
Comparison of the Determinants of the “Chronic Obstructive Pulmonary Disease Assessment Test” (CAT) and the “Asthma Control Test” (ACT) in Patients with Asthma–COPD Overlap

 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of This Study
2.2. Participants
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Study Population
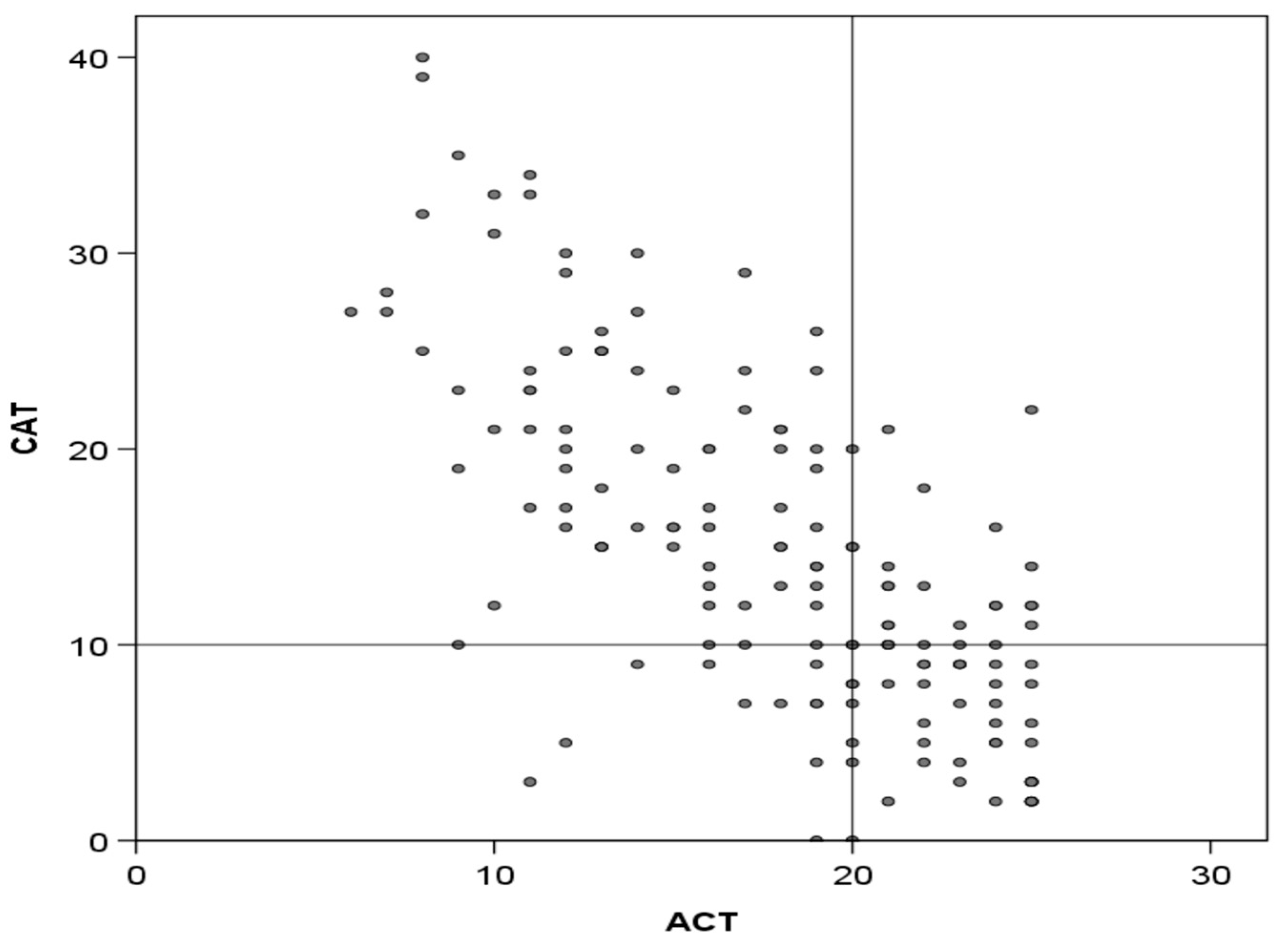
3.2. CAT and ACT Scores and Their Correlation
3.3. Correlations Between CAT and ACT Scores and Markers of Disease Severity
3.4. Factors Significantly Associated with CAT and ACT Scores: Univariate and Multivariate Analyses
3.5. Predictive Values of the CAT and ACT Scores for Exacerbations
3.6. Discordance Between the CAT and ACT Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castillo, E.G.; Pérez, T.A.; Peláez, A.; González, P.P.; Miravitlles, M.; Alfageme, I.; Casanova, C.; Cosío, B.G.; de Lucas, P.; García-Río, F.; et al. Trends of COPD in Spain: Changes Between Cross Sectional Surveys 1997, 2007 and 2017. Arch. Bronconeumol. 2023, 59, 142–151. [Google Scholar] [CrossRef] [PubMed]
- GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Postma, D.S.; Rabe, K.F. The asthma-COPD overlap syndrome. N. Engl. J. Med. 2015, 373, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Mekov, E.; Nuñez, A.; Sin, D.D.; Ichinose, M.; Rhee, C.K.; Maselli, D.J.; Coté, A.; Ulrik, C.S.; Maltais, F.; Anzueto, A.; et al. Update on Asthma-COPD Overlap (ACO): A Narrative Review. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 1783–1799. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Steiling, K.; van den Berge, M.; Hijazi, K.; Hiemstra, P.S.; Postma, D.S.; Lenburg, M.E.; Spira, A.; Woodruff, P.G. Asthma-COPD overlap: Clinical relevance of genomic signatures of Type 2 inflammation in COPD. Am. J. Respir. Crit. Care Med. 2015, 191, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Hardin, M.; Cho, M.; McDonald, M.-L.; Beaty, T.; Ramsdell, J.; Bhatt, S.; van Beek, E.J.; Make, B.J.; Crapo, J.D.; Silverman, E.K.; et al. The clinical and genetic features of COPD-asthma overlap syndrome. Eur. Respir. J. 2014, 44, 341–350. [Google Scholar] [CrossRef]
- Leung, J.M.; Sin, D.D. Asthma-COPD overlap syndrome: Pathogenesis, clinical features, and therapeutic targets. BMJ 2017, 358, j3772. [Google Scholar] [CrossRef]
- Alcázar-Navarrete, B.; Díaz-Lopez, J.M.; García-Flores, P.; Ortega-Antelo, M.; Aguilar-Cruz, I.; Ruiz-Rodríguez, O.; Santiago-Diaz, P.; Palacios, P.J.R. T2 Biomarkers as Predictors of Exacerbations of Chronic Obstructive Pulmonary Disease. Arch. Bronconeumol. 2022, 58, 595–600. [Google Scholar] [CrossRef]
- Plaza, V.; Álvarez, F.; Calle, M.; Casanova, C.; Cosío, B.G.; López-Viña, A.; de Llano, L.P.; Quirce, S.; Román-Rodríguez, M.; Soler-Cataluña, J.J.; et al. Consensus on the Asthma-COPD Overlap Syndrome (ACOS) between the Spanish COPD Guidelines (GesEPOC) and the Spanish Guidelines on the Management of Asthma (GEMA). Arch. Bronconeumol. 2017, 53, 443–449. [Google Scholar] [CrossRef]
- Koblizek, V.; Chlumsky, J.; Zindr, V.; Neumannova, K.; Zatloukal, J.; Zak, J.; Sedlak, V.; Kocianova, J.; Zatloukal, J.; Hejduk, K.; et al. Chronic Obstructive Pulmonary Disease: Official diagnosis and treatment guidelines Biomed of the Czech Pneumological and Phthisiological society: A novel phenotypic approach to COPD with patient oriented care. Pap. Med. Fac. Univ. Palacky Olomouc. Czech Repub. 2013, 157, 189–201. [Google Scholar] [CrossRef]
- Kankaanranta, H.; Harju, T.; Kilpeläinen, M.; Mazur, W.; Lehto, J.T.; Katajisto, M.; Peisa, T.; Meinander, T.; Lehtimäki, L. Diagnosis and pharmacotherapy of Stable Chronic Obstructive Pulmonary Disease: The Finish Guidelines. Basic Clin. Pharmacol. Toxicol. 2015, 116, 291–307. [Google Scholar] [CrossRef] [PubMed]
- Mahboub, B.; Vats, M.; Alzaabi, A.; Iqbal, M.N.; Safwat, T.; Al-Hurish, F.; Miravitlles, M.; Singh, D.; Al-Asad, K.; Zein-El-Dine, S.; et al. Joint Statament for the diagnosis, management, and prevention of chronic obstructive pulmonary disease for Gulf Cooperation Council countries and Middle East-North Africa region. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2869–2890. [Google Scholar] [CrossRef]
- Krishnan, J.A.; Nibber, A.; Chisholm, A.; Price, D.; Bateman, E.D.; Bjermer, L.; van Boven, J.F.M.; Brusselle, G.; Costello, R.W.; Dandurand, R.J.; et al. Prevalence and Characteristics of Asthma–Chronic Obstructive Pulmonary Disease Overlap in Routine Primary Care Practices. Ann. Am. Thorac. Soc. 2019, 16, 1143–1150. [Google Scholar] [CrossRef]
- Cosio, B.G.; Soriano, J.B.; López-Campos, J.L.; Calle-Rubio, M.; Soler-Cataluna, J.J.; De-Torres, J.P.; Marín, J.M.; Martínez-Gonzalez, C.; de Lucas, P.; Mir, I.; et al. Defining the Asthma-COPD Overlap Syndrome in a COPD Cohort. Chest 2016, 149, 45–52. [Google Scholar] [CrossRef]
- Hernández, L.C.; Eraso, C.C.; Ruiz-Duque, B.; Arranz, M.A.; Martín, E.M.; Acuña, C.C.; Lopez-Campos, J.L. Deconstructing Phenotypes in COPD: An Analysis of the TRACE Cohort. Arch. Bronconeumol. 2022, 58, 30–34. [Google Scholar] [CrossRef]
- Wurst, K.E.; Rheault, T.R.; Edwards, L.; Tal-Singer, R.; Agusti, A.; Vestbo, J. A comparison of COPD patients with and without ACOS in the ECLIPSE study. Eur. Respir. J. 2016, 47, 1559–1562. [Google Scholar] [CrossRef]
- Kauppi, P.; Kupiainen, H.; Lindqvist, A.; Tammilehto, L.; Kilpeläinen, M.; Kinnula, V.L.; Haahtela, T.; Laitinen, T. Overlap syndrome of asthma and COPD predicts low quality of life. J. Asthma. 2011, 48, 279–285. [Google Scholar] [CrossRef]
- Menezes, A.M.B.; de Oca, M.M.; Pérez-Padilla, R.; Nadeau, G.; Wehrmeister, F.C.; Lopez-Varela, M.V.; Muiño, A.; Jardim, J.R.B.; Valdivia, G.; Tálamo, C.; et al. Increased risk of exacerbation and hospitalization in subjects with an overlap phenotype: COPD-asthma. Chest 2014, 145, 297–304. [Google Scholar] [CrossRef]
- Suzuki, M.; Makita, H.; Konno, S.; Shimizu, K.; Kimura, H.; Nishimura, M. Asthma-like features and clinical course of chronic obstructive pulmonary disease. An analysis from the Hokkaido COPD cohort study. Am. J. Respir. Crit. Care Med. 2016, 194, 1358–1365. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Arch. Bronconeumol. 2023, 59, 232–248. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Calle, M.; Molina, J.; Almagro, P.; Gómez, J.-T.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; López-Campos, J.L.; Riesco, J.A.; et al. Spanish COPD Guidelines (GesEPOC) 2021: Updated Pharmacological treatment of stable COPD. Arch. Bronconeumol. 2022, 58, 68–91. [Google Scholar] [CrossRef]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Divo, M.; Cote, C.; de Torres, J.P.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.; Zulueta, J.; Cabrera, C.; Zagaceta, J.; Hunninghake, G.; et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2012, 186, 155–161. [Google Scholar] [CrossRef]
- Soler-Cataluña, J.J.; Martínez-García, M.A.; Sánchez, L.S.; Tordera, M.P.; Sánchez, P.R. Severe exacerbations and BODE index: Two independent risk factors for death in male COPD patients. Respir. Med. 2009, 103, 692–699. [Google Scholar] [CrossRef]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Monserrat, S.; Herdman, M.; Segura, A. La versión española del EuroQoL: Descripción y aplicaciones. Med. Clin. 1999, 112, 79–86. (In Spanish) [Google Scholar]
- Esquinas, C.; Ramon, M.A.; Nuñez, A.; Molina, J.; Quintano, J.A.; Roman-Rodríguez, M.; Naberan, K.; Llor, C.; Roncero, C.; Miravitlles, M.; et al. Correlation between disease severity factors and EQ-5D utilities in chronic obstructive pulmonary disease. Qual. Life Res. 2020, 29, 607–617. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Tsiligianni, I.G.; van der Molen, T.; Moraitaki, D.; Lopez, I.; Kocks, J.W.; Karagiannis, K.; Siafakas, N.; Tzanakis, N. Assessing health status in COPD. A head-to-head comparison between the COPD Assessment Test (CAT) and the Clinical COPD Questionnaire (CCQ). BMC Pulm. Med. 2012, 12, 20. [Google Scholar]
- Ringbaek, T.; Martinez, G.; Lange, P. A comparison of the assessment of quality of life with CAT, CCQ, and SGRQ in COPD patients participating in pulmonary rehabilitation. J. Chronic Obstr. Pulm. Dis. 2012, 9, 12–15. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, B.C.P.; Svedsater, H.; Heddini, A.; Nelsen, L.; Balradj, J.S.; Alleman, C. Relationship between the Asthma Control Test (ACT) and other outcomes: A targeted literature review. BMC Pulm. Med. 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021. Executive Summary and Rationale for Key Changes. Arch. Bronconeumol. 2022, 58, 35–51. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Brusselle, G.G.; Canonica, G.W.; Jackson, D.J.; Nair, P.; Buhl, R.; Virchow, J.C. Disease-modifying anti-asthmatic drugs. Lancet 2022, 399, 1664–1668. [Google Scholar] [CrossRef]
- Miravitlles, M.; Molina, J.; Quintano, J.A.; Campuzano, A.; Pérez, J.; Roncero, C. Depressive status explains a significant amount of the variance in COPD assessment test (CAT) scores. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 823–831. [Google Scholar] [CrossRef]
- Miravitlles, M.; Koblizek, V.; Esquinas, C.; Milenkovic, B.; Barczyk, A.; Tkacova, R.; Somfay, A.; Zykov, K.; Tudoric, N.; Kostov, K.; et al. Determinants of CAT (COPD Assessment Test) scores in a population of patients with COPD in central and Eastern Europe: The POPE study. Respir. Med. 2019, 150, 141–148. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Mohme, S.N.; Stoll, P.; Virchow, J.C. Response to Various Biologics in Patients with Both Asthma and Chronic Obstructive Pulmonary Disease. Respiration 2023, 102, 986–990. [Google Scholar] [CrossRef]
- Pavord, I.D.; Chanez, P.; Criner, G.J.; Kerstjens, H.A.; Korn, S.; Lugogo, N.; Martinot, J.-B.; Sagara, H.; Albers, F.C.; Bradford, E.S.; et al. Mepolizumab for Eosinophilic Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2017, 377, 1613–1629. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria | N | % |
|---|---|---|
| Blood eosinophil count (BEC) > 300 cells/μL | 61 | 38.9 |
| Criteria of asthma | 28 | 17.8 |
| Criteria of asthma + BEC > 300 cells/μL | 26 | 16.6 |
| Bronchodilator test (BDT) > 15% and 400 mL | 22 | 14 |
| Criteria of asthma + BDT > 15% and 400 mL | 12 | 7.6 |
| BEC > 300 cells/μL + BDT > 15% and 400 mL | 5 | 3.2 |
| All three criteria | 3 | 1.9 |
| Variables | All (n = 157) | Concordant Poor Control, ACT < 20 and CAT > 10 (n = 78) | Concordant Good Control, ACT > 20 and CAT < 10 (n = 40) | Discordant (n = 39) | p-Value |
|---|---|---|---|---|---|
| Age, mean (SD) | 63.3 (9) | 61.9 (8.7) | 63.9 (8.1) | 65.5 (10.2) | 0.041 |
| Sex (male), n (%) | 109 (69.4) | 51 (65.4) | 28 (70) | 30 (77) | 0.622 |
| Smoker, n (%) Ex-smoker, n (%) | 47 (29.9) 110 (70) | 25 (32) 53 (67) | 11 (27.5) 29 (72.5) | 11 (28.2) 28 (71.8) | 0.952 |
| Smoking pack-years, mean (SD) | 55.4 (154.5) | 66 (218) | 48.1 (24.9) | 41.7 (24.7) | 0.416 |
| BMI, mean (SD) | 27.7 (5.4) | 28.4 (5.9) | 26.9 (4.3) | 27 (5.1) | 0.115 |
| Total Charlson Index Score, mean (SD) | 5.3 (2.3) | 4.6 (2) | 5.8 (2.1) | 6.1 (2.7) | 0.018 |
| COTE Index Score, mean (SD) | 1.5 (2.4) | 1.6 (2.5) | 1 (2) | 1.8 (2.6) | 0.144 |
| BODEx, mean (SD) | 2.2 (1.8) | 3 (1.8) | 1.3 (1.3) | 1.7 (1.5) | <0.001 |
Exacerbations last year, median (IQR)
| 1 (0; 2) 1 (0; 2) 0 (0; 1) | 2 (1; 2) 1 (0; 2) 0 (0; 1) | 0 (0; 1) 0 (0; 1) 0 (0; 0) | 1 (0; 2) 0 (0; 1) 0 (0; 1) | <0.001 0.003 0.163 |
| mMRC dyspnoea, median (IQR) | 1 (1; 2) | 2 (1; 2) | 0.8 (0.8) | 1.3 (0.7) | <0.001 |
| Minutes walked/day, mean (SD) | 75 (85.6) | 74.6 (120.7) | 84.5 (45.3) | 63.8 (36.6) | 0.069 |
| Postbronchodilator FEV1 (mL) Postbronchodilator FEV1 (%) Postbronchodilator FVC (mL) Postbronchodilator FVC (%) Postbronchodilator FEV1/FVC (%) Positive bronchodilator test, n (%) | 1704 (643) 59.7 (20.5) 3117 (921) 86 (20) 54 (11.2) 59 (43.7) | 1566 (678) 55 (20.2) 2930 (1114) 81 (21.5) 52 (12.4) 28 (44.4) | 1778 (583) 64.6 (19.6) 3182 (881) 88.8 (20.5) 53.7 (11.2) 19 (52.8) | 1862 (625) 61.5 (21.3) 3194 (833) 85.6 (19.1) 57 (8.5) 12 (33.3) | 0.047 0.035 0.381 0.117 0.032 0.248 |
| 6MWD, metres, mean (SD) | 410 (120) | 397 (115) | 453 (90) | 396.4 (145) | 0.120 |
| Blood eosinophils, mean (SD) CRP, mean (SD) Fibrinogen, mean (SD) | 317.7 (270) 3.4 (6.1) 392 (573) | 280.9 (230) 3.7 (7.5) 442 (822) | 336 (327.8) 3.5 (4.6) 332 (179) | 371.3 (277) 2.9 (4.3) 363 (153) | 0.277 0.783 0.450 |
| LAMA LABA/ICS LABA/LAMA LABA/LAMA/ICS Montelukast Azithromycin Mucolytics | 3 (1.9) 27 (17.4) 23 (14.8) 101 (65.2) 20 (12.7) 10 (6.4) 7 (4.5) | 0 8 (10.4) 7 (9.1) 62 (80.5) 10 (12.8) 9 (11.5) 4 (5.1) | 2 (5.1) 9 (23.1) 7 (17.9) 20 (51.3) 7 (17.9) 1 (2.6) 3 (7.7) | 1 (2.6) 10 (25.6) 9 (23.1) 19 (48.7) 3 (7.5) 0 0 | 0.158 0.069 0.111 <0.001 0.379 0.028 0.234 |
| EQ-5D EVA, mean (SD) | 61.9 (20.4) | 53.1 (19.6) | 74.1 (16.4) | 67.2 (17.7) | <0.001 |
| EQ-5D index, mean (SD) | 0.8 (0.2) | 0.7 (0.2) | 0.9 (0.15) | 0.8 (0.2) | <0.001 |
| HADS—Anxiety, mean (SD) | 5.8 (4.5) | 7.8 (4.6) | 3.2 (3.5) | 4.4 (2.9) | <0.001 |
| HADS—Depression, mean (SD) | 4.6 (4.5) | 6.9 (4.9) | 1.9 (2.5) | 2.8 (2.9) | <0.001 |
| Total HADS, mean (SD) | 10.4 (8.5) | 14.6 (9) | 5.2 (5.3) | 7.2 (5) | <0.001 |
| CAT score, mean (SD) | 14.5 (8.7) | 20.9 (7) | 5.4 (2.7) | 11.1 (4.6) | <0.001 |
| ACT score, mean (SD) | 17.9 (5.2) | 13.8 (3.6) | 23.1 (1.8) | 20.6 (3.6) | <0.001 |
| CAT r Spearman (p-Value) | ACT r Spearman (p-Value) | |
|---|---|---|
| Total number of exacerbations | 0.237 (0.003) | −0.337 (<0.001) |
| Total number of moderate exacerbations | 0.192 (0.016) | −0.277 (<0.001) |
| Total number of severe exacerbations | 0.179 (0.026) | −0.249 (0.002) |
| BODEx | 0.387 (<0.001) | −0.484 (<0.001) |
| Postbronchodilator FVC (% pred) | −0.141 (0.086) | 0.127 (0.121) |
| Postbronchodilator FEV1 (% pred) | −0.206 (0.011) | 0.234 (0.004) |
| Postbronchodilator FEV1/FVC (%) | −0.123 (0.134) | 0.169 (0.039) |
| Dyspnoea (mMRC) | 0.539 (<0.001) | −0.562 (<0.001) |
| Metres walked (6MWD) | −0.122 (0.171) | 0.174 (0.050) |
| EQ-5D EVA, mean (SD) | −0.410 (p < 0.001) | 0.526 (p < 0.001) |
| EQ-5D index, mean (SD) | −0.491 (p < 0.001) | 0.524 (p <0.001) |
| HADS—Anxiety, mean (SD) | 0.514 (p < 0.001) | −0.535 (p < 0.001) |
| HADS—Depression, mean (SD) | 0.572 (<0.001) | −0.508 (p < 0.001) |
| Total HADS, mean (SD) | 0.573 (p < 0.001) | −0.564 (p < 0.001) |
| ACT | ||||||
|---|---|---|---|---|---|---|
| Simple | Multiple | |||||
| Variables | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value |
| Age | 0.035 | −0.056 to 0.127 | 0.446 | |||
| BMI | −0.014 | −0.168 to 0.140 | 0.857 | |||
| EQ-5D index | 13.172 | 10.134 to 16.211 | <0.001 | 5.316 | 2.058 to 8.575 | 0.002 |
| HADS total | −0.349 | −0.430 to −0.269 | <0.001 | −0.188 | −0.270 to −0.106 | <0.001 |
| Total Charlson Index Score | 0.356 | −0.007 to 0.720 | 0.055 | |||
| Metres walked (6MWD) | 0.003 | −0.007 to 0.013 | 0.596 | |||
| Number of exacerbations | −1.045 | −1.519 to −0.571 | <0.001 | −0.614 | −1.035 to −0.193 | 0.005 |
| Dyspnoea (mMRC) | −3.066 | −3.782 to −2.351 | <0.001 | −2.784 | −3.509 to −2.058 | <0.001 |
| Postbronchodilator FEV1 (%) | 0.058 | 0.019 to 0.097 | 0.004 | |||
| Sex, male | −0.744 | −2.531 to 1.042 | 0.412 | |||
| Smoking | −0.179 | −1.980 to 1.621 | 0.844 | |||
| CAT | ||||||
| Simple | Multiple | |||||
| Variables | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value |
| Age | −0.140 | −0.292 to 0.012 | 0.071 | −0.140 | −0.267 to −0.012 | 0.033 |
| BMI | 0.122 | −0.134 to 0.378 | 0.348 | |||
| EQ-5D index | −18.831 | −24.227 to −13.434 | <0.001 | |||
| HADS total | 0.660 | 0.535 to 0.786 | <0.001 | 0.527 | 0.404 to 0.650 | <0.001 |
| Total Charlson Index Score | −0.814 | −1.415 to −0.212 | 0.008 | |||
| Metres walked (6MWD) | 0.004 | −0.012 to 0.021 | 0.612 | |||
| Number of exacerbations | 1.247 | 0.431 to 2.064 | 0.003 | |||
| Dyspnoea (mMRC) | 4.920 | 3.701 to 6.138 | <0.001 | 4.919 | 3.715 to 6.124 | <0.001 |
| Postbronchodilator FEV1(%) | −0.082 | −0.147 to −0.016 | 0.015 | |||
| Sex, male | 0.880 | −2.112 to 3.871 | 0.562 | |||
| Smoking | 0.360 | −2.652 to 3.372 | 0.814 | |||
| Variables | Good CAT (<10) and Poor ACT (<20) (n = 11) | Poor CAT (>10) and Good ACT (≥20) (n = 28) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 70.4 (8.8) | 63.6 (10.2) | 0.078 |
| Sex, (male), n (%) | 8 (72.7) | 22 (78.6) | 0.679 |
| Smoker, n (%) Ex-smoker, n (%) | 3 (27.3) 8 (72.7) | 8 (28.6) 20 (71.4) | 0.935 |
| Smoking pack-years, mean (SD) | 40.2 (26.3) | 42.3 (24.5) | 0.541 |
| BMI, mean (SD) | 23.9 (4.7) | 28.1 (4.8) | 0.031 |
| Total Charlson Index Score, mean (SD) | 6.8 (3.2) | 5.9 (2.6) | 0.533 |
| COTE Index Score, mean (SD) | 2.7 (2.1) | 1.4 (2.7) | 0.014 |
| BODEx, mean (SD) | 2 (1.7) | 1.6 (1.4) | 0.554 |
Total exacerbations last year, median (IQR)
| 1 (0; 2) 1 (0; 1) 0 (0; 1) | 0.5 (0; 2) 0 (0;1.5) 0 (0; 0) | 0.676 0.595 0.436 |
| mMRC dyspnoea, mean (SD) | 1.5 (0.5) | 1.3 (0.8) | 0.390 |
| Minutes walked/day, mean (SD) | 67.9 (35.8) | 62.6 (37.5) | 0.652 |
| FEV1 (mL) FEV1 (%) FVC (mL) FVC (%) FEV1/FVC (%) Positive bronchodilator test | 1694 (616) 60.4 (16.7) 3121 (763) 92.9 (16.1) 51 (8.9) 6 (60) | 1922.5 (628) 61.9 (23.1) 3220.4 (868) 82.9 (19.7) 59.2 (7.4) 6 (23.1) | 0.075 0.090 0.273 0.894 0.015 0.035 |
| 6MWD, metres, mean (SD) | 359 (154) | 409 (143) | 0.509 |
| Blood eosinophil count, mean (SD) CRP, mean (SD) Fibrinogen, mean (SD) | 392 (233) 2.9 (2.9) 438 (115) | 363 (296) 3 (4.7) 336 (158) | 0.294 0.571 0.124 |
| EQ-5D EVA, mean (SD) | 56.6 (20.3) | 71.4 (15) | 0.042 |
| EQ-5D index, mean (SD) | 0.8 (0.1) | 0.8 (0.2) | 0.504 |
| HADS score—anxiety, mean (SD) | 5.1 (2.5) | 4.1 (3.1) | 0.086 |
| HADS score—depression, mean (SD) | 2.6 (2.5) | 2.9 (3.1) | 0.352 |
| Total HADS score, mean (SD) | 7.6 (4.1) | 7.1 (5.3) | 0.480 |
| CAT sore | 6.1 (2.8) | 13.1 (3.5) | <0.001 |
| ACT score | 16.6 (3) | 22.2 (1.8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljama, C.; Granados, G.; Callejas-González, F.J.; Martínez-Rivera, C.; Pallarés-Sanmartín, A.; Rodríguez-Pons, L.; Cabrera-César, E.; Márquez-Martín, E.; Boldova-Loscertales, A.; Naval-Sendra, E.; et al. Comparison of the Determinants of the “Chronic Obstructive Pulmonary Disease Assessment Test” (CAT) and the “Asthma Control Test” (ACT) in Patients with Asthma–COPD Overlap. J. Clin. Med. 2024, 13, 6367. https://doi.org/10.3390/jcm13216367
Aljama C, Granados G, Callejas-González FJ, Martínez-Rivera C, Pallarés-Sanmartín A, Rodríguez-Pons L, Cabrera-César E, Márquez-Martín E, Boldova-Loscertales A, Naval-Sendra E, et al. Comparison of the Determinants of the “Chronic Obstructive Pulmonary Disease Assessment Test” (CAT) and the “Asthma Control Test” (ACT) in Patients with Asthma–COPD Overlap. Journal of Clinical Medicine. 2024; 13(21):6367. https://doi.org/10.3390/jcm13216367
Chicago/Turabian StyleAljama, Cristina, Galo Granados, Francisco Javier Callejas-González, Carlos Martínez-Rivera, Abel Pallarés-Sanmartín, Laura Rodríguez-Pons, Eva Cabrera-César, Eduardo Márquez-Martín, Ana Boldova-Loscertales, Elsa Naval-Sendra, and et al. 2024. "Comparison of the Determinants of the “Chronic Obstructive Pulmonary Disease Assessment Test” (CAT) and the “Asthma Control Test” (ACT) in Patients with Asthma–COPD Overlap" Journal of Clinical Medicine 13, no. 21: 6367. https://doi.org/10.3390/jcm13216367
APA StyleAljama, C., Granados, G., Callejas-González, F. J., Martínez-Rivera, C., Pallarés-Sanmartín, A., Rodríguez-Pons, L., Cabrera-César, E., Márquez-Martín, E., Boldova-Loscertales, A., Naval-Sendra, E., Abascal-Bolado, B., Cabrera-López, C., Miravitlles, M., Esquinas, C., & Barrecheguren, M. (2024). Comparison of the Determinants of the “Chronic Obstructive Pulmonary Disease Assessment Test” (CAT) and the “Asthma Control Test” (ACT) in Patients with Asthma–COPD Overlap. Journal of Clinical Medicine, 13(21), 6367. https://doi.org/10.3390/jcm13216367