMP groups (p ≤ 0.0001). ATP levels in both MP groups were higher than control groups, but HOPE offered more protection of mitochondrial function of cells than NMP. ATP levels were consistent with and corresponded to bile flow in MP and control groups. HOPE might be superior to NMP in a clinically relevant model in terms of protection of hepatocyte and non-parenchymal injury and survival rates in livers treated with WIT (0.5 h) [90%; 9/10 vs. 70%; 7/10] and in livers treated with WIT (1 h) [63%; 5/8 vs. 0%; 0/10]. |
| Boteon [17] | 10 | - | ~8 | NMP (Hemopure complemented with human albumin solution and other supplements), HOPE (UW) | 6 | NMP only vs. combined HMP (2 h) + NMP (4 h) | 37 °C (NMP), 10 °C (HOPE) | Human, discarded livers (DBD and DCD) | Tissue ATP, pH, pO2, pCO2, O2 saturation, lactate level, bile production, histology, oxidative injury (uncoupling protein 2, 4-hydroxynonenal), tissue inflammation (CD14, CD11b, VCAM-1) | ATP Bioluminescent Assay kit (FLAA, Sigma-Aldrich Inc., St. Louis, MO) | For the HMP+NMP group, a median 1.8 fold increase in tissue ATP with a gradual decline in oxygen uptake were reported during the HOPE phase. Comparable end-perfusion tissue ATP levels were reported in viable grafts of HMP+NMP group vs. NMP group. A significant difference in changes in ATP was noted between viable and non-viable NMP livers (2.5 vs. 1.1 fold, p = 0.05). The combined approach of HOPE and NMP perfusion may be more effective in promoting recovery of mitochondrial function (HOPE phase) and allowing viability assessment (NMP phase) than NMP alone. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End Points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Buchs [44] | 7 | 0 or 0.5 | 0 or 4 or 8 or 18 | KPS-1 with glucose, mannitol, glutathione (reduced form), CaCl2, NaOH, KH2PO4 | 8 or 8 & 18 | HMP | 2–4 | Porcine, DCD | Tissue ATP, precursors (PME, NAD) after SCS or after 8 or 18 h of machine perfusion | 31P NMR spectroscopy | HOPE appears to be effective in supporting ATP resynthesis in kidneys subjected to WIT, but is less effective in kidneys subjected to SCS. Immediate HOPE perfusion should be used after organ retrieval to maintain organ viability. |
| Kay [46] | 18 | Minimal (6.4 +/− 1.0 min) | 2 | AQIX or HOC with sodium, potassium, mannitol, citrate or UW with adenosine | 6 | NMP vs. HMP (control: SCS), ex vivo function testing by perfusion (37 °C) with autologous blood | 30 °C (AQIX), 4 °C (HOC), 4 °C (UW) | Porcine, kidneys | Tissue ADP:ATP ratio (ATP and ADP), perfusate flow rate, histology, serum creatinine, creatinine clearance, urine output | Bioluminescence adenylate nucleotide ratio assay kit (Cambrex BioScience, Berkshire, UK) | Pre-perfusion ADP:ATP ratios were high, demonstrating effects of reduction in cell metabolism due to cold storage. Decrease in ADP:ATP ratios was reported in all NMP (with AQIX), HMP (with HOC) and SCS (with UW) groups, with comparable ADP:ATP ratios amongst the three groups. |
| Lazeyras [45] | 10 | - | 10 (only 1 graft was subjected to cold storage) | KPS-1 with insulin, phosphate, HES | 8 | HMP | 4 | Porcine, DCD | Tissue ATP (n = 9 under O2 + HPP, n = 1 mimics cold-ischaemia injured kidney which is perfused, cold stored and reperfused), PME, NAD(H) | 31P MR spectroscopy and 31P CSI | The combined methods enabled detection of ATP in grafts perfused under 100 kPa pO2. In the CI-injured kidney model (n = 1), ATP levels were detected in after initial perfusion, but not detected after 10 h of SCS. Upon reperfusion, ATP was detected again, reaching close to pre-ischaemic level. The ATP level is one of the important markers for cell and graft viability and this technique could be transferable to clinical evaluation of marginal donor kidneys. |
| Ravaioli [47] | 20 | - | >=20 | Celsior with glutathione, NaOH, mannitol, low K+ | 3 | PE-HMP vs. PE-O2 vs. PE | 4 | Human, discarded kidneys (DBD) | Tissue ATP, histology, pH, lactate, pO2, pCO2, RNA (HIF-1α, eNOS, β-actin, β-2microglobulin) | ATP determination kit (Cat. N A22066, Thermo Fisher, Waltham, MA, USA) | HMP (hyperbaric or normobaric) was superior to conventional SCS or unoxygenated MP in the net increase in graft tissue ATP with respect to baseline level. Limitations of study include the lack of a transplantation model post-MP for assessment of graft function and survival. |
| Kaminski [48] | 15 | 1 | - | KPS-1 | 20 | HMP | 8.2+/−1.0 | Porcine, WIT- injured grafts | Cortical tissue ATP, histology, oxygen arterio-venous difference | ATP Bioluminescent Assay kit (Sigma) | Renal cortical ATP was restored in HMP-treated warm-ischaemia injured kidney grafts to control (non-ischaemic) group (3.3 mmol/L tissue). Tissue ATP in HMP group was significant higher than that in SCS group (5.8 vs. 0.06 mmol/L, p < 0.01). Measurement of tissue oxygen and tissue ATP could be added to the current restricted panel of clinical evaluation criteria of grafts. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Leemkuil [57] | 20 | 18 (DCD only) | ~10 | UW | 6 | HMP | 4 to 7 | Human, discarded pancreata (n = 10 DBD and n = 10 DCD) | Tissue ATP, tissue edema (wet to dry weight ratio), TBARS, amylase, lipase, LDH, islet isolation procedure, perfusion flow | ATP Bioluminescence assay kit CLS II (Roche Diagnostics GmbH, Boehringer Mannheim, Germany) | HMP preservation of DBD and DCD pancreata was associated with a 6.8 fold increase and 2.6 fold increase in ATP concentration respectively, with viable islets isolated from 2 samples and no reported edema formation and indications of tissue injury. This first report of dual arterial HOPE for human donor pancreas suggested that HOPE may help to improve graft viability. |
| Study | N | WIT, h | CIT, h | Perfusate | Perfusion Time, h | Perfusion Technique * | Temp, °C | Model | End points | ATP Measurement Technique | Study Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kumar [59] | 13 | Minimal (4 to 5 min) | ~2 | Soltran kidney perfusion fluid with potassium citrate, sodium citrate, mannitol, magnesium sulphate | 3 h (control, ‘high pressure grafts’, 50 mmHg) or 4 h (test, ‘low pressure’ grafts, 20 mmHg) | NMP | 37 | Porcine, DCD pancreata | ATP Synthetase Complex V activity, blood gas analysis, standard electrolytes, glucose, amylase, insulin, Caspase 3, M30 CytoDEATH | Immunohistochemical staining of biopsied grafts (note activity of ATP synthetase was graded: Grade I (best), >95% of slide section staining positive for target enzyme), Grade II (>90 but ≤95%), Grade III (>85 but ≤90%) | ATP Synthetase Complex V is one of the enzymes essential for ATP production and metabolic functions, such as insulin secretion (ATP-dependent beta islets of Langerhans signalling pathways) and this is one of the markers for graft viability. In this ex vivo porcine pancreas perfusion model, a significant reduction in amylase and increase in ATP Synthetase activity were reported in ‘low pressure’ test group vs ‘high pressure’ control group (p < 0.016). This physiological EVNPPP model may be useful for the study of whole pancreas preservation. |
| Perfusion Technique | Organ | Study |
|---|---|---|
| HMP | Kidneys | Buchs (porcine) [44] Lazeyras (porcine) [45] Ravaioli (human, discarded kidneys) [47] Kaminski (porcine) [48] |
| Liver | Westerkamp (human, discarded livers) [21] | |
| Pancreas | Leemkuil (human, discarded pancreas) [57] | |
| Combined HMP+NMP | Liver | Boteon (human, discarded livers) [17] |
| HMP vs. NMP | Liver | Schlegel (rat) [32] |
| HMP vs. NMP | Kidneys | Kay (porcine) [46] |
| SNMP | Liver | Ferrigno (rat) [22] Berendsen (rat) [23] Bruinsma (rat) [24] Bruinsma (human, discarded livers) [25] Bruinsma (human, discarded livers) [26] Okamura (rat) [39] Ferrigno (rat) [27] |
| COR (controlled oxygenated rewarming) | Liver | Minor (porcine) [18] von Horn (rat) [28] |
| NMP | Liver | Xu (porcine) [29] Maida (rat) [30] |
| NMP | Pancreas | Kumar (porcine) [59] |
| SCS vs. HMP vs. SNMP vs. NMP | Liver | Ferrigno (rat) [31] |
| Temp/°C | Increase in Liver Tissue ATP Levels Post-MP vs. pre-MP Perfusion | Study Type |
|---|---|---|
| 10–12 | Westerkamp [21] | Human, DCD, DBD |
| 20 | Ferrigno [22] | Rat, DCD |
| Berendsen [23] | Rat, DCD | |
| Bruinsma [24] | Rat | |
| Minor (COR20) [18] | Porcine | |
| Bruinsma [25] | Human, DBD, DCD | |
| Ferrigno (20 > 10 > 30 > 37 °C) [24] | Rat | |
| Bruinsma (DBD/DCD/ steatotic livers) [25] | Human | |
| von Horn (COR 20 °C > COR 35 °C) [28] | Rat, DCD | |
| Okamura [39] | Rat, steatotic livers | |
| Ferrigno [27] | Rat, DCD, steatotic livers | |
| 37 | Schlegel [32] (Higher vs. SCS, but HOPE > NMP) **Study compares HOPE (4 °C) to NMP (37 °C) & SCS | Rat, DCD |
| Maida [30] (short oxygenated rewarming prior to SCS) | Rat, DCD | |
| 39 | Xu [29] | Porcine, DCD |
| Combined HMP (4 °C) & NMP (37 °C) | Boteon [17] | Human, DBD, DCD |
| Temp/°C | Increase in Renal Tissue ATP Levels Post-MP vs. Pre-MP Perfusion | Study Type |
|---|---|---|
| 4 | Buchs [44] | Porcine, DCD |
| Lazeyras [45] | Porcine, DCD | |
| Ravaioli [47] | Human, DBD | |
| 8 | Kaminski [48] | Porcine |
| HOPE (4 °C) vs. NMP (30 °C) | Kay [46] (*comparable ATP in HOPE, NMP and SCS groups) | Porcine, WIT-injured |
| Temp/ °C | Increase in Pancreatic Tissue ATP Levels Post-MP vs. Pre-MP Perfusion | Study Type |
|---|---|---|
| 4–7 | Leemkuil [57] | Human (DBD, DCD) |
| 37 | Kumar [59] | Porcine DCD |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, M.I.; Yiu, J.; Nozdrin, M.; Papalois, V. The Effect of Preservation Temperature on Liver, Kidney, and Pancreas Tissue ATP in Animal and Preclinical Human Models. J. Clin. Med. 2019, 8, 1421. https://doi.org/10.3390/jcm8091421
Bellini MI, Yiu J, Nozdrin M, Papalois V. The Effect of Preservation Temperature on Liver, Kidney, and Pancreas Tissue ATP in Animal and Preclinical Human Models. Journal of Clinical Medicine. 2019; 8(9):1421. https://doi.org/10.3390/jcm8091421
Chicago/Turabian StyleBellini, Maria Irene, Janice Yiu, Mikhail Nozdrin, and Vassilios Papalois. 2019. "The Effect of Preservation Temperature on Liver, Kidney, and Pancreas Tissue ATP in Animal and Preclinical Human Models" Journal of Clinical Medicine 8, no. 9: 1421. https://doi.org/10.3390/jcm8091421
APA StyleBellini, M. I., Yiu, J., Nozdrin, M., & Papalois, V. (2019). The Effect of Preservation Temperature on Liver, Kidney, and Pancreas Tissue ATP in Animal and Preclinical Human Models. Journal of Clinical Medicine, 8(9), 1421. https://doi.org/10.3390/jcm8091421