
Comparative Analysis of Seven Equations for Estimated Glomerular Filtration Rate and Their Impact on Chronic Kidney Disease Categorization in Korean Patients at Local Clinics and Hospitals

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Analytical Methods
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Subjects
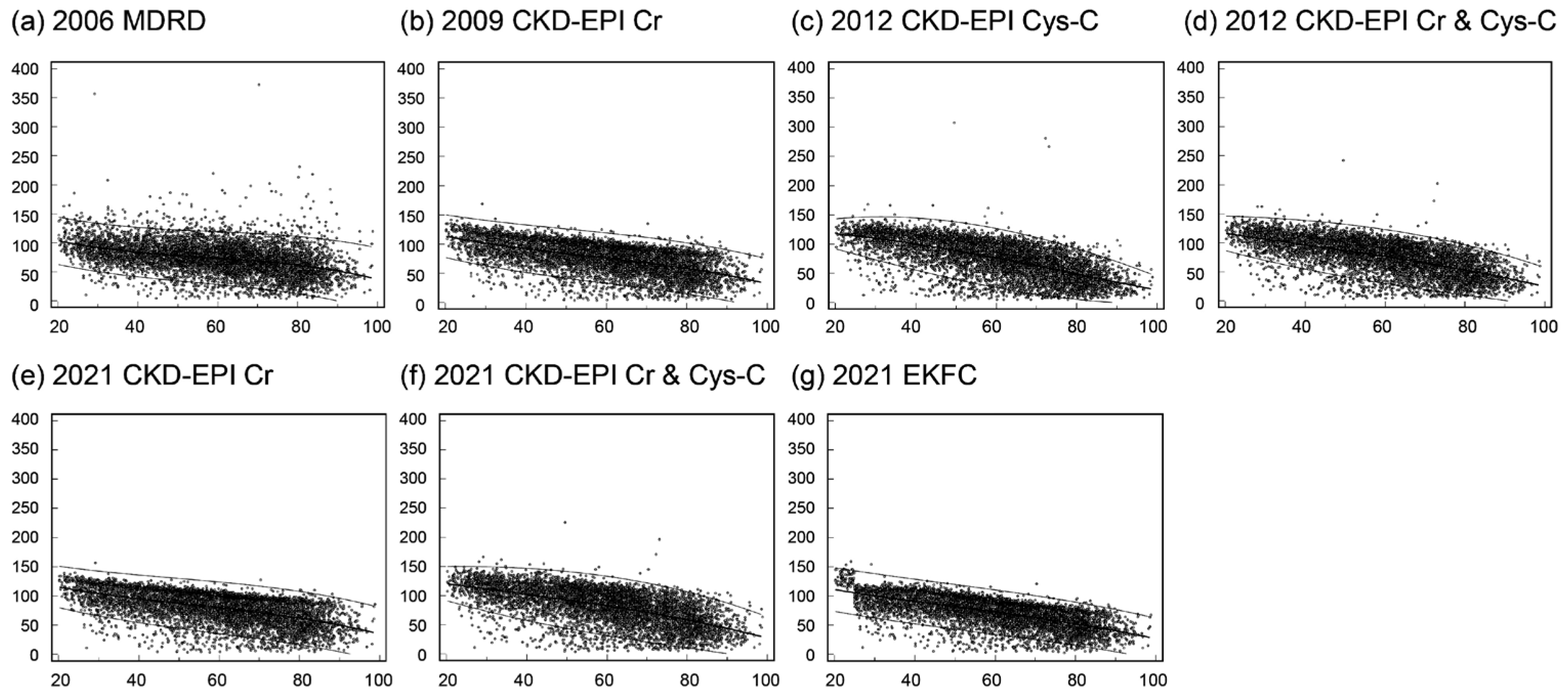
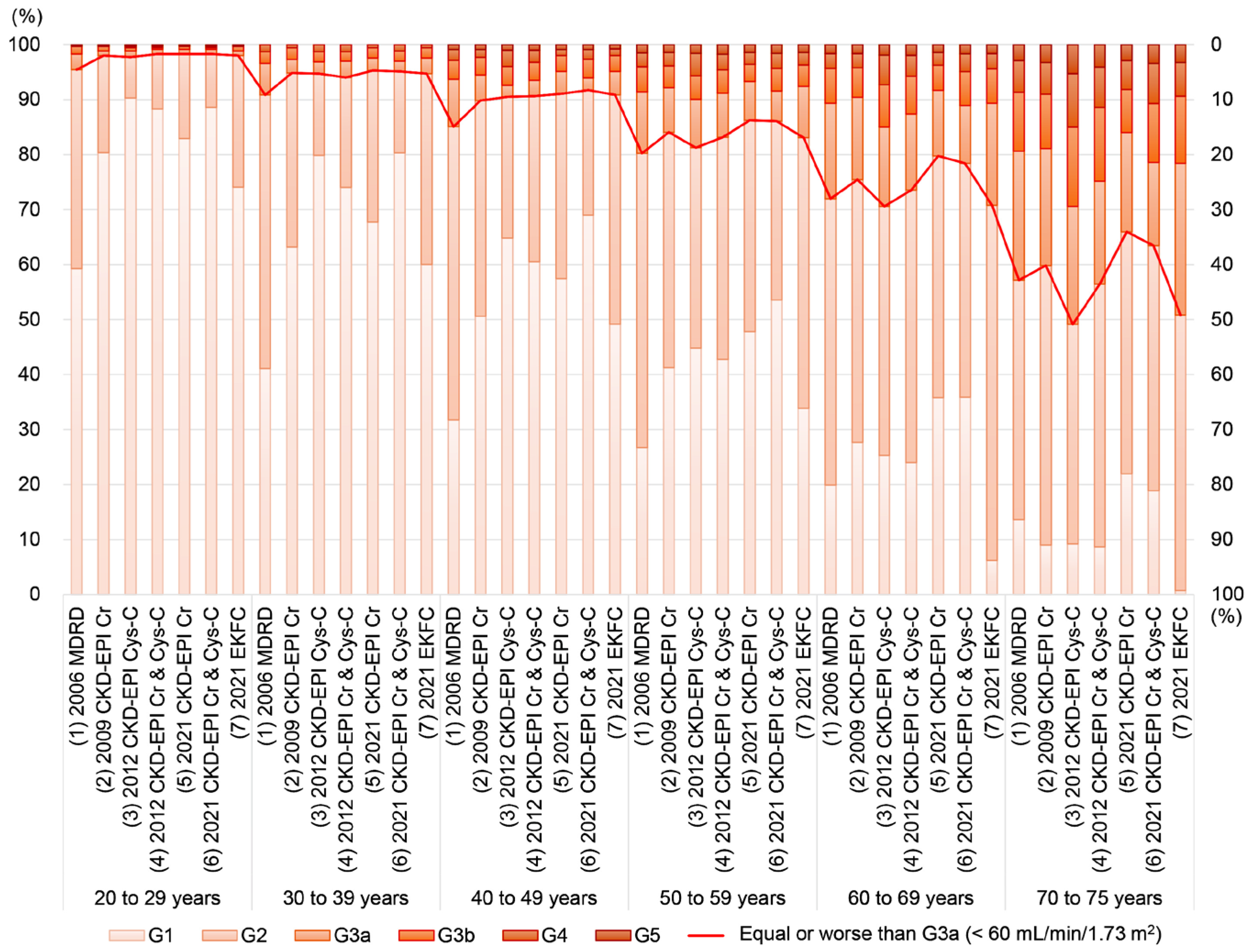
3.2. eGFR Levels and CKD Classification by Age
3.3. Comparison of eGFR Levels and CKD Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- KDIGO. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 5–14. Available online: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf (accessed on 20 March 2024).
- Delanaye, P.; Jager, K.J.; Bökenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J. Am. Soc. Nephrol. 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- Korean Academy of Medical Sciences, Korea Disease Control and Prevention Agency. Evidence-Based Guideline for Chronic Kidney Disease in Primary Care. 2022. Available online: https://ksn.or.kr/bbs/?code=g_guideline (accessed on 14 February 2024).
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Grubb, A.; Blirup-Jensen, S.; Lindström, V.; Schmidt, C.; Althaus, H.; Zegers, I. First certified reference material for cystatin C in human serum ERM-DA471/IFCC. Clin. Chem. Lab. Med. 2010, 48, 1619–1621. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Pottel, H.; Björk, J.; Courbebaisse, M.; Couzi, L.; Ebert, N.; Eriksen, B.O.; Dalton, R.N.; Dubourg, L.; Gaillard, F.; Garrouste, C.; et al. Development and Validation of a Modified Full Age Spectrum Creatinine-Based Equation to Estimate Glomerular Filtration Rate : A Cross-sectional Analysis of Pooled Data. Ann. Intern. Med. 2021, 174, 183–191. [Google Scholar] [CrossRef]
- Buchkremer, F.; Segerer, S. The 2009 and 2021 CKD-EPI Equations: A Graphical Analysis of the Effect of Refitting GFR Estimating Equations without a Race Coefficient. Kidney Med. 2022, 4, 100448. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. Statistics for Chronic Disease and Health. Available online: https://health.kdca.go.kr/healthinfo/biz/pblcVis/main.do (accessed on 13 February 2024).
- Cho, J.M.; Cha, R.H.; Kim, D.K.; Chin, H.J. Performance evaluation of Chronic Kidney Disease Epidemiology Collaboration equations for estimated glomerular filtration rate compared to inulin clearance in Koreans. Kidney Res. Clin. Pract. 2024; Epub ahead of print. [Google Scholar] [CrossRef]
- Kim, D.H.; Hyun, Y.Y.; Cha, J.J.; Lee, S.; Lee, H.K.; Choi, J.W.; Kim, S.H.; Han, S.Y.; Park, C.W.; Lee, E.Y.; et al. Kidney Health Plan 2033 in Korea: Bridging the gap between the present and the future. Kidney Res. Clin. Pract. 2024, 43, 8–19. [Google Scholar] [CrossRef]
- Kim, H.; Park, J.T.; Lee, J.; Jung, J.Y.; Lee, K.B.; Kim, Y.H.; Yoo, T.H.; Kang, S.W.; Choi, K.H.; Oh, K.H.; et al. The difference between cystatin C- and creatinine-based eGFR is associated with adverse cardiovascular outcome in patients with chronic kidney disease. Atherosclerosis 2021, 335, 53–61. [Google Scholar] [CrossRef]
- Kyoung, D.S.; Kim, H.S. Understanding and Utilizing Claim Data from the Korean National Health Insurance Service (NHIS) and Health Insurance Review & Assessment (HIRA) Database for Research. J. Lipid Atheroscler. 2022, 11, 103–110. [Google Scholar]
- Oh, K.H.; Kang, M.; Kang, E.; Ryu, H.; Han, S.H.; Yoo, T.H.; Kim, S.W.; Chae, D.W.; Lee, K.B.; Park, S.K.; et al. The KNOW-CKD Study: What we have learned about chronic kidney diseases. Kidney Res. Clin. Pract. 2020, 39, 121–135. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service. HIRA Bigdata Open Portal. Available online: https://opendata.hira.or.kr/op/opc/olapDiagBhvInfoTab4.do (accessed on 13 February 2024).
- Karger, A.B.; Long, T.; Inker, L.A.; Eckfeldt, J.H. Improved Performance in Measurement of Serum Cystatin C by Laboratories Participating in the College of American Pathologists 2019 CYS Survey. Arch. Pathol. Lab. Med. 2022, 146, 1218–1223. [Google Scholar] [CrossRef]
- Kim, S.; Lee, K.; Park, H.-D.; Lee, Y.-W.; Chun, S.; Min, W.-K. Schemes and Performance Evaluation Criteria of Korean Association of External Quality Assessment (KEQAS) for Improving Laboratory Testing. Ann. Lab. Med. 2021, 41, 230–239. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Jeong, T.-D.; Hong, J.; Lee, W.; Chun, S.; Min, W.-K. Accuracy of the New Creatinine-based Equations for Estimating Glomerular Filtration Rate in Koreans. Ann. Lab. Med. 2023, 43, 244–252. [Google Scholar] [CrossRef]
- Choi, R.; Lee, S.G.; Lee, E.H. Alterations in Glomerular Filtration Rates Using Different Algorithms in the Korean Population Visiting Local Clinics and Hospitals. J. Clin. Med. 2022, 11, 5339. [Google Scholar] [CrossRef]
- Kim, H.; Hur, M.; Lee, S.; Lee, G.H.; Moon, H.W.; Yun, Y.M. European Kidney Function Consortium Equation vs. Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) Refit Equations for Estimating Glomerular Filtration Rate: Comparison with CKD-EPI Equations in the Korean Population. J. Clin. Med. 2022, 11, 4323. [Google Scholar] [CrossRef]
- Cho, J.M.; Koh, J.H.; Kim, M.; Jung, S.; Cho, S.; Lee, S.; Kim, Y.; Kim, Y.C.; Lee, H.; Han, S.S.; et al. Evaluation of risk stratification for acute kidney injury: A comparative analysis of EKFC, 2009 and 2021 CKD-EPI glomerular filtration estimating equations. J. Nephrol. 2024; Epub ahead of print. [Google Scholar] [CrossRef]
- Kim, H.; Hyun, Y.Y.; Yun, H.R.; Joo, Y.S.; Kim, Y.; Jung, J.Y.; Jeong, J.C.; Kim, J.; Park, J.T.; Yoo, T.H.; et al. Predictive performance of the new race-free Chronic Kidney Disease Epidemiology Collaboration equations for kidney outcome in Korean patients with chronic kidney disease. Kidney Res. Clin. Pract. 2023, 42, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kang, M.; Kang, E.; Ryu, H.; Jeong, Y.; Kim, J.; Park, S.K.; Jeong, J.C.; Yoo, T.-H.; Kim, Y.; et al. Comparison of cardiovascular event predictability between the 2009 and 2021 Chronic Kidney Disease Epidemiology Collaboration equations in a Korean chronic kidney disease cohort: The KoreaN Cohort Study for Outcome in Patients With Chronic Kidney Disease. Kidney Res. Clin. Pract. 2023, 42, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Coresh, J.; Deysher, A.E.; Feldman, H.I.; Lash, J.P.; Nelson, R.; Rahman, M.; Deysher, A.E.; Zhang, Y.L.; Schmid, C.H.; et al. Evaluation of the MDRD Study equation in a large diverse population. J. Am. Soc. Nephrol. 2007, 18, 2749–2757. [Google Scholar] [CrossRef] [PubMed]
- Betzler, B.K.; Sultana, R.; He, F.; Tham, Y.C.; Lim, C.C.; Wang, Y.X.; Nangia, V.; Tai, E.S.; Rim, T.H.; Bikbov, M.M.; et al. Impact of Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) GFR Estimating Equations on CKD Prevalence and Classification Among Asians. Front. Med. 2022, 9, 957437. [Google Scholar] [CrossRef] [PubMed]
- Yim, J.; Son, N.H.; Kim, K.M.; Yoon, D.; Cho, Y.; Kyong, T.; Moon, J.Y.; Yi, T.I.; Lee, S.G.; Park, Y.; et al. Establishment of muscle mass-based indications for the cystatin C test in renal function evaluation. Front. Med. 2022, 9, 1021936. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Quinn, R.R.; Lam, N.N.; Elliott, M.J.; Xu, Y.; James, M.T.; Manns, B.; Ravani, P. Accounting for Age in the Definition of Chronic Kidney Disease. JAMA Intern. Med. 2021, 181, 1359–1366. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Data |
|---|---|
| Age, year (median, IQR) | 61.4 (47.2 to 73.4) |
| Age group (n, %) | |
| 20 to 29 years | 351 (5.2) |
| 30 to 39 years | 701 (10.5) |
| 40 to 49 years | 907 (13.6) |
| 50 to 59 years | 1200 (17.9) |
| 60 to 69 years | 1482 (17.9) |
| 70 to 79 years | 1177 (17.6) |
| ≥80 years | 870 (13.0%) |
| Sex (n, %) | |
| Men | 3736 (55.9) |
| Women | 2952 (44.1) |
| Serum Cr (mg/dL, median, IQR) | 0.96 (0.77 to 1.20) |
| Serum Cys-C (mg/L, median, IQR) | 0.98 (0.81 to 1.31) |
| eGFR using 2006 MDRD (mL/min/1.73 m2, median, IQR) | 73.4 (56.8 to 89.7) |
| eGFR using 2009 CKD-EPI Cr (mL/min/1.73 m2, median, IQR) | 79.0 (58.9 to 94.7) |
| eGFR using 2012 CKD-EPI Cys-C (mL/min/1.73 m2, median, IQR) | 77.4 (51.0 to 101.4) |
| eGFR using 2012 CKD-EPI Cr & Cys-C (mL/min/1.73 m2, median, IQR) | 79.0 (55.2 to 97.9) |
| eGFR using 2021 CKD-EPI Cr (mL/min/1.73 m2, median, IQR) | 83.4 (62.5 to 98.8) |
| eGFR using 2021 CKD-EPI Cr & Cys-C (mL/min/1.73 m2, median, IQR) | 85.1 (59.8 to 105.1) |
| eGFR using 2021 EKFC (mL/min/1.73 m2, median, IQR) | 74.3 (55.1 to 89.6) |
| Decreased eGFR (<60 mL/min/1.73 m2, CKD ≥ G3a) | |
| Based on 2006 MDRD 2006 (n, %) | 1926 (28.8%) |
| Based on 2009 CKD-EPI Cr (n, %) | 1754 (26.2%) |
| Based on 2012 CKD-EPI Cys-C (n, %) | 2175 (32.4%) |
| Based on 2012 CKD-EPI Cr & Cys-C (n, %) | 1963 (29.3%) |
| Based on 2021 CKD-EPI Cr (n, %) | 1536 (22.9%) |
| Based on 2021 CKD-EPI Cr & Cys-C (n, %) | 1687 (25.1%) |
| Based on 2021 EKFC (n, %) | 2028 (30.3%) |
| Ref. | Study Period | N of Subjects | Age (y) | Clinical Setting | No. of Eq | Equations | Analytical Methods for Cr | Analytical Methods for Cys-C | Findings (eGFR Levels) |
|---|---|---|---|---|---|---|---|---|---|
| This study | 2022 to 2023 | 6688 | 61.4 a | Subjects underwent serum Cr and Cys-C measurement simultaneously, local clinics and hospitals | 7 | 2006 MDRD, 2009 CKD-EPI Cr, 2012 CKD-EPI Cys-C, 2012 CKD-EPI Cr & Cys-C, 2021 CKD-EPI Cr, 2021 CKD-EPI Cr & Cys-C, and 2021 EKFC | Jaffe method, cobas 8000 system (Roche) | Cias Cys-C kit (Kanto Chemicals) on AU680 analyzer (Beckman Coulter) | 2006 MDRD < 2021 EKFC < 2012 CKD-EPI Cys < 2012 CKD-EPI Cr & Cys-C < 2009 CKD-EPI Cr < 2021 CKD-EPI Cr & Cys-C |
| Choi et al. [23] | 2019 to 2021 | 442,566 | 50.1 | Health checkup, local clinics and hospitals | 3 | 2006 MDRD, 2009 CKD-EPI Cr, and 2021 CKD-EPI Cr | Jaffe method, cobas 8000 system (Roche) | Cys-C was not included | 2006 MDRD < 2009 CKD-EPI < 2021 CKD-EPI Cr |
| Kim et al. [24] | 2018 to 2020 | 106,021 | 48.0 a | Annual physical checkup, single center | 4 | 2009 CKD-EPI Cr, 2012 CKD-EPI Cr & Cys-C, 2021 CKD-EPI Cr & Cys-C, and 2021 EKFC | Jaffe method, Creatinine FS (DiaSys, Holzheim, Germany) on TBA-FX8 (Canon Medical Systems Corporation, Tokyo, Japan) | Gentian Cystatin C Immunoassay kit (Gentian Diagnostics AS Moss, Norway) on TBA-FX8 (Canon Medical Systems Corporation) | 2021 EKFC < 2009 CKD-EPI Cr = 2012 CKD-EPI Cr & Cys-C < 2021 CKD-EPI Cr & Cys-C |
| Cho et al. [25] | 2011 to 2021 | 187,139 | 58.2 | AKI, single center (27,447 AKI patients and 159,692 controls) | 3 | 2009 CKD-EPI Cr, 2021 CKD-EPI Cr, and 2021 EKFC | Not described | Cys-C was not included | 2021 EKFC < 2009 CKD-EPI Cr < 2021 CKD-EPI Cr |
| Cho et al. [13] | 2008 to 2013 | 239 | 49.4 | Single center (201 CKD patients and 38 health volunteers) | 5 | 2009 CKD-EPI Cr, 2012 CKD-EPI Cr & Cys-C, 2012 CKD-EPI Cys-C, 2021 CKD-EPI Cr, and 2021 CKD-EPI Cr & Cys-C | Jaffe method, Hitachi 7600 analyzer (200FR, Toshiba) | Particle-enhanced immunoturbidimetric assay, cobas 6000 system (Roche) | 2009 CKD-EPI Cr < 2021 CKD-EPI Cr < 2012 CKD-EPI Cr & Cys-C < 2021 CKD-EPI Cr & Cys-C < 2012 CKD-EPI Cys-C |
| Jeong et al. [22] | 2009 to 2020 | 1654 | 61.0 a | Subjects underwent 51Cr-EDTA GFR test, single center | 3 | 2009 CKD-EPI Cr, 2012 CKD-EPI Cr, and 2021 EKFC | Jaffe method (Roche) | Cys-C was not included | 2021 EKFC < 2009 CKD-EPI Cr < 2021 CKD-EPI Cr |
| Kim et al. [26] | 2011 to 2015 | 2149 | 53.8 | KNOW-CKD cohort | 4 | 2009 CKD-EPI Cr, 2012 CKD-EPI Cr & Cys-C, 2021 CKD-EPI Cr, and 2021 CKD-EPI Cr & Cys-C | Jaffe method, ADVIA Chemistry XPT System (Siemens) | Particle-enhanced nephelometric immunoassay, BN II System (Siemens) | 2012 CKD-EPI Cr & Cys-C < 2009 CKD-EPI Cr < 2021 CKD-EPI Cr & Cys-C < 2021 CKD-EPI Cr |
| Kim et al. [27] | 2011 to 2015 | 2207 | 55.0 a | KNOW-CKD cohort | 3 | 2009 CKD-EPI Cr, 2021 CKD-EPI Cr, and 2021 CKD-EPI Cr & Cys-C | Not described | Not described | 2009 CKD-EPI Cr < 2021 CKD-EPI Cr < 2021 CKD-EPI Cr & Cys-C equations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, R.; Lee, S.G.; Lee, E.H. Comparative Analysis of Seven Equations for Estimated Glomerular Filtration Rate and Their Impact on Chronic Kidney Disease Categorization in Korean Patients at Local Clinics and Hospitals. J. Clin. Med. 2024, 13, 1945. https://doi.org/10.3390/jcm13071945
Choi R, Lee SG, Lee EH. Comparative Analysis of Seven Equations for Estimated Glomerular Filtration Rate and Their Impact on Chronic Kidney Disease Categorization in Korean Patients at Local Clinics and Hospitals. Journal of Clinical Medicine. 2024; 13(7):1945. https://doi.org/10.3390/jcm13071945
Chicago/Turabian StyleChoi, Rihwa, Sang Gon Lee, and Eun Hee Lee. 2024. "Comparative Analysis of Seven Equations for Estimated Glomerular Filtration Rate and Their Impact on Chronic Kidney Disease Categorization in Korean Patients at Local Clinics and Hospitals" Journal of Clinical Medicine 13, no. 7: 1945. https://doi.org/10.3390/jcm13071945
APA StyleChoi, R., Lee, S. G., & Lee, E. H. (2024). Comparative Analysis of Seven Equations for Estimated Glomerular Filtration Rate and Their Impact on Chronic Kidney Disease Categorization in Korean Patients at Local Clinics and Hospitals. Journal of Clinical Medicine, 13(7), 1945. https://doi.org/10.3390/jcm13071945