

Low-Dose Ionizing Radiation and Thyroid Diseases and Functional Modifications in Exposed Workers: A Systematic Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
3. Results
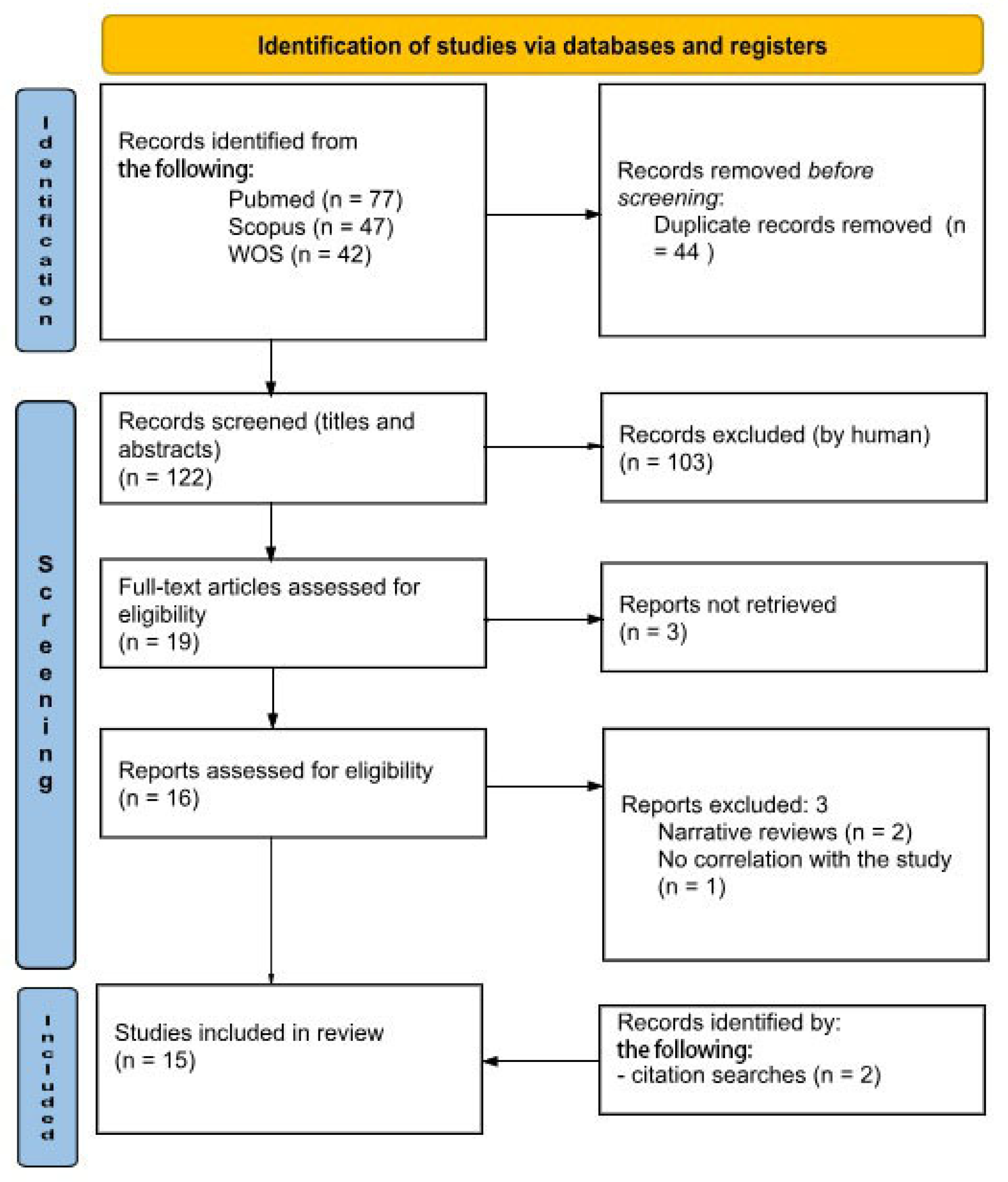
3.1. Search Results Summary
3.2. Characteristics of Included Studies
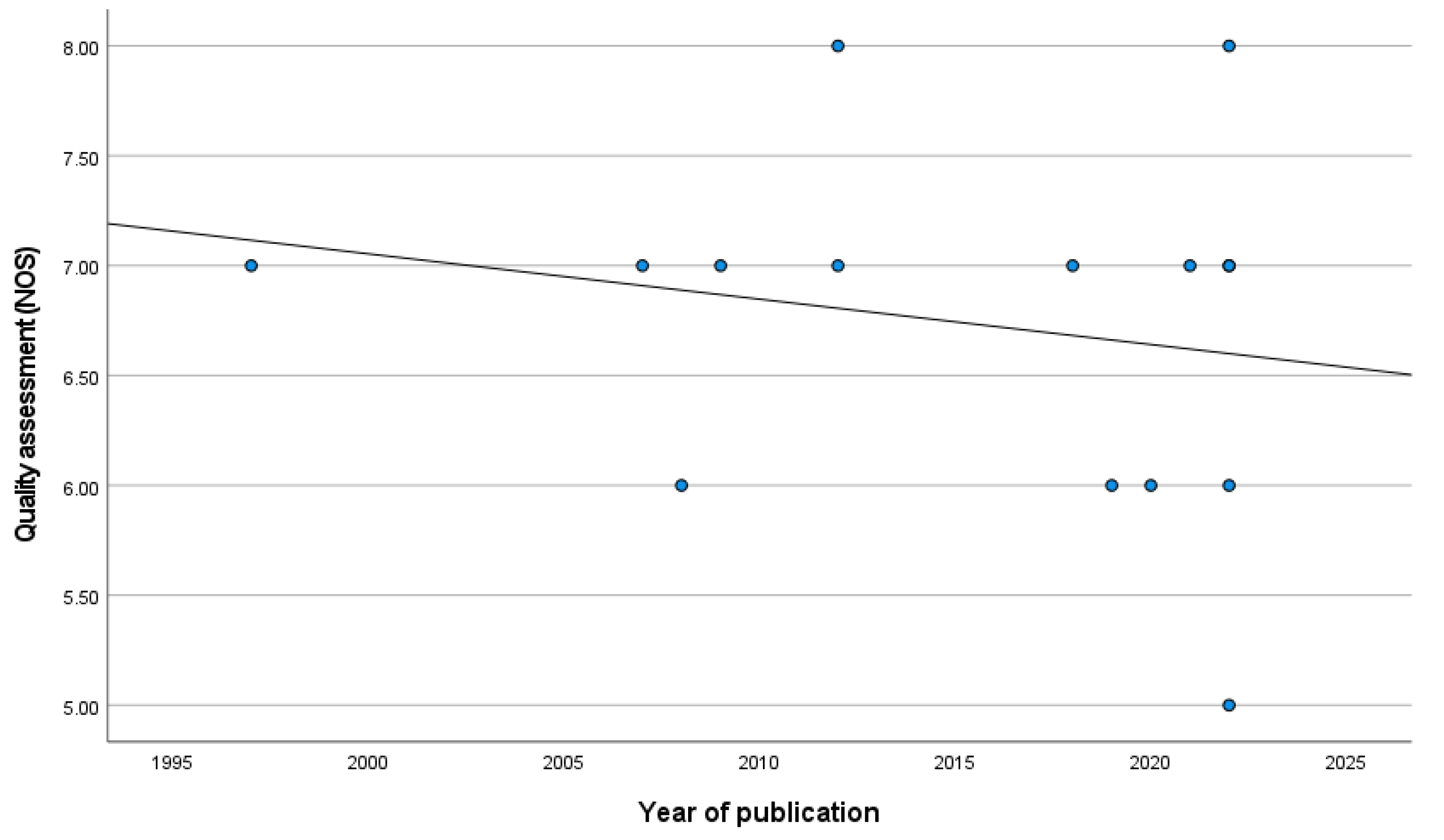
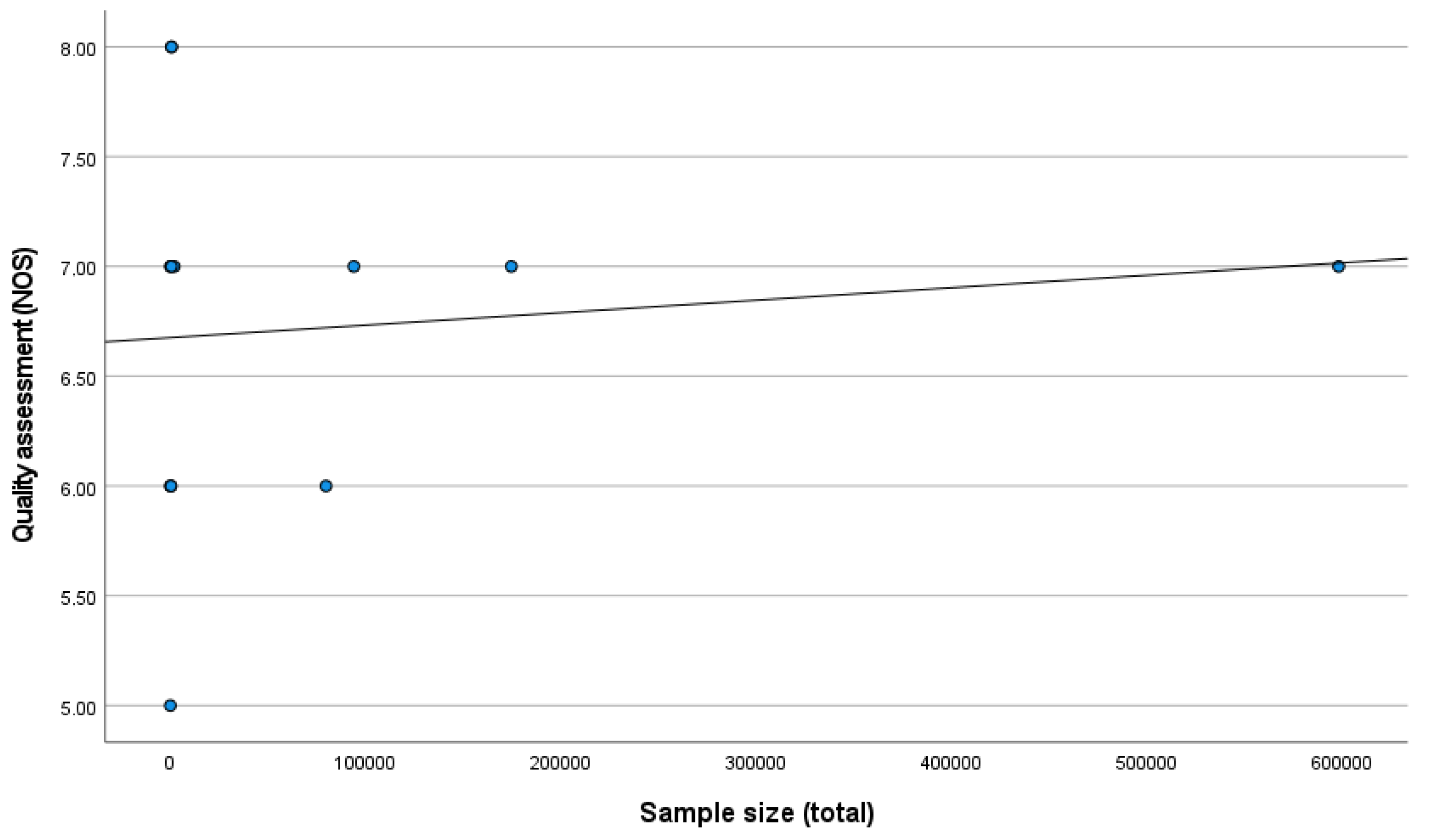
3.3. Quality Assessment
3.4. Thyroid Cancer
3.5. Thyroid Nodules
3.6. Thyroid Hormones
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Zhang, Y.; Rohde, L.H.; Emami, K.; Hammond, D.; Casey, R.; Mehta, S.K.; Jeevarajan, A.S.; Pierson, D.L.; Wu, H. Suppressed expression of non-DSB repair genes inhibits gammaradiation-induced cytogenetic repair and cell cycle arrest. DNA Repair 2008, 7, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- AIRC-Radiazioni Ionizzanti e Cancro. Available online: https://www.airc.it/cancro/informazioni-tumori/cose-il-cancro/radiazioni-ionizzanti-cancro#:~:text=Le%20radiazioni%20ionizzanti%20possono%20danneggiare,allo%20sviluppo%20di%20un%20tumore.&text=Le%20radiazioni%20ionizzanti%20sono%20un,per%20l'insorgenza%20del%20cancro (accessed on 13 July 2024).
- Feinendegen, L.E.; Brooks, A.L.; Morgan, W.F. Biological consequences and health risks of low-level exposure to ionizing radiation: Commentary on the workshop. Health Phys. 2011, 100, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.D. Excerpts of UNSCEAR white paper on “evaluation of data on thyroid cancer in regions affected by the Chernobyl accident”. Radiat. Prot. Environ. 2018, 41, 160. [Google Scholar] [CrossRef]
- Lubin, J.H.; Adams, M.J.; Shore, R.; Holmberg, E.; Schneider, A.B.; Hawkins, M.M.; Robison, L.L.; Inskip, P.D.; Lundell, M.; Johansson, R.; et al. Thyroid Cancer Following Childhood Low-Dose Radiation Exposure: A Pooled Analysis of Nine Cohorts. J. Clin. Endocrinol. Metab. 2017, 102, 2575–2583. [Google Scholar] [CrossRef]
- Hamra, G.B.; Richardson, D.B.; Cardis, E.; Daniels, R.D.; Gillies, M.; O’Hagan, J.A.; Haylock, R.; Laurier, D.; Leuraud, K.; Moissonnier, M.; et al. Cohort Profile: The International Nuclear Workers Study (INWORKS). Int. J. Epidemiol. 2016, 45, 693–699. [Google Scholar] [CrossRef]
- Richardson, D.B.; Leuraud, K.; Laurier, D.; Gillies, M.; Haylock, R.; Kelly-Reif, K.; Bertke, S.; Daniels, R.D.; Thierry-Chef, I.; Moissonnier, M.; et al. Cancer mortality after low dose exposure to ionising radiation in workers in France, the United Kingdom, and the United States (INWORKS): Cohort study. Br. Med. J. 2023, 382, e074520. [Google Scholar] [CrossRef]
- National Research Council. Committee on the Biological Effects of Ionizing Radiation. In Health Risks from Exposure to Low Levels of Ionizing Radiation. BEIR: VII Report, Phase 2; The National Academic Press: Washington, DC, USA, 2006. [Google Scholar]
- Dipartimento Della Protezione Civile, Presidenza del Consiglio dei Ministri-Decreto Legislativo n.101 del 31 Luglio 2020. Available online: https://www.protezionecivile.gov.it/it/normativa/decreto-legislativo-n101-del-31-luglio-2020-0/ (accessed on 13 July 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar]
- Vázquez Rivas, F.; Mahillo, I.; Valverde, J.; Garayoa, J.; Teresa Del Campo, M. Radiaciones ionizantes en trabajadores sanitarios: Función tiroidea y niveles de riesgo de exposición laboral [Ionizing radiation in healthcare workers: Thyroid function and risk levels of occupational exposure]. Rev. Asoc. Esp. Espec. Med. Trab. 2022, 31, 29–40. [Google Scholar]
- El-Benhawy, S.A.; Fahmy, E.I.; Mahdy, S.M.; Khedr, G.H.; Sarhan, A.S.; Nafady, M.H.; Yousef Selim, Y.A.; Salem, T.M.; Abu-Samra, N.; El Khadry, H.A. Assessment of thyroid gland hormones and ultrasonographic abnormalities in medical staff occupationally exposed to ionizing radiation. BMC Endocr. Disord. 2022, 22, 287. [Google Scholar] [CrossRef]
- Cioffi, D.L.; Fontana, L.; Leso, V.; Dolce, P.; Vitale, R.; Vetrani, I.; Galdi, A.; Iavicoli, I. Low dose ionizing radiation exposure and risk of thyroid functional alterations in healthcare workers. Eur. J. Radiol. 2022, 132, 109279. [Google Scholar] [CrossRef]
- Adibi, A.; Rezazade, A.; Hovsepian, S.; Koohi, R.; Hosseini, M. The relationship between occupational radiation exposure and thyroid nodules. J. Res. Med. Sci. 2012, 17, 434–438. [Google Scholar] [PubMed]
- Gudzenko, N.; Mabuchi, K.; Brenner, A.V.; Little, M.P.; Hatch, M.; Drozdovitch, V.; Vij, V.; Chumak, V.; Bakhanova, E.; Trotsyuk, N.; et al. Risk of thyroid cancer in Ukrainian cleanup workers following the Chornobyl accident. Eur. J. Epidemiol. 2022, 37, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.S.; Park, R.M.; Koh, D.H. Cancer admission and mortality in workers exposed to ionizing radiation in Korea. J. Occup. Environ. Med. 2008, 50, 791–803. [Google Scholar] [CrossRef]
- Inskip, P.D.; Hartshorne, M.F.; Tekkel, M.; Rahu, M.; Veidebaum, T.; Auvinen, A.; Crooks, L.A.; Littlefield, L.G.; McFee, A.F.; Salomaa, S.; et al. Thyroid nodularity and cancer among Chernobyl cleanup workers from Estonia. Radiat. Res. 1997, 147, 225–235. [Google Scholar] [CrossRef]
- Muirhead, C.R.; O’Hagan, J.A.; Haylock, R.G.E.; Phillipson, M.A.; Willcock, T.; Berridge, G.L.C.; Zhang, W. Mortality and cancer incidence following occupational radiation exposure: Third analysis of the National Registry for Radiation Workers. Br. J. Cancer 2009, 100, 206–212. [Google Scholar] [CrossRef]
- Kesminiene, A.; Evrard, A.S.; Ivanov, V.K.; Malakhova, I.V.; Kurtinaitise, J.; Stengrevics, A.; Tekkel, M.; Chekin, S.; Drozdovitch, V.; Gavrilin, Y.; et al. Risk of thyroid cancer among chernobyl liquidators. Radiat. Res. 2012, 178, 425–436. [Google Scholar] [CrossRef]
- Duque, C.S.; Vélez, A.; Cuartas, J.; Jaimes, F.; Dueñas, J.P.; Agudelo, M.; Nikiforova, M.N.; Nikiforov, Y.E.; Condello, V. Molecular profiling of papillary thyroid carcinomas in healthcare workers exposed to low dose radiation at the workplace. Endocrine 2022, 76, 95–100. [Google Scholar] [CrossRef]
- Sernia, S.; Bongiovanni, A.; De Giorgi, A.; De Sio, S.; Cafolla, A.; La Torre, G. Thyroid parameters variations in healthcare workers and students exposed to low-dose ionizing radiations. G. Ital. Med. Lav. Ergon. 2022, 44, 338–346. [Google Scholar]
- Wong, Y.S.; Cheng, Y.Y.; Cheng, T.J.; Huang, C.C.; Yeh, J.J.; Guo, H.R. The Relationship Between Occupational Exposure to Low-dose Ionizing Radiation and Changes in Thyroid Hormones in Hospital Workers. Epidemiology 2019, 30, S32–S38. [Google Scholar] [CrossRef]
- Lee, W.J.; Ko, S.; Bang, Y.J.; Choe, S.A.; Choi, Y.; Preston, D.L. Occupational radiation exposure and cancer incidence in a cohort of diagnostic medical radiation workers in South Korea. Occup. Environ. Med. 2021, 78, 876–883. [Google Scholar] [CrossRef]
- Kitahara, C.M.; Preston, D.L.; Neta, G.; Little, M.P.; Doody, M.M.; Simon, S.L.; Sigurdson, A.J.; Alexander, B.H.; Linet, M.S. Occupational radiation exposure and thyroid cancer incidence in a cohort of U.S. radiologic technologists, 1983–2013. Int. J. Cancer 2018, 143, 2145–2149. [Google Scholar] [CrossRef] [PubMed]
- Cardis, E.; Vrijheid, M.; Blettner, M.; Gilbert, E.; Hakama, M.; Hill, C.; Howe, G.; Kaldor, J.; Muirhead, C.R.; Schubauer-Berigan, M.; et al. The 15-Country Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry: Estimates of radiation-related cancer risks. Radiat. Res. 2007, 167, 396–416. [Google Scholar] [CrossRef] [PubMed]
- Modan, B. Low-dose radiation carcinogenesis. Eur. J. Cancer 1992, 28 Pt A, 1010–1012. [Google Scholar] [CrossRef]
- McLean, A.R.; Adlen, E.K.; Cardis, E.; Elliott, A.; Goodhead, D.T.; Harms-Ringdahl, M.; Hendry, J.H.; Hoskin, P.; Jeggo, P.A.; Mackay, D.J.C.; et al. A restatement of the natural science evidence base concerning the health effects of low-level ionizing radiation. Proc. Biol. Sci. 2017, 284, 20171070. [Google Scholar] [CrossRef] [PubMed]
- Krátký, J.; Vítková, H.; Bartáková, J.; Telička, Z.; Antošová, M.; Límanová, Z.; Jiskra, J. Thyroid nodules: Pathophysiological insight on oncogenesis and novel diagnostic techniques. Physiol. Res. 2014, 63 (Suppl. S2), S263–S275. [Google Scholar] [CrossRef]
- Rabinovich, E.I.; Povolotskaya, S.V.; Degteva, M.O.; Tolstykh, E.I. Relation between the thyroid diseases prevalence and doses of radiation exposure in the individuals relocated from radioactively contaminated areas in South Urals. Radiatsionnaya Gygiena 2022, 15, 36–46. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, S.; Guo, W.; Li, M.; Mai, W.; Zhang, L.; Jia, Y.; Yang, Y.; Chen, H.; Huang, W. Thyroid abnormalities and influencing factors in medical radiology workers in Guangdong Province. J. Environ. Occup. Med. 2023, 40, 323–330. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| 1st Author | Country | Study Design | Type of Workplace | Sample Size | Thyroid Cancer | Thyroid Nodules | TSH, fT3, fT4 Variations | Main Results | Quality Assessment (NOS) |
|---|---|---|---|---|---|---|---|---|---|
| Ahn Y, 2008 [16] | South Korea | Cohort | Universities and academia, hospitals and healthcare, nuclear power plants, industrial services, war industry and barracks, and public services | 79,679 | X | - | - | Thyroid cancer was statistically significantly elevated in female radiation workers in medical (SRR = 2.90, 95% CI = 1.05–7.94) and research institutions (SRR = 3.91, 95% CI = 1.36–11.0) and industry (SRR = 5.07, 95% CI = 1.56–15.6) and in all nuclear power workers (SRR = 2.59, 95% CI = 1.33–5.13), and there was a significant association with dose (ERR = 20.4 per Sv, 90% CI = 8 to 60, one-tailed p = 0.049). | 6 |
| El-Benhawy SA, 2022 [12] | Egypt | Case–control | Hospitals and healthcare | 120 | - | X | X | Participants from the group exposed to radioiodine 131I had significantly higher fT3 mean values than participants from the group of non-exposed healthy professionals (3.01 ± 0.41 vs. 2.76 ± 0.38, p = 0.047 *). Regarding anti-TPO, their mean values were substantially higher in participants from group I than in participants from group III (35.61 ± 82.35 vs. 8.40 ± 1.26, p < 0.001 *, respectively). The mean thyroid volume (ml) was significantly larger in participants from group I, in comparison to participants from group III (10.32 ± 3.42 vs. 4.62 ± 1.13, p < 0.001 *). The thyroid nodule percentage in group I was significantly higher than in the control group (p = 0.005 *). | 7 |
| Vazquez Rivas F, 2022 [11] | Spain | Case–control | Hospitals and healthcare | 186 | - | - | X | No statistically significant relationship was found between the levels of thyroid hormones and the occupational exposure to radiation in PER A and PER B, though higher levels of TSH were found in the exposed groups PER B (2.6 ± 1.4) and PER A (2.7 ± 1.3) compared to the TSH levels in the control group (2.4 ± 1.5). | 7 |
| Cioffi DL, 2020 [13] | Italy | Case–control | Hospitals and healthcare | 180 | - | - | X | Exposed workers presented significantly higher levels of TSH (β = 0.88, %95CI [0.43, 1.33], p = 0.001) and significantly lower levels of fT3 (β = −0.61, %95CI [−0.74, −0.47], p < 0.001) and fT4 (β = −0.10, %95CI [−0.16, −0.04], p = 0.001) than non-exposed workers. | 6 |
| Duque C S, 2022 [20] | USA | Cohort | Hospitals and healthcare | 9 | X | - | - | Nine healthcare workers with papillary thyroid carcinoma exposed to LDIR. The molecular analysis of surgical samples of PTCs was informative and revealed genetic alterations in five patients. BRAF V600E was found in four (67%) cases, whereas RET/PTC1 fusion was found in one (17%), and one sample (17%) was wild-type for point mutations and fusions. | 5 |
| Sernia S, 2022 [21] | Italy | Cohort | Universities and academia and hospitals and healthcare | 121 | - | - | X | Data showed no variation in TSH levels related to occupational exposure, an increase in fT3 hormone values in HCW and residents, and a decrease in fT4 in HCW (these results are in conflict with previous studies, in which both free hormones decreased with a concomitant increase in TSH). | 6 |
| Wong YS, 2019 [22] | Taiwan | Cohort | Hospitals and healthcare | 326 | - | - | X | We observed declines in fT3 and fT4 over the study period but not in TSH. In addition, we found negative dose–response relationships between exposure duration and declines in the serum levels of fT3 (a change of −0.037 ng/mL/year after adjusting for sex and age at the beginning of follow-up; 95%CI = −0.042, −0.032 ng/mL/year) and fT4 (−0.115 μg/dL/year; 95%CI = −0.140, −0.091 μg/dL/year). We also observed an increase in the TSH level (0.683 μIU/mL/year; 95% CI = 0.151, 1.214 μIU/mL/year) after the ninth year of follow-up. | 6 |
| Adibi A, 2012 [14] | Iran | Case–control | Hospitals and healthcare | 595 | - | X | - | The prevalence of thyroid nodules in the case and control groups was 22.6% and 24.6%, respectively (p > 0.05). Although thyroid nodules were significantly more prevalent in females in the control group, no such difference was observed between females and males in the case group (p > 0.05). The number of thyroid nodules (single or multiple) and calcifications was not different between the two groups (p > 0.05). In addition, the hypoechogenicity of thyroid nodules was not different between the two groups (p > 0.05). | 8 |
| Inskip PD, 1997 [17] | USA | Cohort | Nuclear power plants | 1984 | - | X | - | The presence of nodules was not significantly associated with the documented radiation dose from external sources [p(1) = 0.70; Excess RR (ERR) = −0.01/cGy; 95% CI: −0.02, 0.01]. Among men with nodules, the mean dose was 10.2 cGy, and for those without nodules, the mean was 10.9 cGy. The mean for the total population was 10.8 cGy, and the maximum recorded dose for any worker was 61 cGy. | 7 |
| Lee WJ, 2021 [23] | South Korea | Cohort | Hospitals and healthcare | 93,920 | X | - | - | The risk of thyroid cancer from workers’ exposure to low-dose ionizing radiation appears to be increased for men and women compared with the general population. In particular, there appears to be an inversely proportional correlation according to cumulative badge dose categories (half of all cases have thyroid cancer for doses <1 mSv). | 7 |
| Kitahara CM, 2018 [24] | USA | Cohort | Hospitals and healthcare | 89,897 | X | - | - | Thyroid cancer risk was not associated with cumulative, occupational ionizing radiation dose to the thyroid gland in fully adjusted models (ERR/100 mGy = −0.05, 95% CI < −0.10, 0.34). Restricting to papillary thyroid cancer (303 cases) yielded nearly identical results (ERR/100 mGy = −0.05, 95% CI < 0.10, 0.39). | 7 |
| Muirhead CR, 2009 [18] | United Kingdom | Cohort | Nuclear power plants, industrial services, and war industry and barracks | 174,541 | X | - | - | Both NRRW−2 and NRRW-3 found a non-statistically significantly raised SMR for thyroid cancer but no association between mortality and dose. As thyroid cancers are usually not fatal, the incidence data should be more informative. Although there was weak evidence of a trend with external dose in thyroid cancer incidence (one-sided P ¼ 0.079), this was driven primarily by two cases with a cumulative dose above 400 mSv. | 7 |
| Cardis S, 2007 [25] | France | Cohort | Nuclear power plants, industrial services, and war industry and barracks | 598,068 | - | - | - | All workers who died of thyroid problems were exposed to doses below 50. The Standardized Mortality Ratio (SMR) appears to be maximum for a cumulative dose of 10 mSv (RR at 100 mSv: 0.91 (0.12, 2.84)). | 7 |
| Gudzenko N, 2022 [15] | Ukraine | Case–control | Nuclear power plants | 607 | x | - | - | Total thyroid dose was associated with nonsignificantly increased risk of thyroid cancer, with some evidence that the magnitude of radiation risk varied with time since exposure. Although category-specific risk estimates were not significant, the OR was highest among the highest dose categories. There was also a nonsignificant elevation in risk for FTC based on a small number of cases. | 8 |
| Kesminiene A, 2012 [19] | France | Case–control | Nuclear power plants | 530 | x | - | - | Most subjects received low doses (median 69 mGy). A statistically significant dose–response relationship was found with total thyroid dose. The Excess Relative Risk (ERR) per 100 mGy was 0.38 [95% confidence interval (CI): 0.10, 1.09]. A significant dose–response relationship was observed between radiation dose to the thyroid received in adulthood and the risk of subsequent thyroid cancer, with a significantly increased risk at doses of 300 mGy or above. | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colaprico, C.; Lomartire, F.; Raccio, I.; Mantione, G.; Ammirati, S.; La Torre, G. Low-Dose Ionizing Radiation and Thyroid Diseases and Functional Modifications in Exposed Workers: A Systematic Review. J. Clin. Med. 2025, 14, 588. https://doi.org/10.3390/jcm14020588
Colaprico C, Lomartire F, Raccio I, Mantione G, Ammirati S, La Torre G. Low-Dose Ionizing Radiation and Thyroid Diseases and Functional Modifications in Exposed Workers: A Systematic Review. Journal of Clinical Medicine. 2025; 14(2):588. https://doi.org/10.3390/jcm14020588
Chicago/Turabian StyleColaprico, Corrado, Francesca Lomartire, Ivana Raccio, Giorgia Mantione, Salvatore Ammirati, and Giuseppe La Torre. 2025. "Low-Dose Ionizing Radiation and Thyroid Diseases and Functional Modifications in Exposed Workers: A Systematic Review" Journal of Clinical Medicine 14, no. 2: 588. https://doi.org/10.3390/jcm14020588
APA StyleColaprico, C., Lomartire, F., Raccio, I., Mantione, G., Ammirati, S., & La Torre, G. (2025). Low-Dose Ionizing Radiation and Thyroid Diseases and Functional Modifications in Exposed Workers: A Systematic Review. Journal of Clinical Medicine, 14(2), 588. https://doi.org/10.3390/jcm14020588