
Clinical Course and Management of Patients with Emergency Surgery Treated with Direct Oral Anticoagulants or Vitamin K Antagonists—Results of the German Prospective RADOA-Registry

 , , and
, , and  on behalf of the RADOA-Registry Investigators
on behalf of the RADOA-Registry Investigators
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
- Age > 18 years.
- Patients anticoagulated with a DOAC or phenprocoumon needing an urgent surgical intervention (not caused by severe bleeding) within 24 h after admission.
2.2. Study Design and Oversight
2.3. Definition of INR-Rebound
2.4. Definition of Major Bleeding
- good hemostasis (for the type of surgery performed)
- severe bleeding outside the surgical area with a drop in hemoglobin ≥ 2 g/dL or a need of >2 RBC transfusions within 24 h after admission
- bleeding in the surgical area requiring re-surgery
- bleeding in the surgical area that was unexpected and persistent and/or led to hemodynamic instability (drop in Hb value ≥ 2 g/dL or transfusion of >2 RBC) within 24 h after admission
2.5. Ethics
2.6. Statistics
3. Results
3.1. Demographic Data of Included Patients
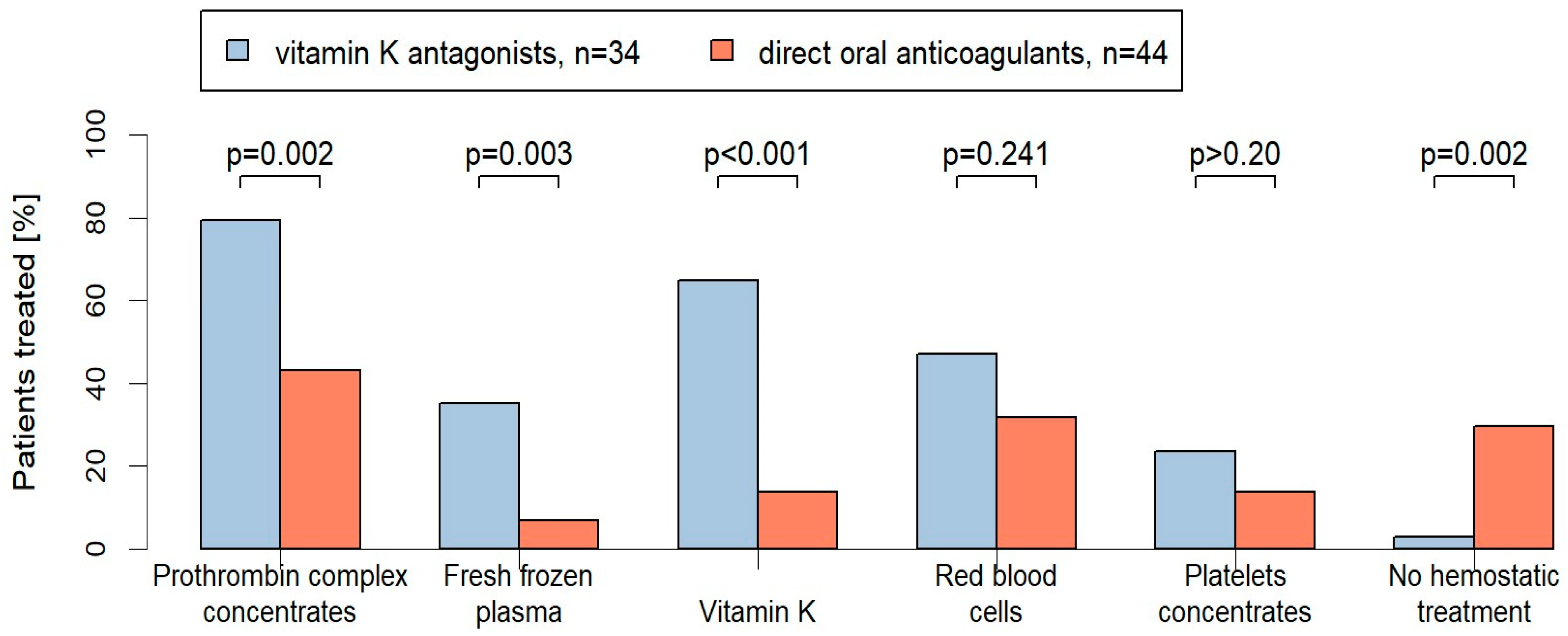
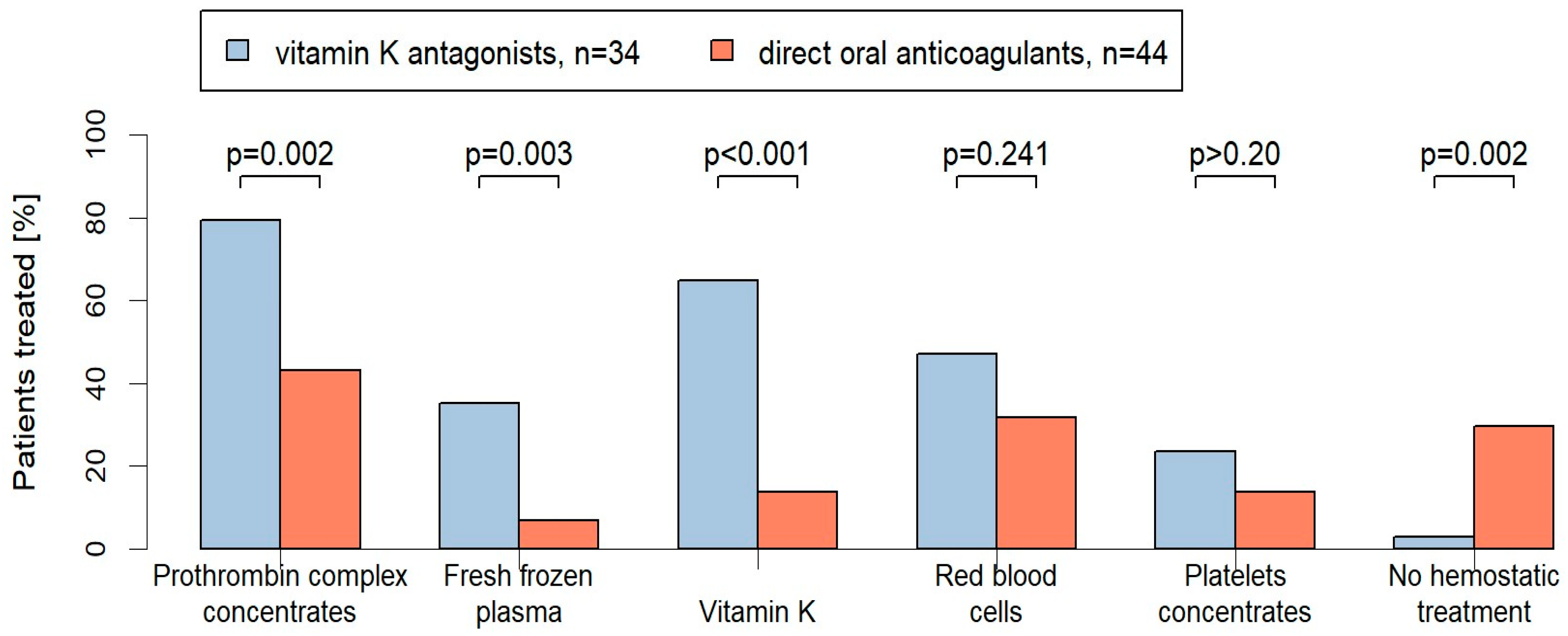
3.2. Management
Use of Specific Antidotes
3.3. Bleeding Complications
3.4. INR-Rebound
3.5. Thromboembolic Complications
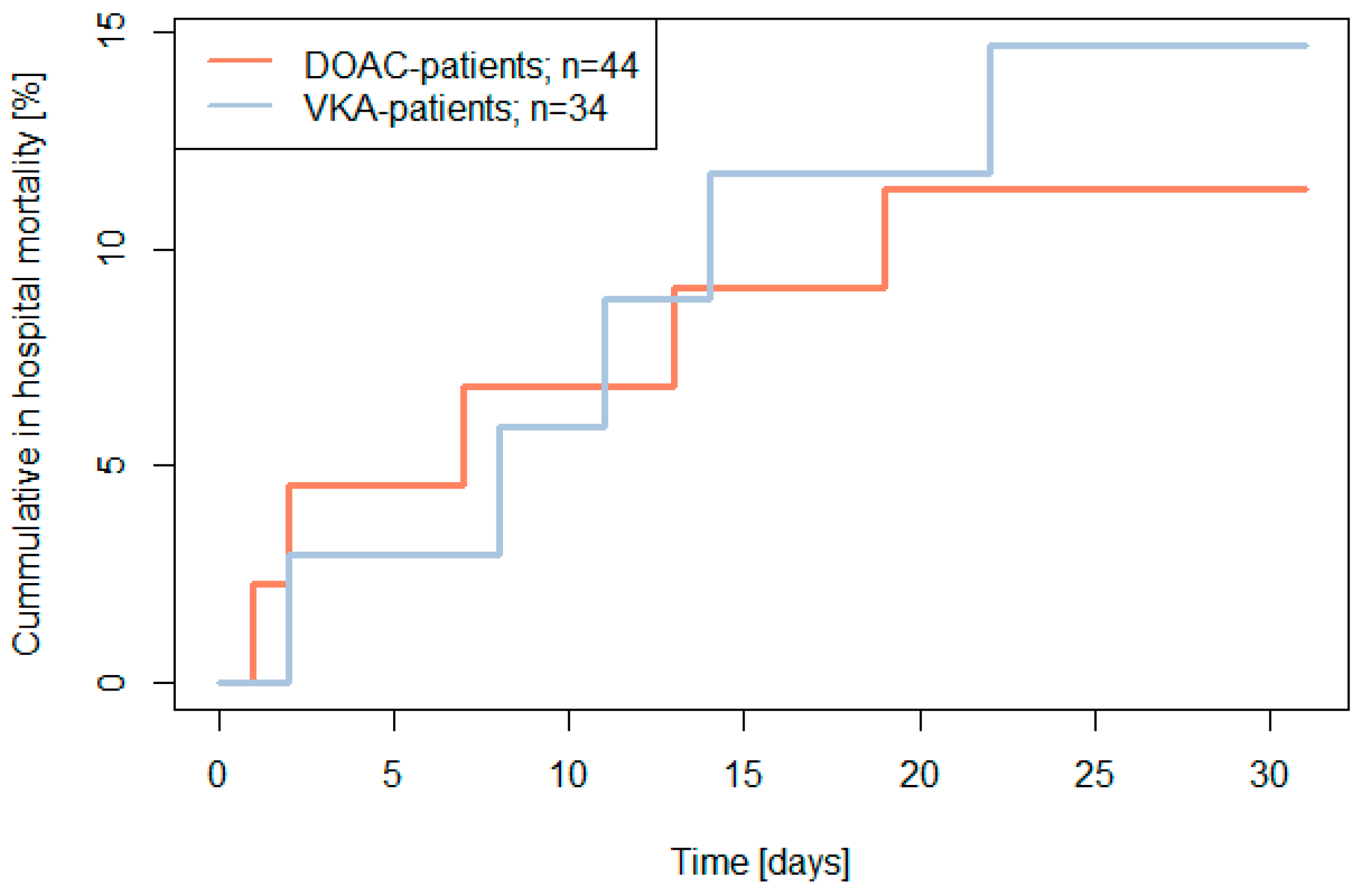
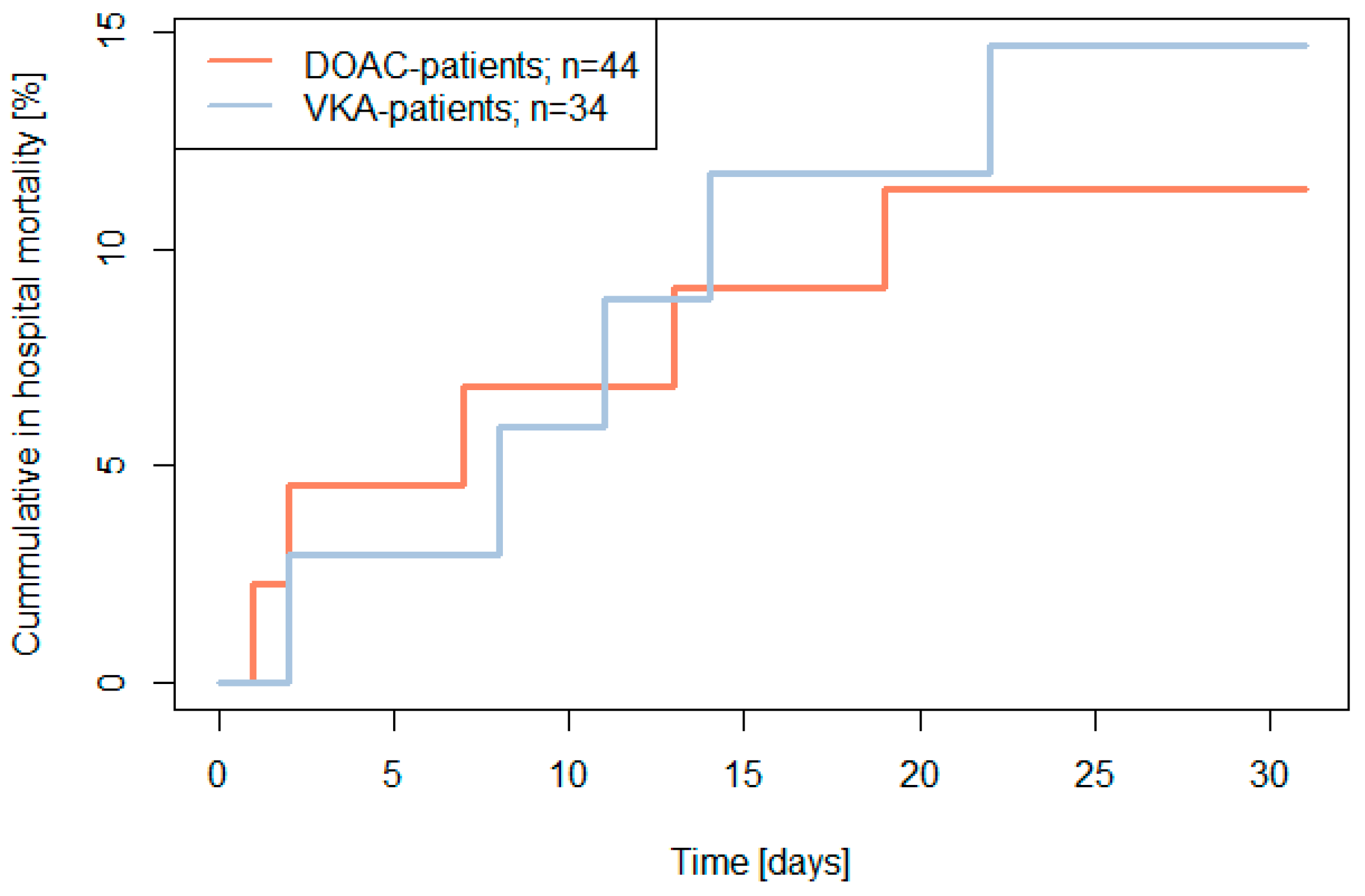
3.6. In-Hospital Mortality (until Day 30 after Admission)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Spinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Investigators, E.; Bauersachs, R.; Berkowitz, S.D.; Brenner, B.; Buller, H.R.; Decousus, H.; Gallus, A.S.; Lensing, A.W.; Misselwitz, F.; Prins, M.H.; et al. Oral rivaroxaban for symptomatic venous thromboembolism. N. Engl. J. Med. 2010, 363, 2499–2510. [Google Scholar] [CrossRef]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jimenez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Siegal, D.M.; Freedman, D.; Ansell, J. Urgent procedures or surgeries in patients receiving oral anticoagulants: A systematic literature review. J. Thromb. Thrombolysis 2023, 55, 197–202. [Google Scholar] [CrossRef]
- Pollack, C.V., Jr.; Reilly, P.A.; van Ryn, J.; Eikelboom, J.W.; Glund, S.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kam, C.W.; et al. Idarucizumab for Dabigatran Reversal—Full Cohort Analysis. N. Engl. J. Med. 2017, 377, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Crowther, M.; Eikelboom, J.W.; Gibson, C.M.; Curnutte, J.T.; Lawrence, J.H.; Yue, P.; Bronson, M.D.; Lu, G.; Conley, P.B.; et al. Full Study Report of Andexanet Alfa for Bleeding Associated with Factor Xa Inhibitors. N. Engl. J. Med. 2019, 380, 1326–1335. [Google Scholar] [CrossRef] [PubMed]
- Lindhoff-Last, E.; Birschmann, I.; Kuhn, J.; Lindau, S.; Konstantinides, S.; Grottke, O.; Nowak-Gottl, U.; Lucks, J.; Zydek, B.; von Heymann, C.; et al. Pharmacokinetics of Direct Oral Anticoagulants in Emergency Situations: Results of the Prospective Observational RADOA-Registry. Thromb. Haemost. 2022, 122, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Gressenberger, P. Reversal strategies in patients treated with direct oral anticoagulants. Vasa 2019, 48, 389–392. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, D.I.; Abdulla, K.; Yang, H.; Sundaresan, S.; Doering, P.; Vaswani, S.G.; Thavorn, K.; Forster, A.J. Association of delay of urgent or emergency surgery with mortality and use of health care resources: A propensity score-matched observational cohort study. CMAJ 2017, 189, E905–E912. [Google Scholar] [CrossRef] [PubMed]
- Lindhoff-Last, E. Direct oral anticoagulants (DOAC)—Management of emergency situations. Hamostaseologie 2017, 37, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Lindhoff-Last, E.; Herrmann, E.; Lindau, S.; Konstantinides, S.; Grottke, O.; Nowak-Goettl, U.; Lucks, J.; Zydek, B.; Heymann, C.V.; Birschmann, I.; et al. Severe Hemorrhage Associated With Oral Anticoagulants. Dtsch. Arztebl. Int. 2020, 117, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Godon, A.; Gabin, M.; Levy, J.H.; Huet, O.; Chapalain, X.; David, J.S.; Tacquard, C.; Sattler, L.; Minville, V.; Memier, V.; et al. Management of urgent invasive procedures in patients treated with direct oral anticoagulants: An observational registry analysis. Thromb. Res. 2022, 216, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Bavalia, R.; Abdoellakhan, R.; Brinkman, H.J.M.; Brekelmans, M.P.A.; Hamulyak, E.N.; Zuurveld, M.; Hutten, B.A.; Westerweel, P.E.; Olie, R.H.; Ten Cate, H.; et al. Emergencies on direct oral anticoagulants: Management, outcomes, and laboratory effects of prothrombin complex concentrate. Res. Pract. Thromb. Haemost. 2020, 4, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Lindhoff-Last, E.; Birschmann, I.; Bidenharn, A.J.; Kuhn, J.; Lindau, S.; Konstantinides, S.; Grottke, O.; Nowak-Gottl, U.; Lucks, J.; Zydek, B.; et al. Pharmacokinetics of Phenprocoumon in Emergency Situations-Results of the Prospective Observational RADOA-Registry (Reversal Agent Use in Patients Treated with Direct Oral Anticoagulants or Vitamin K Antagonists Registry). Pharmaceuticals 2022, 15, 1437. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Total (n = 78) | DOAC 4 (n = 44) | VKA (n = 34) | p-Values 1 | |
|---|---|---|---|---|
| Demographic data | ||||
| Female sex | 31 (40%) | 23 (52%) | 8 (26%) | 0.012 |
| Age (years) | 76.5 (43–94) | 75.5 (43–94) | 76.5 (46–91) | >0.20 |
| Acute renal failure | 5 (6%) | 2 (5%) | 3 (9%) | >0.20 |
| Surgery type | ||||
| traumatic | 31 (40%) | 24 (55%) | 7 (21%) | 0.003 |
| fractures | 27 (35%) | 20 (46%) | 7 (21%) | 0.031 |
| acute abdomen | 23 (30%) | 12 (27%) | 11 (32%) | >0.20 |
| GI tract | 18 (23%) | 9 (21%) | 9 (27%) | >0.20 |
| CNS | 3 (4%) | 2 (5%) | 1 (3%) | >0.20 |
| abscess | 1 (1%) | 1 (2%) | 0 (0.0%) | -- |
| Open-heart surgery | 11 (14%) | 4 (9%) | 7 (21%) | 0.195 |
| vascular | 7 (9%) | 2 (5%) | 5 (15%) | >0.20 |
| other | 6 (8%) | 3 (7%) | 3 (9%) | >0.20 |
| Co-medication, indication for anticoagulation and bleeding risk | ||||
| Antiplatelet drugs | 11 (14%) | 6 (14%) | 5 (15%) | >0.20 |
| Anti-inflammatory drugs | 4 (5%) | 1 (2%) | 3 (9%) | >0.20 |
| Indication | 0.155 | |||
| atrial fibrillation | 58 (74%) | 34 (77%) | 24 (71%) | |
| venous thrombosis | 5 (6%) | 4 (9%) | 1 (3%) | |
| postoperative prophylaxis | 4 (5%) | 1 (2%) | 3 (9%) | |
| arterial thrombosis | 4 (5%) | 1 (2%) | 3 (9%) | |
| artificial heart valve | 2 (3%) | 0 (0%) | 2 (6%) | |
| other | 5 (6%) | 4 (9%) | 1 (3%) | |
| CHADS-VASC Score | 5.0 (1.0–9.0) | 5.0 (2.0–9.0) | 5.0 (1.0–8.0) | >0.20 |
| HASBLED Score 2 | 3.0 (0.0–5.0) | 2.0 (0.0–4.0) | 3.0 (0.0–5.0) | 0.126 |
| HASBLED Score modified 3 | 2.0 (0.0–5.0) | 2.0 (0.0–4.0) | 3.0 (0.0–5.0) | >0.20 |
| Delay of Emergency Surgery in Hours | DOAC (n = 44) | VKA (n = 34) |
|---|---|---|
| No delay | 35 (80%) | 27 (79%) |
| 4–6 h | 4 (9%) | 4 (12%) |
| 7–12 h | 2 (5%) | 1 (3%) |
| 13–24 h | 3 (7%) | 2 (6%) |
| Patient/ Anticoagulant | Age | Gender | INR/DOAC Level | Type of Surgery | Preoperative Treatment | Bleeding ≤24 h after Admission | Postoperative Hemostatic Treatment ≤24 h after Admission | INR-Rebound | Repeat Surgery | Bleeding > 24 h after Admission | Postoperative Hemostatic Treatment > 24 h after Admission | In-Hospital Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VKA1 | 66 | m | 3.9 | acute abdomen | PCC | yes | PCC, RBC, Vit K | yes | yes | no | - | no |
| VKA2 | 64 | m | 2.8 | open heart surgery | TA | yes | PCC, FFP, TA, P, RBC, PC | no | no | no | - | no |
| VKA3 | 82 | m | 2.2 | open heart surgery | no | yes | PCC, FFP, TA, P, RBC, PC | yes | no | no | - | yes, day 22 # |
| VKA4 | 53 | m | 1.4 | open heart surgery | no | yes | PCC, FFP, TA, P, RBC, PC, F | no | no | no | - | no |
| VKA5 | 66 | m | 2.0 | gluteal fasciitis | no | no | PCC | yes | yes | yes, day 3 | PCC, FFP, TA, RBC, F, PCC, Vit K, aFVII, FXIII | yes, day 14 # |
| VKA6 | 81 | m | 3.1 | subdural hematoma | PCC, TA | yes | PCC, RBC, Vit K | yes | yes | yes, day 2 | PCC | yes, day 2 ## |
| VKA7 | 69 | m | 1.8 | peripheral artery occlusion | PCC, Vit K | no | TA, P | yes | yes | yes, day 8 | FFP, RBC, Vit K | no |
| DOAC 1 * | 89 | f | 279 ng/mL | acute abdomen | PCC | yes | PCC, Vit k, TA | - | yes | yes, day 2 | PCC | no |
| DOAC 2 ** | 74 | m | 333 ng/mL | open heart surgery | no | yes | - | - | yes | yes, day 1–3 | PCC, FFP, RBC, PC, F, aFVII | no |
| DOAC 3 *** | 72 | m | 62 ng/mL | open heart surgery | no | yes | PCC, Vit k, TA, P | - | no | yes, day 3–4 | PCC, RBC, PC, F, Vit K | yes, day 7 # |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Last, J.; Herrmann, E.; Birschmann, I.; Lindau, S.; Konstantinides, S.; Grottke, O.; Nowak-Göttl, U.; Zydek, B.; von Heymann, C.; Sümnig, A.; et al. Clinical Course and Management of Patients with Emergency Surgery Treated with Direct Oral Anticoagulants or Vitamin K Antagonists—Results of the German Prospective RADOA-Registry. J. Clin. Med. 2024, 13, 272. https://doi.org/10.3390/jcm13010272
Last J, Herrmann E, Birschmann I, Lindau S, Konstantinides S, Grottke O, Nowak-Göttl U, Zydek B, von Heymann C, Sümnig A, et al. Clinical Course and Management of Patients with Emergency Surgery Treated with Direct Oral Anticoagulants or Vitamin K Antagonists—Results of the German Prospective RADOA-Registry. Journal of Clinical Medicine. 2024; 13(1):272. https://doi.org/10.3390/jcm13010272
Chicago/Turabian StyleLast, Jana, Eva Herrmann, Ingvild Birschmann, Simone Lindau, Stavros Konstantinides, Oliver Grottke, Ulrike Nowak-Göttl, Barbara Zydek, Christian von Heymann, Ariane Sümnig, and et al. 2024. "Clinical Course and Management of Patients with Emergency Surgery Treated with Direct Oral Anticoagulants or Vitamin K Antagonists—Results of the German Prospective RADOA-Registry" Journal of Clinical Medicine 13, no. 1: 272. https://doi.org/10.3390/jcm13010272
APA StyleLast, J., Herrmann, E., Birschmann, I., Lindau, S., Konstantinides, S., Grottke, O., Nowak-Göttl, U., Zydek, B., von Heymann, C., Sümnig, A., Beyer-Westendorf, J., Schellong, S., Meybohm, P., Greinacher, A., & Lindhoff-Last, E., on behalf of the RADOA-Registry Investigators. (2024). Clinical Course and Management of Patients with Emergency Surgery Treated with Direct Oral Anticoagulants or Vitamin K Antagonists—Results of the German Prospective RADOA-Registry. Journal of Clinical Medicine, 13(1), 272. https://doi.org/10.3390/jcm13010272