Abstract
Background and objective: Sex plays a role in Parkinson’s disease (PD) mechanisms. We analyzed sex difference manifestations among Spanish patients with PD. Patients and Methods: PD patients who were recruited from the Spanish cohort COPPADIS from January 2016 to November 2017 were included. A cross-sectional and a two-year follow-up analysis were conducted. Univariate analyses and general linear model repeated measure were used. Results: At baseline, data from 681 PD patients (mean age 62.54 ± 8.93) fit the criteria for analysis. Of them, 410 (60.2%) were males and 271 (39.8%) females. There were no differences between the groups in mean age (62.36 ± 8.73 vs. 62.8 ± 9.24; p = 0.297) or in the time from symptoms onset (5.66 ± 4.65 vs. 5.21 ± 4.11; p = 0.259). Symptoms such as depression (p < 0.0001), fatigue (p < 0.0001), and pain (p < 0.00001) were more frequent and/or severe in females, whereas other symptoms such as hypomimia (p < 0.0001), speech problems (p < 0.0001), rigidity (p < 0.0001), and hypersexuality (p < 0.0001) were more noted in males. Women received a lower levodopa equivalent daily dose (p = 0.002). Perception of quality of life was generally worse in females (PDQ-39, p = 0.002; EUROHIS-QOL8, p = 0.009). After the two-year follow-up, the NMS burden (Non-Motor Symptoms Scale total score) increased more significantly in males (p = 0.012) but the functional capacity (Schwab and England Activities of Daily Living Scale) was more impaired in females (p = 0.001). Conclusion: The present study demonstrates that there are important sex differences in PD. Long-term prospective comparative studies are needed.
1. Introduction
Previously published data indicated that there are sex differences in many features of Parkinson’s disease (PD) [1,2]. Incidence and prevalence of PD are between 1.5 and 2 times higher in men than in woman and disease onset in women is slightly later than in men [3,4]. Clinically, males have more rigidity and speech problems, whereas females seem to have a greater prevalence of dyskinesia and motor and non-motor response fluctuations but more mild motor deterioration [5,6,7]. Regarding non-motor symptoms (NMSs), some studies have observed that symptoms such as fatigue, depression, anxiety, and sleep problems are more frequent in females, whereas other NMSs such as drooling, diurnal somnolence, urinary and sexual dysfunction, and cognitive problems are more prevalent in males [8,9,10]. However, the results are not consistent due to the great heterogeneity between the studies [2], including aspects such as the sample (e.g., differences in age, disease duration, or race), the type of evaluation conducted, or the follow-up period. Although several findings indicate that estrogens may play a role in PD and explain some sex differences, other mechanisms such as gene expression, neuroinflammation, oxidative stress, and lifestyle factors could be involved [11,12]. From a practical point of view, precise identification of the sex differences is important to tailor treatment, predict outcomes, and meet other individual and social needs in women and men with PD. In particular, it may be important to know sex differences in a specific population (i.e., in a province and/or a country) with the intention of developing global care strategies that can improve health care [13].
Although some epidemiological studies about PD have been conducted in Spain, the differences in motor and NMSs and disease progression between males and females in Spanish PD patients are unclear [14,15]. The aim of the present study was to analyze the main sex differences among Spanish patients with PD using data obtained from the COPPADIS cohort [16], the largest cohort of patients with PD studied in Spain to date. Specifically, we analyzed the differences between both sexes in terms of motor and NMSs, quality of life (QoL), autonomy, and disease progression.
2. Material and Methods
Patients with PD who were recruited from 35 centers of 14 Autonomous Communities of Spain from the COPPADIS cohort [16] from January 2016 to November 2017 were included in the present study. Methodology about the COPPADIS-2015 study can be consulted in https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-016-0548-9 (accessed on 31 January 2023) [17]. This is a multi-center, observational, longitudinal-prospective, five-year follow-up study designed to analyze disease progression in a Spanish population of PD patients. All patients included were diagnosed according to UK PD Brain Bank criteria [18].
Specifically, the present study is a post hoc analysis with two parts. The first part included a cross-sectional analysis comparing data collected from the baseline visit (V0) regarding sex. The second was a longitudinal prospective analysis to compare the change between males and females in PD characteristics from the baseline visit (V0) to a follow-up visit at 24 months ± 1 month (V24M). For some variables, data about baseline visit, 12 months ± 1 month (V12M), and V24M were available.
PD Patient Assessment
In PD subjects, information on sociodemographic aspects, factors related to PD, comorbidity, and treatment was collected at baseline (visit V0) and at 24 months ± 1 month (visit V24M). V0 and V24M evaluations included (1) motor assessment (Hoenh and Yahr [HY], Unified Parkinson’s Disease Rating Scale [UPDRS] part III and part IV [19], Freezing of Gait Questionnaire [FOGQ]), (2) NMSs (Non-Motor Symptoms Scale [NMSS], Parkinson’s Disease Sleep Scale [PDSS], Visual Analog Scale-Pain [VAS-Pain], Visual Analog Fatigue Scale [VAFS]), (3) cognition (PD-CRS), (4) mood and neuropsychiatric symptoms (BDI-II, Neuropsychiatric Inventory [NPI], Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale [QUIP-RS]), (5) disability (Schwab and England Activities of Daily Living Scale [ADLS]), and (6) health-related (the 39-item Parkinson’s disease Questionnaire [PDQ-39]) and global QoL (the EUROHIS-QOL 8-item index EUROHIS-QOL8]) [17]. At V12M, only the UPDRS, NMSS, and ADLS were assessed. In all the scales/questionnaires, a higher score indicates a more severe affectation except PD-CRS, PDSS, ADLS, and EUROHIS-QOL8, which is the opposite. Total score of the PDQ-39 (PDQ-39SI) and each domain of the NMSS and the PDQ-39 was expressed as a percentage: (score/total score) × 100 [20]. In patients with motor fluctuations, the motor assessment was made during the OFF state (without medication during the last 12 h) and during the ON state. The assessment was only performed without medication in patients without motor fluctuations. Non-motor assessment was conducted after taking medication.
The presence of motor fluctuations and dyskinesia was assessed according to the UPDRS-IV (items 39 and 32, respectively) [19]. FOG was defined according to the FOGQ-item 3 [21,22]. Motor phenotype was calculated based on a previously published formula [23,24]. Very severe NMS burden was defined as a NMSS total score >70 [20]. Patient with a score <81 on the PD-CRS were considered as with cognitive impairment [25,26]. Patients were classified as with major depression according to the DSM-IV criteria [27,28]. Impulse control disorder (ICD) (pathological gambling, compulsive shopping, hypersexuality, and compulsive eating behavior) and compulsive behavior (CB) (punding, hobbyism, and dopamine dysregulation syndrome) were defined according to the previously published cutoff points of the QUIP-RS: gambling ≥6, buying ≥8, sex ≥8, eating ≥7, hobbyism–punding ≥7 [28,29]. For dopamine dysregulation syndrome, we accounted for the investigator’s criterion since an established cutoff does not exist [30].
3. Data Analysis
Data were processed using SPSS 20.0 for Windows. Only PD patients with data available in both visits at V0 and at V24M were considered valid for the longitudinal analysis. For comparisons between males and females, Student’s t-test, the Mann–Whitney U test, chi-square test, or Fisher’s test, were used as appropriate (distribution for variables was verified by one-sample Kolmogorov–Smirnov test).
General linear model (GLM) repeated measure were used to test for changes in various scores (motor; NMS; QoL; autonomy for ADL) over time (V24M vs. V0 and/or V24M vs. V12M and V12M vs. V0) separately in each group (men vs. women) and test for differences between groups over time. Age at baseline, and levodopa equivalent daily dose (LEDD [31]) at baseline and at V24M were included as covariates. In the latter models, an interaction for visit and group was tested before testing for a group difference over time. Cohen’s d formula was applied for measuring the effect size in both groups, males and females. It was considered: <0.2–Negligible; 0.2–0.49–Small; 0.50–0.79–Moderate; ≥0.80–Large. The Bonferroni method was used to p value correction for multiple comparisons and a p ≤ 0.002 was considered significant.
4. Results
At baseline, data from 681 PD patients (mean age 62.54 ± 8.93) were valid for the analysis. Of them, 410 (60.2%) were males and 271 (39.8%) females. There were no differences between both groups (males vs. females) in mean age (62.36 ± 8.73 vs. 62.8 ± 9.24; p = 0.297) or in the time from symptoms onset (5.66 ± 4.65 vs. 5.21 ± 4.11; p = 0.259). Compared to males, to be single (11.1% vs. 4.4%; p < 0.0001) and living alone (15.6% vs. 7.6%; p < 0.0001) was more frequent in females (Table 1). To be taking antidepressant agents (33.3% vs. 18.1%; p < 0.0001), benzodiazepines (23.2% vs. 11.2%; p < 0.0001), and analgesics (31% vs. 19.8%; p = 0.002) was more frequent in females as well. Up to 91.1% of females were non-drinkers compared to 71.1% of males (p < 0.0001). Regarding antiparkinsonian treatment, LEDD (607.79 ± 432.61 vs. 503.71 ± 381.49; p = 0.002) was higher in males than in females.

Table 1.
Sociodemographic and lifestyle variables and comorbidities in PD patients from the COPPADIS cohort at baseline (V0) regarding sex (n = 681).
Although no differences in the score of the motor scales (HY, UPDRS-III, UPDRS-IV, FOGQ) were observed between sexes (Table 2), sub-scores of the UPDRS-III (OFF) detected a greater severity in hypomimia, speech, and rigidity (p < 0.0001 for all analysis) in males compared to females (Table 3 and Figure 1A). Regarding NMSs, females had a higher score on the BDI-II (9.95 ± 7.89 vs. 7.95 ± 6.84; p = 0.001) and major depression almost doubled (22.9% vs. 12%; p < 0.0001) in females when compared to males. The scores on the VAS about pain and physical fatigue were higher also in females (Table 2). Although the frequency of ICD (12.2%) and CB (9.3%) was similar in both sexes (Table 3), hypersexuality was clearly more frequent in males (7.6% vs. 0.4%; p < 0.0001). There were no differences between males and females in the NMSS total score (43.49 ± 36.89 vs. 47.94 ± 39.52; p = 0.208) but by domains, a trend in significance was detected for a greater burden in sleep/fatigue (18.03 ± 16.72 vs. 15.35 ± 15.63; p = 0.041), mood/apathy (13.78 ± 17.96 vs. 9.79 ± 15.19; p = 0.003), and miscellaneous (16.98 ± 16.71 vs. 13.56 ± 14.49; p = 0.010) in females whereas in urinary symptoms (22.48 ± 22.22 vs. 20.29 ± 22.84; p = 0.047) in males (Table 3 and Figure 1B). The results regarding global, fronto-subcortical, and posterior cortical cognitive function as a whole were similar in both groups (Table 3).
Table 2.
Different PD-related variables in PD patients from the COPPADIS cohort at baseline (V0) regarding sex (n = 681).
Table 3.
Differences in motor aspects, cognition, impulsive-compulsive behaviors, and QoL between men and women with PD from the COPPADIS cohort at baseline (V0) (n = 681).
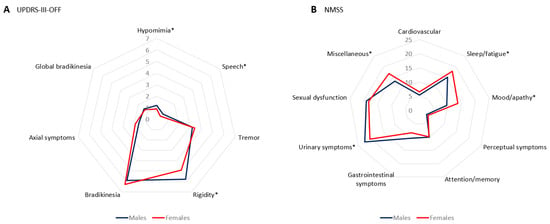
Figure 1.
(A) Mean score of sub-scores of the UPDRS-III-OFF at baseline in PD males vs. females; *, p < 0.0001. (B) Mean score on each domain of the NMSS at baseline in PD males vs. females; *, p < 0.05; Sleep/fatigue, p = 0.041; Mood/apathy, p = 0.003; Urinary symptoms, p = 0.047; Miscellaneous, p = 0.010.
The perception of health-related QoL (PDQ-39SI, 18.88 ± 13.76 vs. 16.05 ± 13.33; p = 0.002) was worse in females. “Emotional well-being” (25.64 ± 20.97 vs. 18.6 ± 18.72; p < 0.0001) and “Pain and discomfort” (33.76 ± 24.31 vs. 21.46 ± 20.2; p < 0.0001) were the domains of the PDQ-39 with the clearest differences with a greater severity in females (Table 3 and Figure 2A), but “Communication” was worse in males (11.99 ± 16.24 vs. 7.74 ± 13.52; p < 0.0001). With regard to the EUROHIS-QOL8, a trend in significance was detected for a worse perception in females in the total score (3.71 ± 0.56 vs. 3.82 ± 0.53; p = 0.009) and in “Quality of life” (3.73 ± 0.72 vs. 3.86 ± 0.7; p = 0.014), “Health status” (3.07 ± 0.87 vs. 3.23 ± 0.87; p = 0.020), and “Energy” (3.65 ± 0.88 vs. 3.84 ± 0.77; p = 0.004) (Table 3 and Figure 2B). No differences were detected between males and females in terms of autonomy for activities of daily living (ADL) (Table 2).
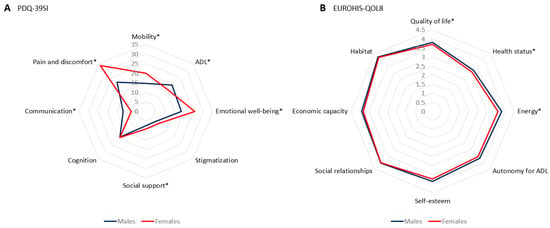
Figure 2.
(A) Mean score of each domain of the PDQ-39 at baseline in PD males vs. females; *, p < 0.05; Mobility, p = 0.01; ADL, Activities of daily living, p = 0.034; Emotional well-being, p < 0.0001; Social support, p = 0.046; Communication, p < 0.0001; Pain and discomfort, p < 0.0001. ADL: Activities of daily living (ADL): (B) Mean score on each domain of the EUROHIS-QOL8 at baseline in PD males vs. females; *, p < 0.05; Quality of life, p = 0.014; Health status, p = 0.020; Energy, p = 0.04.
Although the score on the UPDRS-III increased significantly from V0 to V24M in both groups, males and females, the difference between them was not significant (p = 0.554) (Table 4 and Figure 3). However, hypomimia and speech impairment from V0 to V24M in males but not in females was highly significant (p < 0.0001) (Table 4). Collectively, we observed an impairment of NMS burden (NMSS total score) after the two-year follow-up in both groups (Table 4 and Figure 3), with a trend in significance in males than in females (Cohen’s d, 0.43 vs. 0.25; difference between groups, p = 0.012). From V0 to V24M, functional capacity for ADL (ADLS) was impaired in males (from 89.12 ± 9.08 to 85.23 ± 12.58; p < 0.0001) and females (from 87.91 ± 11.42 to 82.76 ± 14.69; p < 0.0001), but the effect was greater in females than in males (p = 0.001; Table 4). Although LEDD tended to be higher in males than in females in all visits (n = 470; V0, 624.37 ± 434.36 vs. 514.88 ± 379.45 [p = 0.006]; V12M, 702.06 ± 401.64 vs. 621.96 ± 432.72 [p = 0.010]; V24M, 808.55 ± 460.97 vs. 726.31 ± 460.68 [p = 0.017]) (Figure 3), similar results were detected after dividing LEDD by weight (males vs. females, n = 450; V0, 7.81 ± 5.52 vs. 7.74 ± 6.07 [p = 0.550]; V12M, 8.71 ± 4.97 vs. 9.47 ± 6.96 [p = 0.782]; V24M, 10.94 ± 6.16 vs. 10.58 ± 7.44 [p = 0.166]).
Table 4.
Changes from the baseline visit (V0) to the two-year follow-up visit (V24M) in different PD-related variables in PD patients from the COPPADIS cohort regarding sex (n = 496).
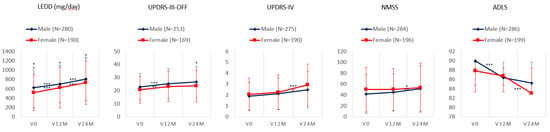
Figure 3.
Mean and standard deviation at V0, V12M, and V24M in males vs. females in the LEDD (mg/day) and the score on UPDRS-III-OFF, UPDRS-IV, NMSS, and ADLS; *, p < 0.05; **, p < 0.001; ***, p < 0.0001. The symbol above the line represents the significance of the change between one visit and another (in men and women) while the symbol above the point/diamond represents the difference in that visit between men and women. ADLS, Schwab and England Activities of Daily Living Scale; LEDD, levodopa equivalent daily dose; NMSS, Non-Motor Symptoms Scale; UPDRS, Unified Parkinson’s Disease Rating Scale.
Finally, after comparison of all data of baseline visit (variables included in Table 1 and Table 2) between patients who were assessed at V24M (n = 496) and those patients who were lost to follow-up at V24M (n = 185), no significant differences were detected (only p < 0.005 in the PDSS total score, with a worse quality of sleep in patients who lost the follow-up; 108.87 ± 32.28 vs. 117.02 ± 24.47; p = 0.019).
5. Discussion
The present study analyzes the differences between Spanish males and females with PD in motor features, NMSs, QoL, and autonomy for ADL. This is the first study carried out in Spain that analyzes sex differences in a large cohort and one of the largest studies with longitudinal data and detailed evaluations carried out to date. Depression, fatigue, pain, and a worse QoL were more frequent in females whereas hypomimia, speech problems, and hypersexuality were associated with the male sex. In the short-term, males showed a tendency to develop a greater NMS burden impairment, but females deteriorated more in their functional capacity to perform their ADL. To know the differences in PD progression by sex is important because it allows for more personalized medicine, considering age, race, sex, and cultural context has become the vanguard of delivery of care [32].
Multiple studies analyzing sex differences in PD have been published to date. Many of them have been case-control, retrospective, or cross-sectional studies, and lack consistent findings [2]. In our cross-sectional analysis, we detected many differences between males and females but not in age and time from symptoms onset, so both groups were appropriate to compare. Aligning with our results, previous studies observed that women are more likely to live alone; however, while a spouse or partner is the most likely individual to serve as a caregiver, homebound women are more likely to be single or widowed compared to men [33]. Additionally, in our cohort, primary education, to receive more drugs for other diseases, and assistance to a PD association tended to be more frequent in women, as opposed to harmful habits (smoking and alcohol consumption), which were significantly more frequent in males. Although lifestyle factors are important in PD [34], reviews about the differences in PD by sex lack information about these factors and focus more other aspects [1,2,11,35,36,37,38,39].
Sex-related differences have been documented in several aspects of PD, including motor features, response to levodopa, NMSs, and QoL, among others [1,2,4,5,6,7,8,9,10,11,35,36,37,38,39]. Motor symptoms emerge later in women, including specific characteristics such as reduced rigidity [6,40,41] but also more risk of falling [11,41], as we found. On the contrary, speech problems, in line with our findings, freezing of gait, and drooling are more associated with male sex [1,2,11,42,43]. Although the frequency of hypomimia seems to be no different between sexes [44], we identified it as more severe in males. In fact, both axial signs, hypomimia, and speech problems were impaired after a two-year follow-up in males but not in females. Other axial symptoms such as camptocormia have been related to male sex as well [45]. Although the score on the UPDRS-III during the OFF state was higher in males from our cohort in all visits compared to females, the differences were not significant, nor was motor progression in both groups at the follow-up. Using data from the PPMI cohort, Picillo et al. [5] detected in a five-year longitudinal analysis that men had more longitudinal progression in clinician-assessed motor features in the ON medication state but a similar increase over time of MDS-UPDRS part III OFF scores in both sexes. Other studies suggests that women with PD have milder motor symptoms compared to men with PD [46]. However, Abraham et al. [47] observed similar rates of progression between males and females until 20 years post-diagnosis, and only women had a quicker rate of progression after this period. A prior study with a ten-year follow-up had found that females had slower initial but faster later impairment progression [48]. Thus, this point is not clear, being an important research area to understand underlying reasons for this heterogeneity in PD progression [49]. Specifically, different genetic, hormonal, neuroendocrinal, and molecular players contribute towards the differences in PD pathogenesis [12,13]. Regarding motor complications, several studies reported a high incidence in females [50,51,52]. We did not find differences in the frequency of motor fluctuations and dyskinesia at baseline between males and females. Additionally, although the UPDRS-IV score was impaired after a two-year follow-up more in females, only a trend in significance was detected. Despite this difference observed in many studies, women with PD did not receive different treatments compared with men, suggesting that non-motor fluctuations in women remain mostly undertreated [53]. In our analysis, LEDD was lower in females at baseline (all cohort) and tended to be lower in all visits (subgroup with data available in all visits), which has been previously reported [5]. However, no differences between both groups were detected when LEDD was divided by weight, which could suggest a similar management in terms of dose requirement. Interestingly, tremor was the only motor sign that decreased after the two-year follow-up in both groups in our cohort. It is well known that motor PD subtype is instable and some cases with tremor-dominant type change to non-tremor subtype in the short-term [23].
There is currently a large amount of evidence available on the sex differences in the spectrum of NMSs in PD patients [11]. However, there are many scales validated to assess different NMSs in PD and this could contribute to heterogeneous results in some respects [2]. PD women have more depression, sleep problems, fatigue, and pain [1,2,8,11,54,55,56,57,58,59]. However, urinary symptoms and sexual dysfunction seem to be more prevalent in men [1,2,8,58,60]. In our cohort, depression was double in women than men. Women also were receiving more frequent antidepressant agents, benzodiazepines, and analgesics. When considering NMSs as a whole, the results were inconsistent. According to Solla et al. [61], women had higher scores on the NMSS, including severe sleep difficulties, increased fatigue, and mood disorders, such as apathy, anxiety, sadness, depression, and lack of motivation, whereas men had higher sexual dysfunction levels. However, Nicoletti et al. [62] reported that the presence of NMSs was more strongly associated with male sex in a cross-sectional study conducted in 585 PD patients, but no differences were detected in another cross-sectional study conducted in 415 PD patients by Kang et al. [46]. In all these studies, the NMS burden was assessed with the same scale we used, the NMSS. Some studies suggest a greater NMS burden in males [61]. In particular, Picillo et al. [62] observed that men complained of a greater number of NMSs as compared to women in a two-year follow-up study as well. Here, we detected only a trend in significance after applying the Bonferroni test (p = 0.012) for a greater NMS burden increase in males after a two-year follow-up, without significant differences by sex in the change of the score of all domains of the NMSS. Although some studies reported that male PD patients have worse general cognitive abilities and that male sex is the primary predictive factor for mild cognitive impairment and its rapid progression in the severe stage of the disease [7,9,10,11,63], we did not find significant differences in the neuropsychiatric symptoms. Regarding ICD and/or CB, the frequency was according to the literature [64] and hypersexuality was the only ICD significantly more frequent in males, being present in 7.6% of them. A recent review reported a mean prevalence of hypersexuality of 3.5% in PD patients and quite convincing demographic data indicating that patients are often males on dopamine agonists [65]. Finally, females have significantly less social support, more psychological distress, and worse self-reported disability and health-related QoL compared to males [47,66,67,68]. In our analysis, we detected differences with a worse perception by females, especially in emotional well-being, pain, and discomfort. Few studies have analyzed differences in the changes over time to develop the ADL in PD between sexes. We detected an impairment in the functional capacity in both sexes after the two-year follow-up conducted, but more significantly in women, as Sperens et al. [69] reported in an eight-year follow-up study conducted in 129 PD patients, with a worse impairment in women in domains such as shopping and cleaning. Other studies emphasize the importance of the progressive disability of women with PD, influencing aspects, such as polypharmacy or comorbidities, that translate into a consumption of health resources [56].
The present study has some limitations. Our findings may not be applicable to all PD patients in the community clinical setting because PD patients enrolled in the COPPADIS study represent a selected population with less disability at baseline than the general population (e.g., no older than 75 years old, not being under a second-line therapy, etc.). For some variables, the information was not collected in all cases and the data in the follow-up were obtained in 496 patients of 681 initially included in the baseline analysis (72.8%), so they could influence the results. However, this percentage is even higher in other longitudinal prospective studies [70] and a bias of withdrawals of more affected patients was excluded after comparing subjects who were lost to follow-up vs. those who were not. Another important aspect is that, due to the large sample size, some differences observed could be statistically significant but not a minimum clinically important difference (e.g., differences detected in motor aspects such as hypomimia, speech, and rigidity) [71], so it is necessary to be cautious about the relevance of some differences detected. Moreover, the observational nature of the study does not provide support for a cause–effect relationship but can only suggest correlation between variables. Furthermore, the medication dose was not adjusted for the body mass index because these data were not collected, but we did do so by weight. On the other hand, and with the intention to reduce the instance of a false positive, we applied the Bonferroni test with a significant p value definition of ≤ 0.002. Finally, we described the differences between men and women with PD in our cohort, but we did not analyze other markers in this manuscript that could explain the reason for them [72]. Nonetheless, the strengths of our study include a large sample size, a very thorough assessment, a prospective longitudinal follow-up design, and the extensive clinical and demographic information recorded.
In conclusion, the present study supports the idea that there are sex differences in PD. Symptoms such as depression, fatigue, or pain seem to be more frequent and/or severe in females, whereas others such as hypomimia, speech problems, rigidity, or hypersexuality were more common in males. Moreover, women could have a worse perception of their QoL. All in all, more studies are needed to better understand the differences between males and females with PD, especially in the long-term follow-up, and their causes.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12041329/s1, Coppadis Study Group.
Author Contributions
Conception, organization, and execution of the project; statistical analysis; writing of the first draft of the manuscript; recruitment and/or evaluation of participants: D.S.-G.; collaboration in the preparation of the manuscript, review and critique: A.L., J.H.-V., C.C.B., M.J.F.P., I.G.D. and M.C.Í.-A.; review and critique; recruitment and/or evaluation of participants: J.H.-V., T.d.D.F., S.J., M.T.B., L.P., M.C., J.G.C., N.C., I.L., I.C., L.L.M., I.G.A., M.A.Á.R., V.G.M., V.N., V.P., J.D.G.-S., C.B., B.S.V., M.Á.S., L.V., S.E., E.C., F.C.P., J.C.M.C., P.S.A., M.G.A.L., N.L.A., I.G., J.K., M.M.G., M.S., J.R.M., C.V., M.K., J.G.A., R.A.R., C.O., L.M.L.D. and P.M.; recruitment and/or evaluation of participants: COPPADIS Study Group; review and critique, review of English style: D.M.; review and critique, supervision: P.M.-M. All authors have read and agreed to the published version of the manuscript.
Funding
COPPADIS and the present study were developed with the help of Fundación Española de Ayuda a la Investigación en Enfermedades Neurodegenerativas y/o de Origen Genético ( https://fundaciondegen.org/) and Alpha Bioresearch (www.alphabioresearch.com). Also, we received grants from the Spanish Ministry of Economy and Competitiveness [PI16/01575] co-founded by ISCIII (Concesión de subvenciones de Proyectos de Investigación en Salud de la convocatoria 2020 de la Acción Estratégica en Salud 2017–2020 por el proyecto “PROGRESIÓN NO MOTORA E IMPACTO EN LA CALIDAD DE VIDA EN LA ENFERMEDAD DE PARKINSON”) to develop a part of the COPPADIS project.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and ap-proved by Comité de Ética de la Investigación Clínica de Galicia from Spain (2014/534; 2/DEC/2014).
Informed Consent Statement
For this study, we received approval from the Comité de Ética de la Investigación Clínica de Galicia from Spain (2014/534; 02/DEC/2014) and written informed consents from all participants in this study were obtained. COPPADIS-2015 was classified by the AEMPS (Agencia Española del Medicamento y Productos Sanitarios) as a Post-authorization Prospective Follow-up study with the code COH-PAK-2014-01. Written informed consent from all participants in this study were obtained before the start of the study.
Data Availability Statement
The protocol and the statistical analysis plan are available on request. Deidentified participant data are not available for legal and ethical reasons.
Acknowledgments
We would like to thank all patients and their caregivers who collaborated in this study. Many thanks also to Fundación Española de Ayuda a la Investigación en Enfermedades Neurodegenerativas y/o de Origen Genético (https://fundaciondegen.org/, accessed on 31 January 2023), Alpha Bioresearch (www.alphabioresearch.com, accessed on 31 January 2023), Instituto de Salud Carlos III, and other institutions for helping us.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| Activities For Daily Living | ADL |
| Schwab and England Activities of Daily Living Scale | ADLS |
| Beck Depression Inventory-Ii | BDI-II |
| Caregiver Strain Index | CSI |
| Freezing Of Gait Questionnaire | FOGQ |
| Levodopa Equivalent Daily Dose | LEDD |
| Non-Motor Symptoms; Non-Motor Symptoms Scale | NMS |
| Neuropsychiatric Inventory | NPI |
| Parkinson’s Disease | PD |
| Parkinson’s Disease Cognitive Rating Scale | PD-CRS |
| The 39-Item Parkinson’s Disease Questionnaire Summary Index | PDQ-39 |
| Parkinson’s Disease Sleep Scale | PDSS |
| Quality Of Life | QoL |
| Questionnaire For Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale | QUIP-RS |
| Unified Parkinson’s Disease Rating Scale | UPDRS |
| Visual Analogue Scale | VAS |
References
- Picillo, M.; Nicoletti, A.; Fetoni, V.; Garavaglia, B.; Barone, P.; Pellecchia, M.T. The relevance of gender in Parkinson’s disease: A review. J. Neurol. 2017, 264, 1583–1607. [Google Scholar] [CrossRef] [PubMed]
- Russillo, M.C.; Andreozzi, V.; Erro, R.; Picillo, M.; Amboni, M.; Cuoco, S.; Barone, P.; Pellecchia, M.T. Sex Differences in Parkinson’s Disease: From Bench to Bedside. Brain Sci. 2022, 12, 917. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Park. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- A Haaxma, C.; Bloem, B.R.; Borm, G.F.; Oyen, W.J.G.; Leenders, K.L.; Eshuis, S.; Booij, J.; E Dluzen, D.; Horstink, M.W.I.M. Gender differences in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2007, 78, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; LaFontant, D.; Bressman, S.; Caspell-Garcia, C.; Coffey, C.; Cho, H.R.; Burghardt, E.L.; Dahodwala, N.; Saunders-Pullman, R.; Tanner, C.M.; et al. Sex-Related Longitudinal Change of Motor, Non-Motor, and Biological Features in Early Parkinson’s Disease. J. Park. Dis. 2022, 12, 421–436. [Google Scholar] [CrossRef]
- Baba, Y.; Putzke, J.D.; Whaley, N.R.; Wszolek, Z.K.; Uitti, R.J. Gender and the Parkinson’s disease phenotype. J. Neurol. 2005, 252, 1201–1205. [Google Scholar] [CrossRef]
- Liu, R.; Umbach, D.M.; Peddada, S.D.; Xu, Z.; Troster, A.I.; Huang, X.; Chen, H. Potential sex differences in non-motor symptoms in early drug-naïve Parkinson disease. Neurology 2015, 84, 2107–2115. [Google Scholar] [CrossRef]
- Martinez-Martin, P.A.P.; Pecurariu, C.F.; Odin, C.A.; van Hilten, J.; Antonini, A.; Rojo-Abuin, J.M.; Borges, V.; Trenkwalder, C.; Aarsland, D.; Brooks, D.; et al. Gender-related differences in the burden of non-motor symptoms in Parkinson’s disease. J. Neurol. 2012, 259, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Cholerton, B.; Johnson, C.O.; Fish, B.; Quinn, J.F.; Chung, K.A.; Peterson-Hiller, A.L.; Rosenthal, L.S.; Dawson, T.M.; Albert, M.S.; Hu, S.-C.; et al. Sex differences in progression to mild cognitive impairment and dementia in Parkinson’s disease. Park. Relat. Disord. 2018, 50, 29–36. [Google Scholar] [CrossRef]
- Szewczyk-Krolikowski, K.; Tomlinson, P.; Nithi, K.; Wade-Martins, R.; Talbot, K.; Ben-Shlomo, Y.; Hu, M.T. The influence of age and gender on motor and non-motor features of early Parkinson’s disease: Initial findings from the Oxford Parkinson Disease Center (OPDC) discovery cohort. Park. Relat. Disord. 2014, 20, 99–105. [Google Scholar] [CrossRef]
- Cerri, S.; Mus, L.; Blandini, F. Parkinson’s Disease in Women and Men: What’s the Difference? J. Park. Dis. 2019, 9, 501–515. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, B.; Dhamija, K.; Guru, P.; Sharma, S.S. Parkinson’s disease in women: Mechanisms underlying sex differences. Eur. J. Pharmacol. 2021, 895, 173862. [Google Scholar] [CrossRef] [PubMed]
- Göttgens, I.; van Halteren, A.D.; de Vries, N.M.; Meinders, M.J.; Ben-Shlomo, Y.; Bloem, B.R.; Darweesh, S.K.L.; Oertelt-Prigione, S. The Impact of Sex and Gender on the Multidisciplinary Management of Care for Persons With Parkinson’s Disease. Front. Neurol. 2020, 11, 576121. [Google Scholar] [CrossRef]
- Benito-Leon, J. Epidemiologia de la enfermedad de Parkinson en España y su contextualizacion mundial [Epidemiology of Parkinson’s disease in Spain and its contextualisation in the world]. Rev. Neurol. 2018, 66, 125–134. [Google Scholar] [PubMed]
- García-Ramos, R.; López Valdés, E.; Ballesteros, L.; Jesús, S.; Mir, P. The social impact of Parkinson’s disease in Spain: Report by the Spanish Foundation for the Brain. Neurologia 2016, 31, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Santos García, D.; Jesús, S.; Aguilar, M.; Planellas, L.L.; García Caldentey, J.; Caballol, N.; Legarda, I.; Hernández Vara, J.; Cabo, I.; López Manzanares, L.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015): An ongoing global Parkinson’s disease project about disease progression with more than 1000 subjects included. Results from the baseline evaluation. Eur. J. Neurol. 2019, 26, 1399–1407. [Google Scholar] [CrossRef]
- Santos-García, D.; Mir, P.; Cubo, E.; Vela, L.; Rodríguez-Oroz, M.C.; Martí, M.J.; Arbelo, J.M.; Infante, J.; Kulisevsky, J.; Martínez-Martín, P.; et al. COPPADIS-2015 (COhort of Patients with PArkinson’s DIsease in Spain, 2015), a global-clinical evaluations, serum biomarkers, genetic studies and neuroimaging-prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurol. 2016, 16, 26. [Google Scholar]
- Daniel, S.E.; Lees, A.J. Parkinson’s Disease Society Brain Bank, London: Overview and research. J. Neural. Transm. Suppl. 1993, 39, 165–172. [Google Scholar]
- Fahn, S.; Elton, R.L.; Members of the UPDRS Development Committee. Unified Parkinson’s disease rating scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsden, C.D., Calne, D.B., Goldstein, M., Eds.; Macmillan Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–164. [Google Scholar]
- Chaudhuri, K.R.; Rojo, J.M.; Schapira, A.; Brooks, D.; Stocchi, F.; Odin, P.; Antonini, A.; Brown, R.; Martinez-Martin, P. A Proposal for a Comprehensive Grading of Parkinson’s Disease Severity Combining Motor and Non-Motor Assessments: Meeting an Unmet Need. PLoS ONE 2013, 8, e57221. [Google Scholar] [CrossRef]
- Giladi, N.; Shabtai, H.; Simon, E.S.; Biran, S.; Tal, J.; Korczyn, A.D. Construction of freezing of gait questionnaire for patients with Parkinsonism. Park. Relat. Disord. 2000, 6, 165–170. [Google Scholar] [CrossRef]
- Santos-García, D.; on behalf of the COPPADIS Study Group; de Deus-Fonticoba, T.; Castro, E.S.; Díaz, M.A.; Feal-Painceiras, M.J.; Paz-González, J.M.; García-Sancho, C.; Jesús, S.; Mir, P.; et al. The impact of freezing of gait on functional dependency in Parkinson’s disease with regard to motor phenotype. Neurol. Sci. 2020, 41, 2883–2892. [Google Scholar] [CrossRef]
- Jankovic, J.; McDermott, M.; Carter, J.; Gauthier, S.; Goetz, C.; Golbe, L.; Huber, S.; Koller, W.; Olanow, C.; Shoulson, I.; et al. Variable expression of Parkinson’s disease: A base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 1990, 40, 1529–1534. [Google Scholar] [CrossRef]
- García, D.S.; Canfield, H.; Fonticoba, T.D.D.; Bartolomé, C.C.; Ríos, L.N.; Roca, L.G.; Miró, C.M.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Parkinson’s Disease Motor Subtypes Change with the Progression of the Disease: Results from the COPPADIS Cohort at 2-Year Follow-Up. J. Park. Dis. 2021, Preprint, 1–21. [Google Scholar] [CrossRef]
- Fernandez de Bobadilla, R.; Pagonabarraga, J.; Martinez-Horta, S.; Pascual-Sedano, B.; Campolongo, A.; Kulisevsky, J. Parkinson’s disease-cognitive rating scale: Psychometrics for mild cognitive impairment. Mov. Disord. 2013, 28, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Horta, S.; Bejr-Kasem, H.; Horta-Barba, A.; Pascual-Sedano, B.; Santos-García, D.; de Deus-Fonticoba, T.; Jesús, S.; Aguilar, M.; Planellas, L.; García-Caldentey, J.; et al. Identifying comorbidities and lifestyle factors contributing to the cognitive profile of early Parkinson’s disease. BMC Neurol. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Santos-García, D.; Fonticoba, T.D.D.; Bartolomé, C.C.; Castro, E.S.; Jesús, S.; Mir, P.; Pascual-Sedano, B.; Pagonabarraga, J.; Kulisevsky, J.; Hernández-Vara, J.; et al. Depression is Associated with Impulse-compulsive Behaviors in Parkinson’s disease. J. Affect. Disord. 2020, 280, 77–89. [Google Scholar] [CrossRef]
- Weintraub, D.; Mamikonyan, E.; Papay, K.; Shea, J.A.; Xie, S.X.; Siderowf, A. Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale. Mov. Disord. 2012, 27, 242–247. [Google Scholar] [CrossRef]
- Jesús, S.; Labrador-Espinosa, M.A.; Adarmes, A.D.; Barrio, C.M.-D.; Martínez-Castrillo, J.C.; Alonso-Cánovas, A.; Alonso, P.S.; Novo-Ponte, S.; Alonso-Losada, M.G.; Ariztegui, N.L.; et al. Non-motor symptom burden in patients with Parkinson’s disease with impulse control disorders and compulsive behaviours: Results from the COPPADIS cohort. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schade, S.; Mollenhauer, B.; Trenkwalder, C. Levodopa Equivalent Dose Conversion Factors: An Updated Proposal Including Opicapone and Safinamide. Mov. Disord. Clin. Pract. 2020, 7, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, I.; Mathur, S.; Oosterbaan, A.; Flanagan, R.; Keener, A.M.; Moro, E. Unmet Needs of Women Living with Parkinson’s Disease: Gaps and Controversies. Mov. Disord. 2022, 37, 444–455. [Google Scholar] [CrossRef]
- Nwabuobi, L.; Barbosa, W.; Sweeney, M.; Oyler, S.; Meisel, T.; Di Rocco, A.; Chodosh, J.; E Fleisher, J. Sex-related differences in homebound advanced Parkinson’s disease patients. Clin. Interv. Aging 2019, ume 14, 1371–1377. [Google Scholar] [CrossRef]
- Nag, N.; Jelinek, G.A. A Narrative Review of Lifestyle Factors Associated with Parkinson’s Disease Risk and Progression. Neurodegener. Dis. 2019, 19, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Augustine, E.F.; Perez, A.; Dhall, R.; Umeh, C.C.; Videnovic, A.; Cambi, F.; Wills, A.-M.A.; Elm, J.J.; Zweig, R.M.; Shulman, L.M.; et al. Sex Differences in Clinical Features of Early, Treated Parkinson’s Disease. PLoS ONE 2015, 10, e0133002. [Google Scholar] [CrossRef]
- Crispino, P.; Gino, M.; Barbagelata, E.; Ciarambino, T.; Politi, C.; Ambrosino, I.; Ragusa, R.; Marranzano, M.; Biondi, A.; Vacante, M. Gender Differences and Quality of Life in Parkinson’s Disease. Int. J. Environ. Res. Public Health 2020, 18, 198. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M. Gender differences in Parkinson’s disease. Gend. Med. 2007, 4, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.N.; Cronin-Golomb, A. Gender differences in Parkinson’s disease: Clinical characteristics and cognition. Mov. Disord. 2010, 25, 2695–2703. [Google Scholar] [CrossRef]
- Georgiev, D.; Hamberg, K.; Hariz, M.; Forsgren, L.; Hariz, G.M. Gender differences in Parkinson’s disease: A clinical perspective. Acta Neurol. Scand. 2017, 136, 570–584. [Google Scholar] [CrossRef]
- Shin, J.Y.; Pohlig, R.T.; Habermann, B. Self-Reported Symptoms of Parkinson’s Disease by Sex and Disease Duration. West. J. Nurs. Res. 2017, 39, 1412–1428. [Google Scholar] [CrossRef]
- Pellecchia, M.T.; Picillo, M.; Russillo, M.C.; De Pandis, M.F.; Bonizzoni, E.; Marjanovic, I.; Cattaneo, C. Efficacy of Safinamide and Gender Differences During Routine Clinical Practice. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef]
- Parashos, S.A.; Bloem, B.R.; Browner, N.M.; Giladi, N.; Gurevich, T.; Hausdorff, J.M.; He, Y.; Lyons, K.E.; Mari, Z.; Morgan, J.C.; et al. What predicts falls in Parkinson disease?: Observations from the Parkinson’s Foundation registry. Neurol. Clin. Pract. 2018, 8, 214–222. [Google Scholar] [CrossRef]
- Rusz, J.; Tykalová, T.; Novotný, M.; Zogala, D.; Růžička, E.; Dušek, P. Automated speech analysis in early untreated Parkinson’s disease: Relation to gender and dopaminergic transporter imaging. Eur. J. Neurol. 2022, 29, 81–90. [Google Scholar] [CrossRef]
- Ricciardi, L.; De Angelis, A.; Marsili, L.; Faiman, I.; Pradhan, P.; Pereira, E.A.; Edwards, M.J.; Morgante, F.; Bologna, M. Hypomimia in Parkinson’s disease: An axial sign responsive to levodopa. Eur. J. Neurol. 2020, 27, 2422–2429. [Google Scholar] [CrossRef]
- Ou, R.; Liu, H.; Hou, Y.; Song, W.; Cao, B.; Wei, Q.; Yuan, X.; Chen, Y.; Zhao, B.; Shang, H. Predictors of camptocormia in patients with Parkinson’s disease: A prospective study from southwest China. Park. Relat. Disord. 2018, 52, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.W.; Choi, S.M.; Kim, B.C. Gender differences in motor and non-motor symptoms in early Parkinson disease. Medicine 2022, 101, e28643. [Google Scholar] [CrossRef]
- Abraham, D.S.; Gruber-Baldini, A.L.; Magder, L.S.; McArdle, P.F.; Tom, S.E.; Barr, E.; Schrader, K.; Shulman, L.M. Sex differences in Parkinson’s disease presentation and progression. Park. Relat. Disord. 2019, 69, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Reinoso, G.; Allen, J.C., Jr.; Au, W.L.; Seah, S.H.; Tay, K.Y.; Tan, L.C. Clinical evolution of Parkinson’s disease and prognostic factors affecting motor progression: 9-year follow-up study. Eur. J. Neurol. 2015, 22, 457–463. [Google Scholar] [CrossRef]
- Sieber, B.A.; Landis, S.; Koroshetz, W.; Bateman, R.; Siderowf, A.; Galpern, W.R.; Montine, T.J.; Orr, H.T.; Torborg, C.; Montine, T.J.; et al. arkinson’s Disease 2014: Advancing Research, Improving Lives Conference Organizing Committee. Prioritized research recommendations from the National Institute of Neurological Disorders and Stroke Parkinson’s Disease 2014 Conference. Ann. Neurol. 2014, 76, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Colombo, D.; Abbruzzese, G.; Antonini, A.; Barone, P.; Bellia, G.; Franconi, F.; Simoni, L.; Attar, M.; Zagni, E.; Haggiag, S.; et al. The “gender factor” in wearing-off among patients with Parkinson’s disease: A post hoc analysis of DEEP study. Sci. World J. 2015, 2015, 787451. [Google Scholar] [CrossRef]
- Wan, Z.; Wang, X.; Ma, H.; Wang, Z.; Feng, T. Risk factors for motor complications in female patients with Parkinson’s disease. Neurol. Sci. 2022, 43, 4735–4743. [Google Scholar] [CrossRef] [PubMed]
- Andreasi, N.G.; Romito, L.M.; Telese, R.; Cilia, R.; Elia, A.E.; Novelli, A.; Tringali, G.; Messina, G.; Levi, V.; Devigili, G.; et al. Short- and long-term motor outcome of STN-DBS in Parkinson’s Disease: Focus on sex differences. Neurol. Sci. 2021, 43, 1769–1781. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Palladino, R.; Moccia, M.; Erro, R.; Amboni, M.; Vitale, C.; Barone, P.; Pellecchia, M.T. Gender and non motor fluctuations in Parkinson’s disease: A prospective study. Park. Relat. Disord. 2016, 27, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Farhadi, F.; Vosoughi, K.; Shahidi, G.A.; Delbari, A.; Lökk, J.; Fereshtehnejad, S.M. Sexual dimorphism in Parkinson’s disease: Differences in clinical manifestations, quality of life and psychosocial functioning between males and females. Neuropsychiatr. Dis. Treat. 2017, 13, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Perrin, A.J.; Nosova, E.; Co, K.; Book, A.; Iu, O.; Silva, V.; Thompson, C.; McKeown, M.; Stoessl, A.J.; Farrer, M.J.; et al. Gender differences in Parkinson’s disease depression. Park. Relat. Disord. 2017, 36, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Fullard, M.E.; Thibault, D.P.; Todaro, V.; Foster, S.; Katz, L.; Morgan, R.; Kern, D.S.; Schwalb, J.M.; Mendoza, E.U.; Dahodwala, N.; et al. Sex disparities in health and health care utilization after Parkinson diagnosis: Rethinking PD associated disability. Park. Relat. Disord. 2017, 48, 45–50. [Google Scholar] [CrossRef]
- Defazio, G.; Antonini, A.; Tinazzi, M.; Gigante, A.F.; Pietracupa, S.; Pellicciari, R.; Bloise, M.; Bacchin, R.; Marcante, A.; Fabbrini, G.; et al. Relationship between pain and motor and non-motor symptoms in Parkinson’s disease. Eur. J. Neurol. 2017, 24, 974–980. [Google Scholar] [CrossRef]
- Guo, X.; Song, W.; Chen, K.; Chen, X.; Zheng, Z.; Cao, B.; Huang, R.; Zhao, B.; Wu, Y.; Shang, H.-F. Gender and onset age-related features of non-motor symptoms of patients with Parkinson’s disease – A study from Southwest China. Park. Relat. Disord. 2013, 19, 961–965. [Google Scholar] [CrossRef]
- Silverdale, M.A.; Kobylecki, C.; Kass-Iliyya, L.; Martinez-Martin, P.; Lawton, M.; Cotterill, S.; Chaudhuri, K.R.; Morris, H.; Baig, F.; Williams, N.; et al. A detailed clinical study of pain in 1957 participants with early/moderate Parkinson’s disease. Park. Relat. Disord. 2018, 56, 27–32. [Google Scholar] [CrossRef]
- Hu, T.; Ou, R.; Liu, H.; Hou, Y.; Wei, Q.; Song, W.; Cao, B.; Chen, Y.; Yuan, X.; Shang, H. Gender and onset age related-differences of non-motor symptoms and quality of life in drug-naïve Parkinson’s disease. Clin. Neurol. Neurosurg. 2018, 175, 124–129. [Google Scholar] [CrossRef]
- Solla, P.; Cannas, A.; Ibba, F.C.; Loi, F.; Corona, M.; Orofino, G.; Marrosu, M.G.; Marrosu, F. Gender differences in motor and non-motor symptoms among Sardinian patients with Parkinson’s disease. J. Neurol. Sci. 2012, 323, 33–39. [Google Scholar] [CrossRef]
- Nicoletti, A.; Vasta, R.; Mostile, G.; Nicoletti, G.; Arabia, G.; Iliceto, G.; Lamberti, P.; Marconi, R.; Morgante, L.; Barone, P.; et al. Gender effect on non-motor symptoms in Parkinson’s disease: Are men more at risk? Park. Relat. Disord. 2017, 35, 69–74. [Google Scholar] [CrossRef]
- Picillo, M.; Erro, R.; Amboni, M.; Longo, K.; Vitale, C.; Moccia, M.; Pierro, A.; Scannapieco, S.; Santangelo, G.; Spina, E.; et al. Gender differences in non-motor symptoms in early Parkinson’s disease: A 2-years follow-up study on previously untreated patients. Park. Relat. Disord. 2014, 20, 850–854. [Google Scholar] [CrossRef]
- Gatto, E.M.; Aldinio, V. Impulse Control Disorders in Parkinson’s Disease. A Brief and Comprehensive Review. Front. Neurol. 2019, 10, 351. [Google Scholar] [CrossRef] [PubMed]
- Codling, D.; Shaw, P.; David, A.S. Hypersexuality in Parkinson’s Disease: Systematic Review and Report of 7 New Cases. Mov. Disord. Clin. Pract. 2015, 2, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Balash, Y.; Korczyn, A.D.; Migirov, A.A.; Gurevich, T. Quality of life in Parkinson’s disease: A gender-specific perspective. Acta Neurol. Scand. 2019, 140, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Meng, D.; Jin, Z.; Gao, L.; Wang, Y.; Wang, R.; Fang, J.; Qi, L.; Su, Y.; Liu, A.; Fang, B. The quality of life in patients with Parkinson’s disease: Focus on gender difference. Brain Behav. 2022, 12, e2517. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.-E.; Kim, J.S.; Jang, W.; Park, J.; Oh, E.; Youn, J.; Park, S.; Cho, J.W. Gender Differences of Nonmotor Symptoms Affecting Quality of Life in Parkinson Disease. Neurodegener. Dis. 2017, 17, 276–280. [Google Scholar] [CrossRef]
- Sperens, M.; Georgiev, D.; Eriksson Domellöf, M.; Forsgren, L.; Hamberg, K.; Hariz, G.M. Activities of daily living in Parkinson’s disease: Time/gender perspective. Acta Neurol. Scand. 2020, 141, 168–176. [Google Scholar] [CrossRef] [PubMed]
- García, D.S.; Fonticoba, T.D.D.; Cores, C.; Muñoz, G.; González, J.M.P.; Miró, C.M.; Suárez, E.; Jesús, S.; Aguilar, M.; Pastor, P.; et al. Predictors of clinically significant quality of life impairment in Parkinson’s disease. npj Park. Dis. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Schrag, A.; Sampaio, C.; Counsell, N.; Poewe, W. Minimal clinically important change on the unified Parkinson’s disease rating scale. Mov. Disord. 2006, 21, 1200–1207. [Google Scholar] [CrossRef]
- Gillies, G.E.; Pienaar, I.S.; Vohra, S.; Qamhawi, Z. Sex differences in Parkinson’s disease. Front. Neuroendocrinol. 2014, 35, 370–384. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).