
Effectiveness of Robotic Arm-Assisted Total Knee Arthroplasty on Transfusion Rate in Staged Bilateral Surgery


Abstract
1. Introduction
2. Materials and Methods
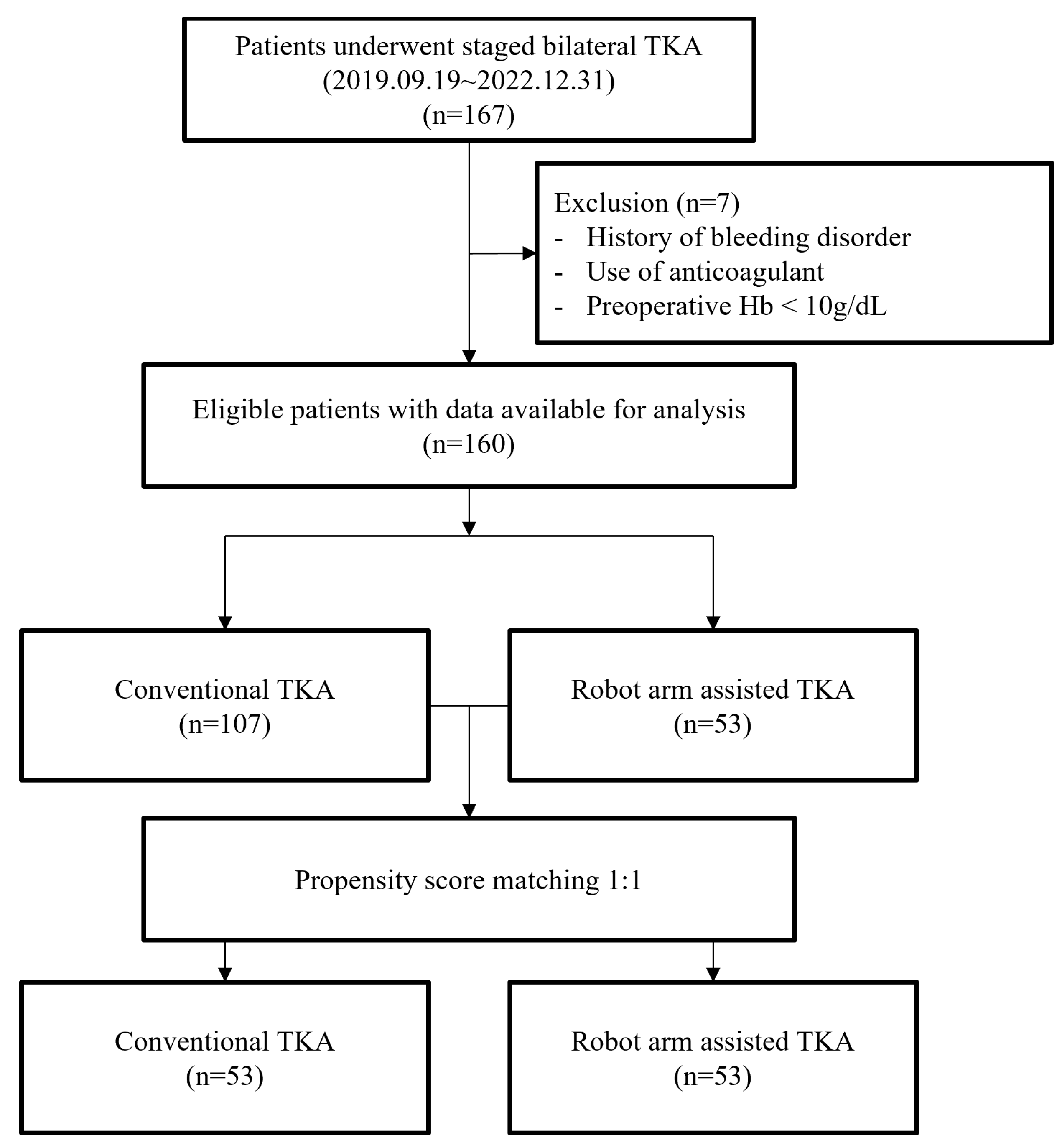
2.1. Patients
2.2. Surgical Intervention
2.3. Postoperative Management
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gascón, P.; Zoumbos, N.C.; Young, N.S. Immunologic abnormalities in patients receiving multiple blood transfusions. Ann. Intern. Med. 1984, 100, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Heddle, N.M.; Klama, L.N.; Griffith, L.; Roberts, R.; Shukla, G.; Kelton, J.G. A prospective study to identify the risk factors associated with acute reactions to platelet and red cell transfusions. Transfusion 1993, 33, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Peng, H.; Zhou, G.J.; Yin, D. Perioperative blood management strategies for total knee arthroplasty. Orthop. Surg. 2018, 10, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, G.B.; Busch, M.P.; Kleinman, S.H.; Korelitz, J.J. The risk of transfusion-transmitted viral infections. The Retrovirus Epidemiology Donor Study. N. Engl. J. Med. 1996, 334, 1685–1690. [Google Scholar] [CrossRef] [PubMed]
- Taneja, A.; El-Bakoury, A.; Khong, H.; Railton, P.; Sharma, R.; Johnston, K.D.; Puloski, S.; Smith, C.; Powell, J. Association between allogeneic blood transfusion and wound infection after total hip or knee arthroplasty: A retrospective case-control study. J. Bone Jt. Infect. 2019, 4, 99–105. [Google Scholar] [CrossRef]
- Husted, H.; Hansen, H.C.; Holm, G.; Bach-Dal, C.; Rud, K.; Andersen, K.L.; Kehlet, H. What determines length of stay after total hip and knee arthroplasty? A nationwide study in Denmark. Arch. Orthop. Trauma Surg. 2010, 130, 263–268. [Google Scholar] [CrossRef]
- Husted, H.; Holm, G.; Jacobsen, S. Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: Fast-track experience in 712 patients. Acta Orthop. 2008, 79, 168–173. [Google Scholar] [CrossRef]
- Good, L.; Peterson, E.; Lisander, B. Tranexamic acid decreases external blood loss but not hidden blood loss in total knee replacement. Br. J. Anaesth. 2003, 90, 596–599. [Google Scholar] [CrossRef]
- Palmer, A.; Chen, A.; Matsumoto, T.; Murphy, M.; Price, A. Blood management in total knee arthroplasty: State-of-the-art review. J. ISAKOS 2018, 3, 358–366. [Google Scholar] [CrossRef]
- Seo, J.G.; Moon, Y.W.; Park, S.H.; Kim, S.M.; Ko, K.R. The comparative efficacies of intra-articular and IV tranexamic acid for reducing blood loss during total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1869–1874. [Google Scholar] [CrossRef]
- Xie, J.; Hu, Q.; Huang, Q.; Ma, J.; Lei, Y.; Pei, F. Comparison of intravenous versus topical tranexamic acid in primary total hip and knee arthroplasty: An updated meta-analysis. Thromb. Res. 2017, 153, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Zufferey, P.; Merquiol, F.; Laporte, S.; Decousus, H.; Mismetti, P.; Auboyer, C.; Samama, C.M.; Molliex, S. Do antifibrinolytics reduce allogeneic blood transfusion in orthopedic surgery? Anesthesiology 2006, 105, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Zhang, Z.; Wang, G.; Rong, C.; Zhu, W.; Lu, X.; Liu, Y.; Zhang, H. Accuracies of bone resection, implant position, and limb alignment in robotic-arm-assisted total knee arthroplasty: A prospective single-centre study. J. Orthop. Surg. Res. 2022, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Stimson, L.N.; Steelman, K.R.; Hamilton, D.A.; Chen, C.; Darwiche, H.F.; Mehaidli, A. Evaluation of blood loss in conventional vs MAKOplasty total knee arthroplasty. Arthroplast. Today 2022, 16, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Dhillon, K.; Mahapatra, P.; Popat, R.; Zakieh, O.; Kim, W.J.; Nathwani, D. Blood loss and transfusion risk in robotic-assisted knee arthroplasty: A retrospective analysis. Int. J. Med. Robot. 2021, 17, e2308. [Google Scholar] [CrossRef] [PubMed]
- St Mart, J.P.; Goh, E.L. The current state of robotics in total knee arthroplasty. EFORT Open Rev. 2021, 6, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Cushner, F.D.; Friedman, R.J. Blood loss in total knee arthroplasty. Clin. Orthop. Relat. Res. 1991, 269, 98–101. [Google Scholar] [CrossRef]
- Chan, P.K.; Hwang, Y.Y.; Cheung, A.; Yan, C.H.; Fu, H.; Chan, T.; Fung, W.C.; Cheung, M.H.; Chan, V.W.K.; Chiu, K.Y. Blood transfusions in total knee arthroplasty: A retrospective analysis of a multimodal patient blood management programme. Hong Kong Med. J. 2020, 26, 201–207. [Google Scholar] [CrossRef]
- Vaish, A.; Belbase, R.J.; Vaishya, R. Is blood transfusion really required in simultaneous bilateral total knee replacement: A retrospective observational study. J. Clin. Orthop. Trauma 2020, 11 (Suppl. 2), S214–S218. [Google Scholar] [CrossRef]
- Lee, S.S.; Lee, J.; Moon, Y.W. Efficacy of immediate postoperative intravenous iron supplementation after staged bilateral total knee arthroplasty. BMC Musculoskelet. Disord. 2023, 24, 17. [Google Scholar] [CrossRef]
- Van der List, J.P.; Chawla, H.; Pearle, A.D. Robotic-assisted knee arthroplasty: An overview. Am. J. Orthop. (Belle Mead NJ) 2016, 45, 202–211. [Google Scholar] [PubMed]
- Kayani, B.; Konan, S.; Pietrzak, J.R.T.; Haddad, F.S. Iatrogenic bone and soft tissue trauma in robotic-arm assisted total knee arthroplasty compared with conventional jig-based total knee arthroplasty: A prospective cohort study and validation of a new classification system. J. Arthroplast. 2018, 33, 2496–2501. [Google Scholar] [CrossRef]
- Molloy, D.O.; Mockford, B.J.; Wilson, R.K.; Beverland, D.E. Blood loss following soft tissue release in total knee arthroplasty of the valgus knee. Orthop. Proc. 2005, 87 (Supp_II), 156. [Google Scholar] [CrossRef]
- Hampp, E.L.; Sodhi, N.; Scholl, L.; Deren, M.E.; Yenna, Z.; Westrich, G.; Mont, M.A. Less iatrogenic soft-tissue damage utilizing robotic-assisted total knee arthroplasty when compared with a manual approach: A blinded assessment. Bone Jt. Res. 2019, 8, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Lei, K.; Liu, L.M.; Guo, L. Robotic systems in total knee arthroplasty: Current surgical trauma perspectives. Burn. Trauma 2022, 10, tkac049. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Li, Q.; Wei, B.G.; Zhang, X.S.; Torsha, T.T.; Xiao, J.; Shi, Z.J. Blood loss of total knee arthroplasty in osteoarthritis: An analysis of influential factors. J. Orthop. Surg. Res. 2018, 13, 325. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Dan, M.; Martinez Martos, S.; Beller, E. Blood management strategies in total knee arthroplasty. Knee Surg. Relat. Res. 2016, 28, 179–187. [Google Scholar] [CrossRef]
- Lee, Q.J.; Mak, W.P.; Yeung, S.T.; Wong, Y.C.; Wai, Y.L. Blood management protocol for total knee arthroplasty to reduce blood wastage and unnecessary transfusion. J. Orthop. Surg. 2015, 23, 66–70. [Google Scholar] [CrossRef]
- Moráis, S.; Ortega-Andreu, M.; Rodríguez-Merchán, E.C.; Padilla-Eguiluz, N.G.; Pérez-Chrzanowska, H.; Figueredo-Zalve, R.; Gómez-Barrena, E. Blood transfusion after primary total knee arthroplasty can be significantly minimised through a multimodal blood-loss prevention approach. Int. Orthop. 2014, 38, 347–354. [Google Scholar] [CrossRef]
- Chen, Z.Y.; Wu, H.Z.; Zhu, P.; Feng, X.B. Postoperative changes in hemoglobin and hematocrit in patients undergoing primary total hip and knee arthroplasty. Chin. Med. J. 2015, 128, 1977–1979. [Google Scholar] [CrossRef]
- Makaram, N.S.; Roberts, S.B.; Macpherson, G.J. Simultaneous bilateral total knee arthroplasty is associated with shorter length of stay but increased mortality compared with staged bilateral total knee arthroplasty: A systematic review and meta-analysis. J. Arthroplast. 2021, 36, 2227–2238. [Google Scholar] [CrossRef] [PubMed]
- Tsay, E.L.; Grace, T.R.; Vail, T.; Ward, D. Bilateral simultaneous vs staged total knee arthroplasty: Minimal difference in perioperative risks. J. Arthroplast. 2019, 34, 2944–2949.e1. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.S.; Calem, D.; Sherman, M.B.; Sharkey, P.F. Short interval staged bilateral total knee arthroplasty: Safety compared to simultaneous and later staged bilateral total knee arthroplasty. J. Arthroplast. 2021, 36, 3901–3908. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.F.; Rasouli, M.R.; Vegari, D.N.; Huang, R.C.; Maltenfort, M.G.; Parvizi, J. Staged bilateral total knee arthroplasty: Time of the second side. J. Knee Surg. 2015, 28, 311–314. [Google Scholar] [CrossRef]
- Johnson, M.A.; Barchick, S.R.; Kerbel, Y.E.; DeAngelis, R.D.; Velasco, B.; Nelson, C.L.; Israelite, C.L. No difference in perioperative complications for bilateral total knee arthroplasty staged at 1 week compared with delayed staging. J. Am. Acad. Orthop. Surg. 2022, 30, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liu, H.; Zhang, H.; Song, J.; Zhang, L. Bilateral total knee arthroplasty: Simultaneous or staged? A systematic review and meta-analysis. Medicine 2019, 98, e15931. [Google Scholar] [CrossRef] [PubMed]
- Cankaya, D.; Ozkurt, B.; Aydin, C.; Tabak, A.Y. No difference in blood loss between posterior-cruciate-ligament-retaining and posterior-cruciate-ligament-stabilized total knee arthroplasties. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1865–1869. [Google Scholar] [CrossRef] [PubMed]
- Mähringer-Kunz, A.; Efe, T.; Fuchs-Winkelmann, S.; Schüttler, K.F.; Paletta, J.R.; Heyse, T.J. Bleeding in TKA: Posterior stabilized vs. cruciate retaining. Arch. Orthop. Trauma Surg. 2015, 135, 867–870. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | C-TKA (n = 53) | R-TKA (n = 53) | p Value * |
|---|---|---|---|
| Age, years | 70.6 ± 7.5 | 72.3 ± 5.9 | 0.187 a |
| Sex (F:M) | 42:11 | 45:8 | 0.447 b |
| BMI (kg/m2) | 27.2 ± 3.6 | 27.7 ± 3.4 | 0.459 a |
| ASA physical status score (1/2/3) | 2/37/14 | 1/36/16 | 0.788 b |
| Preop Hb level | 13.4 ± 1.4 | 13.1 ± 1.2 | 0.177 a |
| 1st TKA | |||
| HKA angle (°) | 9.9 ± 5.3 | 8.6 ± 5.5 | 0.203 a |
| K–L grade (III/IV) | 13/40 | 13/40 | 1.0 b |
| 2nd TKA | |||
| HKA angle (°) | 7.3 ± 5.8 | 8.0 ± 4.1 | 0.473 a |
| K–L grade (III/IV) | 22/31 | 21/32 | 1.0 b |
| C-TKA (n = 53) | R-TKA (n = 53) | p Value * | |
|---|---|---|---|
| Mean, std dev | Mean, std dev | ||
| Preop Hb level (g/dL) | 13.50 ± 1.44 | 13.15 ± 1.19 | 0.177 a |
| 1st TKA POD 0 | 12.65 ± 1.36 | 12.96 ± 1.39 | 0.241 a |
| 1st TKA POD 1 | 11.22 ± 1.19 | 11.12 ± 1.32 | 0.671 a |
| 1st TKA POD 2 | 10.09 ± 1.12 | 10.13 ± 1.13 | 0.863 a |
| 1st TKA POD 4 | 10.03 ± 1.09 | 10.18 ± 1.06 | 0.463 a |
| 1st TKA POD 6 | 10.04 ± 0.97 | 10.40 ± 1.02 | 0.069 a |
| 2nd TKA POD 0 | 10.32 ± 1.25 | 10.75 ± 1.20 | 0.078 a |
| 2nd TKA POD 1 | 8.89 ± 1.05 | 9.27 ± 0.85 | 0.044 a |
| 2nd TKA POD 2 | 8.47 ± 1.01 | 8.74 ± 0.61 | 0.110 a |
| 2nd TKA POD 4 | 9.13 ± 0.85 | 9.44 ± 0.88 | <0.001 |
| 2nd TKA POD 6 | 9.41 ± 1.12 | 9.55 ± 0.71 | 0.487 a |
| Nadir Hb level after 1st TKA (g/dL) | 9.63 ± 1.06 | 9.80 ± 0.99 | 0.405 a |
| Nadir Hb level after 2nd TKA (g/dL) | 8.11 ± 0.86 | 8.55 ± 0.50 | 0.002 a |
| 1st TKA operation time (min) | 90.3 ± 10.4 | 94.8 ± 14.6 | 0.068 a |
| 2nd TKA operation time (min) | 89.4 ± 18.5 | 93.8 ± 15.3 | 0.194 a |
| C-TKA (n = 53) | R-TKA (n = 53) | p Value * | |
|---|---|---|---|
| Transfusion rate after 1st TKA (%) | 2/53 (3.8%) | 1/53 (1.9%) | 0.558 b |
| Transfusion rate after 2nd TKA (%) | 12/51 (23.5%) | 4/52 (7.7%) | 0.030 b |
| Overall transfusion (%) | 14/53 (26.4%) | 5/53 (9.4%) | 0.023 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Jung, H.J.; Choi, B.S.; Ro, D.H.; Kim, J.I. Effectiveness of Robotic Arm-Assisted Total Knee Arthroplasty on Transfusion Rate in Staged Bilateral Surgery. J. Clin. Med. 2023, 12, 4570. https://doi.org/10.3390/jcm12144570
Lee JH, Jung HJ, Choi BS, Ro DH, Kim JI. Effectiveness of Robotic Arm-Assisted Total Knee Arthroplasty on Transfusion Rate in Staged Bilateral Surgery. Journal of Clinical Medicine. 2023; 12(14):4570. https://doi.org/10.3390/jcm12144570
Chicago/Turabian StyleLee, Jong Hwa, Ho Jung Jung, Byung Sun Choi, Du Hyun Ro, and Joong Il Kim. 2023. "Effectiveness of Robotic Arm-Assisted Total Knee Arthroplasty on Transfusion Rate in Staged Bilateral Surgery" Journal of Clinical Medicine 12, no. 14: 4570. https://doi.org/10.3390/jcm12144570
APA StyleLee, J. H., Jung, H. J., Choi, B. S., Ro, D. H., & Kim, J. I. (2023). Effectiveness of Robotic Arm-Assisted Total Knee Arthroplasty on Transfusion Rate in Staged Bilateral Surgery. Journal of Clinical Medicine, 12(14), 4570. https://doi.org/10.3390/jcm12144570