

The Role of Renal PLA2R Staining Combined with Serum PLA2R Antibody in Membranous Nephropathy Risk Stratification
Abstract
:1. Introduction
2. Materials and Methods
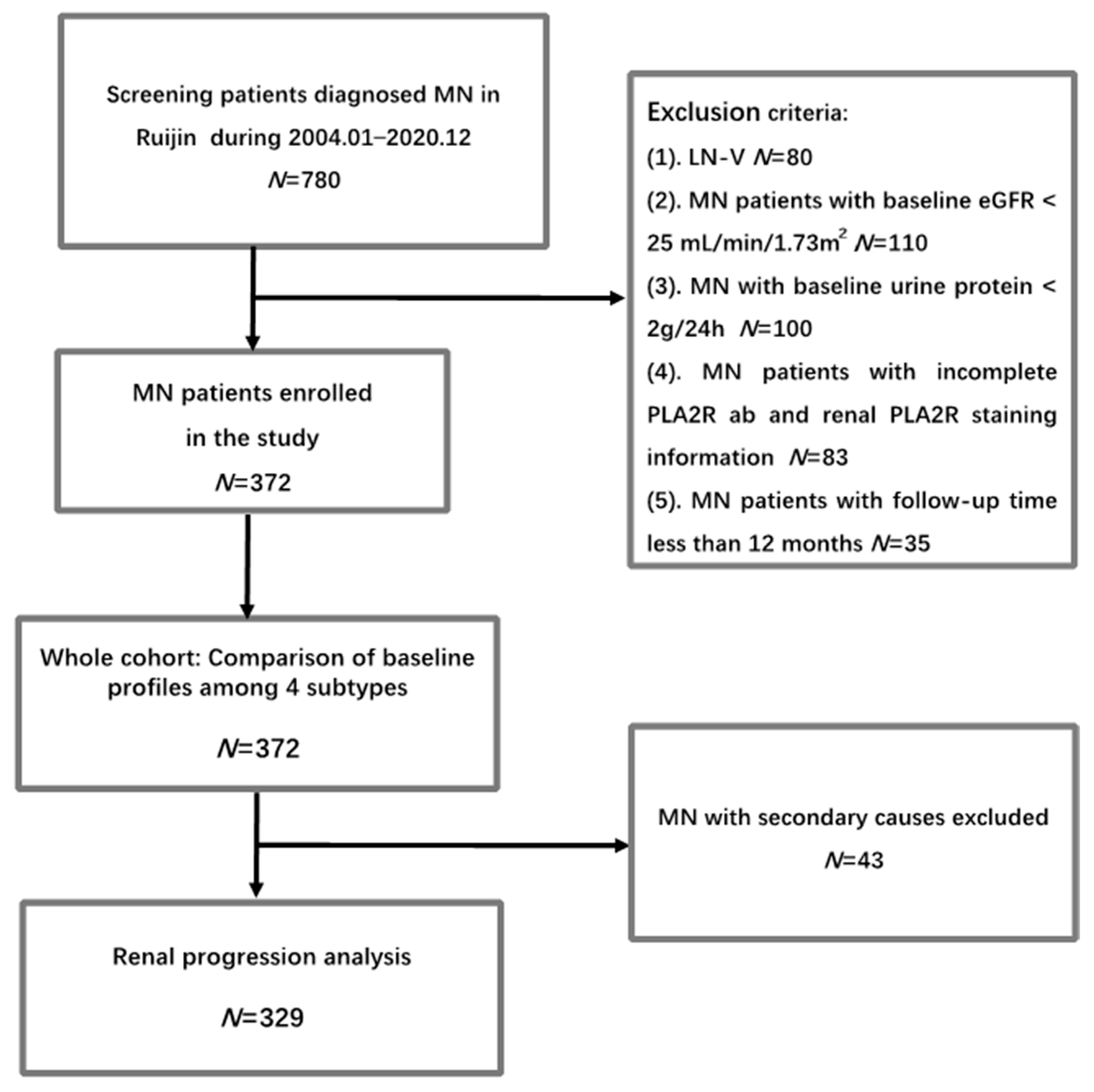
2.1. Participants and Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Whole Cohort and Comparison of Baseline Profiles among Different Subtypes Based on PLA2R ab and Glomerular PLA2R Staining in PMN
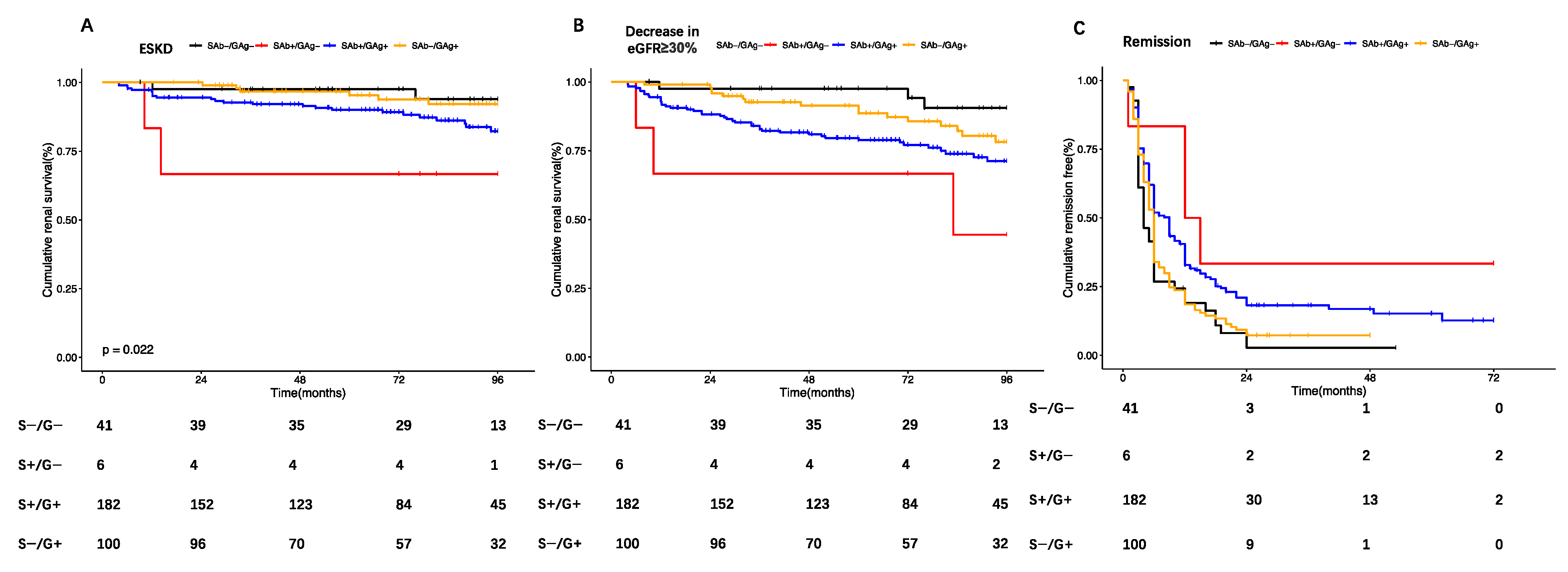
3.2. Comparison of Renal Prognosis among Different Subtypes Based on PLA2R ab and Glomerular PLA2R Staining in PMN
3.3. Predictors of Early Remission and Renal Progression in PMN
3.4. Comparison of Response to Immunosuppressive Therapy among Different Subtypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pan, X.; Xu, J.; Ren, H.; Zhang, W.; Xu, Y.; Shen, P.; Li, X.; Wang, W.; Chen, X.; Wu, P.; et al. Changing spectrum of biopsy-proven primary glomerular diseases over the past 15 years: A single-center study in China. Contrib. Nephrol. 2013, 181, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Zhu, P.; Zhou, F.D.; Wang, S.X.; Zhao, M.H.; Wang, H.Y. Increasing frequency of idiopathic membranous nephropathy in primary glomerular disease: A 10-year renal biopsy study from a single Chinese nephrology centre. Nephrology 2015, 20, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, G.; Chen, N.; Lu, T.; Nie, S.; Xu, G.; Zhang, P.; Luo, Y.; Wang, Y.; Wang, X.; et al. Long-Term Exposure to Air Pollution and Increased Risk of Membranous Nephropathy in China. J. Am. Soc. Nephrol. 2016, 27, 3739–3746. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.H., Jr.; Bonegio, R.G.; Lambeau, G.; Beck, D.M.; Powell, D.W.; Cummins, T.D.; Klein, J.B.; Salant, D.J. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N. Engl. J. Med. 2009, 361, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Tomas, N.M.; Beck, L.H.; Meyer-Schwesinger, C.; Seitz-Polski, B.; Ma, H.; Zahner, G.; Dolla, G.; Hoxha, E.; Helmchen, U.; Dabert-Gay, A.-S.; et al. Thrombospondin Type-1 Domain-Containing 7A in Idiopathic Membranous Nephropathy. N. Engl. J. Med. 2014, 371, 2277–2287. [Google Scholar] [CrossRef]
- Sethi, S.; Debiec, H.; Madden, B.; Vivarelli, M.; Charlesworth, M.C.; Ravindran, A.; Gross, L.; Ulinski, T.; Buob, D.; Tran, C.L.; et al. Semaphorin 3B-associated membranous nephropathy is a distinct type of disease predominantly present in pediatric patients. Kidney Int. 2020, 98, 1253–1264. [Google Scholar] [CrossRef]
- Xie, J.; Liu, L.; Mladkova, N.; Li, Y.; Ren, H.; Wang, W.; Cui, Z.; Lin, L.; Hu, X.; Yu, X.; et al. The genetic architecture of membranous nephropathy and its potential to improve non-invasive diagnosis. Nat. Commun. 2020, 11, 1600. [Google Scholar] [CrossRef]
- Stanescu, H.C.; Arcos-Burgos, M.; Medlar, A.; Bockenhauer, D.; Kottgen, A.; Dragomirescu, L.; Voinescu, C.; Patel, N.; Pearce, K.; Hubank, M.; et al. Risk HLA-DQA1 and PLA2R1 alleles in idiopathic membranous nephropathy. N. Engl. J. Med. 2011, 364, 616–626. [Google Scholar] [CrossRef]
- Bullich, G.; Ballarín, J.; Oliver, A.; Ayasreh, N.; Silva, I.; Santín, S.; Díaz-Encarnación, M.M.; Torra, R.; Ars, E. HLA-DQA1 and PLA2R1 polymorphisms and risk of idiopathic membranous nephropathy. Clin. J. Am. Soc. Nephrol. 2014, 9, 335–343. [Google Scholar] [CrossRef]
- Qin, W.; Beck, L.H.; Zeng, C.; Chen, Z.; Li, S.; Zuo, K.; Salant, D.J.; Liu, Z. Anti-Phospholipase A2 Receptor Antibody in Membranous Nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1137–1143. [Google Scholar] [CrossRef]
- Hanset, N.; Aydin, S.; Demoulin, N.; Cosyns, J.-P.; Castanares-Zapatero, D.; Crott, R.; Cambier, J.-F.; Pochet, J.-M.; Gillerot, G.; Reginster, F.; et al. Podocyte Antigen Staining to Identify Distinct Phenotypes and Outcomes in Membranous Nephropathy: A Retrospective Multicenter Cohort Study. Am. J. Kidney Dis. 2020, 76, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Sun, L.; Dong, H.; Wang, Y.; Xu, X.; Zhao, Z.; Cheng, W.; Liu, X.; Zhao, X.; Geng, Y.; et al. Neural Epidermal Growth Factor-Like 1 Protein-Positive Membranous Nephropathy in Chinese Patients. Clin. J. Am. Soc. Nephrol. 2021, 16, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.S.; Satoskar, A.A.; Nadasdy, G.M.; Brodsky, S.V.; Hemminger, J.A.; Nadasdy, T. Phospholipase A2 receptor staining is absent in many kidney biopsies with early-stage membranous glomerulonephritis. Kidney Int. 2016, 89, 1402–1403. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Yuan, Y.; Tian, J.; Zhou, Z.; Su, C.; Yang, F.; Wang, G. Clinicopathological Characteristics and Outcomes of PLA2R-Associated Membranous Nephropathy in Seropositive Patients Without PLA2R Staining on Kidney Biopsy. Am. J. Kidney Dis. 2022, 80, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Zhang, W.; Su, C.; Zhou, Z.; Wang, G. Seropositive PLA2R-associated membranous nephropathy but biopsy-negative PLA2R staining. Nephrol. Dial. Transplant. 2021, 36, 2216–2223. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.-Z.; Zhang, M.-C.; Le, W.-B.; Ren, Q.; Chen, D.-C.; Zeng, C.-H.; Liu, L.; Zuo, K.; Xu, F.; Liu, Z.-H. Combined Assessment of Phospholipase A2 Receptor Autoantibodies and Glomerular Deposits in Membranous Nephropathy. J. Am. Soc. Nephrol. 2016, 27, 3195–3203. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Stefansson, B.V.; Batiushin, M.; Bilchenko, O.; Cherney, D.Z.I.; Chertow, G.M.; Douthat, W.; Dwyer, J.P.; Escudero, E.; Pecoits-Filho, R.; et al. The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial: Baseline characteristics. Nephrol. Dial. Transplant. 2020, 35, 1700–1711. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 753–779. [Google Scholar] [CrossRef]
- Sethi, S.; Debiec, H.; Madden, B.; Charlesworth, M.C.; Morelle, J.; Gross, L.; Ravindran, A.; Buob, D.; Jadoul, M.; Fervenza, F.C.; et al. Neural epidermal growth factor-like 1 protein (NELL-1) associated membranous nephropathy. Kidney Int. 2020, 97, 163–174. [Google Scholar] [CrossRef]
- Caza, T.N.; Hassen, S.I.; Dvanajscak, Z.; Kuperman, M.; Edmondson, R.; Herzog, C.; Storey, A.; Arthur, J.; Cossey, L.N.; Sharma, S.G.; et al. NELL1 is a target antigen in malignancy-associated membranous nephropathy. Kidney Int. 2021, 99, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Madden, B.J.; Debiec, H.; Charlesworth, M.C.; Gross, L.; Ravindran, A.; Hummel, A.M.; Specks, U.; Fervenza, F.C.; Ronco, P. Exostosin 1/Exostosin 2-Associated Membranous Nephropathy. J. Am. Soc. Nephrol. 2019, 30, 1123–1136. [Google Scholar] [CrossRef] [PubMed]
- Svobodova, B.; Honsova, E.; Ronco, P.; Tesar, V.; Debiec, H. Kidney biopsy is a sensitive tool for retrospective diagnosis of PLA2R-related membranous nephropathy. Nephrol. Dial. Transplant. 2013, 28, 1839–1844. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All | SAb−/GAg− | SAb+/GAg− | SAb+/GAg+ | SAb−/GAg+ | p Value | |
|---|---|---|---|---|---|---|
| No (%) | 372 | 54 (14.52) | 7 (1.89) | 201 (54.03) | 110 (29.57) | - |
| PLA2R ab (RU/mL) | 28.22 (3.50, 96.38) | 1.41 (1.08, 2.24) | 240.10 (74.17, 369.18) | 78.59 (42.95, 158.81) | 4.57 (1.65, 9.47) | <0.01 |
| Female (%) | 135 (36.29) | 22 (40.74) | 4 (57.14) | 71 (35.32) | 38 (34.55) | 0.57 |
| Age (y) | 56.00 (43.75, 64.00] | 53.50 (38.75, 64.00) | 53.00 (44.00, 63.50) | 57.00 (46.00, 65.00) | 54.00 (41.50, 62.00) | 0.50 |
| Microscopic Hematuria (%) | 174 (46.77) | 22 (40.74) | 4 (57.14) | 96 (47.76) | 52 (47.27) | 0.76 |
| Urine protein (g/24 h) | 5.71 (4.11, 8.25) | 5.39 (3.97, 6.79) | 6.84 (4.45, 8.19) | 6.38 (4.33, 9.06) | 5.09 (3.64, 7.37) | 0.01 |
| Albumin (g/L) | 21 (17, 26) | 23.5 (17, 28) | 14 (13, 21) | 21 (16, 25) | 23.5 (18, 29) | <0.01 |
| eGFR-EPI (mL/min × 1.73 m2) | 99.13 (78.61, 113.92) | 101.88 (87.33, 113.94) | 99.71 (85.91, 119.00) | 96.07 (74.60, 113.58) | 99.62 (86.55, 112.13) | 0.48 |
| Uric acid (umol/L) | 350.5 (295.5, 401.3) | 352.0 (297.0, 391.0) | 319.0 (302.5, 363.5) | 350.0 (293.0, 403.0) | 352.0 (300.5, 401.5) | 0.87 |
| Hypertension (%) | 170 (45.70) | 12 (22.22) | 3 (42.86) | 101 (50.25) | 54 (49.09) | <0.01 |
| Diabetes Mellitus (%) | 52 (13.98) | 7 (12.96) | 1 (14.29) | 31 (15.42) | 13 (11.82) | 0.84 |
| Treatment (%) | 0.1 | |||||
| Pred + CTX | 123 (33.06) | 16 (29.63) | 3 (42.86) | 73 (36.32) | 31 (28.18) | |
| pred + CSA | 138 (37.10) | 19 (35.19) | 3 (42.86) | 80 (39.80) | 36 (32.73) | |
| ACEI/ARB | 95 (25.54) | 19 (35.19) | 1 (14.29) | 38 (18.91) | 37 (33.64) | |
| RTX | 16 (4.30) | 0 (0.00) | 0 (0.00) | 10 (4.98) | 6 (5.45) | |
| Secondary causes (%) | 43 (11.56) | 13 (24.07) | 1 (14.29) | 19 (9.45) | 10 (9.09) | 0.02 |
| Pathology stage (%) | <0.01 | |||||
| I | 77 (20.70) | 21 (38.89) | 0 (0.00) | 31 (15.42) | 25 (22.73) | |
| II | 246 (66.13) | 24 (44.44) | 6 (85.71) | 143 (71.14) | 73 (66.36) | |
| III + IV | 49 (13.17) | 9 (16.67) | 1 (14.29) | 27 (13.43) | 12 (10.91) | |
| Tubulo-interstitial lesions ≥ 25(%) | 8 (2.15) | 0 (0.00) | 0 (0.00) | 6 (2.99) | 2 (1.82) | 0.56 |
| Prognosis * (N) | 329 | 41 | 6 | 182 | 100 | |
| Follow-up time (m) | 79.20 (48.70, 97.40) | 84.00 (51.77, 98.43) | 85.23 (60, 97.40) | 74.55 (28.65, 80.13) | 84.22 (44.63, 106.75) | 0.22 |
| Death (%) | 13 (3.95) | 2 (4.88) | 1 (16.67) | 8 (4.40) | 2 (2.00) | 0.29 |
| ESRD (%) | 38 (11.55) | 3 (7.32) | 2 (33.33) | 27 (14.84) | 6 (6.00) | 0.04 |
| Tumor (%) | 12 (3.65) | 0 (0.00) | 0 (0.00) | 6 (3.30) | 6 (6.00) | 0.33 |
| Thrombosis (%) | 25 (7.60) | 3 (7.32) | 1 (16.67) | 14 (7.69) | 7 (7.00) | 0.86 |
| Decrease in eGFR ≥ 30% (%) | 73 (22.19) | 4 (9.76) | 4 (66.67) | 47 (25.82) | 18 (18.00) | <0.01 |
| 6m remission (%) | 183 (55.62) | 30 (73.17) | 1 (16.67) | 87 (47.80) | 65 (65.00) | <0.01 |
| 24m remission (%) | 281 (85.41) | 39 (95.12) | 5 (83.33) | 145 (79.67) | 92 (92.00) | 0.01 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR: 95% CI | p Value | HR: 95% CI | p Value | |
| Male (%) | 1.18 (0.73–1.92) | 0.49 | ||
| Age (y) | 1.06 (1.04–1.08) | <0.01 | 1.06 (1.03–1.08) | <0.01 |
| Microscopic Hematuria (%) | 0.79 (0.49–1.25) | 0.31 | ||
| Urine protein (g/24 h) | 1.02 (0.96–1.09) | 0.48 | ||
| Albumin (g/L) | 0.97 (0.94–1.01) | 0.11 | ||
| eGFR-EPI (mL/min × 1.73 m2) | 0.98 (0.97–0.99) | <0.01 | 1.004 (0.99–1.02) | 0.50 |
| Uric acid (umol/L) | 1.001 (0.999–1.004) | 0.32 | ||
| Hypertension (%) | 1.75 (1.10–2.80) | 0.02 | 0.92 (0.55–1.57) | 0.77 |
| Diabetes Mellitus (%) | 2.89 (1.71–4.90) | <0.01 | 2.35 (1.35–4.09) | <0.01 |
| Immunosuppressive therapy (%) | 2.73 (1.36–5.48) | 0.01 | ||
| Pathology stage (%) | ||||
| I | reference | |||
| II | 1.32 (0.72–2.40) | 0.37 | ||
| III + IV | 1.37 (0.62–3.03) | 0.44 | ||
| Tubulo-interstitial lesions ≥ 25 (%) | 2.98 (1.08–8.18) | 0.03 | 2.34 (0.76–7.19) | 0.14 |
| Serum PLA2R ab and glomerular PLA2R staining | ||||
| SAb−/GAg− | reference | reference | ||
| SAb+/GAg− | 9.13 (2.28–36.62) | <0.01 | 9.17 (2.26–37.16) | <0.01 |
| SAb+/GAg+ | 3.26 (1.17–9.07) | 0.02 | 2.32 (0.83–6.53) | 0.11 |
| SAb−/GAg+ | 1.92 (0.65–5.67) | 0.24 | 1.53 (0.51–4.60) | 0.45 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR: 95% CI | p Value | OR: 95% CI | p Value | |
| Male (%) | 1.20 (0.76–1.87) | 0.43 | ||
| Age (y) | 0.997 (0.98–1.01) | 0.73 | ||
| Microscopic Hematuria (%) | 0.95 (0.61–1.46) | 0.81 | ||
| Urine protein (g/24 h) | 0.94 (0.89–0.99) | 0.046 | 0.92 (0.85–0.98) | 0.02 |
| Albumin (g/L) | 1.03 (0.99–1.06) | 0.11 | ||
| eGFR-EPI (mL/min × 1.73m2) | 0.999 (0.99–1.01) | 0.92 | ||
| Uric acid (umol/L) | 0.999 (0.997–1.002) | 0.90 | ||
| Hypertension (%) | 0.84 (0.55–1.31) | 0.44 | ||
| Diabetes Mellitus (%) | 0.41 (0.22–0.79) | 0.01 | 0.47 (0.24–0.94) | 0.03 |
| Immunosuppressive therapy (%) | 1.81 (1.01–2.98) | 0.02 | 3.19 (1.78–5.73) | <0.01 |
| Pathology stage (%) | ||||
| I | reference | |||
| II | 0.78 (0.45–1.35) | 0.38 | ||
| III + IV | 0.87 (0.41–1.84) | 0.71 | ||
| Tubulo-interstitial lesions ≥ 25 (%) | 0.59 (0.13–2.69) | 0.50 | ||
| Serum PLA2R ab and glomerular PLA2R staining | ||||
| SAb−/GAg− | reference | reference | ||
| SAb+/GAg− | 0.07 (0.01–0.70) | 0.02 | 0.06 (0.01–0.56) | 0.01 |
| SAb+/GAg+ | 0.34 (0.16–0.71) | <0.01 | 0.30 (0.14–0.66) | <0.01 |
| SAb−/GAg+ | 0.68 (0.31–1.52) | 0.35 | 0.70 (0.30–1.61) | 0.40 |
| CTX | SAb+/GAg+ | SAb−/GAg+ | SAb−/GAg− | SAb+/GAg− |
|---|---|---|---|---|
| N | 63 | 29 | 12 | 3 |
| 6 m remission (%) | 30 (47.62) | 14 (48.28) | 8 (66.67) | 0 (0) |
| OR | reference | 1.03 (0.43–2.48) | 2.20 (0.60–8.06) | - |
| OR adjusted a | reference | 0.94 (0.38–2.33) | 2.10 (0.56–7.88) | - |
| CSA | SAb+/GAg+ | SAb−/GAg+ | SAb−/GAg− | SAb+/GAg− |
| N | 76 | 31 | 16 | 2 |
| 6 m remission (%) | 44 (57.89) | 30 (96.77) | 12 (75) | 1 (50) |
| OR | reference | 21.82 (2.83–168.42) ** | 2.18 (0.64–7.39) | 0.73 (0.04–12.07) |
| OR adjusted a | reference | 16.77 (2.10–134.14) * | 2.21 (0.59–8.27) | 0.25 (0.01–4.56) |
| ACEI/ARB | SAb+/GAg+ | SAb−/GAg+ | SAb−/GAg− | SAb+/GAg− |
| N | 35 | 35 | 13 | 1 |
| 6 m remission (%) | 10 (28.57) | 18 (51.43) | 10 (76.92) | 0 (0) |
| OR | reference | 2.65 (0.99–7.11) | 8.33 (1.89–36.76) * | - |
| OR adjusted a | reference | 2.50 (0.90–6.99) | 12.25 (2.48–60.53) ** | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, X.; Wang, X.; Yu, X.; Ni, L.; Gao, C.; Pan, X.; Ren, H.; Xu, J.; Ma, J. The Role of Renal PLA2R Staining Combined with Serum PLA2R Antibody in Membranous Nephropathy Risk Stratification. J. Clin. Med. 2024, 13, 68. https://doi.org/10.3390/jcm13010068
Hu X, Wang X, Yu X, Ni L, Gao C, Pan X, Ren H, Xu J, Ma J. The Role of Renal PLA2R Staining Combined with Serum PLA2R Antibody in Membranous Nephropathy Risk Stratification. Journal of Clinical Medicine. 2024; 13(1):68. https://doi.org/10.3390/jcm13010068
Chicago/Turabian StyleHu, Xiaofan, Xinlu Wang, Xialian Yu, Liyan Ni, Chenni Gao, Xiaoxia Pan, Hong Ren, Jing Xu, and Jun Ma. 2024. "The Role of Renal PLA2R Staining Combined with Serum PLA2R Antibody in Membranous Nephropathy Risk Stratification" Journal of Clinical Medicine 13, no. 1: 68. https://doi.org/10.3390/jcm13010068
APA StyleHu, X., Wang, X., Yu, X., Ni, L., Gao, C., Pan, X., Ren, H., Xu, J., & Ma, J. (2024). The Role of Renal PLA2R Staining Combined with Serum PLA2R Antibody in Membranous Nephropathy Risk Stratification. Journal of Clinical Medicine, 13(1), 68. https://doi.org/10.3390/jcm13010068