

Endoscopic Lumbar Disc Surgery Experience with the TESSYS Technique in 253 Case Series

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Data
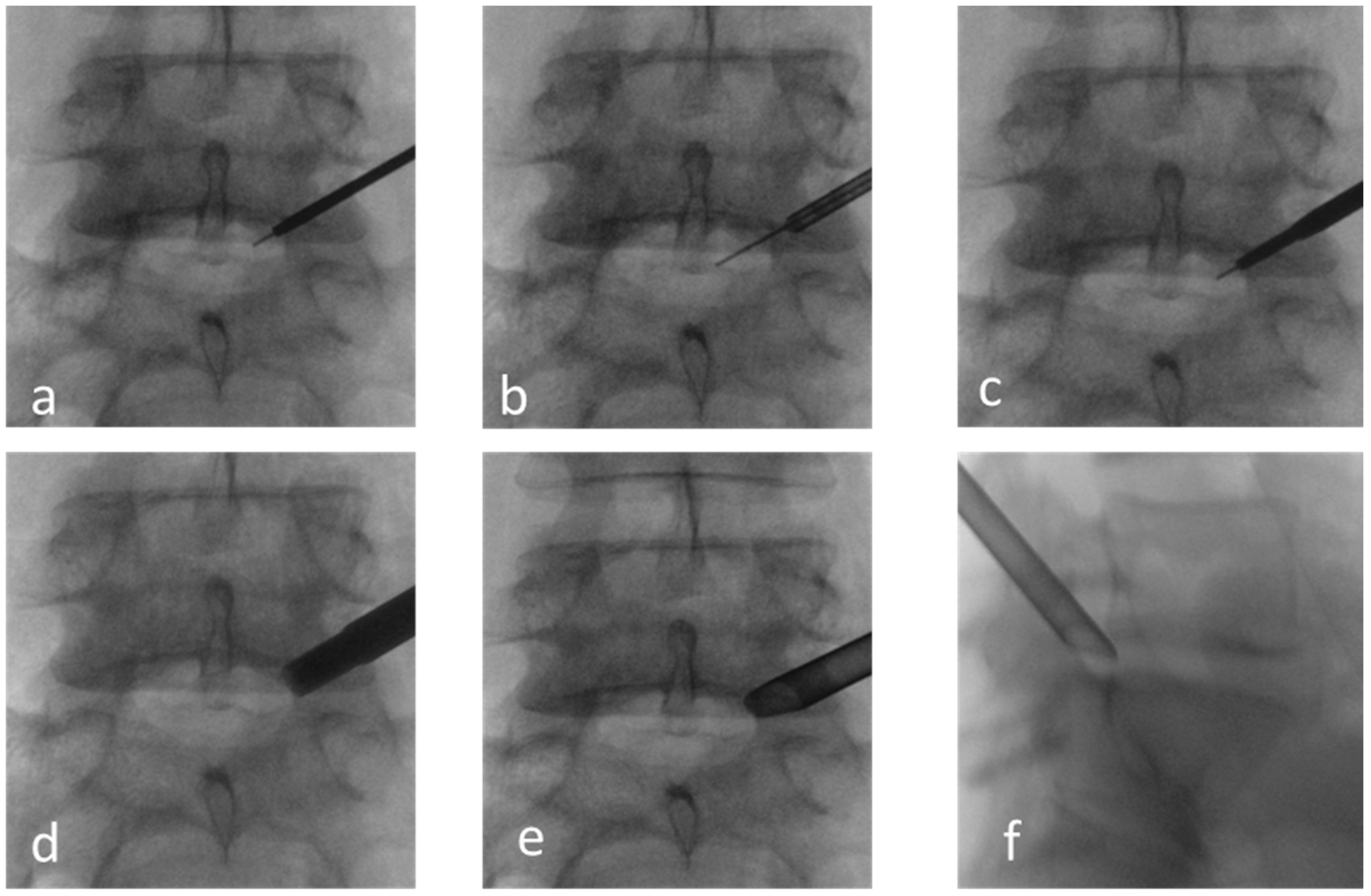
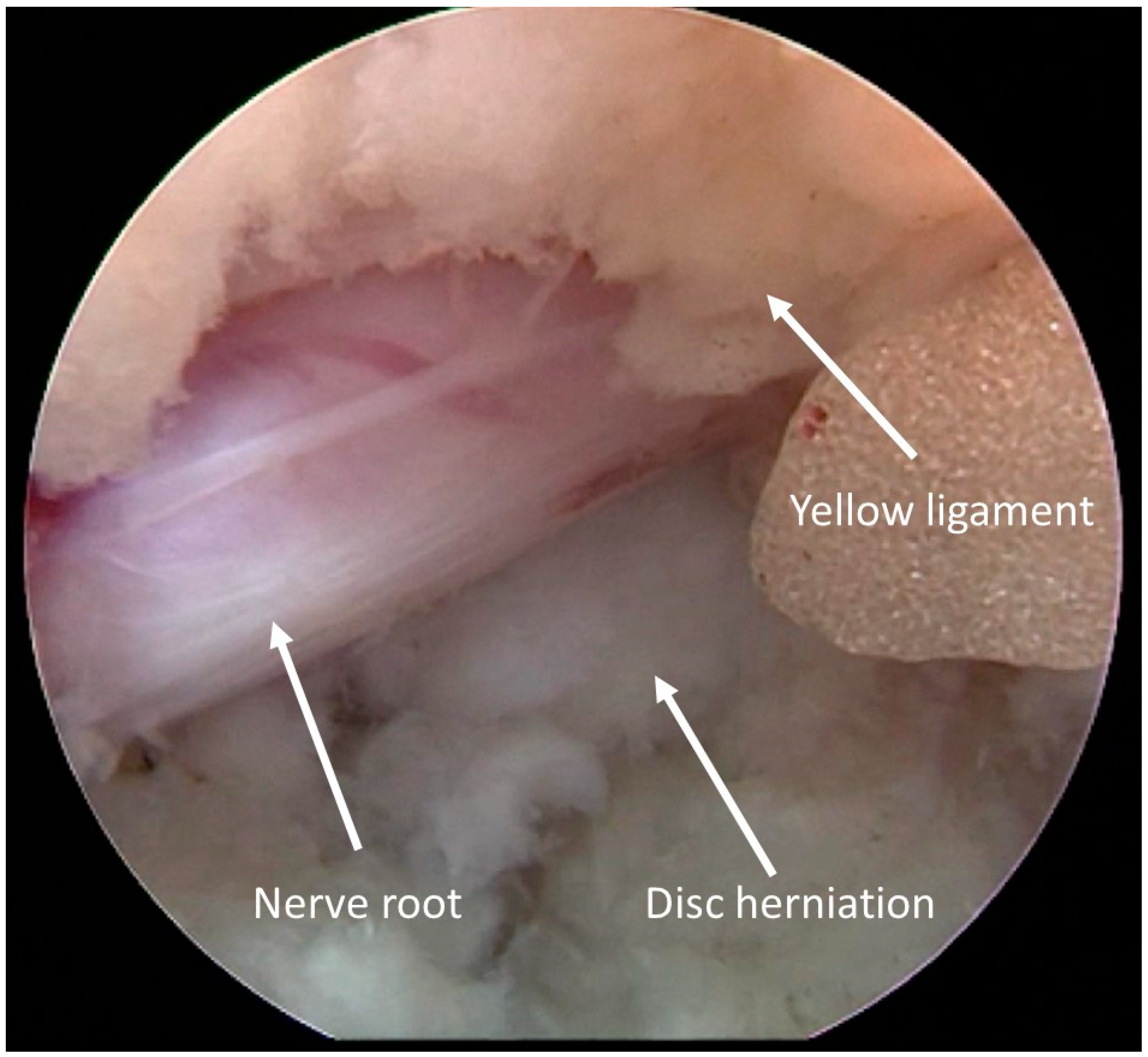
2.3. Surgical Data
2.4. Statistical Analysis
3. Results
3.1. Clinical Outcomes
3.2. Complications
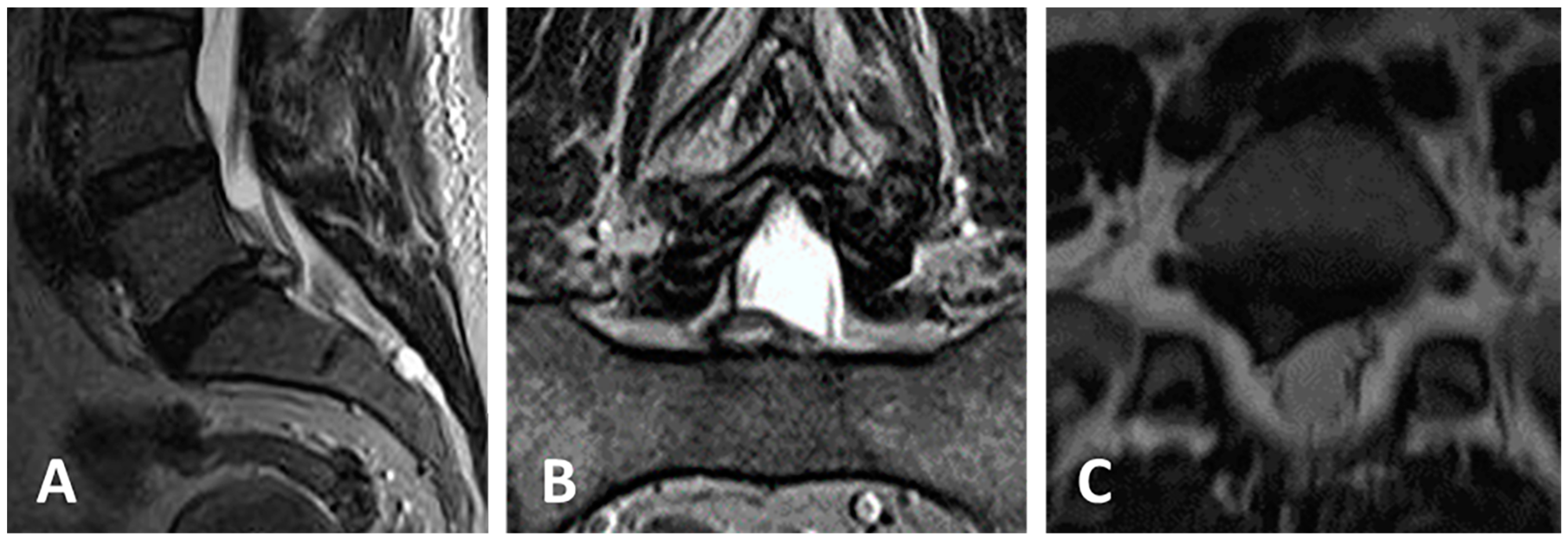
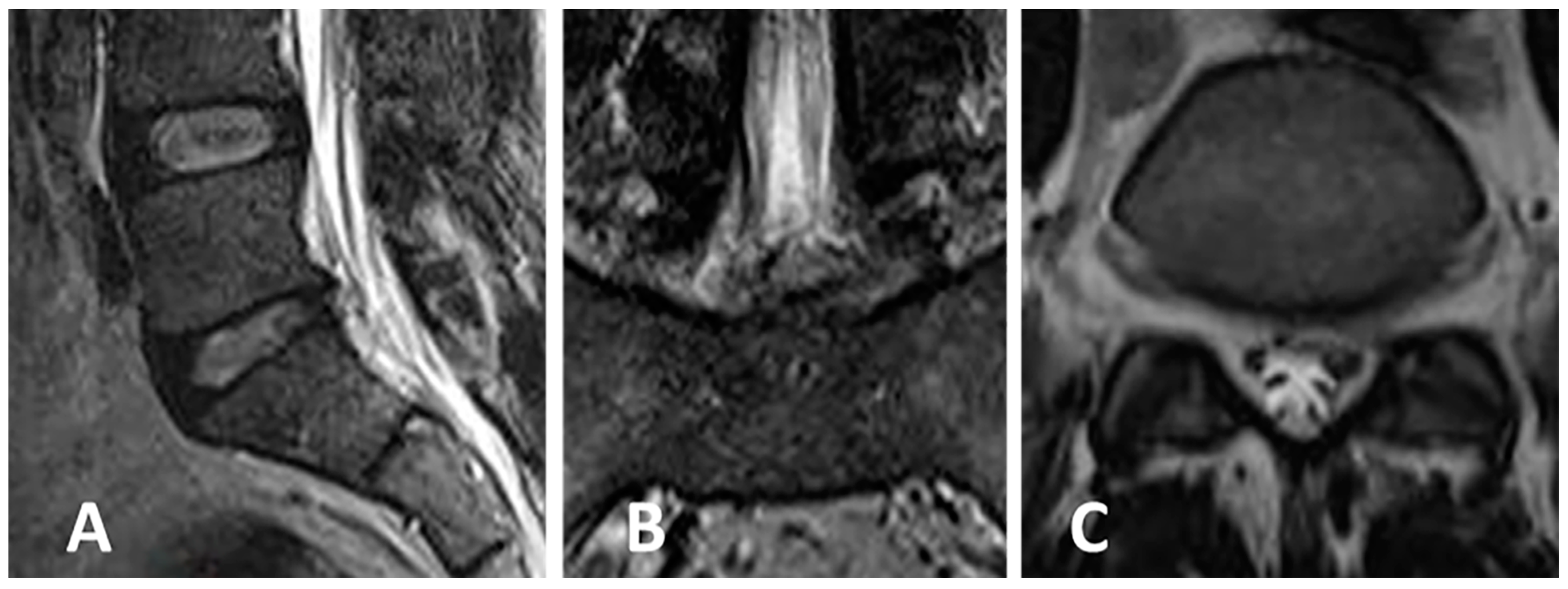
3.3. Clinical Case 1
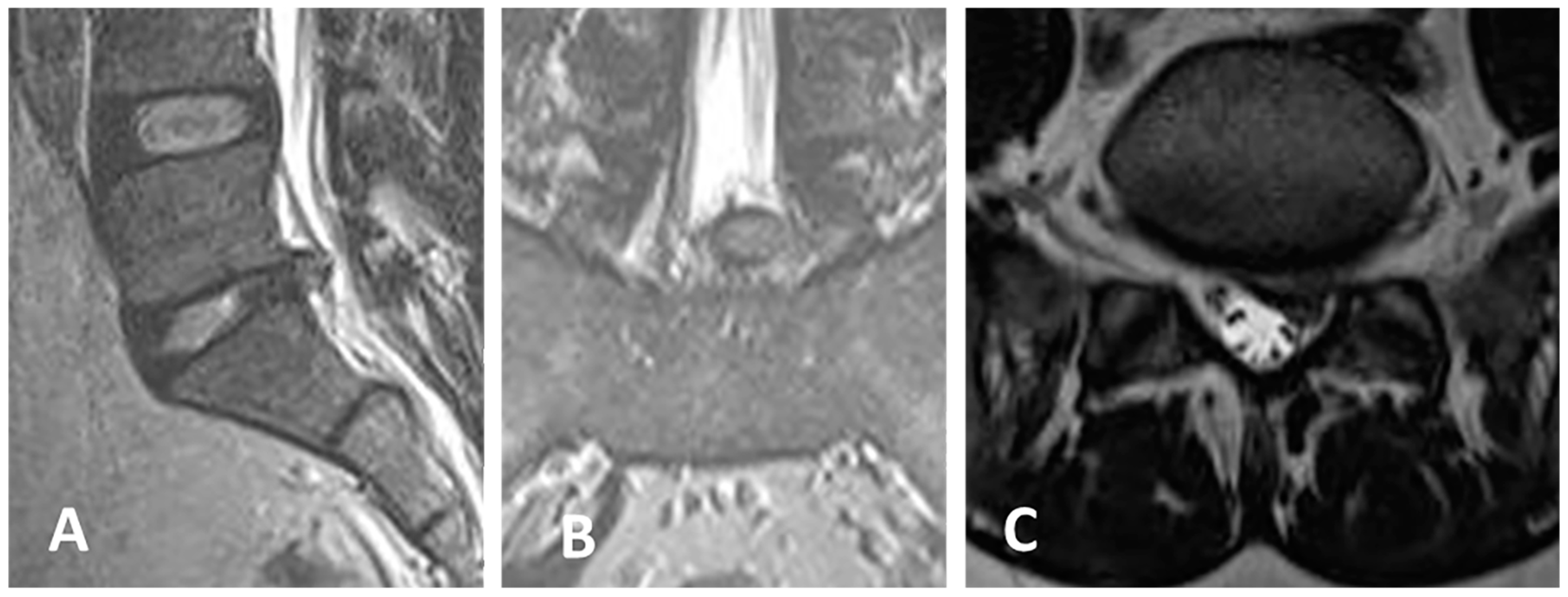
3.4. Clinical Case 2
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cowperthwaite, M.C.; van den Hout, W.B.; Webb, K.M. The impact of early recovery on long-term outcomes in a cohort of patients undergoing prolonged non operative treatment for lumbar disc herniation: Clinical article. J. Neurosurg. Spine 2013, 19, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, W.C.; van Tulder, M.; Arts, M.; Rubinstein, S.M.; van Middelkoop, M.; Ostelo, R.; Verhagen, A.; Koes, B.; Peul, W.C. Surgery versus conservative management of sciatica due to a lumbar herniated disc: A systematic review. Eur. Spine J. 2011, 20, 513–522. [Google Scholar] [CrossRef]
- Konstantinou, K.; Dunn, K.M. Sciatica: Review of epidemiological studies and prevalence estimates. Spine 2008, 33, 2464–2472. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Choi, G.; Lee, S.H. Endoscopic Spine Procedures; Thieme Medical Publishers, Inc.: New York, NY, USA, 2011. [Google Scholar]
- Mixter, W.J.; Barr, J.S. Rupture of the intervertebral disc with involvement of the spinal canal. N. Engl. J. Med. 1934, 211, 210–215. [Google Scholar] [CrossRef]
- Nellensteijn, J.; Ostelo, R.; Bartels, R.; Peul, W.; van Royen, B.; van Tulder, M. Transforaminal endoscopic surgery for symptomatic lumbar disc herniations: A systematic review of the literature. Eur. Spine J. 2010, 19, 181–204. [Google Scholar] [CrossRef] [PubMed]
- Blamoutier, A. Surgical discectomy for lumbar disc herniation: Surgical techniques. Orthop. Traumatol. Surg. Res. 2013, 99, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Caspar, W. Lumbar Disc Adult Hydrocephalus; Springer: Berlin/Heidelberg, Germany, 1977. [Google Scholar]
- Williams, R.W. Microlumbar discectomy: A conservative surgical approach to the virgin herniated lumbar disc. Spine 1978, 3, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Kambin, P.; O’Brien, E.; Zhou, L.; Schaffer, J. Arthroscopic microdiscectomy and selective fragmentectomy. Clin. Orthop. Relat. Res. 1998, 347, 150–167. [Google Scholar] [CrossRef]
- Pan, Z.; Ha, Y.; Yi, S.; Cao, K. Efficacy of Transforaminal Endoscopic Spine System (TESSYS) Technique in Treating Lumbar Disc Herniation. Med. Sci. Monit. 2016, 22, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Li, Q.; Li, S.; Mao, H.; Meng, B.; Zhou, F.; Yang, H. Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications. Pain Physician 2020, 23, 49–56. [Google Scholar]
- Gadjradj, P.S.; Harhangi, B.S.; Amelink, J.; van Susante, J.; Kamper, S.; van Tulder, M.; Peul, W.C.; Vleggeert-Lankamp, C.; Rubinstein, S.M. Percutaneous Transforaminal Endoscopic Discectomy Versus Open Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-analysis. Spine 2021, 46, 538–549. [Google Scholar] [CrossRef]
- Kim, M.; Lee, S.; Kim, H.S.; Park, S.; Shim, S.Y.; Lim, D.J. A Comparison of Percutaneous Endoscopic Lumbar Discectomy and Open Lumbar Microdiscectomy for Lumbar Disc Herniation in the Korean: A Meta-Analysis. BioMed Res. Int. 2018, 2018, 9073460. [Google Scholar] [CrossRef]
- Muthu, S.; Ramakrishnan, E.; Chellamuthu, G. Is Endoscopic Discectomy the Next Gold Standard in the Management of Lumbar Disc Disease? Systematic Review and Superiority Analysis. Glob. Spine J. 2021, 11, 1104–1120. [Google Scholar] [CrossRef]
- Jitpakdee, K.; Liu, Y.; Kotheeranurak, V.; Kim, J.S. Transforaminal Versus Interlaminar Endoscopic Lumbar Discectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Glob. Spine J. 2023, 13, 575–587. [Google Scholar] [CrossRef]
- Wang, G.C.; Chen, C.M. Full Endoscopic Transforaminal Lumbar Discectomy: A Literature Review. J. Minim. Invasive Spine Surg. Tech. 2021, 6, S103–S108. [Google Scholar] [CrossRef]
- Yuh, W.T.; Lee, C.H.; Chung, C.K.; Kim, C.H. Narrative Review of Uniportal, Transforaminal Endoscopic Lumbar Discectomy. Int. J. Pain 2022, 13, 11–19. [Google Scholar] [CrossRef]
- Zhang, J.; Gao, Y.; Zhao, B.; Li, H.; Hou, X.; Yin, L. Comparison of percutaneous transforaminal endoscopic discectomy and open lumbar discectomy for lumbar disc herniations: A systematic review and meta-analysis. Front. Surg. 2022, 9, 984868. [Google Scholar] [CrossRef]
- Gu, X.; He, S.-S.; Zhang, H.-L. Morphometric analysis of the YESS and TESSYS techniques of percutaneous transforaminal endoscopic lumbar discectomy. Clin. Anat. 2013, 26, 728–734. [Google Scholar]
- Jasper, G.P.; Francisco, G.M.; Telfeian, A.E. Clinical success of transforaminal endoscopic discectomy with foraminotomy: A retrospective evaluation. Clin. Neurol. Neurosurg. 2013, 115, 1961–1965. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, J.X.; Sun, B.; Cao, P.; Tian, Y.; Shen, X.L.; Liu, Y.; Chen, H.J.; Wang, X.W.; Yuan, W.; et al. Percutaneous endoscopic lumbar discectomy in treating calcified lumbar intervertebral disc herniation. World Neurosurg. 2019, 122, 1449–1456. [Google Scholar] [CrossRef]
- Tian, W.; Lv, Y.; Liu, Y.; Xiao, B.; Han, X. The high prevalence of symptomatic degenerative lumbar osteoarthritis in Chinese adults: A population-based study. Spine 2014, 39, 1301–1310. [Google Scholar] [CrossRef]
- Liu, X.; Yuan, S.; Tian, Y.; Wang, L.; Gong, L.; Zheng, Y.; Li, J. Comparison of percutaneous endoscopic transforaminal discectomy, microendoscopic discectomy, and microdiscectomy for symptomatic lumbar disc herniation: Minimum 2-year follow-up results. J. Neurosurg. Spine 2018, 28, 317–325. [Google Scholar] [CrossRef]
- Yuan, C.; Zhou, Y.; Pan, Y.; Wang, J. Curative effect comparison of transforaminal endoscopic spine system and traditional open discectomy: A meta-analysis. ANZ J. Surg. 2020, 90, 123–129. [Google Scholar] [CrossRef]
- Hoogland, T.; Schubert, M.; Miklitz, B.; Ramirez, A. Transforaminal posterolateral endoscopic discectomy with or without the combination of a low-dose chymopapain: A prospective randomized study in 280 consecutive cases. Spine 2006, 31, 890–897. [Google Scholar] [CrossRef]
- Li, X.; Hu, Z.; Cui, J.; Han, Y.; Pan, J.; Yang, M.; Tan, J.; Sun, G.; Li, L. Percutaneous endoscopic lumbar discectomy for recurrent lumbar disc herniation. Int. J. Surg. 2016, 27, 8–16. [Google Scholar] [CrossRef]
- Ahn, Y. Transforaminal percutaneous endoscopic lumbar discectomy: Technical tips to prevent complications. Expert. Rev. Med. Devices 2012, 9, 361–366. [Google Scholar] [CrossRef]
- He, S.; Sun, Z.; Wang, Y.; Ma, D.; Tan, W.; Lai, J. Combining YESS and TESSYS techniques during percutaneous transforaminal endoscopic discectomy for multilevel lumbar disc herniation. Medicine 2018, 97, e112140. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Merk, H. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: A prospective, randomized, controlled study. Spine 2008, 33, 931–939. [Google Scholar] [CrossRef]
- Gibson, J.N.; Cowie, J.G.; Iprenburg, M. Transforaminal endoscopic spinal surgery: The future ‘gold standard’ for discectomy?—A review. Surgeon 2012, 10, 290–296. [Google Scholar] [CrossRef]
- Pan, L.; Zhang, P.; Yin, Q. Comparison of tissue damages caused by endoscopic lumbar discectomy and traditional lumbar discectomy: A randomised controlled trial. Int. J. Surg. 2014, 12, 534–537. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Russian | Italian | |
|---|---|---|---|
| Number of patients | 183 | 139 | 44 |
| Age | 39.4/38 (31–46) | ||
| Sex | female—99 (54%), male—84 (46%) | female—75 (53.9%), male—64 (46.1%) | female—24 (54.5%), male—20 (45.5%) |
| Body mass index (BMI) | 28.1/27.4 (23.3–30.9) | ||
| Overweight | 29 (15.8%) | 18 (12.9%) | 11 (25%) |
| Level | Number | % |
|---|---|---|
| Th12-L1 | 1 | 0.5% |
| L2–3 | 2 | 1.1% |
| L3–4 | 14 | 7.7% |
| L4–5 | 82 | 44.8% |
| L5-S1 | 84 | 45.9% |
| Follow-Up 36.1/36 [23; 50.2] Months | |||||
|---|---|---|---|---|---|
| Before Surgery (183) | The Day after Surgery (183) | Follow-Up (183) Months | p (Before Surgery—The Day after Surgery) | p (Before Surgery—Follow-Up) | |
| VAS spine | 4/4 (2–6) | 1/0 (0–2) | 1.2/1 (0–2) | <10−15 | <10−14 |
| VAS leg | 6.4/7 (5–8) | 0.8/0 (0–1) | 0.6/0 (0–0) | <10−15 | <10−15 |
| ODI | 60.8/60 (48–72) | - | 6.2/2 (0–10) | - | <10−15 |
| McNab (excellent, good, fair, poor); number—percent | - - | (77, 95, 7, 2)– (43, 52, 4, 1)% | (53, 67, 18, 1)– (38, 48, 13, 1)% | - - | - - |
| Before Surgery—The Day after Surgery | Before Surgery—Follow-Up | |
|---|---|---|
| VAS leg/MCID | −3.6/−3.8 (−4.4–−3.1) | −3.7/−3.8 (−5–−3.1) |
| Δ VAS leg < −1.6 | 93% (170 of 183) | 93% (170 of 183) |
| VAS spine/MCID | −2.5/−2.5 (−4.2–−0.8) | −2.2/−2.5 (−4.2–0) |
| Δ VAS spine < −1.2 | 67% (122 of 183) | 66% (121 of 183) |
| ODI/MCID | - | −4.3/−4.2 (−5.1–−3.2) |
| Δ ODI < −12.8 | - | 99% (138 of 139) |
| Type | Type of Complication | Total Number | First Year * | Later On |
|---|---|---|---|---|
| I | Nerve root damage without neurological deficite | 4 | 3 | 1 |
| Unintended durotomy | 1 | 1 | 0 | |
| Total of type I 6 (3.2%) | 5 (2.7%) | 1 (0.5%) | ||
| II | Hypalgesia L5 contralateral | 1 | 1 | 0 |
| L4 neuropathic pain | 1 | 0 | 1 | |
| Retroperitoneal hematoma (conservative treatment) | 1 | 0 | 1 | |
| Nerve root damage with paresis in the foot | 1 | 1 | 0 | |
| Hypesthesia L5 | 1 | 0 | 1 | |
| Total of type II 5 (2.7%) | 2 (1%) | 3 (1.6%) | ||
| IIIb | Early disc herniation recurrence (before 90 days after surgery) | 4 | 3 | 1 |
| Unresolved nerve root compression (before 90 days after surgery) | 2 | 2 | 0 | |
| Recurrent disc herniation (90 days after surgery) | 4 | 2 | 2 | |
| Adjacent segment disease | 1 | 0 | 1 | |
| Total of type III 11 (6%) | 7 (3.8%) | 4 (2.1%) | ||
| Total of complications 22 (12%) | 14 (7.6%) | 8 (4.3%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spallone, A.; Khalepa, R.V.; Amelina, E.; Asif ogly, A.M. Endoscopic Lumbar Disc Surgery Experience with the TESSYS Technique in 253 Case Series. J. Clin. Med. 2024, 13, 1911. https://doi.org/10.3390/jcm13071911
Spallone A, Khalepa RV, Amelina E, Asif ogly AM. Endoscopic Lumbar Disc Surgery Experience with the TESSYS Technique in 253 Case Series. Journal of Clinical Medicine. 2024; 13(7):1911. https://doi.org/10.3390/jcm13071911
Chicago/Turabian StyleSpallone, Aldo, Roman Vladimirovich Khalepa, Evgeniya Amelina, and Amrakh Magerramov Asif ogly. 2024. "Endoscopic Lumbar Disc Surgery Experience with the TESSYS Technique in 253 Case Series" Journal of Clinical Medicine 13, no. 7: 1911. https://doi.org/10.3390/jcm13071911
APA StyleSpallone, A., Khalepa, R. V., Amelina, E., & Asif ogly, A. M. (2024). Endoscopic Lumbar Disc Surgery Experience with the TESSYS Technique in 253 Case Series. Journal of Clinical Medicine, 13(7), 1911. https://doi.org/10.3390/jcm13071911