

Heart Rate Reduction and Outcomes in Heart Failure Outpatients

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Methods
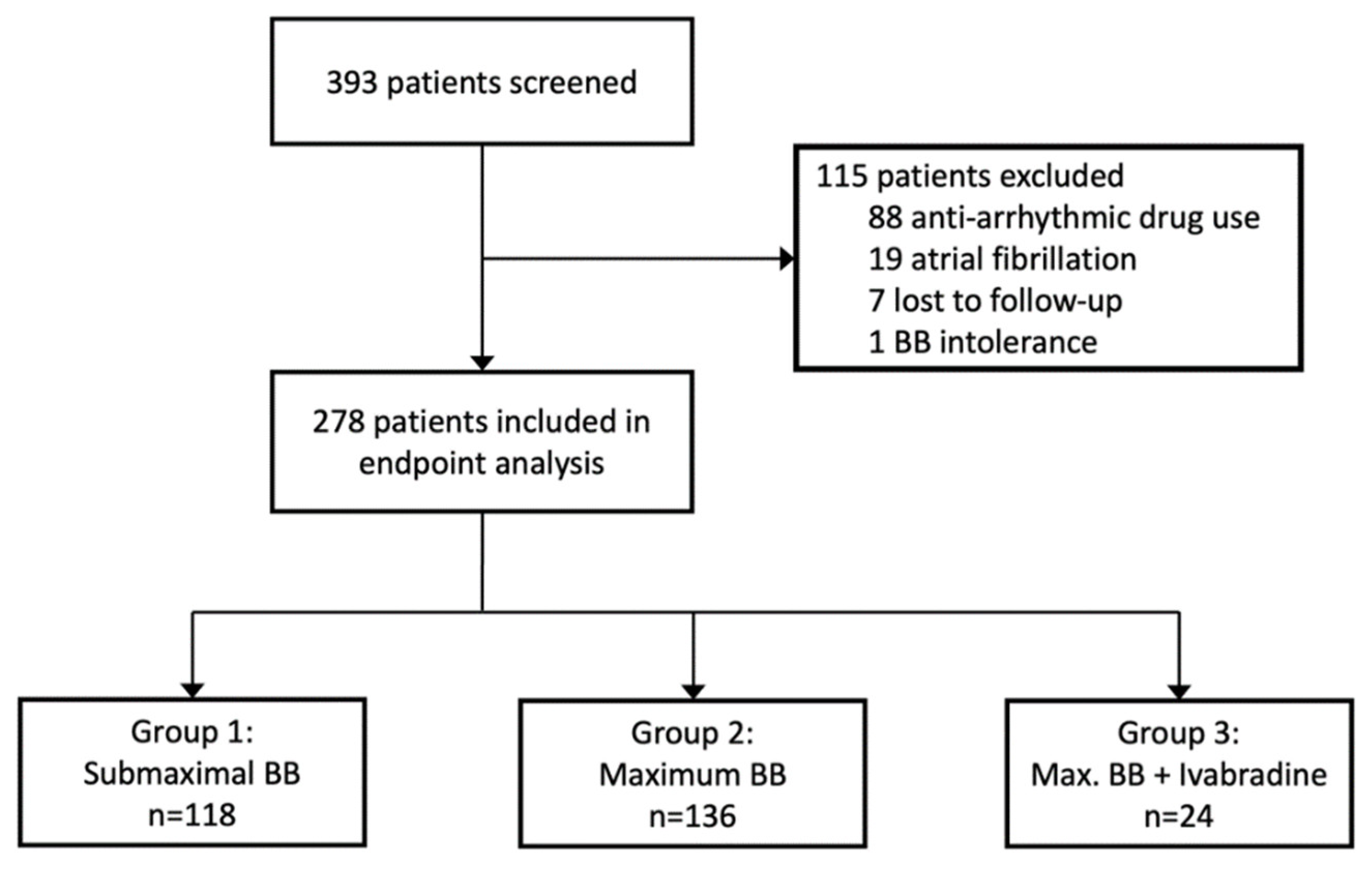
2.1. Study Population
2.2. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEI | angiotensin-converting-enzyme inhibitor |
| ARB | angiotensin receptor blocker |
| ARNI | angiotensin receptor neprilysin inhibitor |
| BB | beta blocker |
| BMI | body mass index |
| CRT | cardiac resynchronization therapy |
| EF | ejection fraction |
| EMA | European Medicines Agency |
| ESC | European Society of Cardiology |
| FDA | U.S. Food and Drug Administration |
| HF | heart failure |
| HFmrEF | heart failure with mildly reduced ejection fraction |
| HFrEF | heart failure with reduced ejection fraction |
| HR | heart rate |
| ICD | implantable cardioverter defibrillator |
| IF | funny channel |
| LVAD | left ventricular assist device |
| LVEF | left ventricular ejection fraction |
| MRA | mineralocorticoid receptor antagonist |
| NT-proBNP | N-terminal pro-brain natriuretic peptide |
| NYHA | New York Heart Association |
| SGLT2 | sodium glucose linked transporter 2 |
| SR | sinus rhythm |
References
- Böhm, M.; Bewarder, Y.; Kindermann, I.; Slawik, J.; Wintrich, J.; Werner, C. Optimization of Heart Failure Treatment by Heart Rate Reduction. Int. J. Heart Fail. 2019, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Hasenfuss, G. Benefit of heart rate reduction in heart failure. Curr. Heart Fail. Rep. 2010, 7, 156–158. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Togni, M.; Schaub, M.C.; Wenaweser, P.; Hess, O.M. High heart rate: A cardiovascular risk factor? Eur. Heart J. 2006, 27, 2387–2393. [Google Scholar] [CrossRef] [PubMed]
- Kurgansky, K.E.; Schubert, P.; Parker, R.; Djousse, L.; Riebman, J.B.; Gagnon, D.R.; Joseph, J. Association of pulse rate with outcomes in heart failure with reduced ejection fraction: A retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 92. [Google Scholar] [CrossRef]
- Domanski, M.J.; Krause-Steinrauf, H.; Massie, B.M.; Deedwania, P.; Follmann, D.; Kovar, D.; Murray, D.; Oren, R.; Rosenberg, Y.; Young, J.; et al. A comparative analysis of the results from 4 trials of beta-blocker therapy for heart failure: BEST, CIBIS-II, MERIT-HF, and COPERNICUS. J. Card. Fail. 2003, 9, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Coats, A.J.; Fowler, M.B.; Katus, H.A.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Castaigne, A.; Roecker, E.B.; et al. Effect of carvedilol on survival in severe chronic heart failure. N. Engl. J. Med. 2001, 344, 1651–1658. [Google Scholar] [CrossRef] [PubMed]
- Swedberg, K.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing [Computer Program]; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Hori, M.; Okamoto, H. Heart rate as a target of treatment of chronic heart failure. J. Cardiol. 2012, 60, 86–90. [Google Scholar] [CrossRef]
- Borer, J.S.; Böhm, M.; Ford, I.; Robertson, M.; Komajda, M.; Tavazzi, L.; Swedberg, K. Efficacy and Safety of Ivabradine in Patients with Severe Chronic Systolic Heart Failure (from the SHIFT Study). Am. J. Cardiol. 2014, 113, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, A.P.; Dahlström, U.; Filippatos, G.; Chioncel, O.; Leiro, M.C.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Fabbri, G.; et al. EURObservational Research Programme: Regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur. J. Heart Fail. 2013, 15, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Jimenez, J.F.D.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur. J. Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Nanchen, D.; Leening, M.J.G.; Locatelli, I.; Cornuz, J.; Kors, J.A.; Heeringa, J.; Deckers, J.W.; Hofman, A.; Franco, O.H.; Stricker, B.H.; et al. Resting Heart Rate and the Risk of Heart Failure in Healthy Adults. Circ. Heart Fail. 2013, 6, 403–410. [Google Scholar] [CrossRef]
- Solomon, S.D.; Anavekar, N.; Skali, H.; McMurray, J.J.; Swedberg, K.; Yusuf, S.; Granger, C.B.; Michelson, E.L.; Wang, D.; Pocock, S.; et al. Influence of Ejection Fraction on Cardiovascular Outcomes in a Broad Spectrum of Heart Failure Patients. Circulation 2005, 112, 3738–3744. [Google Scholar] [CrossRef]
- Ouwerkerk, W.; Zwinderman, A.H.; Ng, L.L.; Demissei, B.; Hillege, H.L.; Zannad, F.; van Veldhuisen, D.J.; Samani, N.J.; Ponikowski, P.; Metra, M.; et al. Biomarker-Guided Versus Guideline-Based Treatment of Patients With Heart Failure: Results From BIOSTAT-CHF. J. Am. Coll. Cardiol. 2018, 71, 386–398. [Google Scholar] [CrossRef]
- Mordi, I.R.; Ouwerkerk, W.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Metra, M.; Ng, L.L.; Samani, N.J.; van Veldhuisen, D.J.; Zannad, F.; et al. Heart failure treatment up-titration and outcome and age: An analysis of BIOSTAT-CHF. Eur. J. Heart Fail. 2021, 23, 436–444. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Packer, M. How Should We Sequence the Treatments for Heart Failure and a Reduced Ejection Fraction? Circulation 2021, 143, 875–877. [Google Scholar] [CrossRef]
- Pinilla-Vera, M.; Hahn, V.S.; Kass, D.A. Leveraging Signaling Pathways to Treat Heart Failure with Reduced Ejection Fraction. Circ. Res. 2019, 124, 1618–1632. [Google Scholar] [CrossRef]
- Stolfo, D.; Uijl, A.; Vedin, O.; Strömberg, A.; Faxén, U.L.; Rosano, G.M.C.; Sinagra, G.; Dahlström, U.; Savarese, G. Sex-Based Differences in Heart Failure Across the Ejection Fraction Spectrum: Phenotyping, and Prognostic and Therapeutic Implications. JACC Heart Fail. 2019, 7, 505–515. [Google Scholar] [CrossRef]
- Norberg, H. Clinical trial enrolment favours men. Eur. Heart J. 2019, 40, 1104–1105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| 1 | 2 | 3 | |||
|---|---|---|---|---|---|
| Total | BB in Submax. Dose | BB in Max. Dose | BB in Max. Dose + Ivabradine | p-Value | |
| N | 278 | 118 | 136 | 24 | |
| Clinical variables | |||||
| Male gender (%) | 213 (76.6) | 83 (70.3) | 112 (82.4) | 18 (75.0) | 0.077 |
| Age (years) | 57.0 (49.0, 66.1) | 60.0 (51.0, 67.1) | 56.0 (48.0, 66.0) | 53.0 (43.7, 58.2) | 0.031 |
| Height (cm) | 177 (170, 184) | 174 (168, 180) | 180 (172, 186) | 178 (171, 183) | 0.0014 |
| weight (kg) | 83.0 (72.0, 96.3) | 76.0 (67.8, 88.1) | 88.0 (74.3, 100.8) | 87.0 (77.2, 99.8) | <0.001 |
| BMI (kg/m2) | 26.0 (23.2, 29.9) | 25.4 (22.9, 28.6) | 27.0 (24.1, 31.0) | 28.7 (24.7, 33.5) | 0.0089 |
| Systolic blood pressure (mmHg) | 115 (100, 130) | 114 (100, 130) | 116 (105, 135) | 112 (95, 118) | 0.17 |
| Diastolic blood pressure (mmHg) | 69 (60, 78) | 70 (59, 77) | 67 (60, 78) | 69 (60, 80) | 0.89 |
| Type of cardiomyopathy, n (%) | |||||
| Dilated cardiomyopathy | 108 (38.99) | 35 (29.66) | 61 (45.19) | 12 (50.00) | 0.021 |
| on LVAD support | 1 (0.36) | 0 (0) | 1 (0.74) | 0 (0) | 0.59 |
| Ischemic cardiomyopathy | 108 (38.99) | 43 (36.44) | 53 (39.26) | 12 (50.00) | 0.46 |
| on LVAD support | 3 (1.08) | 3 (2.54) | 0 (0) | 0 (0) | 0.13 |
| Ischemic/dilated cardiomyopathy | 1 (0.36) | 0 (0) | 1 (0.74) | 0 (0) | 0.59 |
| Hypertrophic cardiomyopathy | 1 (0.36) | 0 (0) | 1 (0.74) | 0 (0) | 0.59 |
| Hypertrophic obstructive cardiomyopathy | 1 (0.36) | 1 (0.85) | 0 (0) | 0 (0) | 0.51 |
| Restrictive cardiomyopathy | 5 (1.81) | 3 (2.54) | 2 (1.48) | 0 (0) | 0.64 |
| Valvular cardiomyopathy | 7 (2.53) | 5 (4.24) | 2 (1.48) | 0 (0) | 0.27 |
| Toxic cardiomyopathy | 7 (2.53) | 6 (5.08) | 1 (0.74) | 0 (0) | 0.064 |
| Non-compaction cardiomyopathy | 1 (0.36) | 0 (0) | 1 (0.74) | 0 (0) | 0.59 |
| Others | 33 (11.91) | 21 (17.80) | 12 (8.89) | 0 (0) | 0.016 |
| Functional parameters | |||||
| NYHA class: I (%) | 59 (23.32) | 31 (28.70) | 21 (17.07) | 7 (31.82) | 0.070 |
| NYHA class: II (%) | 107 (42.29) | 41 (37.96) | 56 (45.53) | 10 (45.45) | 0.48 |
| NYHA class: III (%) | 58 (22.92) | 26 (24.07) | 29 (23.58) | 3 (13.64) | 0.55 |
| NYHA class: IV (%) | 1 (0.40) | 1 (0.93) | 0 (0) | 0 (0) | 0.51 |
| NYHA class: I–II (%) | 6 (2.37) | 3 (2.78) | 3 (2.44) | 0 (0) | 0.74 |
| NYHA class: II–III (%) | 20 (7.91) | 5 (4.63) | 13 (10.57) | 2 (9.09) | 0.24 |
| NYHA class: III–IV (%) | 2 (0.79) | 1 (0.93) | 1 (0.81) | 0 (0) | 0.90 |
| 6 min walk test (m) | 370.84 ± 145.25 | 340.43 ± 147.15 | 376.14 ± 149.16 | 427.67 ± 134.46 | 0.47 |
| History of comorbidities, n (%) | |||||
| Arterial hypertension | 137 (50.55) | 60 (52.17) | 65 (48.87) | 12 (52.17) | 0.86 |
| Hypercholesterolemia | 98 (42.42) | 38 (39.18) | 50 (44.25) | 10 (47.62) | 0.67 |
| Diabetes | 52 (19.05) | 17 (14.91) | 29 (21.32) | 6 (26.09) | 0.29 |
| COPD | 22 (9.48) | 13 (13.54) | 6 (5.26) | 3 (13.64) | 0.098 |
| Asthma bronchiale | 22 (9.48) | 7 (7.29) | 9 (7.89) | 6 (27.27) | 0.011 |
| Other lung disease | 25 (10.82) | 9 (9.28) | 13 (11.50) | 3 (14.29) | 0.76 |
| Chronic renal failure | 86 (37.23) | 32 (33.68) | 44 (38.60) | 10 (45.45) | 0.54 |
| Severe hepatic failure | 6 (2.60) | 1 (1.04) | 3 (2.65) | 2 (9.09) | 0.10 |
| Transient ischemic attack/ Ischemic stroke | 20 (8.66) | 4 (4.08) | 14 (12.50) | 2 (9.52) | 0.095 |
| Hemorrhagic stroke | 1 (0.44) | 0 (0) | 1 (0.91) | 0 (0) | 0.58 |
| Peripheral arterial disease | 9 (3.88) | 4 (4.12) | 5 (4.39) | 0 (0) | 0.62 |
| Hyperthyroidism | 19 (8.15) | 8 (8.16) | 11 (9.65) | 0 (0) | 0.33 |
| Hypothyroidism | 27 (11.64) | 11 (11.34) | 14 (12.28) | 2 (9.52) | 0.93 |
| Cardiac history, n (%) | |||||
| Myocardial infarction | 90 (38.79) | 36 (37.11) | 44 (38.94) | 10 (45.45) | 0.77 |
| Cardiogenic shock | 32 (15.38) | 12 (13.79) | 16 (15.69) | 4 (21.05) | 0.72 |
| Left ventricular thrombus | 26 (11.16) | 8 (8.16) | 14 (12.39) | 4 (18.18) | 0.34 |
| Atrial fibrillation | 57 (24.68) | 23 (23.71) | 32 (28.32) | 2 (9.52) | 0.18 |
| Atrial flutter | 12 (5.22) | 8 (8.25) | 4 (3.57) | 0 (0) | 0.17 |
| Ventricular tachycardia | 28 (12.44) | 6 (6.32) | 21 (19.09) | 1 (5.00) | 0.013 |
| Ventricular fibrillation | 16 (6.93) | 2 (2.04) | 10 (8.93) | 4 (19.05) | 0.011 |
| Electrocardiogram | |||||
| Heart rate (bpm) | 68.00 (60.00, 77.00) | 66.00 (59.00, 77.83) | 68.00 (60.00, 76.00) | 75.50 (67.83, 81.00) | 0.030 |
| Atrial fibrillation (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Echocardiography | |||||
| EF (Simpson) (%) | 31.00 (25.00, 40.00) | 35.00 (27.00, 42.00) | 30.00 (25.00, 36.00) | 25.00 (21.42, 31.17) | <0.001 |
| EF <40% (%) | 185 (73.71) | 66 (63.46) | 99 (80.49) | 20 (83.33) | 0.0078 |
| EF 40–50% (%) | 63 (25.10) | 35 (33.65) | 24 (19.51) | 4 (16.67) | 0.030 |
| EF >50% (%) | 3 (1.20) | 3 (2.88) | 0 (0) | 0 (0) | 0.12 |
| Diastolic dysfunction: none (%) | 45 (20.36) | 21 (22.58) | 22 (20.37) | 2 (10.00) | 0.45 |
| Diastolic dysfunction I° (%) | 98 (44.34) | 40 (43.01) | 48 (44.44) | 10 (50.00) | 0.85 |
| Diastolic dysfunction II° (%) | 48 (21.72) | 20 (21.51) | 24 (22.22) | 4 (20.00) | 0.97 |
| Diastolic dysfunction: III° (%) | 30 (13.57) | 12 (12.90) | 14 (12.96) | 4 (20.00) | 0.68 |
| E/E’ | 11.25 (8.47, 15.39) | 11.39 (8.17, 17.02) | 10.20 (7.85, 15.08) | 13.25 (11.11, 14.64) | 0.10 |
| E/A | 1.14 (0.71, 1.94) | 1.00 (0.70, 1.86) | 1.19 (0.77, 1.83) | 1.07 (0.69, 2.51) | 0.77 |
| RVP (mmHg) | 29.00 (22.00, 37.00) | 29.00 (21.20, 39.00) | 28.00 (22.00, 34.83) | 30.00 (25.00, 34.67) | 0.64 |
| TAPSE (mm) | 18.60 (15.00, 21.39) | 18.00 (14.07, 22.00) | 19.00 (16.00, 21.00) | 17.00 (13.17, 22.00) | 0.79 |
| Aortic valve stenosis moderate/severe (%) | 2 (0.72) | 1 (0.85) | 1 (0.74) | 0 (0) | 0.90 |
| Aortic valve regurgitation moderate/severe (%) | 3 (1.08) | 2 (1.69) | 1 (0.74) | 0 (0) | 0.66 |
| Mitral valve stenosis moderate/ severe (%) | 1 (0.36) | 0 (0) | 1 (0.74) | 0 (0) | 0.59 |
| Mitral valve regurgitation moderate/severe (%) | 55 (19.78) | 20 (16.95) | 29 (21.32) | 6 (25.00) | 0.55 |
| Tricuspid valve regurgitation moderate/severe (%) | 34 (12.23) | 10 (8.47) | 18 (13.24) | 6 (25.00) | 0.070 |
| Left atrial volume (mL) | 69.03 (50.88, 91.13) | 67.15 (44.33, 85.08) | 70.10 (54.12, 95.30) | 78.42 (46.94, 97.97) | 0.22 |
| Right atrial area (cm2) | 16.55 (12.94, 20.50) | 16.00 (12.38, 19.82) | 16.80 (13.31, 20.64) | 16.22 (13.55, 20.63) | 0.29 |
| IVSD (mm) | 10.00 (8.00, 11.57) | 10.00 (8.63, 12.00) | 10.00 (8.00, 11.27) | 9.90 (7.92, 11.00) | 0.57 |
| LVEDD (mm) | 62.00 (56.00, 68.53) | 58.35 (53.18, 64.91) | 64.00 (59.00, 73.00) | 66.00 (60.75, 70.08) | <0.001 |
| Laboratory data | |||||
| Hemoglobin (g/dL) | 13.70 (12.40, 14.60) | 13.30 (12.00, 14.28) | 13.90 (12.50, 14.70) | 14.60 (13.13, 15.00) | 0.0049 |
| Ferritin (ug/L) | 114.00 (64.00, 189.83) | 104.00 (64.00, 175.00) | 133.00 (59.83, 237.33) | 91.00 (63.00, 170.08) | 0.31 |
| Transferrin (g/L) | 2.60 (2.40, 3.00) | 2.60 (2.40, 3.00) | 2.60 (2.40, 2.90) | 2.85 (2.60, 3.20) | 0.034 |
| Transferrin saturation (%) | 24.50 (18.92, 30.00) | 24.00 (18.42, 29.00) | 26.00 (18.42, 31.00) | 22.50 (19.83, 28.00) | 0.10 |
| Creatinine (mg/dL) | 1.20 (0.97, 1.40) | 1.11 (0.95, 1.40) | 1.20 (1.07, 1.50) | 1.10 (0.97, 1.37) | 0.12 |
| eGFR (mL/min/1.73 m2) | 69.48 (51.60, 90.28) | 70.19 (51.50, 90.21) | 69.47 (49.46, 89.47) | 69.48 (60.51, 91.97) | 0.79 |
| Creatin kinase (U/L) | 105.00 (70.17, 147.00) | 92.00 (67.00, 137.33) | 113.00 (73.00, 157.67) | 106.00 (86.33, 156.00) | 0.20 |
| NT-proBNP (ng/L) | 1073.00 (407.33, 2704.33) | 926.00 (334.83, 2417.25) | 1109.50 (463.42, 2727.58) | 2089.00 (685.83, 3401.33) | 0.13 |
| 1 | 2 | 3 | |||
|---|---|---|---|---|---|
| Total | BB in Submax. Dose | BB in Max. Dose | BB in Max. Dose + Ivabradin | p-Value | |
| N | 278 | 118 | 136 | 24 | |
| HF medication, n (%) | |||||
| Beta Blocker (%) | 278 (100) | 118 (100) | 136 (100) | 24 (100) | |
| MRA (%) | 184 (81.78) | 70 (75.27) | 93 (84.55) | 21 (95.45) | 0.051 |
| RAAS (%) | 219 (96.90) | 88 (94.62) | 109 (98.20) | 22 (100) | 0.23 |
| ACE-I (%) | 124 (54.87) | 56 (59.57) | 62 (56.36) | 6 (27.27) | 0.021 |
| ARB (%) | 50 (22.03) | 18 (19.15) | 25 (22.52) | 7 (31.82) | 0.43 |
| ARNI (%) | 50 (22.22) | 17 (18.48) | 24 (21.62) | 9 (40.91) | 0.074 |
| Prior interventions, n (%) | |||||
| Coronary stenting | 76 (33.48) | 34 (35.79) | 33 (29.73) | 9 (42.86) | 0.42 |
| Coronary artery bypass graft | 26 (11.21) | 12 (12.24) | 13 (11.50) | 1 (4.76) | 0.61 |
| Prior valve surgery * | 33 (14.22) | 15 (15.46) | 18 (15.79) | 0 (0) | 0.15 |
| MitraClip™ procedure | 8 (3.43) | 4 (4.08) | 2 (1.75) | 2 (9.52) | 0.18 |
| Transcatheter aortic valve implantation | 1 (0.43) | 0 (0) | 0 (0) | 1 (4.76) | 0.0066 |
| History of ablation | 29 (12.50) | 8 (8.16) | 21 (18.58) | 0 (0) | 0.014 |
| Type of ablation procedure | |||||
| Atrial fibrillation | 13 (9.42) | 3 (5.36) | 10 (14.08) | 0 (0) | 0.13 |
| Atrial flutter | 5 (3.62) | 3 (5.26) | 2 (2.86) | 0 (0) | 0.62 |
| Ventricular tachycardia | 6 (4.41) | 1 (1.79) | 5 (7.25) | 0 (0) | 0.25 |
| Premature ventricular contractions | 6 (4.38) | 0 (0) | 6 (8.57) | 0 (0) | 0.050 |
| Device therapy, n (%) | |||||
| Pacemaker | 23 (10.04) | 7 (7.37) | 16 (14.29) | 0 (0) | 0.066 |
| ICD | 116 (51.10) | 30 (31.91) | 66 (59.46) | 20 (90.91) | <0.001 |
| ICD for primary prevention | 86 (76.11) | 22 (73.33) | 46 (73.02) | 18 (90.00) | 0.28 |
| Cardiac resynchronization therapy | 43 (19.03) | 8 (8.51) | 26 (23.64) | 9 (40.91) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Memenga, F.; Rybczynski, M.; Magnussen, C.; Goßling, A.; Kondziella, C.; Becher, N.; Becher, P.M.; Bernadyn, J.; Berisha, F.; Bremer, W.; et al. Heart Rate Reduction and Outcomes in Heart Failure Outpatients. J. Clin. Med. 2023, 12, 6779. https://doi.org/10.3390/jcm12216779
Memenga F, Rybczynski M, Magnussen C, Goßling A, Kondziella C, Becher N, Becher PM, Bernadyn J, Berisha F, Bremer W, et al. Heart Rate Reduction and Outcomes in Heart Failure Outpatients. Journal of Clinical Medicine. 2023; 12(21):6779. https://doi.org/10.3390/jcm12216779
Chicago/Turabian StyleMemenga, Felix, Meike Rybczynski, Christina Magnussen, Alina Goßling, Christoph Kondziella, Nina Becher, Peter Moritz Becher, Julia Bernadyn, Filip Berisha, Wiebke Bremer, and et al. 2023. "Heart Rate Reduction and Outcomes in Heart Failure Outpatients" Journal of Clinical Medicine 12, no. 21: 6779. https://doi.org/10.3390/jcm12216779
APA StyleMemenga, F., Rybczynski, M., Magnussen, C., Goßling, A., Kondziella, C., Becher, N., Becher, P. M., Bernadyn, J., Berisha, F., Bremer, W., Sinning, C., Blankenberg, S., Kirchhof, P., & Knappe, D. (2023). Heart Rate Reduction and Outcomes in Heart Failure Outpatients. Journal of Clinical Medicine, 12(21), 6779. https://doi.org/10.3390/jcm12216779