
Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study
 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility Criteria
2.2. Anesthetic Management
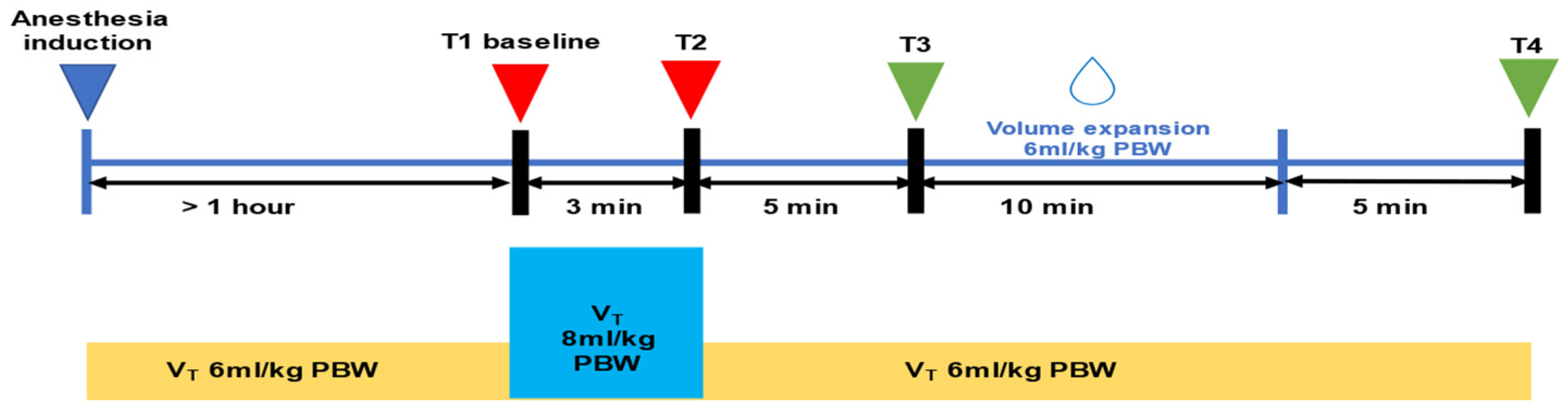
2.3. Study Protocol
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Effects of VtC and VE on Hemodynamic and Respiratory Variables
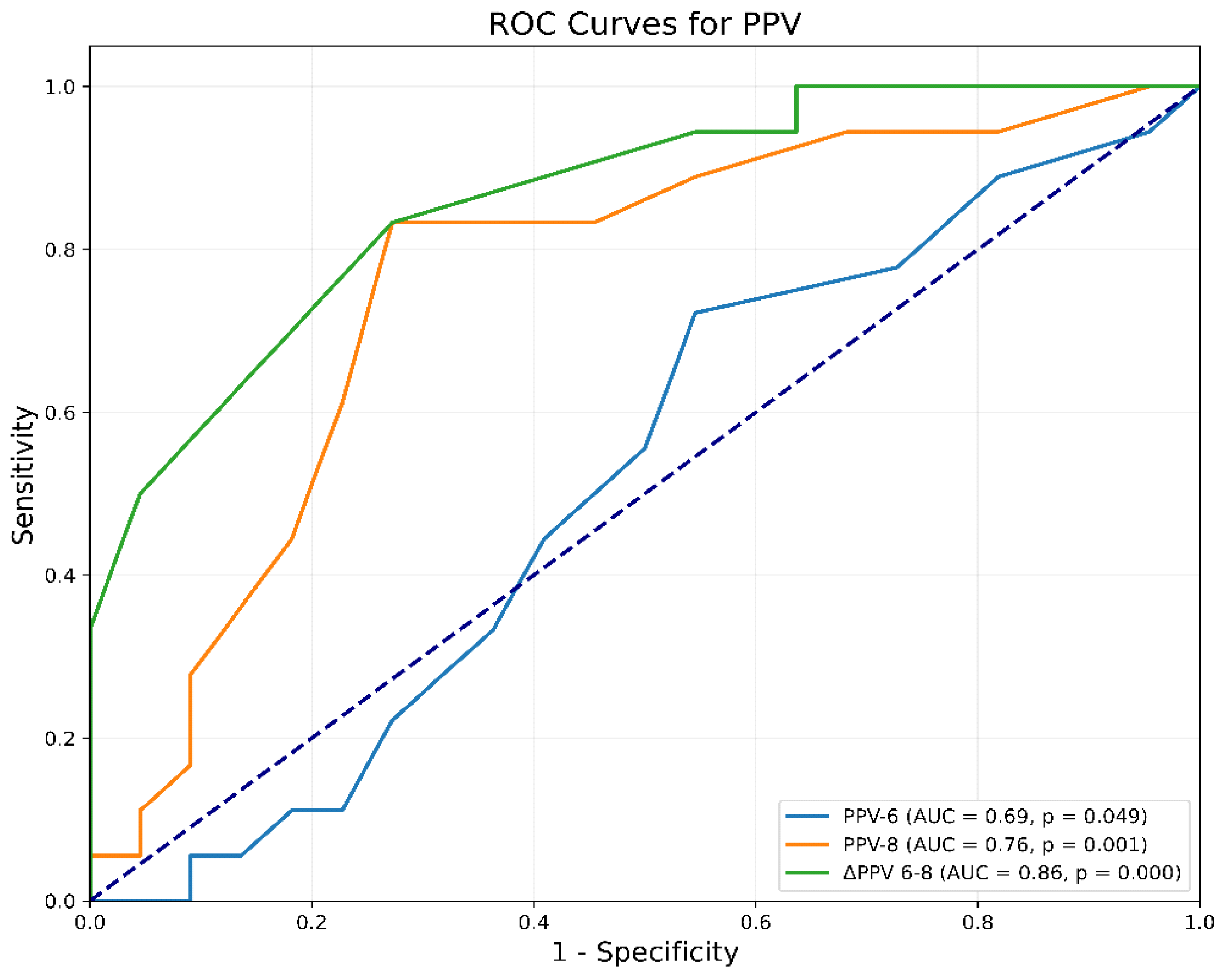
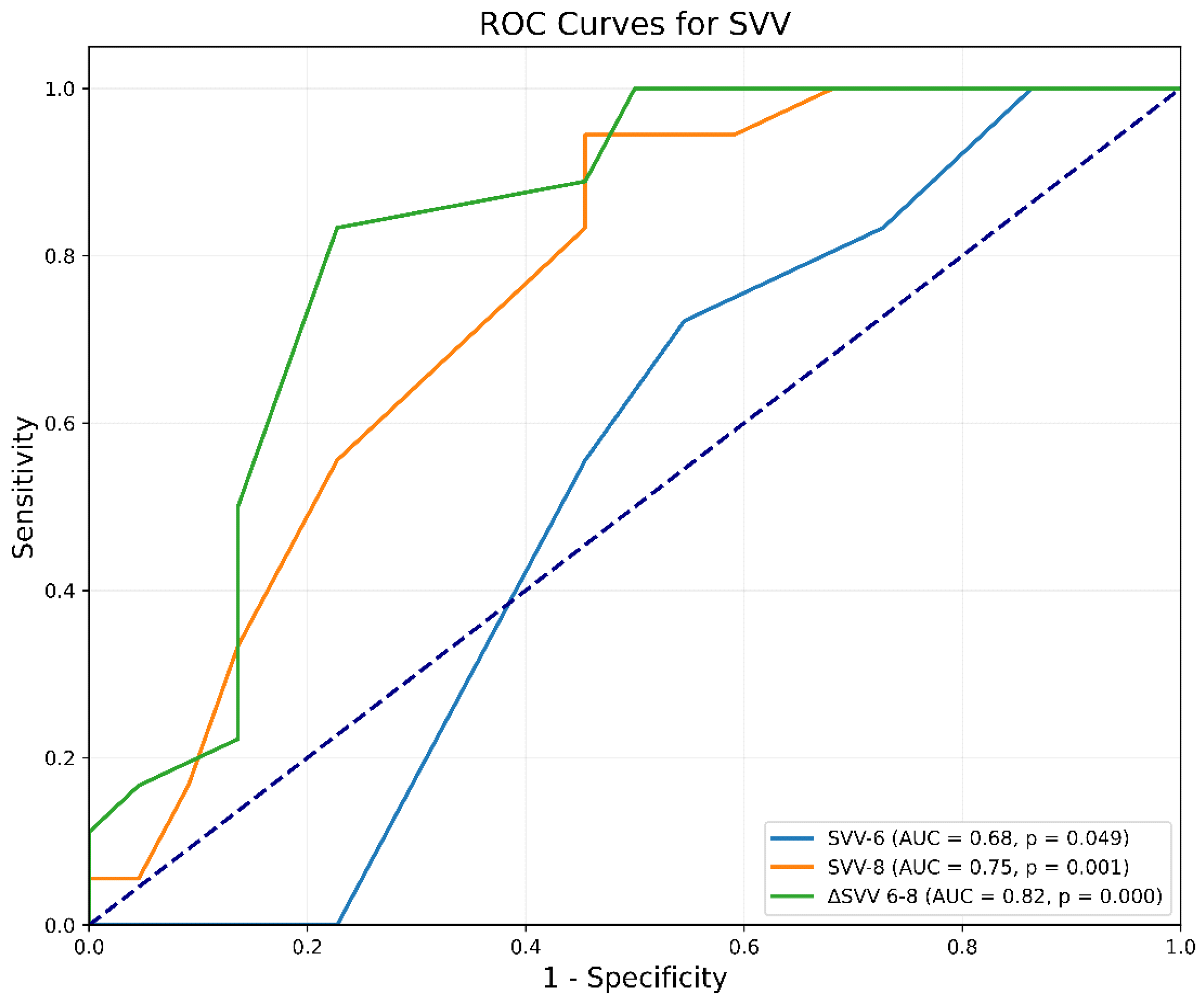
3.3. Prediction of Fluid Responsiveness
3.4. Gray-Zone Approach for ΔPPV(6–8) and ΔSVV(6–8)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, R.; Gan, T.J. Peri-operative fluid management to enhance recovery. Anaesthesia 2016, 71 (Suppl. 1), 40–45. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Dai, S.; Tao, X.; Chen, X.; Xu, L. Corrected flow time and respirophasic variation in blood flow peak velocity of radial artery predict fluid responsiveness in gynecological surgical patients with mechanical ventilation. BMC Anesthesiol. 2022, 22, 299. [Google Scholar] [CrossRef] [PubMed]
- Thacker, J.K.; Mountford, W.K.; Ernst, F.R.; Krukas, M.R.; Mythen, M.M.G. Perioperative fluid utilization variability and association with outcomes: Considerations for enhanced recovery efforts in sample US surgical populations. Ann. Surg. 2016, 263, 502–510. [Google Scholar] [CrossRef]
- Monnet, X.; Marik, P.E.; Teboul, J.L. Prediction of fluid responsiveness: An update. Ann. Intensive Care 2016, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Jozwiak, M.; Monnet, X.; Teboul, J.L. Prediction of fluid responsiveness in ventilated patients. Ann. Transl. Med. 2018, 6, 352. [Google Scholar] [CrossRef]
- Szrama, J.; Gradys, A.; Bartkowiak, T.; Woźniak, A.; Kusza, K.; Molnar, Z. Intraoperative Hypotension Prediction-A Proactive Perioperative Hemodynamic Management-A Literature Review. Medicina 2023, 59, 491. [Google Scholar] [CrossRef]
- Nimje, G.R.; Goyal, V.K.; Singh, P.; Shekhrajka, P.; Mishra, A.; Mittal, S. Assessment of fluid responsiveness after tidal volume challenge in renal transplant recipients: A nonrandomized prospective interventional study. Clin. Transpl. Res. 2024, 38, 188–196. [Google Scholar] [CrossRef]
- Muzaffar, S.N.; Pradhan, A.; Siddiqui, S.S.; Roy, S.; Suresh, T. Monitoring Macro- and Microcirculation in the Critically Ill: A Narrative Review. Avicenna J. Med. 2023, 13, 138–150. [Google Scholar] [CrossRef]
- Bruscagnin, C.; Shi, R.; Rosalba, D.; Fouqué, G.; Hagry, J.; Lai, C.; Donadello, K.; Pham, T.; Teboul, J.-L.; Monnet, X. Testing preload responsiveness by the tidal volume challenge assessed by the photoplethysmographic perfusion index. Crit. Care 2024, 28, 305. [Google Scholar] [CrossRef]
- Jalil, B.A.; Cavallazzi, R. Predicting fluid responsiveness: A review of literature and a guide for the clinician. Am. J. Emerg. Med. 2018, 36, 2093–2102. [Google Scholar] [CrossRef] [PubMed]
- Douglas, I.S.; Elwan, M.H.; Najarro, M.; Romagnoli, S. Dynamic monitoring tools for patients admitted to the emergency department with circulatory failure: Narrative review with panel-based recommendations. Eur. J. Emerg. Med. 2024, 31, 98–107. [Google Scholar] [CrossRef]
- Messina, A.; Albini, M.; Samuelli, N.; Brunati, A.; Costantini, E.; Lionetti, G.; Lubian, M.; Greco, M.; Matronola, G.M.; Piccirillo, F.; et al. Fluid boluses and infusions in the early phase of resuscitation from septic shock and sepsis-induced hypotension: A retrospective report and outcome analysis from a tertiary hospital. Ann. Intensive Care 2024, 14, 123. [Google Scholar] [CrossRef]
- El Hadouti, Y.; Valencia, L.; Becerra, A.; Rodríguez-Pérez, A.; Vincent, J.L. Echocardiography and passive leg raising in the postoperative period: A prospective observational study. Eur. J. Anaesthesiol. 2017, 34, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Eikermann, M.; Kurth, T. Apply protective mechanical ventilation in the operating room in an individualized approach to perioperative respiratory care. Anesthesiology 2015, 123, 12–14. [Google Scholar] [CrossRef]
- Pinsky, M.R. Discovering the Clinical Relevance of Heart-Lung Interactions. Anesthesiology 2024, 140, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Myatra, S.N.; Prabu, N.R.; Divatia, J.V.; Monnet, X.; Kulkarni, A.P.; Teboul, J.-L. The changes in pulse pressure variation or stroke volume variation after a ‘tidal volume challenge’ reliably predict fluid responsiveness during low tidal volume ventilation. Crit. Care Med. 2017, 45, 415–421. [Google Scholar] [CrossRef]
- Messina, A.; Montagnini, C.; Cammarota, G.; Giuliani, F.; Muratore, L.; Baggiani, M.; Bennett, V.; Della Corte, F.; Navalesi, P.; Cecconi, M. Assessment of Fluid Responsiveness in Prone Neurosurgical Patients Undergoing Protective Ventilation: Role of Dynamic Indices, Tidal Volume Challenge, and End-Expiratory Occlusion Test. Anesth. Analg. 2020, 130, 752–761. [Google Scholar] [CrossRef]
- Jun, J.H.; Chung, R.K.; Baik, H.J.; Chung, M.H.; Hyeon, J.S.; Lee, Y.G.; Park, S.H. The tidal volume challenge improves the reliability of dynamic preload indices during robot-assisted laparoscopic surgery in the Trendelenburg position with lung-protective ventilation. BMC Anesthesiol. 2019, 19, 142. [Google Scholar] [CrossRef]
- Kaptein, E.M.; Kaptein, M.J. Inferior vena cava ultrasound and other techniques for assessment of intravascular and extravascular volume: An update. Clin. Kidney J. 2023, 16, 1861–1877. [Google Scholar] [CrossRef] [PubMed]
- Punzo, G.; Beccia, G.; Cambise, C.; Iacobucci, T.; Sessa, F.; Sgreccia, M.; Sacco, T.; Leone, A.; Congedo, M.T.; Meacci, E.; et al. Goal-Directed Fluid Therapy Using Pulse Pressure Variation in Thoracic Surgery Requiring One-Lung Ventilation: A Randomized Controlled Trial. J. Clin. Med. 2024, 13, 5589. [Google Scholar] [CrossRef] [PubMed]
- Linares-Perdomo, O.; East, T.D.; Brower, R.; Morris, A.H. Standardizing predicted body weight equations for mechanical ventilation tidal volume settings. Chest 2015, 148, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.J.; Lee, S.; Yi, J.W.; Kim, J.H.; Lee, B.J.; Seo, H. Stroke Volume Variation and Stroke Volume Index Can Predict Fluid Responsiveness after Mini-Volume Challenge Test in Patients Undergoing Laparoscopic Cholecystectomy. Medicina 2019, 56, 3. [Google Scholar] [CrossRef] [PubMed]
- Min, J.Y.; Jeon, J.P.; Chung, M.Y.; Kim, C.J. Use of the cardiac power index to predict fluid responsiveness in the prone position: A proof-of-concept study. Braz. J. Anesthesiol. 2024, 74, 844545. [Google Scholar] [CrossRef] [PubMed]
- Botros, J.M.; Salem, Y.S.M.; Khalil, M.; Algyar, M.F.; Yassin, H.M. Effects of tidal volume challenge on the reliability of plethysmography variability index in hepatobiliary and pancreatic surgeries: A prospective interventional study. J. Clin. Monit. Comput. 2023, 37, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Chen, Q.; Huang, Z.; Liang, J.; An, R.; Liu, H. Comparison of the carotid corrected flow time and tidal volume challenge for assessing fluid responsiveness in robot-assisted laparoscopic surgery. J. Robot. Surg. 2023, 17, 2763–2772. [Google Scholar] [CrossRef] [PubMed]
- Corp, A.; Thomas, C.; Adlam, M. The cardiovascular effects of positive pressure ventilation. BJA Educ. 2021, 21, 202–209. [Google Scholar] [CrossRef]
- Messina, A.; Caporale, M.; Calabrò, L.; Lionetti, G.; Bono, D.; Matronola, G.M.; Brunati, A.; Frassanito, L.; Morenghi, E.; Antonelli, M.; et al. Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: A metanalysis and a metaregression. Crit. Care 2023, 27, 431. [Google Scholar] [CrossRef] [PubMed]
- Prütz, M.; Bozkurt, A.; Löser, B.; Haas, S.A.; Tschopp, D.; Rieder, P.; Trachsel, S.; Vorderwülbecke, G.; Menk, M.; Balzer, F.; et al. Dynamic parameters of fluid responsiveness in the operating room: An analysis of intraoperative ventilation framework conditions. Dynamische Parameter der Flüssigkeitsreagibilität im Operationssaal: Eine Analyse der intraoperativen, beatmungsbezogenen Rahmenbedingungen. Anaesthesiologie 2024, 73, 462–468. [Google Scholar]
- Alvarado Sánchez, J.I.; Caicedo Ruiz, J.D.; Diaztagle Fernández, J.J.; Cruz Martínez, L.E.; Carreño Hernández, F.L.; Santacruz Herrera, C.A.; Ospina-Tascón, G.A. Variables influencing the prediction of fluid responsiveness: A systematic review and meta-analysis. Crit. Care 2023, 27, 361. [Google Scholar] [CrossRef] [PubMed]
- Zamani-Aliabadi, S.M.; Qanadli, S.D.; Fatehi-Feyzabad, S.H.; Ghasemnezhad, M.; Ghaemi, H.; Azarine, A.; Mohammadzadeh, A.; Bitarafan-Rajabi, A.; Mortezaeian, H.; Rezaei-Kalantari, K. Assessment of 4D flow MRI for quantification of left-to-right shunt in pediatric patients with ventricular septal defect: Comparison with right heart catheterization. Front. Cardiovasc. Med. 2024, 11, 1399110. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, Y.; Zhang, J.; Huang, T.; Gao, J. Tidal volume challenge-induced hemodynamic changes can predict fluid responsiveness during one-lung ventilation: An observational study. Front. Med. 2023, 10, 1169912. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhao, S.; Zhu, Q. Reliability of stroke volume or pulse pressure variation as dynamic predictors of fluid responsiveness in laparoscopic surgery: A systematic review. J. Clin. Monit. Comput. 2023, 37, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Chaves, R.C.F.; Barbas, C.S.V.; Queiroz, V.N.F.; Serpa Neto, A.; Deliberato, R.O.; Pereira, A.J.; Timenetsky, K.T.; Júnior, J.M.S.; Takaoka, F.; de Backer, D.; et al. Assessment of fluid responsiveness using pulse pressure variation, stroke volume variation, plethysmographic variability index, central venous pressure, and inferior vena cava variation in patients undergoing mechanical ventilation: A systematic review and meta-analysis. Crit. Care 2024, 28, 289. [Google Scholar]
- Xu, Y.; Guo, J.; Wu, Q.; Chen, J. Efficacy of using tidal volume challenge to improve the reliability of pulse pressure variation reduced in low tidal volume ventilated critically ill patients with decreased respiratory system compliance. BMC Anesthesiol. 2022, 22, 137. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Ayed, S.; Moretto, F.; Azzolina, D.; De Vita, N.; Gavelli, F.; Carelli, S.; Pavot, A.; Lai, C.; Monnet, X.; et al. Tidal volume challenge to predict preload responsiveness in patients with acute respiratory distress syndrome under prone position. Crit. Care 2022, 26, 219. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, A.I.; Selim, K.A.; Zaghla, H.E.; Mowafy, H.E.; Fakher, M.A. Comparison of Changes in PPV Using a Tidal Volume Challenge with a Passive Leg Raising Test to Predict Fluid Responsiveness in Patients Ventilated Using Low Tidal Volume. Indian J. Crit. Care Med. 2021, 25, 685–690. [Google Scholar] [CrossRef]
- Zhang, H.; Lian, H.; Zhang, Q.; Zhao, H.; Wang, X. Can central venous pressure help identify acute right ventricular dysfunction in mechanically ventilated critically ill patients? Ann. Intensive Care 2024, 14, 114. [Google Scholar] [CrossRef]
- Vignon, P.; Evrard, B.; Asfar, P.; Busana, M.; Calfee, C.S.; Coppola, S.; Demiselle, J.; Geri, G.; Jozwiak, M.; Martin, G.S.; et al. Fluid administration and monitoring in ARDS: Which management? Intensive Care Med. 2020, 46, 2252–2264. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Montagnini, C.; Cammarota, G.; De Rosa, S.; Giuliani, F.; Muratore, L.; Della Corte, F.; Navalesi, P.; Cecconi, M. Tidal volume challenge to predict fluid responsiveness in the operating room: An observational study. Eur. J. Anaesthesiol. 2019, 36, 583–591. [Google Scholar] [CrossRef]
- de Keijzer, I.N.; Scheeren, T.W.L. Perioperative Hemodynamic Monitoring: An Overview of Current Methods. Anesthesiol. Clin. 2021, 39, 441–456. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.R.; Senefeld, J.W.; Larson, K.F.; Joyner, M.J. Consequences of group III/IV afferent feedback and respiratory muscle work on exercise tolerance in heart failure with reduced ejection fraction. Exp. Physiol. 2023, 108, 1351–1365. [Google Scholar] [CrossRef]
- Kosta, S.; Dauby, P.C. Frank-Starling mechanism, fluid responsiveness, and length-dependent activation: Unravelling the multiscale behaviors with an in silico analysis. PLoS Comput. Biol. 2021, 17, e1009469. [Google Scholar]
- Constantin, J.M.; Godet, T.; Jabaudon, M.; Bazin, J.E.; Futier, E. Recruitment maneuvers in acute respiratory distress syndrome. Ann. Transl. Med. 2017, 5, 290. [Google Scholar] [CrossRef]
- Yi, J.M.; Bang, J.Y.; Choi, B.; Cho, C.; Lee, Y.-H.; Lee, E.-K.; Choi, B.-M.; Noh, G.-J. Population-based volume kinetics of crystalloids and colloids in healthy volunteers. Sci. Rep. 2019, 9, 18638. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Responders (n = 19) | Non-Responders (n = 21) | |
|---|---|---|
| Age (years) | 64.9 ± 12.3 | 63.8 ± 12.7 |
| Sex (M/F) | 9/10 | 12/9 |
| BMI (kg/m2) | 25.2 [6.3] | 25.9 [5.5] |
| IBW (kg) | 62.6 ± 10.3 | 61.8 ± 7.9 |
| ASA score | 2.0 [0.8] | 2.0 [1.0] |
| Preop Hb (g/dL) | 11.5 ± 2.3 | 12.5 ± 1.6 |
| Preop Cr (mg/dL) | 0.81 ± 0.22 | 0.8 [0.4] |
| Baseline eGFR (mL/min/1.73 m2) | 42.0 ± 8.9 | 47.5 ± 11.1 |
| Comorbidities | ||
| Hypertension | 47% | 53% |
| Coronary Artery Disease | 5% | 5% |
| COPD/Asthma | 0% | 11% |
| Cerebrovascular Disease | 0% | 5% |
| Diabetes Mellitus | 26% | 16% |
| Chronic Renal Disease | 0% | 5% |
| Malignancy | 79% | 90% |
| Perioperative data | ||
| Surgery duration (minutes) | 253.0 ± 115.7 | 200.0 [88.2] |
| Anesthesia duration (minutes) | 284.0 ± 115.4 | 233.5 [108] |
| Epidural (Yes/No) | 53%/47% | 52%/48% |
| Total Crystalloids (mL) | 3294.0 ± 1442.0 | 3000.0 [1850] |
| Fluids infused before VE (mL) | 1200.0 [650] | 1200.0 [375] |
| Sevoflurane (% min) | 539.0 ± 237.0 | 490.0 [191.5] |
| Total Phenylephrine (mg) | 8.3 [6] | 4.8 [25.7] |
| Total Ephedrine (mg) | 0.0 [9.4] | 2.5 [17.5] |
| Intraoperative Diuresis (mL) | 831.0 ± 475.0 | 600.0 [550] |
| Blood loss (mL) | 525 [312.5] | 400 [825] |
| In-hospital stay (days) | 8.5 [6.8] | 9.0 [14.0] |
| NSQIP score for any complication (%) | 22.5 ± 0.09 | 17.4 ± 0.09 |
| NSQIP score for serious complication (%) | 19.2 ± 0.08 | 15.5 ± 0.08 |
| Before VtC (T1) | After VtC (T2) | Before VE (T3) | After VE (T4) | ||
|---|---|---|---|---|---|
| HR (beats/min) | Responders | 76 (68–85) | 73 (59–80) | 77 (67–82) | 71 (66–79) |
| Non-R | 76 (62–78) | 73.5 (66–81) | 70 (65–81) | 69.5 (63 to 78) | |
| MAP (mmHg) | Responders | 78 (71–87) | 73 (59–79) * | 83 (74–90) * | 85 (78–93) |
| Non-R | 80 (69–87) | 80 (69–91) | 90 (83–99) | 83 (74–96) | |
| SVI (mL/min2) | Responders | 38 (35–43.8) | 36.5 (34–43) | 39 (32.5–44.8) | 46.5 (39.3–51.8) $ |
| Non-R | 43.5 (36.8–50.8) | 47 (35.5–58) | 50.5 (34.5–60) | 42 (34.3–59.8) | |
| CI (L/min/m2) | Responders | 2.9 (2.6–3.5) | 2.8 (2.5–3.4) | 3.0 (2.2–3.6) | 3.3 (2.7–4.1) |
| Non-R | 2.9 (2.5–3.5) | 3.3 (2.5–3.7) | 3.0 (2.5–3.7) | 2.9 (2.2–3.8) | |
| PPV (%) | Responders | 8 (6.3–10) ** | 11 (10–12.8) **,$$ | 9 (8–13.3) * | 7.5 (5–9) $ |
| Non-R | 7.5 (5.3–10.8) | 7 (5–9.8) | 6.5 (5–10.5) | 6.5 (4–8.8) | |
| SVV (%) | Responders | 8 (6.3 to 9) ** | 10 (9–12) **,$$ | 8.5 (7.3–10.8) * | 7.5 (5.3–8) $ |
| Non-R | 7 (5.3–9.8) | 7 (5–9) | 6 (5.3–9) | 6 (5–9.5) | |
| CVP (mmHg) | Responders | 10 (9–12) | 10 (7.3–11) | 9.5 (7–11.8) | 11 (9.3–12.8) |
| Non-R | 10 (8–13) | 10 (8.3–11) | 10.5 (6.3–12) | 10 (8–13) |
| AUC (95% CI) | p Value | Youden Index | Cut-Off Value (%) | Sensitivity (%) | p Value | Specificity (%) | p Value | |
|---|---|---|---|---|---|---|---|---|
| PPV6 | 0.69(0.33–0.69) | 0.05 | 0.18 | 7 | 72 | 0.002 | 45 | 0.56 |
| PPV8 | 0.76 (0.59–0.89) | 0.0006 | 0.56 | 10 | 83 | <0.0001 | 73 | <0.001 |
| ΔPPV(6–8) | 0.86 (0.74–0.95) | <0.0001 | 0.56 | 2 | 83 | <0.0001 | 73 | 0.0012 |
| SVV6 | 0.68 (0.33–0.69) | 0.049 | 0.18 | 7 | 72 | <0.0001 | 45 | 0.56 |
| SVV8 | 0.75 (0.59–0.89) | <0.0001 | 0.49 | 8 | 94 | <0.0001 | 54 | 0.56 |
| ΔSVV(6–8) | 0.82 (0.67–0.94) | <0.0001 | 0.61 | 2 | 83 | <0.0001 | 77 | <0.0001 |
| Gray Zone (%) | Number of Patients in the Gray Zone (%) | Responders in the Gray Zone | Non-Responders in the Gray Zone | Gray-Zone Sensitivity (90% CI) | Gray-Zone Specificity (90% CI) | |
|---|---|---|---|---|---|---|
| PPV6 | 4 to 16 | 36 (90%) | 17/19 | 19/21 | 72 | 45 |
| SVV6 | 5 to 14 | 37 (92.5%) | 18/19 | 19/21 | 73 | 46 |
| PPV8 | 6 to 13 | 26 (65%) | 13/19 | 13/21 | 83 | 73 |
| SVV8 | 8 to 13 | 25 (63%) | 16/19 | 9/21 | 94 | 54 |
| ΔPPV(6–8) | 1.6 to 2.4 | 11 (27.5%) | 6/19 | 5/21 | 83 | 73 |
| ΔSVV(6–8) | 1.6 to 3.4 | 13 (22.5%) | 11/19 | 2/21 | 83 | 77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griva, P.; Kapetanakis, E.I.; Milionis, O.; Panagouli, K.; Fountoulaki, M.; Sidiropoulou, T. Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study. J. Clin. Med. 2025, 14, 101. https://doi.org/10.3390/jcm14010101
Griva P, Kapetanakis EI, Milionis O, Panagouli K, Fountoulaki M, Sidiropoulou T. Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study. Journal of Clinical Medicine. 2025; 14(1):101. https://doi.org/10.3390/jcm14010101
Chicago/Turabian StyleGriva, Panagiota, Emmanouil I. Kapetanakis, Orestis Milionis, Konstantina Panagouli, Maria Fountoulaki, and Tatiana Sidiropoulou. 2025. "Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study" Journal of Clinical Medicine 14, no. 1: 101. https://doi.org/10.3390/jcm14010101
APA StyleGriva, P., Kapetanakis, E. I., Milionis, O., Panagouli, K., Fountoulaki, M., & Sidiropoulou, T. (2025). Tidal Volume Challenge to Assess Volume Responsiveness with Dynamic Preload Indices During Non-Cardiac Surgery: A Prospective Study. Journal of Clinical Medicine, 14(1), 101. https://doi.org/10.3390/jcm14010101