
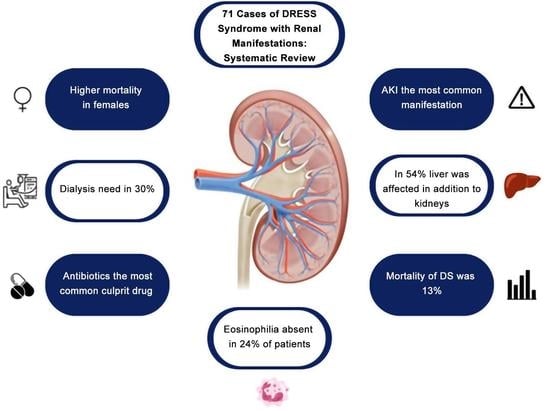
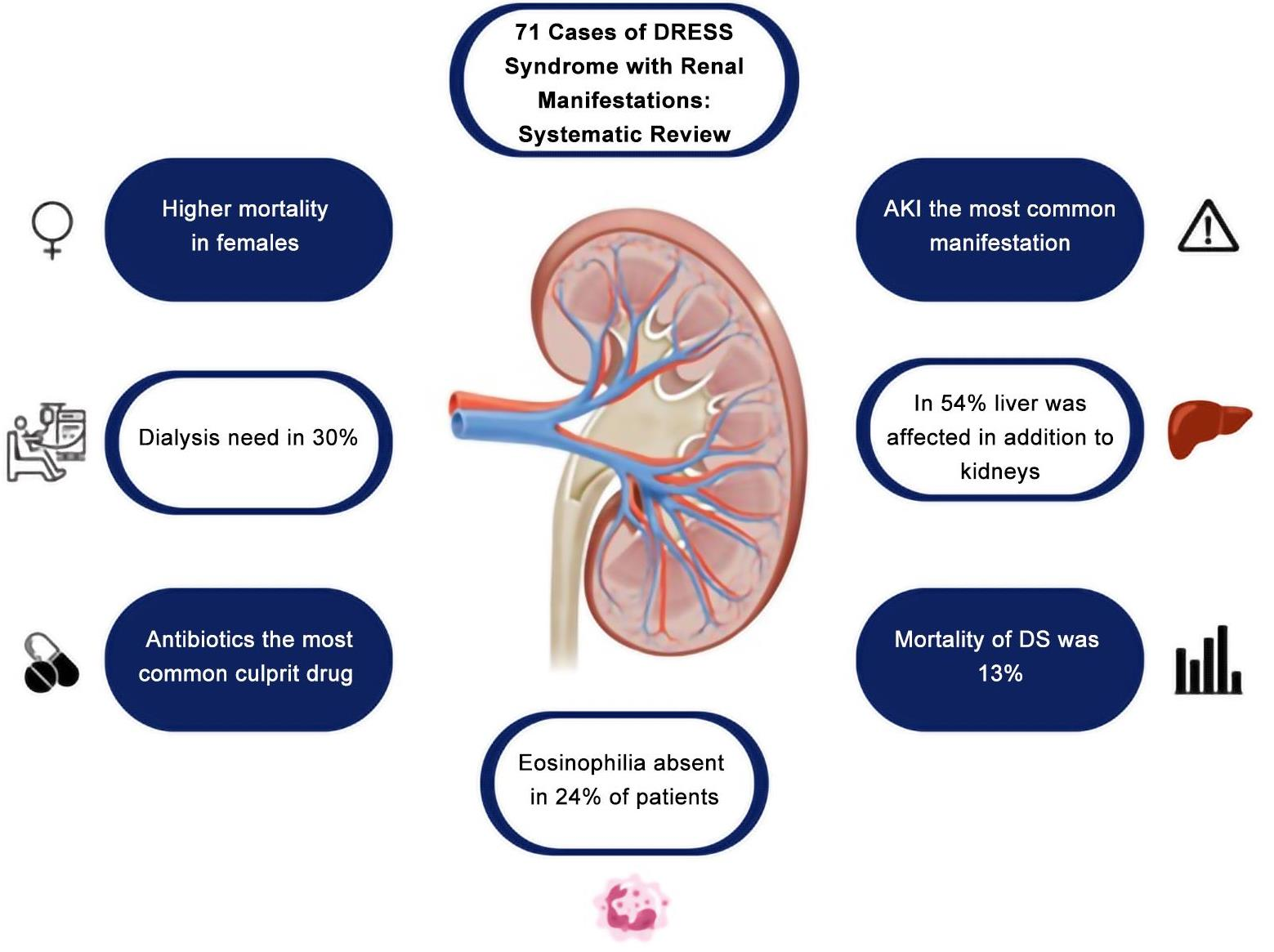
Renal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of 71 Cases
 ,
,  , ,
, ,  , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy, Definitions, and Selection Criteria
2.2. Data Collection and Statistical Analysis
3. Results
3.1. Literature Search
3.2. Demographics and Comorbidities
3.3. Visceral Organ Involvement
3.4. Causative Drugs and Latency
3.5. Eosinophilia
3.6. Viral Reactivation
3.7. Renal Manifestations
3.8. Renal Imaging
3.9. Renal Biopsy
3.10. Treatment, Sequelae, and Outcome
4. Discussion
4.1. Demographics and Comorbidities
4.2. Visceral Organ Involvement
4.3. Causative Drugs and Latency
4.4. Pathophysiology
4.5. Eosinophilia and Differential Diagnosis
- (I)
- Hypersensitivity reactions (AIN, DS);
- (II)
- Autoimmune diseases (EGPA, anti-GBM disease);
- (III)
- Other (Kimura’s disease, TINU syndrome, IgG4-RD).
4.6. Viral Reactivation
4.7. Clinical Manifestations of Renal Involvement
4.8. Renal Imaging
4.9. Renal Biopsy Findings
4.10. Treatment and Outcomes
4.11. Sequelae
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bocquet, H.; Bagot, M.; Roujeau, J.C. Drug-induced pseudolymphoma and drug hypersensitivity syndrome (Drug Rash with Eosinophilia and Systemic Symptoms: DRESS). Semin. Cutan. Med. Surg. 1996, 15, 250–257. [Google Scholar] [CrossRef]
- Kano, Y.; Ishida, T.; Hirahara, K.; Shiohara, T. Visceral involvements and long-term sequelae in drug-induced hypersensitivity syndrome. Med. Clin. N. Am. 2010, 94, 743–759. [Google Scholar] [CrossRef]
- Musette, P.; Janela, B. New Insights into Drug Reaction with Eosinophilia and Systemic Symptoms Pathophysiology. Front. Med. 2017, 4, 179. [Google Scholar] [CrossRef] [PubMed]
- Husain, Z.; Reddy, B.Y.; Schwartz, R.A. DRESS syndrome: Part I. Clinical perspectives. J. Am. Acad. Dermatol. 2013, 68, 693.e1–693.e14; quiz 706–708. [Google Scholar] [CrossRef]
- Artuković, M.; Kustelega, J.; Lugović-Mihić, L. DRESS syndrome with mild manifestations as a diagnostic and therapeutic problem: Case report. Acta Clin. Croat. 2010, 49, 479–484. [Google Scholar] [PubMed]
- Kardaun, S.H.; Sidoroff, A.; Valeyrie-Allanore, L.; Halevy, S.; Davidovici, B.B.; Mockenhaupt, M.; Hillaire-Buys, D.; Network of the French Pharmacovigilance Centers. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: Does a DRESS syndrome really exist? Br. J. Dermatol. 2007, 156, 609–611. [Google Scholar] [CrossRef]
- Behera, S.K.; Das, S.; Xavier, A.S.; Selvarajan, S. DRESS syndrome: A detailed insight. Hosp. Pr. 2018, 46, 152–162. [Google Scholar] [CrossRef]
- Taweesedt, P.T.; Nordstrom, C.W.; Stoeckel, J.; Dumic, I. Pulmonary Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review. BioMed Res. Int. 2019, 2019, 7863815. [Google Scholar] [CrossRef] [PubMed]
- Cacoub, P.; Musette, P.; Descamps, V.; Meyer, O.; Speirs, C.; Finzi, L.; Roujeau, J.C. The DRESS syndrome: A literature review. Am. J. Med. 2011, 124, 588–597. [Google Scholar] [CrossRef]
- Radovanovic, M.; Jevtic, D.; Calvin, A.D.; Petrovic, M.; Paulson, M.; Prada, L.R.; Sprecher, L.; Savic, I.; Dumic, I. “Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review. J. Clin. Med. 2022, 11, 704. [Google Scholar] [CrossRef]
- Ingelfinger, J.R. Hematuria in Adults. N. Engl. J. Med. 2021, 385, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Saha, M.K.; Massicotte-Azarniouch, D.; Reynolds, M.L.; Mottl, A.K.; Falk, R.J.; Jennette, J.C.; Derebail, V.K. Glomerular Hematuria and the Utility of Urine Microscopy: A Review. Am. J. Kidney Dis. 2022, 80, 383–392. [Google Scholar] [CrossRef]
- Haynes, J.; Haynes, R. Proteinuria. BMJ 2006, 332, 284. [Google Scholar] [CrossRef]
- Pinto, B.; Dhir, V.; Krishnan, S.; Nada, R. Leflunomide-induced DRESS syndrome with renal involvement and vasculitis. Clin. Rheumatol. 2012, 32, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Hasegawa, M.; Nabeshima, K.; Tomita, M.; Murakami, K.; Nakai, S.; Yamakita, T.; Matsunaga, K. Acute kidney injury caused by zonisam-ide-induced hypersensitivity syndrome. Intern. Med. 2010, 49, 409–413. [Google Scholar] [CrossRef]
- Ono, Y.; Shimo, T.; Shirafuji, Y.; Hamada, T.; Masui, M.; Obata, K.; Yao, M.; Kishimoto, K.; Sasaki, A. Drug-Induced Hypersensitivity Syndrome Caused by Carbamazepine Used for the Treatment of Trigeminal Neuralgia. Case Rep. Dent. 2016, 2016, 4605231. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Iwamuro, M.; Tanaka, T.; Hasegawa, K.; Hanayama, Y.; Kimura, M.; Otsuka, F. Reactivation of Human Herpes Virus-6 in the Renal Tissue of a Patient with Drug-induced Hypersensitivity Syndrome/Drug Rash with Eosinophilia and Systemic Symptoms (DIHS/DRESS). Intern. Med. 2016, 55, 1769–1774. [Google Scholar] [CrossRef] [PubMed]
- Mitani, N.; Aihara, M.; Yamakawa, Y.; Yamada, M.; Itoh, N.; Mizuki, N.; Ikezawa, Z. Drug-induced hypersensitivity syndrome due to cyanamide associated with multiple reactivation of human herpesviruses. J. Med. Virol. 2005, 75, 430–434. [Google Scholar] [CrossRef]
- Wu, F.; Jin, T.; Shang, C.; Lin, X.; Gong, X.; Wang, Z. Drug-induced hypersensitivity syndrome induced by propylthiouracil: Case report and literature review. Allergy Asthma Clin. Immunol. 2022, 18, 69. [Google Scholar] [CrossRef]
- Higashi, Y.; Baba, N.; Yoshimine, H.; Sakaguchi, I.; Kanekura, T. Late-onset interstitial nephritis in a patient with drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms. J. Dermatol. 2019, 47, 174–177. [Google Scholar] [CrossRef]
- Czapka, M.; Shukla, S.; Slosar-Cheah, M. Urine trouble: Genitourinary tuberculosis and subsequent DRESS syndrome. BMJ Case Rep. 2017, 2017, bcr2017220440. [Google Scholar] [CrossRef] [PubMed]
- Jamel, E.G.; Ahmed, S. DRESS Syndrome and Chronic Renal Failure Induced by Ethambutol. Am. J. Med. Sci. 2019, 358, e19. [Google Scholar] [CrossRef]
- Laban, E.; Hainaut-Wierzbicka, E.; Pourreau, F.; Yacoub, M.; Sztermer, E.; Guillet, G.; Touchard, G.; Bridoux, F. Cyclophosphamide therapy for corti-coresistant drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome in a patient with severe kidney and eye involvement and Epstein-Barr virus reactivation. Am. J. Kidney Dis. 2010, 55, e11–e14. [Google Scholar] [CrossRef] [PubMed]
- Torroba Sanz, B.; Mendez Martínez, E.; Cacho Asenjo, E.; Aquerreta Gonzalez, I. Permanent renal sequelae secondary to drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome induced by quetiapine. Eur. J. Hosp. Pharm. 2021, 28, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Mata, L.; Torres-Zevallos, H.; Guerreros, A.G. Life-threatening DRESS syndrome with kidney damage following severe COVID-19 in a patient with Down syndrome. BMJ Case Rep. 2021, 14, e241418. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, M.P.; Chinta, S.; Sosa, F.; Nasr, R.; Kelly, P. Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) Syndrome Due to Vancomycin. Cureus 2022, 14, e26219. [Google Scholar] [CrossRef]
- Chou, H.-Y.; Chen, C.-B.; Cheng, C.-Y.; Chen, Y.-A.; Ng, C.Y.; Kuo, K.-L.; Chen, W.-L. Febuxostat-associated drug reaction with eosinophilia and systemic symptoms (DRESS). J. Clin. Pharm. Ther. 2015, 40, 689–692. [Google Scholar] [CrossRef]
- Miller Quidley, A.; Bookstaver, P.B.; Gainey, A.B.; Gainey, M.D. Fatal clindamycin-induced drug rash with eosinophilia and systemic symptoms (DRESS) syndrome. Pharmacotherapy 2012, 32, e387–e392. [Google Scholar] [CrossRef]
- Hindosh, N.; Kotala, R.; Nguyen, K.; Pintor, A. Trimethoprim-Sulfamethoxazole-Induced Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Complicated by Acute Liver Failure. Cureus 2022, 14, e30852. [Google Scholar] [CrossRef]
- Velasco, M.J.; McDermott, J. Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome and hepatitis induced by phenytoin. Int. J. Dermatol. 2013, 53, 490–493. [Google Scholar] [CrossRef]
- Shaaban, H.; Layne, T.; Guron, G. A case of DRESS (drug reaction with eosinophilia and systemic symptoms) with acute interstitial nephritis secondary to lenalidomide. J. Oncol. Pharm. Pract. 2013, 20, 302–304. [Google Scholar] [CrossRef]
- Qadri, I.; Zeng, X.; Guo, R.; Koratala, A. Acute interstitial nephritis and DRESS syndrome without eosinophilia associated with cefepime. BMJ Case Rep. 2017, 2017, bcr2017221401. [Google Scholar] [CrossRef]
- Shaughnessy, K.K.; Bouchard, S.M.; Mohr, M.R.; Herre, J.M.; Salkey, K.S. Minocycline-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome with persistent myocarditis. J. Am. Acad. Dermatol. 2010, 62, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Ghislain, P.D.; Bodarwe, A.D.; Vanderdonckt, O.; Tennstedt, D.; Marot, L.; Lachapelle, J.M. Drug-induced eosinophilia and multi-systemic failure with positive patch-test reaction to spironolactone: DRESS syndrome. Acta Derm. Venereol. 2004, 84, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Byun, J.; Moon, C.H.; Yoon, J.H.; Yang, K.Y.; Park, S.C.; Han, C.J. Allopurinol-induced DRESS syndrome mimicking biliary obstruction. Clin. Mol. Hepatol. 2014, 20, 71–75. [Google Scholar] [CrossRef]
- Aatif, T.; Fatihi, J.; El Annaz, H.; Qamouss, O. Allopurinol-Induced Drug Reactions with Eosinophilia and Systemic Symptoms Syndrome with Interstitial Nephritis. Indian J. Nephrol. 2018, 28, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.K.; Lee, S.W.; Nam, H.S.; Jeon, D.S.; Park, N.R.; Nam, Y.H.; Lee, S.K.; Baek, Y.H.; Han, S.Y. A Case of Sorafenib-induced DRESS Syndrome in Hepatocelluar Carcinoma. Korean J. Gastroenterol. 2016, 67, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Vaida, I.; Roszkiewicz, F.; Gruson, B.; Makdassi, R.; Damaj, G. Drug rash with eosinophilia and systemic symptoms after chlo-rambucil treatment in chronic lymphocytic leukaemia. Pharmacology 2009, 83, 148–149. [Google Scholar] [CrossRef]
- Singh, S.; Khurana, A.; Muddebihal, A.; Jangra, M. Trimetazidine, a hitherto unreported cause of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) syndrome. Contact Dermat. 2020, 84, 208–210. [Google Scholar] [CrossRef]
- Abdelnabi, M.; Elmssary, M.; Sekhon, J.; Benjanuwattra, J. Acute onset of fever, eosinophilia, rash, acute kidney injury, and a positive Monospot test in a patient on lamotrigine: DRESS syndrome. Lancet 2022, 399, 1902. [Google Scholar] [CrossRef]
- Liu, Q.; Hou, W.; Shen, Y.; Zhao, S. Allopurinol-induced acute kidney injury and DRESS syndrome without eosinophilia: A case report. Clin. Nephrol. 2021, 96, 188–190. [Google Scholar] [CrossRef]
- Higuchi, M.; Agatsuma, T.; Iizima, M.; Yamazaki, Y.; Saita, T.; Ichikawa, T.; Kamijo, Y.; Arakura, H.; Hora, K.; Kiyosawa, K. A case of drug-induced hypersensitivity syndrome with multiple organ involvement treated with plasma exchange. Ther. Apher. Dial. 2005, 9, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Savard, S.; Desmeules, S.; Riopel, J.; Agharazii, M. Linezolid-associated acute interstitial nephritis and drug rash with eosinophilia and systemic symptoms (DRESS) syndrome. Am. J. Kidney Dis. 2009, 54, e17–e20. [Google Scholar] [CrossRef]
- Leão, R.N.; Barreto, P.; Ribeiro, J.V. Nitrofurantoin: Cause of DRESS syndrome. BMJ Case Rep. 2013, 2013, bcr2013008991. [Google Scholar] [CrossRef] [PubMed]
- Paydas, S.; Balal, M.; Kocabas, F.; Ay, N. Acute renal failure secondary to drug-related crystalluria and/or drug reaction with eosinophilia and systemic symptom syndrome in a patient with metastatic lung cancer. Saudi J. Kidney Dis. Transplant. 2017, 28, 934–936. [Google Scholar]
- Iyer, D.; Buggy, Y.; O’Reilly, K.; Searle, M. Strontium ranelate as a cause of acute renal failure and dress syndrome. Nephrology 2009, 14, 624. [Google Scholar] [CrossRef]
- Schnetzke, U.; Bossert, T.; Scholl, S.; Freesmeyer, M.; Hochhaus, A.; La Rosée, P. Drug-induced lymphadenopathy with eosinophilia and renal failure mimicking lymphoma disease: Dramatic onset of DRESS syndrome associated with antibiotic treatment. Ann. Hematol. 2011, 90, 1353–1355. [Google Scholar] [CrossRef]
- An, J.; Lee, J.H.; Lee, H.; Yu, E.; Lee, D.B.; Shim, J.H.; Yoon, S.; Lee, Y.; Park, S.; Lee, H.C. Drug rash with eosinophilia and systemic symptoms syndrome following cholestatic hepatitis A: A case report. Clin. Mol. Hepatol. 2012, 18, 84–88. [Google Scholar] [CrossRef]
- Ibrahim, M.; Nunley, D.L. Two Catastrophes in One Patient: Drug Reaction with Eosinophilia and Systemic Symptoms and Toxic Shock Syndrome. Cureus 2017, 9, e1359. [Google Scholar] [CrossRef]
- Bobot, M.; Coen, M.; Simon, C.; Daniel, L.; Habib, G.; Serratrice, J. DRESS syndrome with thrombotic microangiopathy revealing a Noonan syndrome: Case report. Medicine 2018, 97, e0297. [Google Scholar] [CrossRef]
- Velema, M.; Voerman, H.J. DRESS syndrome caused by nitrofurantoin. Neth. J. Med. 2009, 67, 147–149. [Google Scholar]
- de Campos, F.P.F.; de Lima, P.P.; Maragno, L.; Watanabe, F.T. Hepatic necrosis associated with drug-induced hypersensitivity syndrome. Autops. Case Rep. 2012, 2, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.; Paviour, S.; Gregory, S.; Chew, R. When fever is more than infection: Two cases of vancomycin-induced drug reaction with eosinophilia and systemic symptoms (DRESS). BMJ Case Rep. 2021, 14, e238006. [Google Scholar] [CrossRef]
- Ben Salha, W.; Moussaoui, E.; Oualha, L.; Anoun, J.; Douki, N. Erosive cheilitis as an early manifestation in DRESS syndrome. Clin. Case Rep. 2021, 9, e05123. [Google Scholar] [CrossRef] [PubMed]
- Suga, T.; Sato, K.; Yamazaki, Y.; Ohyama, T.; Horiguchi, N.; Kakizaki, S.; Kusano, M.; Yamada, M. Probable case of drug reaction with eosinophilia and systemic symptom syndrome due to combination therapy with daclatasvir and asunaprevir. World J. Clin. Cases 2015, 3, 1005–1010. [Google Scholar] [CrossRef]
- Eguchi, E.; Shimazu, K.; Nishiguchi, K.; Yorifuji, S.; Tanaka, A.; Kuwahara, T. Granulomatous interstitial nephritis associated with atypical drug-induced hypersensitivity syndrome induced by carbamazepine. Clin. Exp. Nephrol. 2011, 16, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Sin, C.; Mahé, E.; Sigal, M.-L. Drug reaction with eosinophilia and systemic symptoms (DRESS) in a patient taking sitagliptin. Diabetes Metab. 2012, 38, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Hakim, C.; Melitas, C.; Nguyen, E.; Ngo, K. Atypical Manifestation of DRESS Syndrome. Case Rep. Gastrointest. Med. 2020, 2020, 6863582. [Google Scholar] [CrossRef]
- Ichiche, M.; Kiesch, N.; De Bels, D. DRESS syndrome associated with HHV-6 reactivation. Eur. J. Intern. Med. 2003, 14, 498–500. [Google Scholar] [CrossRef]
- Mukit, W.; Cooper, R.; Moudgil, H.; Ahmad, N. DRESS syndrome: An important differential for eosinophilia with systemic organ dysfunction. BMJ Case Rep. 2020, 13, e234251. [Google Scholar] [CrossRef]
- Pawar, P.; Gupta, V.A.; Karnik, N.D.; Vaidya, M.; Khopkar, U. Allopurinol Induced DRESS Syndrome. J. Assoc. Physicians India 2014, 62, 63–65. [Google Scholar] [PubMed]
- Zuliani, E.; Zwahlen, H.; Gilliet, F.; Marone, C. Vancomycin-induced hypersensitivity reaction with acute renal failure: Resolution following cyclosporine treatment. Clin. Nephrol. 2005, 64, 155–158. [Google Scholar] [CrossRef]
- Myers, C.M.; Miller, J.J.; Davis, W.D. Allopurinol-Induced Drug Reaction with Eosinophilia and Systemic Symptoms: A Case Report. Adv. Emerg. Nurs. J. 2020, 42, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Augusto, J.-F.; Sayegh, J.; Simon, A.; Croue, A.; Chennebault, J.-M.; Cousin, M.; Subra, J.-F. A case of sulphasalazine-induced DRESS syndrome with delayed acute interstitial nephritis. Nephrol. Dial. Transplant. 2009, 24, 2940–2942. [Google Scholar] [CrossRef]
- Gangireddy, M.; Sarao, M.S.; Shrimanker, I.; Nookala, V.K. A Fatal Case of Vancomycin Associated Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome in a Septuagenarian. Cureus 2019, 11, e5015. [Google Scholar] [CrossRef]
- Jafry, A.; Nimri, J.; Akhtar, K.; Qureshi, S.; Bray-Hall, S. Amoxicillin-clavulanate induced DRESS syndrome masquerading as red man syndrome. J. Fam. Med. Prim. Care 2022, 11, 3992. [Google Scholar] [CrossRef] [PubMed]
- Adike, A.; Boppana, V.; Lam-Himlin, D.; Stanton, M.; Nelson, S.; Ruff, K.C. A Mysterious DRESS Case: Autoimmune Enteropathy Associated with DRESS Syndrome. Case Rep. Gastrointest. Med. 2017, 2017, 7861857. [Google Scholar] [CrossRef]
- Chan, L.; Chan, C.; Cook, D.K. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: Case report of severe multiorgan involvement to perindopril/amlodipine combination antihypertensive. JAAD Case Rep. 2018, 4, 170–174. [Google Scholar] [CrossRef]
- He, Q.; Ying, G.; Fei, X.; Zha, C.; Chen, Z.; Bao, Y.; Long, J.; Wang, Z.; He, X.; Xia, M. Drug rash with eosinophilia and systemic symptoms and severe renal injury induced by proton pump inhibitor therapy: A case report. Medicine 2020, 99, e22509. [Google Scholar] [CrossRef]
- Ros, J.; Muñoz-Couselo, E. DRESS syndrome due to vemurafenib treatment: Switching BRAF inhibitor to solve a big problem. BMJ Case Rep. 2018, 2018, bcr2018224379. [Google Scholar] [CrossRef]
- Morikawa, D.; Hiraoka, E.; Obunai, K.; Norisue, Y. Myocarditis Associated with Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Case Report and Review of the Literature. Am. J. Case Rep. 2018, 19, 978–984. [Google Scholar] [CrossRef]
- Maximova, N.; Maestro, A.; Zanon, D.; Marcuzzi, A. Rapid recovery of postnivolumab vemurafenib-induced Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) syndrome after tocilizumab and infliximab administration. J. Immunother. Cancer 2019, 8, e000388. [Google Scholar] [CrossRef]
- Portney, D.A.; Baker, H.P.; Boyle, M.M.; Barbosa, V.H.; Luu, H.H. Drug Reaction with Eosinophilia and Systemic Syndrome in Revision Arthroplasty for a Prosthetic Knee Infection: A Case Report. JBJS Case Connect. 2021, 11, e20.00805. [Google Scholar] [CrossRef]
- Ben Fadhel, N.; Ben Romdhane, H.; Chaabane, A.; Ali, H.B.; Boughattas, N.; Aouam, K.; Ben Fredj, N. DRESS syndrome following furosemide administration: An unusual association. Nephrol. Ther. 2020, 16, 437–438. [Google Scholar] [CrossRef]
- Gupta, T. Valproate-induced Drug Rash Eosinophilia with Systemic Symptoms Syndrome: An Unknown Hepatotoxicity. Euroasian J. Hepato-Gastroenterol. 2017, 9, 102–103. [Google Scholar] [CrossRef]
- Mustafa, S.F.; Zafar, M.R.; Miller, T.W. Rosuvastatin Use Implicated in the Drug Reaction with Eosinophilia and Systemic Symptoms. Cureus 2020, 12, e7098. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Sung, K.; Yang, H.K.; Kim, S.H.; Kim, H.Y.; Ban, G.H.; Park, S.E.; Lee, H.D.; Kim, S.Y. Acute tubular necrosis as a part of vancomycin induced drug rash with eosinophilia and systemic symptoms syndrome with coincident postinfectious glomerulonephritis. Korean J. Pediatr. 2016, 59, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Erdem, S.B.; Nacaroglu, H.T.; Bag, O.; Karkiner, C.S.U.; Korkmaz, H.A.; Can, D. DRESS syndrome associated with type 2 diabetes in a child. Cent. Eur. J. Immunol. 2015, 40, 493–496. [Google Scholar] [CrossRef]
- Tomani, M.; Caridi, C.; Tatarina-Nulman, O.; Charlot, C.; Narula, P. Complicated Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome History in a 14-Year-Old. Am. J. Case Rep. 2021, 22, e927951-1–e927951-7. [Google Scholar] [CrossRef] [PubMed]
- Nawaz, F.; Wall, B.M. Drug rash with eosinophilia and systemic symptoms (DRESS) syndrome: Suspected association with titanium bioprosthesis. Am. J. Med. Sci. 2007, 334, 215–218. [Google Scholar] [CrossRef]
- Piñana, E.; Lei, S.H.; Merino, R.; Melgosa, M.; De La Vega, R.; Gonzales-Obeso, E.; Ramírez, E.; Borobia, A.; Carcas, A. DRESS-syndrome on sulfasalazine and naproxen treatment for juvenile idiopathic arthritis and reactivation of human herpevirus 6 in an 11-year-old caucasian boy. J. Clin. Pharm. Ther. 2010, 35, 365–370. [Google Scholar] [CrossRef]
- Esposito, A.J.; Murphy, R.C.; Toukatly, M.N.; Amro, O.W.; Kestenbaum, B.R.; Najafian, B. Acute kidney injury in allopurinol-induced DRESS syndrome: A case report of concurrent tubulointerstitial nephritis and kidney-limited necrotizing vasculitis. Clin. Nephrol. 2017, 87, 316–319. [Google Scholar] [CrossRef]
- Sasidharanpillai, S.; Riyaz, N.; Rajan, U.; Binitha, M.; Khader, A.; Mariyath, O.R.; John, R.; Puravoor, J. Drug reaction with eosinophilia and systemic symptoms: Observations from a tertiary care institution. Indian J. Dermatol. Venereol. Leprol. 2014, 80, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.J.; Sameem, F.; Ashraf, M. Drug reaction with eosinophilia and systemic symptoms: Manifestations, treatment, and outcome in 17 patients. Int. J. Dermatol. 2014, 54, 537–542. [Google Scholar] [CrossRef]
- Hiransuthikul, A.; Rattananupong, T.; Klaewsongkram, J.; Rerknimitr, P.; Pongprutthipan, M.; Ruxrungtham, K. Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms (DIHS/DRESS): 11 years retrospective study in Thailand. Allergol. Int. 2016, 65, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Toniato, A.; Gamba, C.; Schroeder, J.W.; Fabbri, V.; Ortiz, S.V.B.; Borgonovo, L.; Piantanida, M.; Scibilia, J.; Balossi, L.; Brusamolino, E.; et al. Role of Multiple Comorbidities and Therapies in Conditioning the Clinical Severity of DRESS: A Mono-Center Retrospective Study of 25 Cases. Int. J. Mol. Sci. 2021, 22, 7072. [Google Scholar] [CrossRef]
- Um, S.J.; Lee, S.K.; Kim, Y.H.; Kim, K.H.; Son, C.H.; Roh, M.S.; Lee, M.K. Clinical features of drug-induced hypersensitivity syndrome in 38 patients. J. Investig. Allergol. Clin. Immunol. 2010, 20, 556–562. [Google Scholar] [PubMed]
- Ben M’rad, M.; Leclerc-Mercier, S.; Blanche, P.; Franck, N.; Rozenberg, F.; Fulla, Y.; Guesmi, M.; Rollot, F.; Dehoux, M.; Guillevin, L.; et al. Drug-induced hypersensitivity syndrome: Clinical and biologic disease patterns in 24 patients. Medicine 2009, 88, 131–140. [Google Scholar] [CrossRef]
- Metterle, L.; Hatch, L.; Seminario-Vidal, L. Pediatric drug reaction with eosinophilia and systemic symptoms: A systematic review of the literature. Pediatr. Dermatol. 2019, 37, 124–129. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chiu, H.C.; Chu, C.Y. Drug reaction with eosinophilia and systemic symptoms: A retrospective study of 60 cases. Arch. Dermatol. 2010, 146, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Eshki, M.; Allanore, L.; Musette, P.; Milpied, B.; Grange, A.; Guillaume, J.C.; Chosidow, O.; Guillot, I.; Paradis, V.; Joly, P.; et al. Twelve-year analysis of severe cases of drug reaction with eosinophilia and systemic symptoms: A cause of unpredictable multiorgan failure. Arch. Dermatol. 2009, 145, 67–72. [Google Scholar] [CrossRef]
- Walsh, S.; Diaz-Cano, S.; Higgins, E.; Morris-Jones, R.; Bashir, S.; Bernal, W.; Creamer, D. Drug reaction with eosinophilia and systemic symptoms: Is cutaneous phenotype a prognostic marker for outcome? A review of clinicopathological features of 27 cases. Br. J. Dermatol. 2013, 168, 391–401. [Google Scholar] [CrossRef]
- Ushigome, Y.; Kano, Y.; Ishida, T.; Hirahara, K.; Shiohara, T. Short- and long-term outcomes of 34 patients with drug-induced hypersensitivity syndrome in a single institution. J. Am. Acad. Dermatol. 2012, 68, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, S.-Y.; Hahm, J.E.; Ha, J.W.; Kim, C.W.; Kim, S.S. Clinical features of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A study of 25 patients in Korea. Int. J. Dermatol. 2017, 56, 944–951. [Google Scholar] [CrossRef]
- Mehrholz, D.; Urban, A.; Herstowska, M.; Nowicki, R.; Cubała, W.; Barańska-Rybak, W. A retrospective study of DRESS—Drug reaction with eosinophilia and systemic symptoms. Psychiatr. Polska 2017, 51, 1079–1093. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.Y.; Anderson, K.R.; Davis, D.M.; Hand, J.L.; Tollefson, M.M. Drug reaction with eosinophilia and systemic symptoms (DRESS) in the pediatric population: A systematic review of the literature. J. Am. Acad. Dermatol. 2020, 83, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, S.; Neema, S.; Vashisht, D.; Venugopal, R.; Sengupta, P.; Radhakrishnan, S. Drug reaction with eosinophilia and systemic symptoms: A single center descriptive observational study. Dermatol. Ther. 2020, 34, e14670. [Google Scholar] [CrossRef]
- Bedouelle, E.; Ben Said, B.; Tetart, F.; Milpied, B.; Welfringer-Morin, A.; Maruani, A.; Catteau, B.; Dezoteux, F.; Staumont-Sallé, D.; Mazereeuw-Hautier, J.; et al. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): Series of 49 French Pediatric Cases. J. Allergy Clin. Immunol. Pr. 2021, 10, 267–274.e5. [Google Scholar] [CrossRef]
- Martínez-Cabriales, S.A.; Rodríguez-Bolaños, F.; Shear, N.H. Drug Reaction with Eosinophilia and Systemic Symptoms (DReSS): How Far Have We Come? Am. J. Clin. Dermatol. 2019, 20, 217–236. [Google Scholar] [CrossRef]
- Lee, T.; Lee, Y.S.; Yoon, S.-Y.; Kim, S.; Bae, Y.-J.; Kwon, H.-S.; Cho, Y.S.; Moon, H.-B.; Kim, T.-B. Characteristics of liver injury in drug-induced systemic hypersensitivity reactions. J. Am. Acad. Dermatol. 2013, 69, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Delgado, M.G.; Casu, S.; Montani, M.; Brunner, F.; Semmo, N.; Berzigotti, A.B.; Dufour, J.F. Hepatic manifestations of drug reaction with eosinophilia and systemic symptoms syndrome. Explor. Med. 2021, 2, 122–134. [Google Scholar] [CrossRef]
- Jevtic, D.; Dumic, I.; Nordin, T.; Singh, A.; Sulovic, N.; Radovanovic, M.; Jecmenica, M.; Milovanovic, T. Less Known Gastrointestinal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of the Literature. J. Clin. Med. 2021, 10, 4287. [Google Scholar] [CrossRef]
- Lin, I.-C.; Yang, H.-C.; Strong, C.; Yang, C.-W.; Cho, Y.-T.; Chen, K.-L.; Chu, C.-Y. Liver injury in patients with DRESS: A clinical study of 72 cases. J. Am. Acad. Dermatol. 2015, 72, 984–991. [Google Scholar] [CrossRef]
- Soria, A.; Bernier, C.; Veyrac, G.; Barbaud, A.; Puymirat, E.; Milpied, B. Drug reaction with eosinophilia and systemic symptoms may occur within 2 weeks of drug exposure: A retrospective study. J. Am. Acad. Dermatol. 2019, 82, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.W.; Preclaro, I.A.C.; Lin, W.H.; Chung, W.H. An Updated Review of Genetic Associations with Severe Adverse Drug Re-actions: Translation and Implementation of Pharmacogenomic Testing in Clinical Practice. Front. Pharmacol. 2022, 13, 886377. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.-T.; Yang, C.-W.; Chu, C.-Y. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): An Interplay among Drugs, Viruses, and Immune System. Int. J. Mol. Sci. 2017, 18, 1243. [Google Scholar] [CrossRef]
- Stirton, H.; Shear, N.H.; Dodiuk-Gad, R.P. Drug Reaction with Eosinophilia and Systemic Symptoms (DReSS)/Drug-Induced Hypersensitivity Syndrome (DiHS)-Readdressing the DReSS. Biomedicines 2022, 10, 999. [Google Scholar] [CrossRef]
- Ramirez, G.A.; Ripa, M.; Burastero, S.; Benanti, G.; Bagnasco, D.; Nannipieri, S.; Monardo, R.; Ponta, G.; Asperti, C.; Cilona, M.B.; et al. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): Focus on the Pathophysiological and Diagnostic Role of Viruses. Microorganisms 2023, 11, 346. [Google Scholar] [CrossRef] [PubMed]
- Pichler, W.J.; Brüggen, M. Viral infections and drug hypersensitivity. Allergy 2022, 78, 60–70. [Google Scholar] [CrossRef]
- Gibson, A.; Deshpande, P.; Campbell, C.N.; Krantz, M.S.; Mukherjee, E.; Mockenhaupt, M.; Pirmohamed, M.; Palubinsky, A.M.; Phillips, E.J. Updates on the immunopathology and genomics of severe cutaneous adverse drug reactions. J. Allergy Clin. Immunol. 2023, 151, 289–300.e4. [Google Scholar] [CrossRef]
- Del Pozzo-Magaña, B.R.; Liy-Wong, C. Drugs and the skin: A concise review of cutaneous adverse drug reactions. Br. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Gotlib, J. World Health Organization-defined eosinophilic disorders: 2017 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2017, 92, 1243–1259. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Klion, A.D.; Horny, H.-P.; Roufosse, F.; Gotlib, J.; Weller, P.F.; Hellmann, A.; Metzgeroth, G.; Leiferman, K.M.; Arock, M.; et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J. Allergy Clin. Immunol. 2012, 130, 607–612.e9. [Google Scholar] [CrossRef]
- Sanchez-Alamo, B.; Cases-Corona, C.; Fernandez-Juarez, G. Facing the Challenge of Drug-Induced Acute Interstitial Nephritis. Nephron 2022, 147, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Doreille, A.; Buob, D.; Bay, P.; Julien, M.; Riviere, F.; Rafat, C. Renal Involvement in Eosinophilic Granulomatosis with Polyangiitis. Kidney Int. Rep. 2021, 6, 2718–2721. [Google Scholar] [CrossRef]
- Furuta, S.; Iwamoto, T.; Nakajima, H. Update on eosinophilic granulomatosis with polyangiitis. Allergol. Int. 2019, 68, 430–436. [Google Scholar] [CrossRef]
- Esson, G.A.; Hussain, A.B.; Meggitt, S.J.; Reynolds, N.J.; Sayer, J.A. Cutaneous manifestations of acute kidney injury. Clin. Kidney J. 2021, 15, 855–864. [Google Scholar] [CrossRef]
- Yang, B.; Liao, H.; Wang, M.; Long, Q.; Zhong, H.; Luo, L.; Liu, Z.; Cheng, X. Kimura’s disease successively affecting multiple body parts: A case-based literature review. BMC Ophthalmol. 2022, 22, 154. [Google Scholar]
- Okafor, L.O.; Hewins, P.; Murray, P.I.; Denniston, A.K. Tubulointerstitial nephritis and uveitis (TINU) syndrome: A systematic review of its epidemiology, demographics and risk factors. Orphanet J. Rare Dis. 2017, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Ming, B.; Zhong, J.; Dong, L. Role of eosinophilia in IgG4-related disease. Ann. Rheum. Dis. 2021, 40, 1038–1044. [Google Scholar] [CrossRef]
- Shenoy, A.; Mohandas, N.; Gottlieb, A. Cutaneous and systemic IgG4-related disease: A review for dermatologists. Dermatol. Online J. 2019, 25, 13030. [Google Scholar] [CrossRef]
- Gauckler, P.; Shin, J.I.; Mayer, G.; Kronbichler, A. Eosinophilia and Kidney Disease: More than Just an Incidental Finding? J. Clin. Med. 2018, 7, 529. [Google Scholar] [CrossRef]
- Miyagawa, F.; Asada, H. Current Perspective Regarding the Immunopathogenesis of Drug-Induced Hypersensitivity Syn-drome/Drug Reaction with Eosinophilia and Systemic Symptoms (DIHS/DRESS). Int. J. Mol. Sci. 2021, 22, 2147. [Google Scholar] [CrossRef]
- Shiohara, T.; Iijima, M.; Ikezawa, Z.; Hashimoto, K. The diagnosis of a DRESS syndrome has been sufficiently established on the basis of typical clinical features and viral reactivations. Br. J. Dermatol. 2007, 156, 1083–1084. [Google Scholar] [CrossRef] [PubMed]
- Kano, Y.; Tohyama, M.; Aihara, M.; Matsukura, S.; Watanabe, H.; Sueki, H.; Iijima, M.; Morita, E.; Niihara, H.; Asada, H.; et al. Sequelae in 145 patients with drug-induced hy-persensitivity syndrome/drug reaction with eosinophilia and systemic symptoms: Survey conducted by the Asian Research Committee on Severe Cutaneous Adverse Reactions (ASCAR). J. Dermatol. 2015, 42, 276–282. [Google Scholar] [CrossRef]
- Asano, Y.; Kagawa, H.; Kano, Y.; Shiohara, T. Cytomegalovirus disease during severe drug eruptions: Report of 2 cases and retrospective study of 18 patients with drug-induced hypersensitivity syndrome. Arch. Dermatol. 2009, 145, 1030–1036. [Google Scholar] [CrossRef] [PubMed]
- Descamps, V. Drug reaction with eosinophilia and systemic symptoms and thyroiditis: Human herpesvirus-6, the possible common link. Br. J. Dermatol. 2013, 169, 952. [Google Scholar] [CrossRef]
- Hama, N.; Abe, R.; Gibson, A.; Phillips, E.J. Drug-Induced Hypersensitivity Syndrome (DIHS)/Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): Clinical Features and Pathogenesis. J. Allergy Clin. Immunol. Pract. 2022, 10, 1155–1167.e5. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.N.; Shwe, S.; Ravi, V.; Miller, M.; Mesinkovska, N.A.; Rojek, N.W.; Worswick, S. Characterizing DRESS syndrome recurrence: A systematic review. Arch. Dermatol. Res. 2021, 314, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, R.; Shawar, S. Mechanisms of Drug-Induced Interstitial Nephritis. Adv. Chronic Kidney Dis. 2017, 24, 64–71. [Google Scholar] [CrossRef]
- Perazella, M.A.; Markowitz, G.S. Drug-induced acute interstitial nephritis. Nat. Rev. Nephrol. 2010, 6, 461–470. [Google Scholar] [CrossRef]
- Moledina, D.G.; Perazella, M.A. Drug-Induced Acute Interstitial Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 2046–2049. [Google Scholar] [CrossRef]
- Praga, M.; González, E. Acute interstitial nephritis. Kidney Int. 2010, 77, 956–961. [Google Scholar] [CrossRef]
- Huang, L.; Liang, S.; Dong, J.; Fan, W.; Zeng, C.; Zhang, T.; Cheng, S.; Ge, Y. Prognosis of severe drug-induced acute interstitial nephritis requiring renal replacement therapy. Ren. Fail. 2021, 43, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, R.; Eknoyan, G. Acute interstitial nephritis—A reappraisal and update. Clin. Nephrol. 2014, 82, 149–162. [Google Scholar] [CrossRef]
- Verstegen, R.H.J.; Phillips, E.J.; Juurlink, D.N. First-line therapy in drug reaction with eosinophilia and systemic symptoms (DReSS): Thinking beyond corticosteroids. Front. Med. 2023, 10, 1138464. [Google Scholar] [CrossRef]
- Chiou, C.C.; Yang, L.C.; Hung, S.I.; Chang, Y.C.; Kuo, T.T.; Ho, H.C.; Hu, S.; Hong, H.-S.; Chung, W.-H. Clinicopathological features and prognosis of drug rash with eosinophilia and systemic symptoms: A study of 30 cases in Taiwan. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, E.; Yanes, D.; Imadojemu, S.; Kroshinsky, D. Evaluation of Cyclosporine for the Treatment of DRESS Syndrome. JAMA Dermatol. 2020, 156, 704–706. [Google Scholar] [CrossRef]
- Tan, K.; Testro, A. Cyclosporine as an alternative immunosuppressant for steroid-resistant drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome. BMJ Case Rep. 2023, 16, e250983. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, M.G.; Wong, A.; Dutz, J.P. Cyclosporine Treatment of Drug-Induced Hypersensitivity Syndrome. JAMA Dermatol. 2016, 152, 1254–1257. [Google Scholar] [CrossRef]
- Hashizume, H.; Kageyama, R.; Kaneko, Y. Short course of cyclosporin A as a treatment option for drug-induced hypersensitivity syndrome: Case reports and review of the published work. J. Dermatol. 2018, 45, e169–e170. [Google Scholar] [CrossRef] [PubMed]
- Durak, C.; Aydemir, S.; Varol, F.; Aygün, F.; Çokuğraş, H.C. A case of severe DRESS syndrome treated with therapeutic plasma exchange and intravenous immunoglobulin therapy. J. Clin. Apher. 2022, 37, 600–605. [Google Scholar] [CrossRef]
- Alexander, T.; Ba, E.I.; Park, Y.; Duncan, D.; Peden, D.; Sheikh, S.; Ferris, M. Severe DRESS Syndrome Managed with Therapeutic Plasma Exchange. Pediatrics 2013, 131, e945–e949. [Google Scholar] [CrossRef] [PubMed]
- de Lagrán, I.M.; Marcos, P.; Batlle, M.; Alonso, E.; Plana, A.; Tomasa, T. Leukapheresis in the management of drug rash with eosinophilia and systemic symptoms syndrome. Med. Intensiv. 2017, 41, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Ange, N.; Alley, S.; Fernando, S.L.; Coyle, L.; Yun, J. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) syndrome successfully treated with mepolizumab. J. Allergy Clin. Immunol. Pr. 2017, 6, 1059–1060. [Google Scholar] [CrossRef]
- Thein, O.S.; Sutton, B.; Thickett, D.R.; Parekh, D. Mepolizumab rescue therapy for acute pneumonitis secondary to DRESS. BMJ Case Rep. 2019, 12, e231355. [Google Scholar] [CrossRef]
- Truong, K.; Kelly, S.; Bayly, A.; Smith, A. Successful Mepolizumab Treatment for DRESS-Induced Refractory Eosinophilic Myocarditis and Concurrent Thyroiditis. BMJ Case Rep. 2021, 14, e242240. [Google Scholar] [CrossRef]
- Pitlick, M.M.; Li, J.T.; Pongdee, T. Current and emerging biologic therapies targeting eosinophilic disorders. World Allergy Organ. J. 2022, 15, 100676. [Google Scholar] [CrossRef]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; Fitzgerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef]
- Pavord, I.D.; Chanez, P.; Criner, G.J.; Kerstjens, H.A.; Korn, S.; Lugogo, N.; Martinot, J.-B.; Sagara, H.; Albers, F.C.; Bradford, E.S.; et al. Mepolizumab for Eosinophilic Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2017, 377, 1613–1629. [Google Scholar] [CrossRef]
- Rothenberg, M.E.; Klion, A.D.; Roufosse, F.E.; Kahn, J.E.; Weller, P.F.; Simon, H.-U.; Schwartz, L.B.; Rosenwasser, L.J.; Ring, J.; Griffin, E.F.; et al. Treatment of patients with the hypereosinophilic syndrome with mepolizumab. N. Engl. J. Med. 2008, 358, 1215–1228. [Google Scholar] [CrossRef] [PubMed]
- Damsky, W.E.; Vesely, M.; Lee, A.I.; Choi, J.; Meyer, A.-C.; Chen, M.; Ahmad, T.; King, B. Drug-induced hypersensitivity syndrome with myocardial involvement treated with tofacitinib. JAAD Case Rep. 2019, 5, 1018–1026. [Google Scholar] [CrossRef]
- Kim, D.Y.; Kobayashi, T.; Voisin, B.; Jo, J.-H.; Sakamoto, K.; Jin, S.-P.; Kelly, M.; Pasieka, H.B.; Naff, J.L.; Meyerle, J.H.; et al. Targeted therapy guided by single-cell transcriptomic analysis in drug-induced hypersensitivity syndrome: A case report. Nat. Med. 2020, 26, 236–243. [Google Scholar] [CrossRef]
- Martinez-Cabriales, S.A.; Shear, N.H.; I Gonzalez-Moreno, E. Liver involvement in the drug reaction, eosinophilia, and systemic symptoms syndrome. World J. Clin. Cases 2019, 7, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J.C.; Stern, R.S. Severe Adverse Cutaneous Reactions to Drugs. N. Engl. J. Med. 1994, 331, 1272–1285. [Google Scholar] [CrossRef]
- Ichai, P.; Laurent-Bellue, A.; Saliba, F.; Moreau, D.; Besch, C.; Francoz, C.; Valeyrie-Allanore, L.; Bretagne, S.R.; Boudon, M.; Antonini, T.M.; et al. Acute Liver Failure/Injury Related to Drug Reaction with Eosinophilia and Systemic Symptoms: Outcomes and Prognostic Factors. Transplantation 2017, 101, 1830–1837. [Google Scholar] [CrossRef]
- Deng, M.; Wu, H.; Yu, M.; Tian, Y.; Li, Y.; Xiao, X. Co-Occurrence of Multiple Endocrine Abnormalities Induced by the DIHS/DRESS. Int. J. Endocrinol. 2019, 2019, 7959615. [Google Scholar] [CrossRef] [PubMed]
- Sasidharanpillai, S.; Joseph, A.; Ajithkumar, K.; Devi, K. Autoimmune Diseases, End Organ Dysfunction and Adverse Drug Reaction Following Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): A retrospective cohort study. Indian Dermatol. Online J. 2021, 12, 722. [Google Scholar] [CrossRef]
- Teo, R.Y.; Tay, Y.-K.; Tan, C.-H.; Ng, V.; Oh, D.C. Presumed dapsone-induced drug hypersensitivity syndrome causing reversible hypersensitivity myocarditis and thyrotoxicosis. Ann. Acad. Med. Singap. 2006, 35, 833–836. [Google Scholar] [CrossRef]
- Brown, R.J.; Rother, K.I.; Artman, H.; Mercurio, M.G.; Wang, R.; Looney, R.J.; Cowen, E.W. Minocycline-induced drug hypersensitivity syndrome followed by multiple autoimmune sequelae. Arch. Dermatol. 2009, 145, 63–66. [Google Scholar] [CrossRef]
- Funck-Brentano, E.; Duong, T.; Family, D.; Bouaziz, J.D.; Ortonne, N.; Bagot, M.; Roujeau, J.-C.; Wolkenstein, P.; Valeyrie-Allanore, L. Auto-immune thyroiditis and drug reaction with eosinophilia and systemic symptoms (DRESS) associated with HHV-6 viral reactivation. Ann. Dermatol. Venereol. 2011, 138, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Cookson, H.; Creamer, D.; Walsh, S. Thyroid dysfunction in drug reaction with eosinophilia and systemic symptoms (DRESS): An unusual manifestation of systemic drug hypersensitivity. Br. J. Dermatol. 2013, 168, 1130–1132. [Google Scholar] [CrossRef] [PubMed]
- Kano, Y.; Sakuma, K.; Shiohara, T. Sclerodermoid graft-versus-host disease-like lesions occurring after drug-induced hypersen-sitivity syndrome. Br. J. Dermatol. 2007, 156, 1061–1063. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Chang, C.-Y.; Cho, Y.-T.; Chiu, H.-C.; Chu, C.-Y. Long-term sequelae of drug reaction with eosinophilia and systemic symptoms: A retrospective cohort study from Taiwan. J. Am. Acad. Dermatol. 2013, 68, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Botelho, L.F.F.; Higashi, V.S.; Padilha, M.H.V.D.Q.; Enokihara, M.M.S.E.S.; Porro, A.M. DRESS: Clinicopathological features of 10 cases from an University Hospital in São Paulo. An. Bras. Dermatol. 2012, 87, 703–707. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | |||
|---|---|---|---|
| Sex | |||
| Female | 31 (31/71, 43.66%) | ||
| Male | 40 (40/71, 56.34%) | ||
| Age (Years) | |||
| ≤18 | 4 (4/71, 5.63%) | ||
| 19–64 | 41 (41/71, 57.75%) | ||
| ≥65 | 26 (26/71, 36.62%) | ||
| Comorbidities | |||
| Reported | Positive | Negative | |
| CKD | 14 (14/71, 19.72%) | 10 (10/14, 71.43%) | 4 (4/14, 28.57%) |
| HTN | 27 (27/71, 38.02%) | 21 (21/27, 77.78%) | 6 (6/27, 22.22%) |
| Immunosuppression | 5 (5/71, 7.04%) | 3 (3/5, 60%) | 2 (2/5, 40%) |
| Viral Reactivation | |||
| Reported | Positive | Negative | |
| CMV | 43 (43/71, 60.56%) | 7 (7/43, 16.28%) | 36 (36/43, 83.72%) |
| HHV-6 | 43 (43/71, 60.56%) | 10 (10/43, 23.26%) | 33 (33/43, 76.74%) |
| EBV | 43 (43/71, 60.56%) | 9 (9/43, 20.93%) | 34 (34/43, 79.07%) |
| Prognoses | |||
| Reported | Positive | Negative | |
| Sequelae | 7 (7/71, 9.86%) | 6 (6/7, 85.71%) | 1 (1/7, 14.29%) |
| Reported | Discharged | Death | |
| Outcome | 69 (69/71, 97.18%) | 60 (60/69, 86.96%) | 9 (9/69, 13.04%) |
| Variables | Alive | Died | Univariate |
|---|---|---|---|
| N (%) or Mean ± SD | N (%) or Mean ± SD | p-Value | |
| Female sex | 24 (40.0) | 7 (77.8) | 0.034 * |
| Age, years | 51.8 ± 20.3 | 62.5 ± 14.7 | 0.075 ** |
| Chronic kidney disease present | 8 (72.7) | 2 (66.7) | 0.837 * |
| Latency, days | 22.0 ± 15.2 | 24.7 ± 17.7 | 0.643 ** |
| Organs involved, number | 2.0 ± 0.8 | 2.2 ± 0.4 | 0.277 ** |
| Renal manifestation | |||
| Oliguria | 10 (76.9) | 2 (100.0) | 0.749 * |
| Anuria | 2 (15.4) | 0 (0.0) | |
| Oligoanuria | 1 (7.7) | 0 (0.0) | |
| Creatinine peak, mg/dL | 4.7 ± 3.6 | 4.2 ± 2.6 | 0.693 ** |
| Creatinine high values | 49 (92.5) | 8 (88.9) | 0.717 * |
| Proteinuria present | 19 (86.4) | 1 (50.0) | 0.186 * |
| Hematuria present | 11 (64.7) | 0 (0.0) | 0.197 * |
| Eosinophils peak | 4088.9 ± 5062.5 | 2712.2 ± 3512.9 | 0.327 ** |
| Eosinophilia present | 46 (85.2) | 7 (77.8) | 0.573 * |
| RegiSCAR score | 6.2 ± 0.9 | 6.7 ± 1.8 | 0.290 ** |
| Probable | 13 (21.7) | 3 (33.3) | 0.439 * |
| Definite | 47 (78.3) | 6 (66.7) | |
| Complications (hemodialysis) | 16 (84.2) | 3 (75.0) | 0.659 * |
| Hemodialysis, days | 23.7 ± 33.3 | 21.0 ± 33.8 | 0.902 ** |
| Improvement in renal function, days | 66.92 ± 132.2 | 9.00 ± 4.3 | 0.255 ** |
| CMV, positive | 7 (18.9) | 0 (0.0) | 0.339 * |
| HHV7, positive | 0 (0.0) | 0 (0.0) | 1.000 * |
| EBV, positive | 8 (21.6) | 0 (0.0) | 0.300 * |
| Therapy with steroids | |||
| Steroids monotherapy | 34 (58.6) | 8 (88.9) | 0.140 |
| Steroids + other therapy | 18 (31.0) | 0 (0.0) | |
| other | 6 (10.3) | 1 (11.1) | |
| Way of administration of therapy | |||
| Per oral | 8 (28.6) | 1 (33.3) | 0.414 |
| i.v. | 10 (35.7) | 2 (66.7) | |
| Combination | 10 (35.7) | 0 (0.0) | |
| Topic steroids | 8 (13.3) | 0 (0.0) | 0.244 |
| Renal Findings | |
|---|---|
| Urine output | |
| Reported | 16 (16/71, 22.53%) |
| Anuria | 4 (4/16, 25%) |
| Oliguria | 12 (12/16, 75%) |
| Proteinuria | |
| Reported | 25 (25/71, 35.21%) |
| Yes | 21 (21/25, 84%) |
| No | 4 (4/25, 16%) |
| Hematuria | |
| Reported | 18 (18/71, 25.35%) |
| Yes | 11 (11/18, 61.1%) |
| No | 7 (7/18, 38.9%) |
| Renal biopsy | |
| Reported | 18 (18/71, 25.35%) |
| Hemodialysis | |
| Yes | 21 (21/71, 29.58%) |
| Imaging | |
| Reported | 22 (22/71, 30.98%) |
| Ultrasound | 21 (21/22, 95.45%) |
| CT ABD | 11 (11/22, 50%) |
| MRI Body | 1 (1/22, 4.54%) |
| Variables | Multivariate | |
|---|---|---|
| OR | p-Value * | |
| Female sex | 3.53 | 1.000 |
| Age, years | 0.07 | 0.998 |
| Chronic kidney disease present | 0.00 | 0.999 |
| Creatinine high values | 0.00 | 0.998 |
| Proteinuria present | 0.21 | 0.999 |
| Hematuria present | 0.92 | 0.999 |
| Eosinophilia present | 0.98 | 1.000 |
| RegiSCAR score | 0.72 | 0.999 |
| Hemodialysis, days | 0.35 | 0.999 |
| CMV, positive | 0.40 | 0.999 |
| Study | Country | Most Common Causative Medication | Number of Patients in the Study | % of Patients with Renal Involvement |
|---|---|---|---|---|
| Ben M’rad M et al., 2009 [88] | France | Antibiotics | 24 cases—12 females (50%) | 17% |
| Eshki M et al., 2009 [91] | France | Xanthine oxidase enzyme inhibitor | 15 cases—10 females (66.66%) | 40% |
| Um SJ et al., 2010 [87] | Korea | Anticonvulsants | 38 cases—20 females (52.6%) | 15.8% |
| Chen YC et al., 2010 [90] | Taiwan | Xanthine oxidase enzyme inhibitor | 60 cases—34 females (56.66%) | 40% |
| Walsh S et al., 2013 [92] | U.K. | Anticonvulsants | 27 cases—17 females (62.96%) | 7.41% |
| Ushigome Y et al., 2013 [93] | Japan | Anticonvulsants | 34 cases—16 females (47.05%) | 0.0% |
| Sasidharanpillai S et al., 2014 [83] | India | Anticonvulsants | 26 cases—14 females (53.84%) | 7.69% |
| Sultan SJ et al., 2015 [84] | India | Anticonvulsants | 17 cases—9 females (52.9%) | 64.7% |
| Hiransuthikul A et al., 2015 [85] | Thailand | Anticonvulsants | 52 cases—37 females (71.2%) | 15.4% |
| Lee JY et al., 2017 [94] | Korea | Anticonvulsants | 25 cases—14 females (56%) | 28% |
| Mehrholz D et al., 2017 [95] | Poland | Anticonvulsants | 10 cases—7 females (70%) | 30% |
| Metterle L et al., 2020 [89] | USA | Anticonvulsants | 130 cases—66 females (50.8%) | 15.4% |
| Kim GY et al., 2020 [96] | USA | Anticonvulsants | 148 cases—66 females (44.6%) | 16.9% |
| Toniato A et al., 2021 [86] | Italy | Xanthine oxidase enzyme inhibitor | 25 cases—15 females (60%) | 37.5% |
| Sandhu S et al., 2021 [97] | India | Anticonvulsants and anti-infectives | 20 cases—8 females (40%) | 15% |
| Bedouelle E et al., 2022 [98] | France | Antibiotics | 49 cases—27 females (55.1%) | 26.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dagnon da Silva, M.; Domingues, S.M.; Oluic, S.; Radovanovic, M.; Kodela, P.; Nordin, T.; Paulson, M.R.; Joksimović, B.; Adetimehin, O.; Singh, D.; et al. Renal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of 71 Cases. J. Clin. Med. 2023, 12, 4576. https://doi.org/10.3390/jcm12144576
Dagnon da Silva M, Domingues SM, Oluic S, Radovanovic M, Kodela P, Nordin T, Paulson MR, Joksimović B, Adetimehin O, Singh D, et al. Renal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of 71 Cases. Journal of Clinical Medicine. 2023; 12(14):4576. https://doi.org/10.3390/jcm12144576
Chicago/Turabian StyleDagnon da Silva, Marilia, Sidney Marcel Domingues, Stevan Oluic, Milan Radovanovic, Pratyusha Kodela, Terri Nordin, Margaret R. Paulson, Bojan Joksimović, Omobolanle Adetimehin, Devender Singh, and et al. 2023. "Renal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of 71 Cases" Journal of Clinical Medicine 12, no. 14: 4576. https://doi.org/10.3390/jcm12144576
APA StyleDagnon da Silva, M., Domingues, S. M., Oluic, S., Radovanovic, M., Kodela, P., Nordin, T., Paulson, M. R., Joksimović, B., Adetimehin, O., Singh, D., Madrid, C., Cardozo, M., Baralic, M., & Dumic, I. (2023). Renal Manifestations of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome: A Systematic Review of 71 Cases. Journal of Clinical Medicine, 12(14), 4576. https://doi.org/10.3390/jcm12144576