1. Introduction
Frailty, defined as an aging-related syndrome of physiological decline, is characterized by diminished ability to cope with acute stressors. Numerous physical and psychosocial determinants are factored in when defining frailty. Patient frailty has been identified as an independent risk factor for adverse clinical outcomes for a wide array of medical conditions and procedures [
1,
2,
3,
4,
5,
6]. Furthermore, studies have demonstrated that frailty increases healthcare resource utilization and adds to the economic burden on the healthcare sector [
7]. As an example, a UK-based longitudinal study estimated that frailty accounts for an added £5.8 billion/year of healthcare-related expenditure across the country [
8]. Despite its ubiquity and significant impact on healthcare outcomes, quantifying frailty has been rather challenging. The lack of such quantification has continued to be a significant barrier to the incorporation of frailty into medical decision-making and physician stewardship of healthcare resources. Furthermore, in addition to being inaccurate, previously used frailty assessment tools were often criticized for being quite cumbersome. These tools required varying degrees of manual assessment, which led to a lack of objectivity.
Developed by Gilbert et al. using the International Classification of Diseases (ICD) codes, the hospital frailty risk score (HFRS) has revolutionized assessment of frailty, particularly in an inpatient setting [
9]. Using a set of 109 ICD-10 codes that are highly prevalent in frail patients, Gilbert et al. produced a model to weigh the impact of each diagnosis code on frailty. Essentially, an individual’s HFRS is the arithmetic sum of these numeric values. Using this score, the spectrum of frailty can be categorized, making a comparison of individuals in each category possible [
9,
10,
11,
12].
Endoscopic retrograde cholangiopancreatography (ERCP), a vital procedure in the arsenal of therapeutic endoscopists, involves the utilization of a side-viewing endoscope under fluoroscopic guidance to perform a wide variety of interventions for pancreaticobiliary disorders [
13]. Due to its widespread availability and minimally invasive nature, the utilization of ERCP is on the rise [
14]. Advancements in endoscopic techniques and increasing operator experience have led to ensuring the safe use of ERCP for therapeutic purposes [
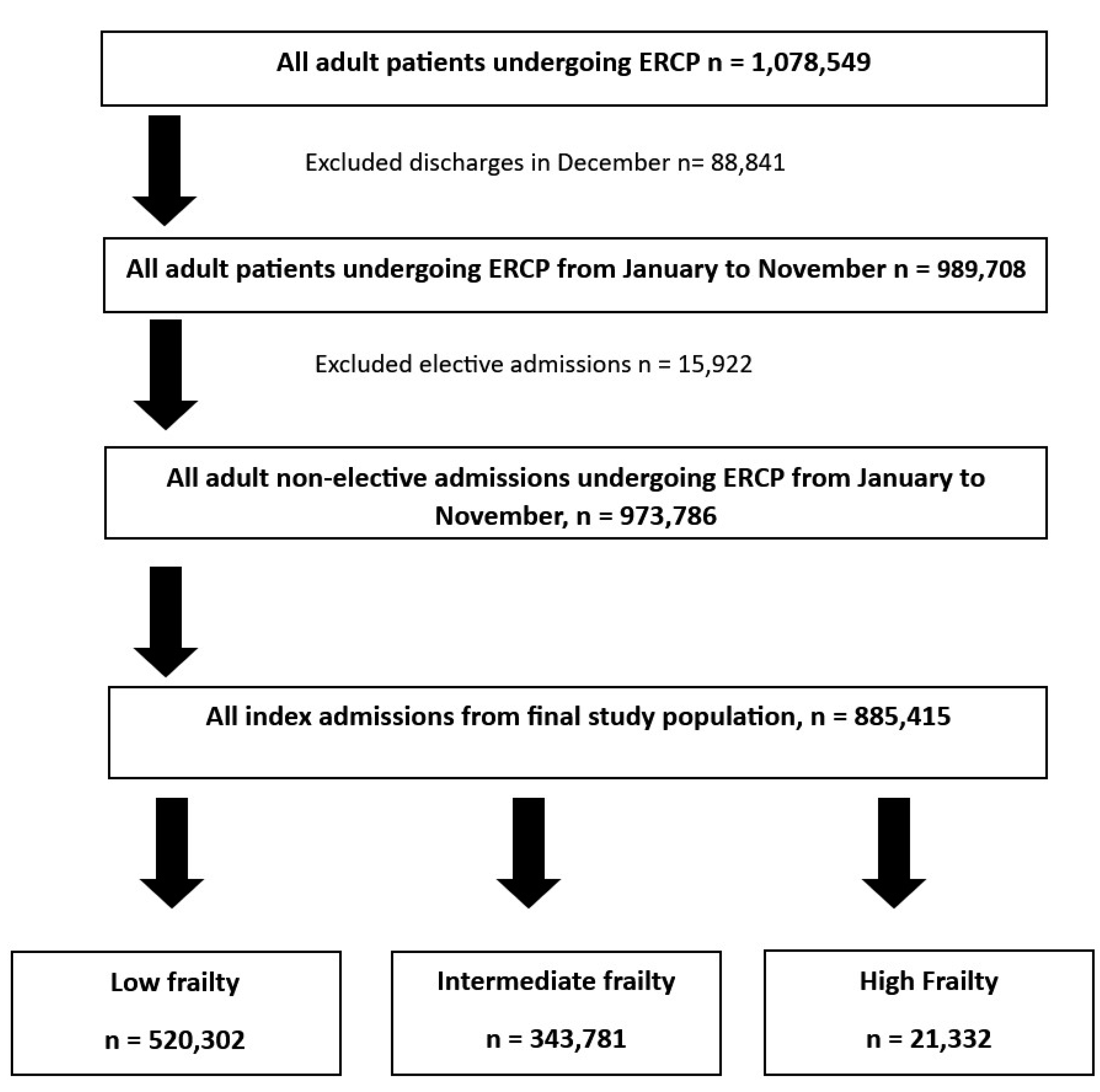
15]. However, there is a significant paucity of data on the impact of frailty in individuals receiving ERCP, particularly in an inpatient setting. Hence, in this study, we aimed to evaluate the utility of the HFRS in predicting outcomes for inpatient use of ERCP. We used one of the largest publicly available healthcare databases, the nationwide readmissions database (NRD), to study the impact of the HFRS on readmission rates, inpatient mortality, and the healthcare burden in the United States (US).
4. Discussion
Our study highlights that increasing frailty is associated with an increase in the rate of 30-day readmission in patients undergoing ERCP, ranging from 8.2% to 12.59% based on the degree of frailty. This increase in odds of readmission was higher for females compared to males. Frailty increased readmission rates in all age groups; However, the presence of frailty in younger patients had a more dramatic increase in the odds of 30-day readmissions. Overall, 30-day readmissions had higher odds of mortality compared to index admissions. Furthermore, the THC and LOS increased significantly with higher frailty scores. In clinical practice, quantifying the impact of frailty on outcomes in patients undergoing ERCP is crucial as it allows therapeutic endoscopists to prognosticate such patients and take preemptive measures to reduce the risk of unfavorable outcomes in these high-risk individuals.
Previous studies have established an association between frailty and readmissions rates for numerous pathologies such as chronic pancreatitis, inflammatory bowel disease, heart failure, and many more [
17,
18,
19]. Despite a clinical understanding of the fact that frail individuals have worse clinical outcomes with ERCP, there is limited data on the impact of frailty on ERCP outcomes [
20,
21,
22,
23,
24]. Furthermore, the extent of frailty’s impact on these outcomes is also poorly understood, owing to the dearth of real-world data, which has made operationalizing frailty quite challenging. A possible solution for this could be the effective use of HFRS as a frailty indicator. A major finding of our study was increased 30-day readmission rates for frail patients. This finding is in line with a previously published study in 2017 that had a smaller sample size and demonstrated that frail patients undergoing ERCP experienced a higher readmission rate [
20]. Another 4-year national study also had similar findings to our study as the authors noted that frailty increased the odds of readmission in admissions for acute biliary pancreatitis [
21]. Furthermore, frail patients may have multiple readmissions owing to procedural complications, to which they are more prone compared to the general population [
25,
26,
27,
28]. Like any other medical intervention, ERCP is not without risks, and frailty has emerged as a potential predictor for worse clinical outcomes following ERCP. Additional large prospective studies are required to examine the impact of frailty on the incidence of post-ERCP complications, most importantly post-ERCP pancreatitis. An interesting finding in our study was that of a relatively higher readmission risk with increasing frailty in younger patients. There is a substantial amount of literature evaluating frailty in the aged. However, there is scarcity of data on frailty in the young, making this a relatively challenging aspect to contextualize. This finding of our study sheds light on the importance of addressing frailty in the younger patient population. We hypothesize that the fundamental difference in the etiological basis of frailty in younger patients and the psychosocial impact of such frailty play a key role in this finding. Further prospective studies are essential to selectively study the impact of frailty on young patients undergoing ERCP.
Interestingly, another key finding of our study was that in admissions with a CCI score >1, higher frailty did not increase the odds of readmission. This meant that with an increasing comorbid burden, readmission rates become somewhat similar between frail and non-frail patients. This finding further strengthens the reliability of HFRS and reveals the true impact of frailty in individuals with a lower comorbidity burden. CCI scores have previously been used extensively as predictors of readmission in admissions for biliary pathologies [
29,
30]. However, in patients with lower or no comorbidities, anticipating readmissions becomes more challenging, and limited tools exist to predict readmissions in this subset population. Based on our results, HFRS could prove to be an effective tool for therapeutic endoscopists to screen for and anticipate a higher likelihood of readmission in this subset population.
In our study, we observed that frailty is associated with a significantly higher odds of readmission in females than in males. There are likely multiple reasons for this finding. Firstly, gender-based physiological differences are associated with a higher degree of frailty in women. Low muscle mass and post-menopausal changes attribute a higher degree of frailty to women. Additionally, prior studies have shown that women have a higher risk of post-ERCP complications like post-ERCP pancreatitis [
31], which further increases the short-term readmission risk. There are also studies showing that polypharmacy is more prevalent in women [
32], which further increases the risk of adverse events. Furthermore, frail women, especially elderly women, may have less robust social support than men, which potentially contributes to poorer care post-discharge, which culminates in higher readmission risk. Women also have a higher prevalence of anxiety and depression [
33], which is further worsened by the presence of frailty. This is known to limit optimal post-discharge care, further contributing to a higher readmission burden.
In our study, sepsis was the most commonly identified readmission diagnosis in all three cohorts. This is explained by the association of sepsis with multiple indications for which ERCP is undertaken. These include cholangitis, acute pancreatitis, malignant biliary obstruction, choledocholithiasis with incomplete stone clearance, and so forth. Pancreatic cancer and cholangiocarcinoma were also noted to be significant diagnoses on 30-day readmission. Malignant biliary obstruction can prove to be a therapeutic challenge. ERCP is often undertaken as a measure to provide palliation in this patient population. Owing to the advanced stages at which these malignancies are often diagnosed and the poor therapeutic response encountered in such patients, an inherently high readmission risk is often observed. This is evident in our study as well, where these diagnoses contributed to significant readmission burden across varying degrees of frailty.
Higher frailty is associated with reduced physical activity, multi-morbidity, disability, and adverse outcomes [
34]. These can lead to an increased healthcare burden and utilization, in terms of LOS, THC, and inpatient mortality, as observed in our study. In prior published literature, frailty has been also linked to worse in-hospital outcomes with exposure to operative stress [
35,
36]. A prospective cohort study of 200 patients admitted for acute biliary conditions noted that frail individuals experienced higher rates of mortality and incidence of peri-procedural complications, which translated to longer hospital stays and THC, similar to our study [
28]. This further demonstrates that frail patients require more complex, thorough, and multi-disciplinary care to optimize health at discharge and reduce the burden of readmissions. Furthermore, screening for frailty and addressing modifiable factors may be an important factor in optimizing outcomes and reducing the risk of adverse events following ERCP. Further research is needed to develop and validate frailty-screening tools specifically for ERCP and to determine the most effective interventions to mitigate the impact of frailty on procedural outcomes. A multifaceted approach to improve frailty in this high-risk population is crucial. In our study, we only included non-elective admissions. Such admissions need ERCP on a more time-sensitive basis, compared to elective admissions. While this could limit the potential measures to improve frailty pre-procedurally, there is still scope to implement post-procedural measures to reduce frailty-related adverse outcomes. Physical and nutritional rehabilitation, psychosocial support, and vocational rehabilitation could be utilized in optimizing periprocedural patient outcomes and in reducing readmission burden following ERCP, especially in patients with high frailty. Periprocedural optimization of medical comorbidities could directly have a positive impact on reducing readmission burden. Careful selection of patients for periprocedural antimicrobial therapy and early recognition of infectious complications should be emphasized as patients with high frailty are commonly readmitted with sepsis, as evident in our study. Further prospective studies are necessary to evaluate the impact of such measures on reducing frailty-associated adverse outcomes.
Our study has numerous strengths and some limitations. An important strength of our study is the large study population, which has been derived from one of the largest, multi-ethnic and most inclusive inpatient databases in the US. With the weighted nature of the sample, the results of our study are generalizable and applicable to all index hospitalizations and readmissions in the US, offering therapeutic endoscopists real-world data. Despite these strengths, we acknowledge all the limitations associated with our study. The NRD database does not contain information on the etiology, hospital course, pharmacological data, and other treatment aspects of the disease. It also lacks data on patient selection, pre-procedural evaluation, intra-procedural details, specific procedural techniques utilized during the procedure, operator preferences, and pharmacological aspects of management before, during, or after the procedure. Furthermore, due to the retrospective nature of the study design, all biases associated with retrospective studies are applicable to our study. In performing a multivariate regression analysis while evaluating readmission risk, we were unable to adjust for the reason for readmission, due to the nature of the NIS database. Lastly, the NRD is an administrative database maintained through data collection organizations that use the ICD coding system to store inpatient data. Hence, the possibility of human coding errors cannot be excluded. However, despite these limitations, we believe that the large sample size and a comprehensive analysis technique help us better understand the clinical outcomes of 30-day readmissions of ERCP in the US.
In conclusion, ERCP readmissions are a significant healthcare burden that can lead to patient morbidity, mortality, and decreased quality of life. Frailty is a common co-existent factor in patients undergoing ERCP, and it is vital to recognize its key role in readmissions following ERCP. In this study, we noted that frailty not only increases readmissions but also inpatient mortality, LOS, and THC. Furthermore, females are disproportionately affected. HFRS can serve as a vital tool in predicting adverse outcomes, incorporating a multi-disciplinary approach in patient care and careful patient selection to help improve outcomes in patients undergoing ERCP. Additional large prospective studies are essential to assess the utility of incorporating HFRS into complex clinical decision making in an attempt to identify individuals at higher risk of adverse outcomes.




 ,
, 

{kind=link}