

A Comparison of Hypotension, Bradycardia, and Hypoxia Incidence between the Use of Remimazolam and Other Sedative Agents during Colonoscopy Procedures: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Outcomes
2.3.1. Primary Outcomes
2.3.2. Secondary Outcomes
2.4. Data Extraction
2.5. Data Synthesis
2.6. Risk of Bias
2.7. Assessments of Confidence
3. Results
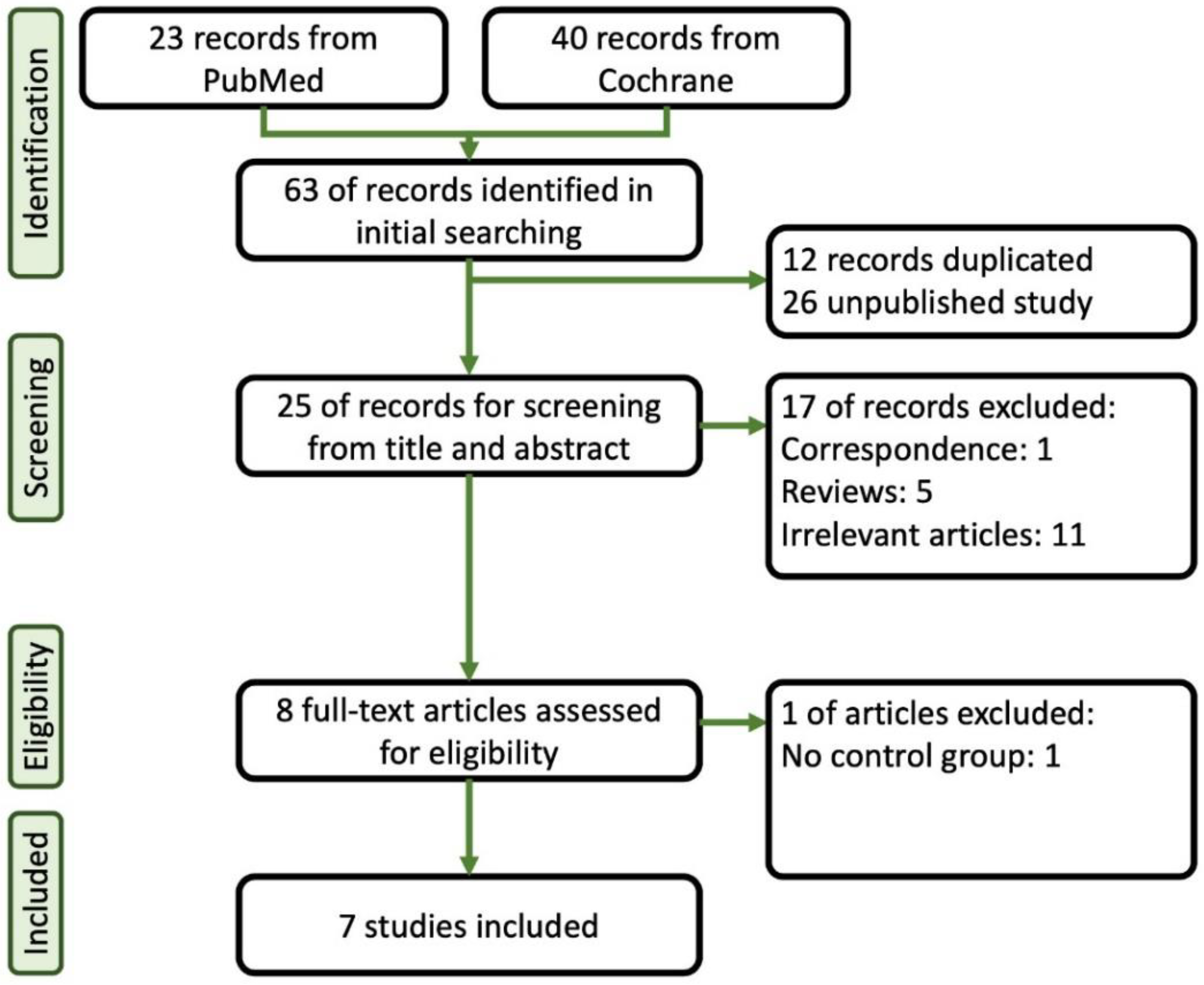
3.1. Search Results
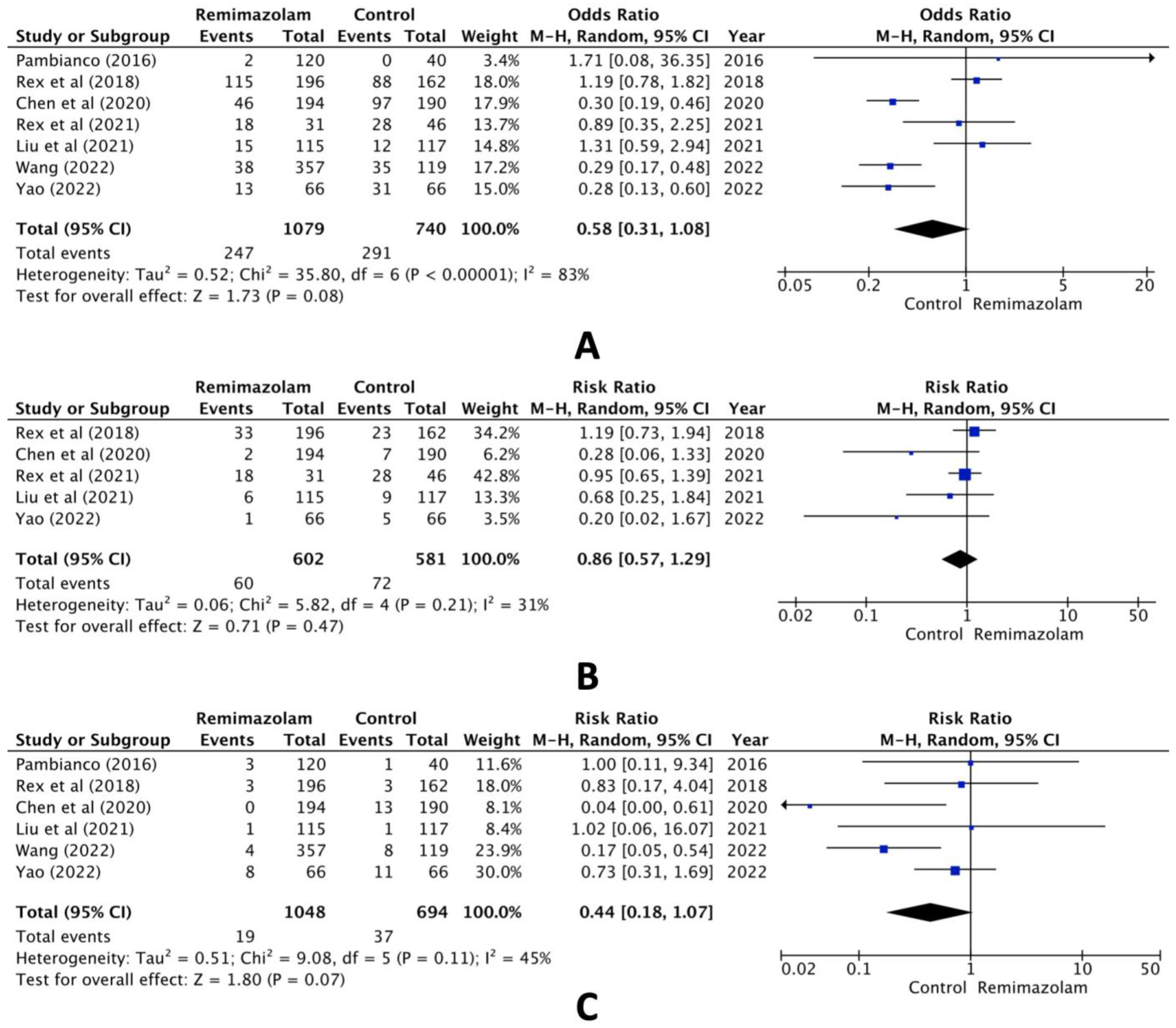
3.2. Primary Outcomes
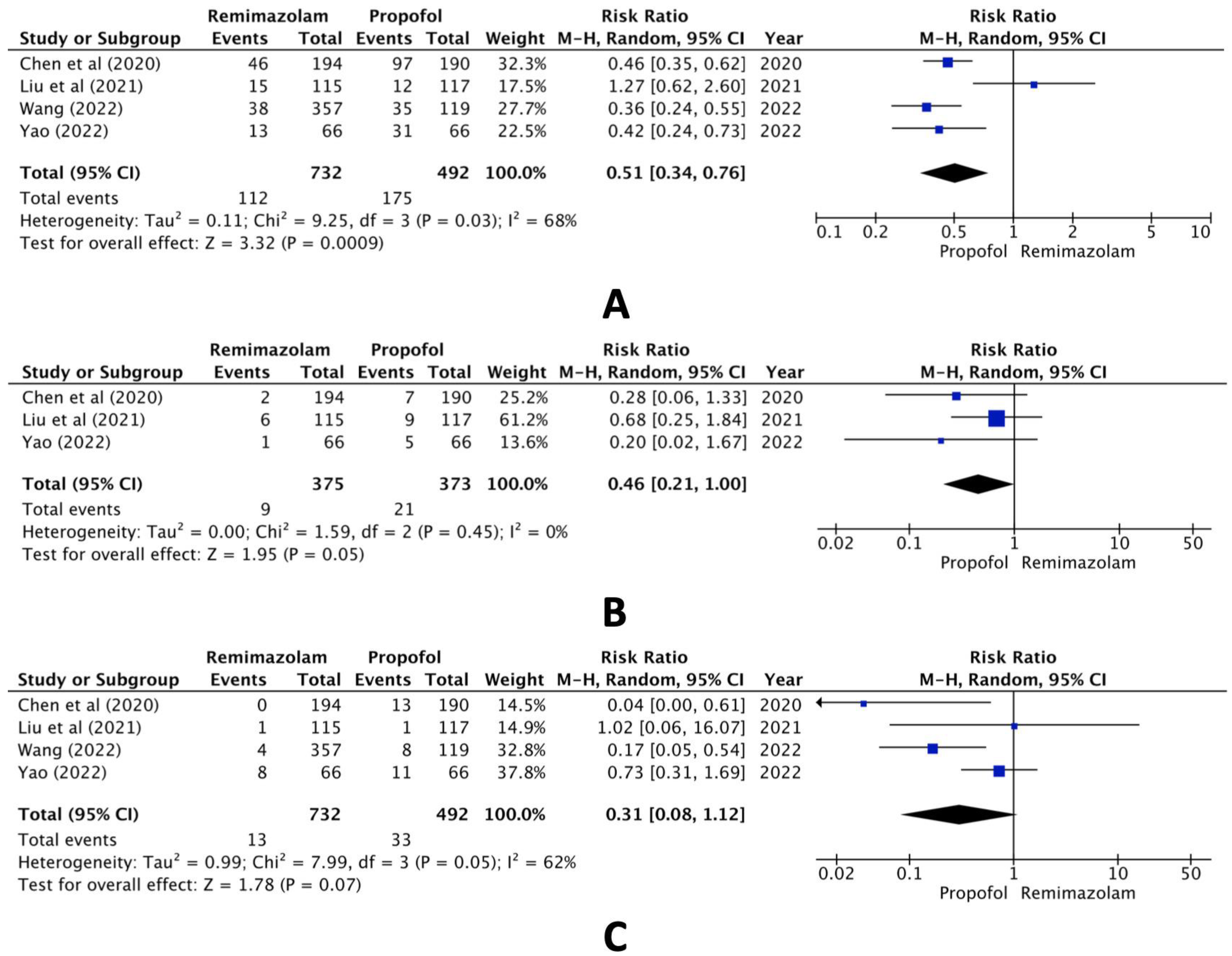
3.3. Secondary Outcomes
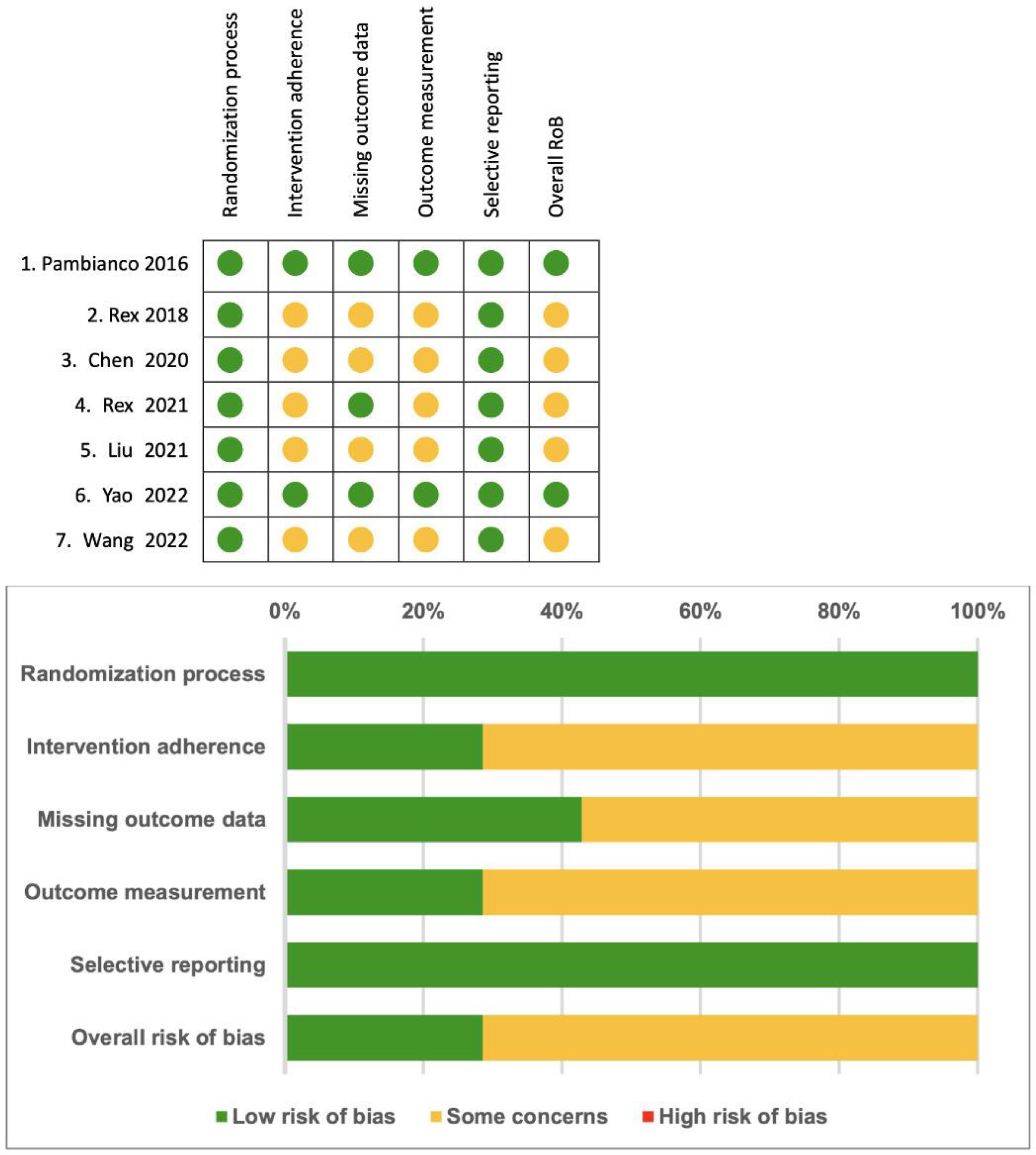
3.4. Risk of Bias
3.5. Assessments of Confidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Goudra, B.G.; Singh, P.M. Remimazolam: The Future of Its Sedative Potential. Saudi J. Anaesth. 2014, 8, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Sneyd, J.R.; Rigby-Jones, A.E. Remimazolam for Anaesthesia or Sedation. Curr. Opin. Anaesthesiol. 2020, 33, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Wang, H.; Yuan, S.; Li, Y.; Jia, Y.; Zhang, Z.; Yan, F.; Wang, Z. Efficacy and Safety of Remimazolam in Endoscopic Sedation—A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 655042. [Google Scholar] [CrossRef] [PubMed]
- Sneyd, J.R.; Absalom, A.R.; Barends, C.R.M.; Jones, J.B. Hypotension during Propofol Sedation for Colonoscopy: A Retrospective Exploratory Analysis and Meta-Analysis. Br. J. Anaesth. 2022, 128, 610–622. [Google Scholar] [CrossRef] [PubMed]
- Murabito, P.; Astuto, M.; Sanfilippo, F.; La Via, L.; Vasile, F.; Basile, F.; Cappellani, A.; Longhitano, L.; Distefano, A.; Li Volti, G. Proactive Management of Intraoperative Hypotension Reduces Biomarkers of Organ Injury and Oxidative Stress during Elective Non-Cardiac Surgery: A Pilot Randomized Controlled Trial. J. Clin. Med. 2022, 11, 392. [Google Scholar] [CrossRef] [PubMed]
- La Via, L.; Vasile, F.; Perna, F.; Zawadka, M. Prediction of Fluid Responsiveness in Critical Care: Current Evidence and Future Perspective. Trends Anaesth. Crit. Care 2024, 54, 101316. [Google Scholar] [CrossRef]
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Jensen, E.T.; Shaheen, N.J.; Barritt, A.S.; Lieber, S.R.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272.e11. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, T.; Khan, A.; Winstead, N. Sedation, Analgesia, and Monitoring. Clin. Colon Rectal Surg. 2010, 23, 014–020. [Google Scholar] [CrossRef]
- Wu, X.; Wang, C.; Gao, H.; Bai, X.; Zhang, Z.; Chen, R.; Huang, X.; An, L.; Yi, J.; Tong, R. Comparison of Remimazolam and Propofol about Safety Outcome Indicators during General Anesthesia in Surgical Patients: A Systematic Review and Meta-Analysis. Minerva Anestesiol. 2023, 89, 553–564. [Google Scholar] [CrossRef]
- Ul-Haque, I.; Shaikh, T.G.; Ahmed, S.H.; Waseem, S.; Qadir, N.A.; Bin Arif, T.; Haque, S.U. Efficacy of Remimazolam for Procedural Sedation in American Society of Anesthesiologists (ASA) I to IV Patients Undergoing Colonoscopy: A Systematic Review and Meta-Analysis. Cureus 2022, 14, e22881. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Pambianco, D.J.; Borkett, K.M.; Riff, D.S.; Winkle, P.J.; Schwartz, H.I.; Melson, T.I.; Wilhelm-Ogunbiyi, K. A Phase IIb Study Comparing the Safety and Efficacy of Remimazolam and Midazolam in Patients Undergoing Colonoscopy. Gastrointest. Endosc. 2016, 83, 984–992. [Google Scholar] [CrossRef]
- Rex, D.K.; Bhandari, R.; Desta, T.; DeMicco, M.P.; Schaeffer, C.; Etzkorn, K.; Barish, C.F.; Pruitt, R.; Cash, B.D.; Quirk, D.; et al. A Phase III Study Evaluating the Efficacy and Safety of Remimazolam (CNS 7056) Compared with Placebo and Midazolam in Patients Undergoing Colonoscopy. Gastrointest. Endosc. 2018, 88, 427–437.e6. [Google Scholar] [CrossRef]
- Chen, S.; Wang, J.; Xu, X.; Huang, Y.; Xue, S.; Wu, A.; Jin, X.; Wang, Q.; Lyu, J.; Wang, S.; et al. The Efficacy and Safety of Remimazolam Tosylate versus Propofol in Patients Undergoing Colonoscopy: A Multicentered, Randomized, Positive-Controlled, Phase III Clinical Trial. Am. J. Transl. Res. 2020, 12, 4594–4603. [Google Scholar] [PubMed]
- Rex, D.K.; Bhandari, R.; Lorch, D.G.; Meyers, M.; Schippers, F.; Bernstein, D. Safety and Efficacy of Remimazolam in High Risk Colonoscopy: A Randomized Trial. Dig. Liver Dis. 2021, 53, 94–101. [Google Scholar] [CrossRef]
- Liu, X.; Ding, B.; Shi, F.; Zhang, Y.; Liu, L.; Sha, Y.; Zhao, T. The Efficacy and Safety of Remimazolam Tosilate versus Etomidate-Propofol in Elderly Outpatients Undergoing Colonoscopy: A Prospective, Randomized, Single-Blind, Non-Inferiority Trial. Drug Des. Dev. Ther. 2021, 15, 4675–4685. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Hu, X.; Bai, N.; Li, L.; Zhang, M.; Cheng, Z.; Guo, Q. Safety and Efficacy of Remimazolam Besylate in Patients Undergoing Colonoscopy: A Multicentre, Single-Blind, Randomized, Controlled, Phase Ⅲ Trial. Front. Pharmacol. 2022, 13, 900723. [Google Scholar] [CrossRef]
- Yao, Y.; Guan, J.; Liu, L.; Fu, B.; Chen, L.; Zheng, X. Discharge Readiness after Remimazolam versus Propofol for Colonoscopy: A Randomised, Double-Blind Trial. Eur. J. Anaesthesiol. 2022, 39, 911–917. [Google Scholar] [CrossRef]
- Saari, T.I.; Uusi-Oukari, M.; Ahonen, J.; Olkkola, K.T. Enhancement of GABAergic Activity: Neuropharmacological Effects of Benzodiazepines and Therapeutic Use in Anesthesiology. Pharmacol. Rev. 2011, 63, 243–267. [Google Scholar] [CrossRef] [PubMed]
- Freyer, N.; Knöspel, F.; Damm, G.; Greuel, S.; Schneider, C.; Seehofer, D.; Stöhr, T.; Petersen, K.-U.; Zeilinger, K. Metabolism of Remimazolam in Primary Human Hepatocytes during Continuous Long-Term Infusion in a 3-D Bioreactor System. Drug Des. Dev. Ther. 2019, 13, 1033–1047. [Google Scholar] [CrossRef]
- Oka, S.; Satomi, H.; Sekino, R.; Taguchi, K.; Kajiwara, M.; Oi, Y.; Kobayashi, R. Sedation Outcomes for Remimazolam, a New Benzodiazepine. J. Oral. Sci. 2021, 63, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Jhuang, B.-J.; Yeh, B.-H.; Huang, Y.-T.; Lai, P.-C. Efficacy and Safety of Remimazolam for Procedural Sedation: A Meta-Analysis of Randomized Controlled Trials with Trial Sequential Analysis. Front. Med. 2021, 8, 641866. [Google Scholar] [CrossRef] [PubMed]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and Safety of Remimazolam versus Propofol for General Anesthesia: A Multicenter, Single-Blind, Randomized, Parallel-Group, Phase IIb/III Trial. J. Anesth. 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Dai, G.; Pei, L.; Duan, F.; Liao, M.; Zhang, Y.; Zhu, M.; Zhao, Z.; Zhang, X. Safety and Efficacy of Remimazolam Compared with Propofol in Induction of General Anesthesia. Minerva Anestesiol. 2021, 87, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Fechner, J. Remimazolam—Current Knowledge on a New Intravenous Benzodiazepine Anesthetic Agent. Korean J. Anesthesiol. 2022, 75, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, U. Einschätzung Des Abhängigkeitsrisikos von Propofol. Fortschr. Neurol. Psychiatr. 2011, 79, 442–452. [Google Scholar] [CrossRef]
- Schippers, F.; Pesic, M.; Saunders, R.; Borkett, K.; Searle, S.; Webster, L.; Stoehr, T. Randomized Crossover Trial to Compare Abuse Liability of Intravenous Remimazolam versus Intravenous Midazolam and Placebo in Recreational Central Nervous System Depressant Users. J. Clin. Pharmacol. 2020, 60, 1189–1197. [Google Scholar] [CrossRef]
- Pedersen, M.H.; Danø, A.; Englev, E.; Kattenhøj, L.; Munk, E. Economic Benefits of Remimazolam Compared to Midazolam and Propofol for Procedural Sedation in Colonoscopies and Bronchoscopies. Curr. Med. Res. Opin. 2023, 39, 691–699. [Google Scholar] [CrossRef]
- Lee, B.; Kim, M.H.; Kong, H.J.; Shin, H.J.; Yang, S.; Kim, N.Y.; Chae, D. Effects of Remimazolam vs. Sevoflurane Anesth. Intraoperative Hemodynamics Patients Gastric Cancer Undergoing Robot. Gastrectomy: A Propensity Score-Matched Analysis. J. Clin. Med. 2022, 11, 2643. [Google Scholar] [CrossRef]
- Wu, Q.; Xu, F.; Wang, J.; Jiang, M. Comparison of Remimazolam–Flumazenil versus Propofol for Recovery from General Anesthesia: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 7316. [Google Scholar] [CrossRef] [PubMed]
- Ahmer, W.; Imtiaz, S.; Alam, D.M.; Ahmed, K.; Sajid, B.; Yousuf, J.; Asnani, S.; Fahim, M.A.A.; Ali, R.; Mansoor, M.; et al. Remimazolam versus Propofol for Sedation in Gastrointestinal Endoscopy and Colonoscopy within Elderly Patients: A Meta-Analysis of Randomized Controlled Trials. Eur. J. Clin. Pharmacol. 2024, 80, 493–503. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Country | Year | Author | ASA 1 | Case (R 2/C 3) | Comparison | Age (Years) | BMI 4 (kg/m2) |
|---|---|---|---|---|---|---|---|---|
| 1 | US | 2016 | Pambianco [14] | 1–2 | 160 (120/40) | Midazolam | Overall mean 55 | Overall mean 27 |
| 2 | US | 2018 | Rex [15] | 1–3 | 458 (296/162) | Placebo n = 60, Midazolam n = 102 | Remimazolam 54.4 ± 10.12 Placebo 56.0 ± 9.51 Midazolam 55.6 ± 10.15 | Remimazolam 28.9 ± 4.72 Placebo 30.0 ± 5.31 Midazolam 28.8 ± 4.75 |
| 3 | China | 2020 | Chen [16] | 1–2 | 384 (194/190) | Propofol | Remimazolam 44.47 ± 11.67 Propofol 44.43 ± 11.37 | Remimazolam 23.19 ± 2.92 Propofol 23.21 ± 2.84 |
| 4 | US | 2021 | Rex [17] | 3–4 | 77 (31/46) | Placebo n = 16, Midazolam n = 30 | Remimazolam 63.1 ± 8.6 Placebo 63.0 ± 8.37 Midazolam 61.5 ± 10.60 | Remimazolam 30.9 ± 8.24 Placebo 30.8 ± 5.53 Midazolam 30.8 ± 6.75 |
| 5 | China | 2021 | Liu [18] | 1–2 | 232 (115/117) | Etomidate-Propofol | Remimazolam 68.87 ± 2.58 Etomidate-Propofol 69.12 ± 2.75 | Remimazolam 25.35 ± 2.07 Etomidate-Propofol 24.75 ± 2.16 |
| 6 | China | 2022 | Wang [19] | 1–3 | 476 (357/119) | Propofol | Remimazolam 44.3 [33.0–54.0] Propofol 46.4 [37.5–56.0] | Remimazolam 22.82 [20.70–24.90] Propofol 22.87 [21.10–24.60] |
| 7 | China | 2022 | Yao [20] | 1–2 | 132 (66/66) | Propofol | Remimazolam 49 [41–56] Propofol 48 [39–56] | Remimazolam 22.4 [19.8–24.6] Propofol 22.0 [20.1–25.3] |
| No | Country | Year | Author | Dose of Remimazolam (Induction/Maintenance) | Dose of other Sedative Agents (Induction/Maintenance) | Opioids Use (Induction/Supplemental Dose) |
|---|---|---|---|---|---|---|
| 1 | US | 2016 | Pambianco [14] | 8.0 mg/3.0 mg, 7.0 mg/2.0 mg, or 5.0 mg/3.0 mg | 2.5 mg/1 mg | 100 mcg/25 mcg of fentanyl |
| 2 | US | 2018 | Rex [15] | 5.0 mg/2.5 mg | 1.75 mg/1.0 mg for <60 years old patients 1.0 mg/0.5 mg for >60 years old patients | 80% patients 75 mcg/25 mcg of fentanyl 20% patients 50 mcg/25 mcg of fentanyl |
| 3 | China | 2020 | Chen [16] | 5.0 mg/2.5 mg | 1.5 mg/kg/0.5 mg/kg | 2 Remimazolam 62.99 ± 10.81 of fentanyl 2 Propofol 63.64 ± 11.19 of fentanyl |
| 4 | US | 2021 | Rex [17] | 2.5-5.0 mg/1.25-2.5 mg | 1 mg/0.5 mg | 50 mcg/25 mcg of fentanyl |
| 5 | China | 2021 | Liu [18] | 0.15 mg/kg/0.075 mg/kg | E-P 1 0.1 mL/kg/0.05 mL/kg | 0.5 mcg/kg/0.5 mcg/kg of fentanyl |
| 6 | China | 2022 | Wang [19] | 7 mg/2.5 mg | 1.5 mg/kg/0.5 mg/kg | 50 mcg of fentanyl |
| 7 | China | 2022 | Yao [20] | 0.2 mg/kg/6 mg | 1 mg/kg/30 mg | 5 mcg of sufentanil |
| No | Country | Year | Author | Hypoxia | Hypotension | Bradycardia |
|---|---|---|---|---|---|---|
| 1 | US | 2016 | Pambianco [14] | Oxygen saturation < 90% | SBP 1 < 80 mmHg | Not mentioned in the article |
| 2 | US | 2018 | Rex [15] | Oxygen saturation < 90% for ≥1 min or any drop necessitating medical intervention | SBP ≤ 80 mmHg or DBP 2 ≤ 40 mm Hg, or a fall in SBP or DBP of 20% or more below baseline or necessitating medical intervention | <40 bpm 4 or drop in heart rate of 20% > 30 s |
| 3 | China | 2020 | Chen [16] | Oxygen saturation < 90% | The reduction of SBP ≥ 20% (compared to baseline SBP before sedation) or decreased to ≤80 mmHg | Not mentioned in the article |
| 4 | US | 2021 | Rex [17] | Oxygen saturation < 90% for ≥1 min, or any drop necessitating medical intervention | SBP ≤ 80 mmHg or DBP 2 ≤ 40 mm Hg, or a fall in SBP or DBP of 20% or more below baseline or necessitating medical intervention | <40 bpm 4 or drop in heart rate of 20% > 30 s |
| 5 | China | 2021 | Liu [18] | Oxygen saturation < 90% | SBP < 90 mmHg, DBP < 50 mmHg, or a MAP 3 decrease of 20% or more below baseline | <50 bpm or a decrease in heart rate of 20% or more from baseline |
| 6 | China | 2022 | Wang [19] | Oxygen saturation < 90% | SBP ≤ 80 mmHg | Not mentioned in the article |
| 7 | China | 2022 | Yao [20] | Oxygen saturation < 92% | Decrease in MAP at least 20% from the baseline value | Heart rate less than 50 bpm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-H.; Chang, C.-Y.; Lu, C.-W. A Comparison of Hypotension, Bradycardia, and Hypoxia Incidence between the Use of Remimazolam and Other Sedative Agents during Colonoscopy Procedures: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 4352. https://doi.org/10.3390/jcm13154352
Ho C-H, Chang C-Y, Lu C-W. A Comparison of Hypotension, Bradycardia, and Hypoxia Incidence between the Use of Remimazolam and Other Sedative Agents during Colonoscopy Procedures: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(15):4352. https://doi.org/10.3390/jcm13154352
Chicago/Turabian StyleHo, Chia-Hao, Cheng-Ying Chang, and Cheng-Wei Lu. 2024. "A Comparison of Hypotension, Bradycardia, and Hypoxia Incidence between the Use of Remimazolam and Other Sedative Agents during Colonoscopy Procedures: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 15: 4352. https://doi.org/10.3390/jcm13154352
APA StyleHo, C.-H., Chang, C.-Y., & Lu, C.-W. (2024). A Comparison of Hypotension, Bradycardia, and Hypoxia Incidence between the Use of Remimazolam and Other Sedative Agents during Colonoscopy Procedures: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(15), 4352. https://doi.org/10.3390/jcm13154352