
Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction
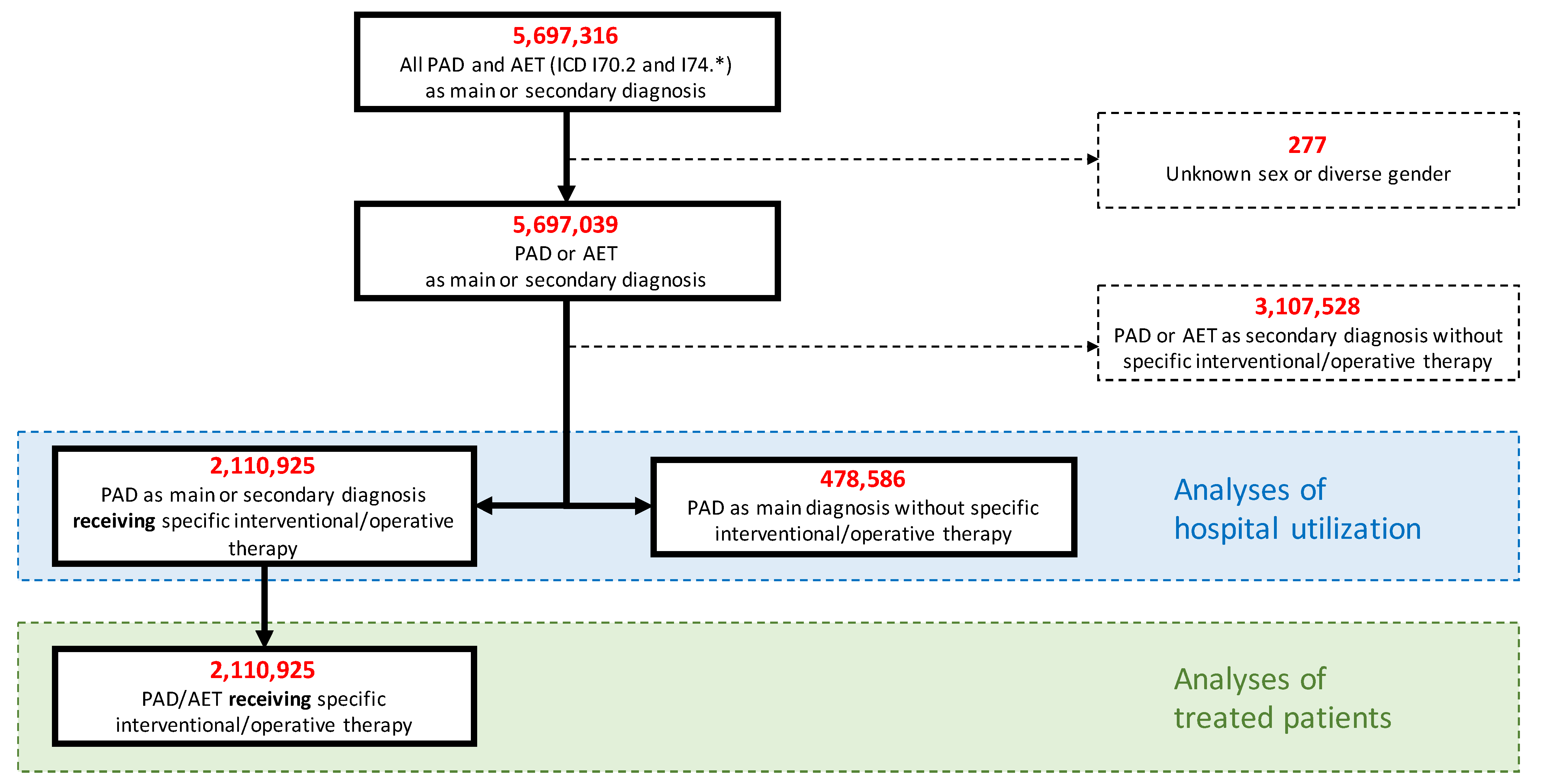
2.2. Study Population
2.3. Patient Characteristics, Hospital Incidence and Utilization, Outcomes
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Characteristics of Interventionally or Surgically Treated Cases
3.3. Procedural Characteristics of Interventionally or Surgically Treated Cases
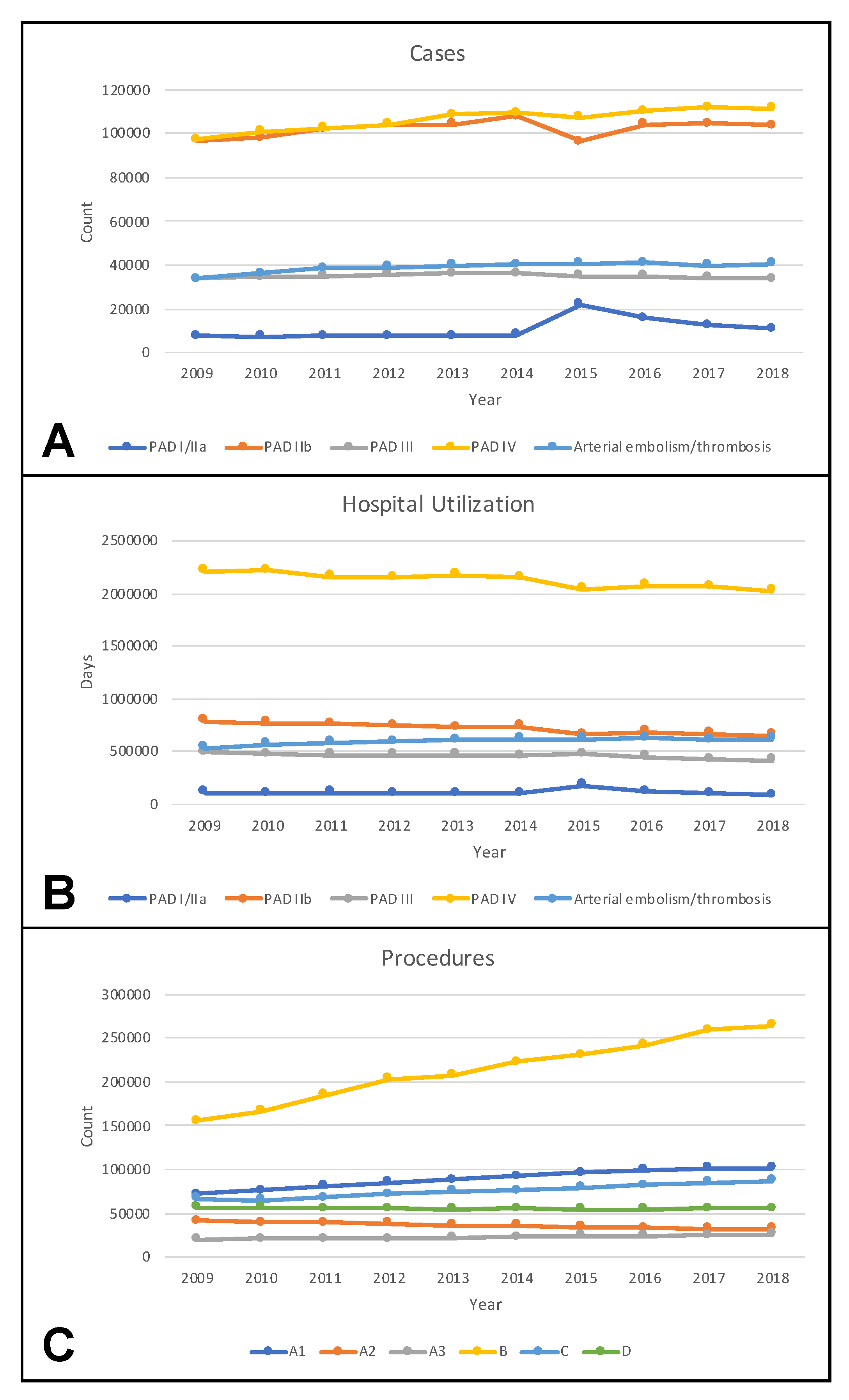
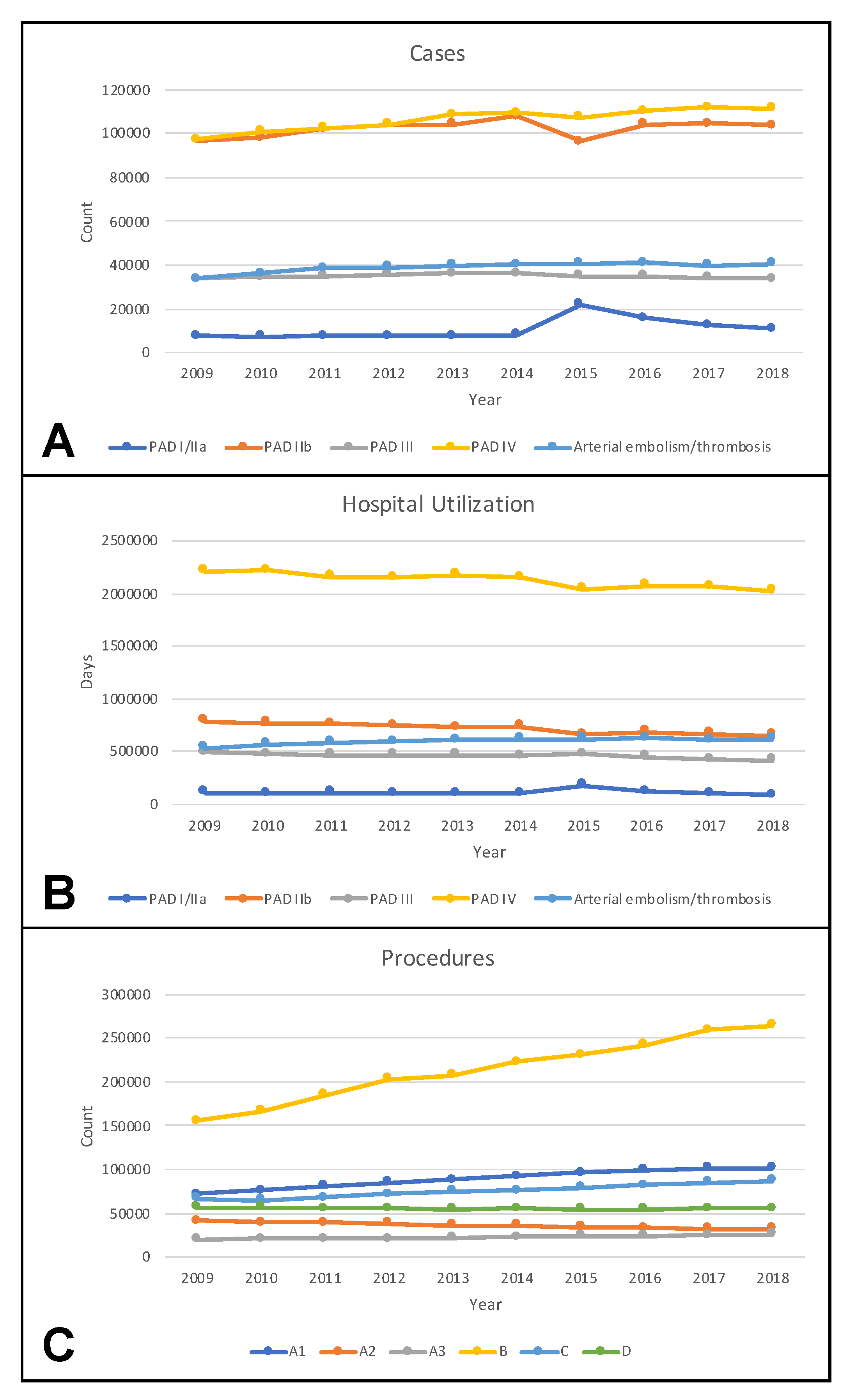
3.4. Temporal Trends of Cases, Hospital Utilization, and Procedures
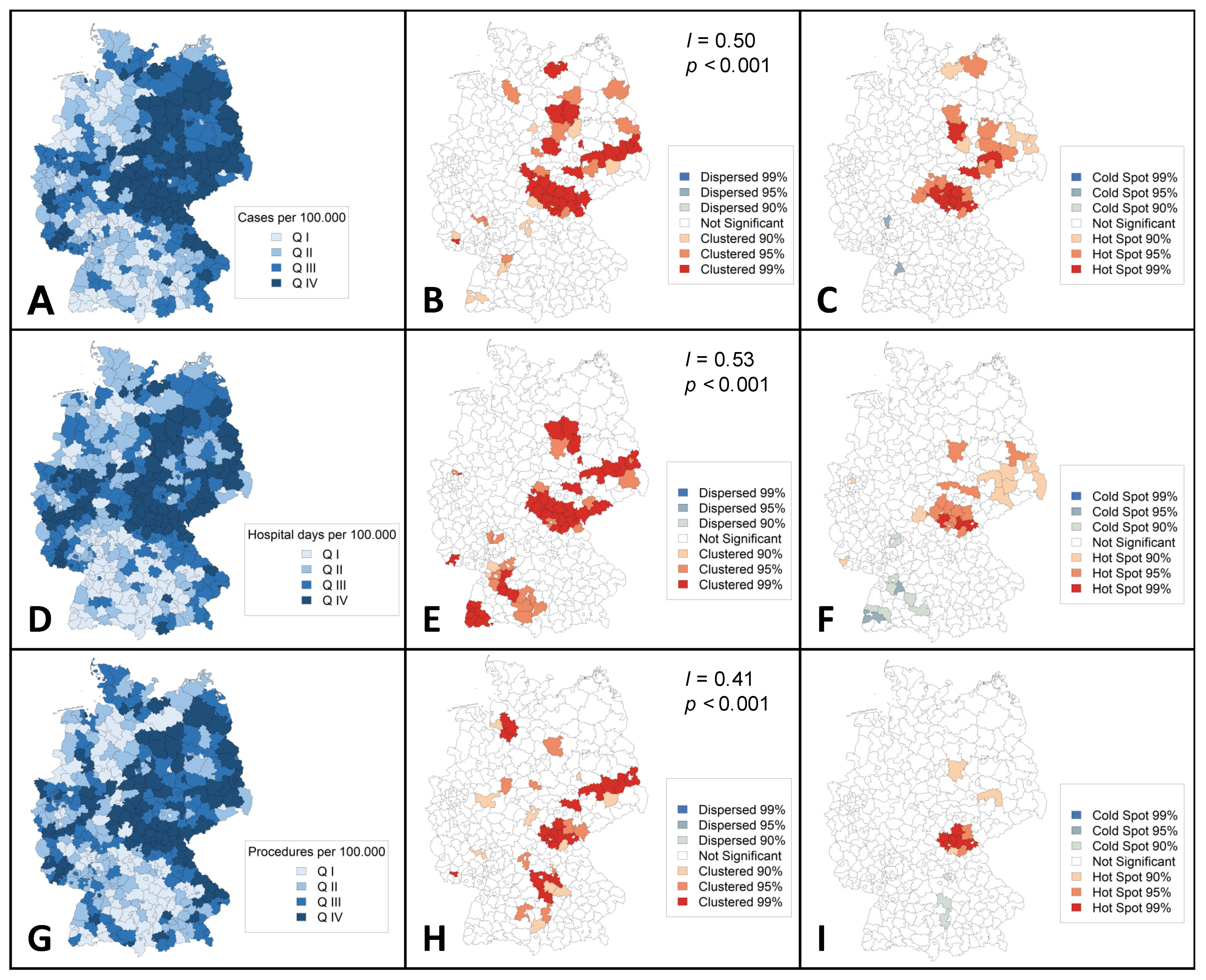
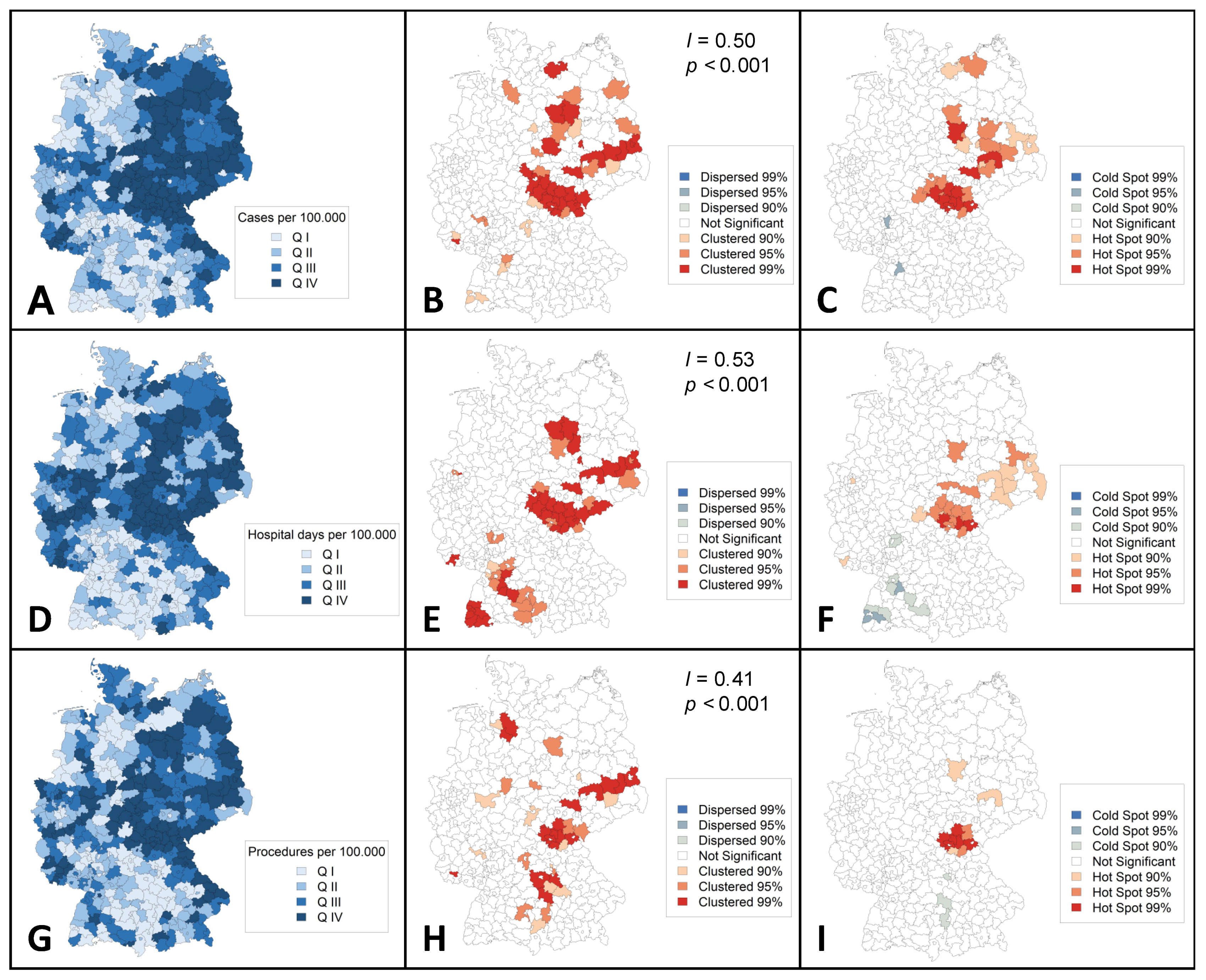
3.5. Regional Distribution of Cases, Hospital Utilization, and Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Nehler, M.R.; Duval, S.; Diao, L.; Annex, B.H.; Hiatt, W.R.; Rogers, K.; Zakharyan, A.; Hirsch, A.T. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J. Vasc. Surg. 2014, 60, 686–695 e682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinecke, H.; Unrath, M.; Freisinger, E.; Bunzemeier, H.; Meyborg, M.; Luders, F.; Gebauer, K.; Roeder, N.; Berger, K.; Malyar, N.M. Peripheral arterial disease and critical limb ischaemia: Still poor outcomes and lack of guideline adherence. Eur. Heart J. 2015, 36, 932–938. [Google Scholar] [CrossRef] [Green Version]
- Kotov, A.; Peters, F.; Debus, E.S.; Zeller, T.; Heider, P.; Stavroulakis, K.; Remig, J.; Gussmann, A.; Hoffmann, J.; Friedrich, O.; et al. The prospective GermanVasc cohort study. Vasa 2021, 50, 446–452. [Google Scholar] [CrossRef]
- Scully, R.E.; Arnaoutakis, D.J.; DeBord Smith, A.; Semel, M.; Nguyen, L.L. Estimated annual health care expenditures in individuals with peripheral arterial disease. J. Vasc. Surg. 2018, 67, 558–567. [Google Scholar] [CrossRef]
- Kreutzburg, T.; Peters, F.; Riess, H.C.; Hischke, S.; Marschall, U.; Kriston, L.; L’Hoest, H.; Sedrakyan, A.; Debus, E.S.; Behrendt, C.A. Editor’s Choice—Comorbidity Patterns Among Patients with Peripheral Arterial Occlusive Disease in Germany: A Trend Analysis of Health Insurance Claims Data. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Mustapha, J.A.; Katzen, B.T.; Neville, R.F.; Lookstein, R.A.; Zeller, T.; Miller, L.E.; Jaff, M.R. Determinants of Long-Term Outcomes and Costs in the Management of Critical Limb Ischemia: A Population-Based Cohort Study. J. Am. Heart Assoc. 2018, 7, e009724. [Google Scholar] [CrossRef]
- Callum, K.; Bradbury, A. ABC of arterial and venous disease: Acute limb ischaemia. BMJ 2000, 320, 764–767. [Google Scholar] [CrossRef] [Green Version]
- Bjorck, M.; Earnshaw, J.J.; Acosta, S.; Bastos Goncalves, F.; Cochennec, F.; Debus, E.S.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.W.; Menyhei, G.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [Google Scholar] [CrossRef] [Green Version]
- Kulezic, A.; Acosta, S. Epidemiology and Prognostic Factors in Acute Lower Limb Ischaemia: A Population Based Study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Kuhnl, A.; Erk, A.; Trenner, M.; Salvermoser, M.; Schmid, V.; Eckstein, H.H. Incidence, Treatment and Mortality in Patients with Abdominal Aortic Aneurysms. Dtsch. Arztebl. Int. 2017, 114, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krautz, C.; Nimptsch, U.; Weber, G.F.; Mansky, T.; Grutzmann, R. Effect of Hospital Volume on In-hospital Morbidity and Mortality Following Pancreatic Surgery in Germany. Ann. Surg. 2018, 267, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Nimptsch, U.; Krautz, C.; Weber, G.F.; Mansky, T.; Grutzmann, R. Nationwide In-hospital Mortality Following Pancreatic Surgery in Germany is Higher than Anticipated. Ann. Surg. 2016, 264, 1082–1090. [Google Scholar] [CrossRef]
- Nimptsch, U.; Mansky, T. Trends in acute inpatient stroke care in Germany--an observational study using administrative hospital data from 2005-2010. Dtsch. Arztebl. Int. 2012, 109, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Trenner, M.; Kuehnl, A.; Reutersberg, B.; Salvermoser, M.; Eckstein, H.H. Nationwide analysis of risk factors for in-hospital mortality in patients undergoing abdominal aortic aneurysm repair. Br. J. Surg. 2018, 105, 379–387. [Google Scholar] [CrossRef]
- Swart, E.; Gothe, H.; Geyer, S.; Jaunzeme, J.; Maier, B.; Grobe, T.G.; Ihle, P. Good Practice of Secondary Data Analysis (GPS): Guidelines and recommendations. Gesundheitswesen 2015, 77, 120–126. [Google Scholar]
- Swart, E.; Bitzer, E.M.; Gothe, H.; Harling, M.; Hoffmann, F.; Horenkamp-Sonntag, D.; Maier, B.; March, S.; Petzold, T.; Rohrig, R.; et al. A Consensus German Reporting Standard for Secondary Data Analyses, Version 2 (STROSA-STandardisierte BerichtsROutine fur SekundardatenAnalysen). Gesundheitswesen 2016, 78, e161. [Google Scholar] [CrossRef] [Green Version]
- Getis, A.; Ord, J.K. The Analysis of Spatial Association by Use of Distance Statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Ord, J.K.; Getis, A. Local Spatial Autocorrelation Statistics: Distributional Issues and an Application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Casagrande, S.; Geiss, L.; Cowie, C.C. Prevalence of and Trends in Diabetes Among Adults in the United States, 1988–2012. JAMA 2015, 314, 1021–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrendt, C.A.; Sigvant, B.; Szeberin, Z.; Beiles, B.; Eldrup, N.; Thomson, I.A.; Venermo, M.; Altreuther, M.; Menyhei, G.; Nordanstig, J.; et al. International Variations in Amputation Practice: A VASCUNET Report. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 391–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuehnl, A.; Salvermoser, M.; Erk, A.; Trenner, M.; Schmid, V.; Eckstein, H.H. Spatial Analysis of Hospital Incidence and in Hospital Mortality of Abdominal Aortic Aneurysms in Germany: Secondary Data Analysis of Nationwide Hospital Episode (DRG) Data. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 852–859. [Google Scholar] [CrossRef] [Green Version]
- Kuhnl, A.S.M.; Knipfer, E.; Zimmermann, A.; Schmid, V.; Eckstein, H.H. Regional frequency variation of revascularization procedures for carotid stenosis in Germany. Secondary data analysis of DRG data from 2012 to 2014. Gefasschirurgie: Zeitschrift fur vaskulare und endovaskulare Chirurgie: Organ der Deutschen und der Osterreichischen Gesellschaft fur Gefasschirurgie unter Mitarbeit der Schweizerischen Gesellschaft fur Gefasschirurgie. Gefässchirurgie 2018, 23, 519–528. [Google Scholar] [CrossRef]
- Deutsche Herzstiftung. Deutscher Herzbericht 2020. Available online: https://www.herzstiftung.de/system/files/2021-06/Deutscher-Herzbericht-2020.pdf (accessed on 10 March 2022).
- Dornquast, C.; Kroll, L.E.; Neuhauser, H.K.; Willich, S.N.; Reinhold, T.; Busch, M.A. Regional Differences in the Prevalence of Cardiovascular Disease. Dtsch. Arztebl. Int. 2016, 113, 704–711. [Google Scholar] [CrossRef] [Green Version]
- Kotz, D.; Bockmann, M.; Kastaun, S. The Use of Tobacco, E-Cigarettes, and Methods to Quit Smoking in Germany. Dtsch. Arztebl. Int. 2018, 115, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Hans Böckler Stiftung. WSI Verteilungsmonitor—Verfügbare Pro-Kopf-Einkommen, Regional. Available online: https://www.boeckler.de/pdf/wsi_vm_verfuegbare_einkommen.pdf (accessed on 10 March 2022).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peripheral Arterial Disease or Arterial Embolism or Thrombosis | |||
|---|---|---|---|
| As MD/SD with Specific Interventional/Surgical Therapy n = 2,110,925 | As MD without Specific Interventional/Surgical Therapy n = 478,586 | Total n = 2,589,511 | |
| Age in years (median, Q1–Q3) | 72 (63–79) | 75 (66–83) | 72 (63–80) |
| Male sex | 1,363,772 (65) | 272,242 (57) | 1,636,014 (63) |
| Elixhauser Score (median, Q1–Q3) | 5 (0–10) | 5 (0–11) | 5 (0–10) |
| Comorbidities | |||
| Hypertension | 1,509,994 (72) | 326,668 (68) | 1,836,662 (71) |
| Diabetes mellitus | 652,631 (31) | 155,785 (33) | 808,416 (31) |
| Renal disease | 596,071 (28) | 143,048 (30) | 739,119 (29) |
| Chronic ischemic heart disease | 604,810 (29) | 131,969 (28) | 736,779 (29) |
| Chronic pulmonary disease | 229,536 (11) | 54,700 (11) | 284,236 (11) |
| Aortic Aneurysm | 28,479 (1.4) | 8179 (1.7) | 36,658 (1.4) |
| Distance from residency to hospital | |||
| Linear distance in km (median, Q1–Q3) | 9.64 (4.2–19.2) | 8.81 (3.7–17.4) | 9.47 (4.1–18.8) |
| Treating Department | |||
| Vascular Surgery | 655,086 (31) | 114,249 (24) | 769,335 (30) |
| General Surgery | 838,201 (40) | 177,838 (37) | 1,016,039 (39) |
| Cardiology and Angiology | 156,151 (7.4) | 27,645 (5.8) | 183,796 (7.1) |
| Internal medicine | 299,850 (14) | 93,555 (20) | 393,405 (15) |
| Other | 295,255 (14) | 85,089 (18) | 380,344 (15) |
| Outcomes | |||
| Length of stay in days (median, Q1–Q3) | 9 (3–18) | 6 (2–12) | 8 (3–17) |
| Annual sum of days in hospital (Q1–Q3) | 6838 (4388–9540) | 5690 (2767–8805) | 6632 (4144–9421) |
| Minor amputation | 302,724 (14) | - | 302,724 (14) |
| Major amputation | 146,749 (7.0) | - | 146,749 (7.0) |
| In-hospital mortality | 84,894 (4.0) | 22,303 (4.7) | 107,197 (4.1) |
| Main Diagnosis | Fontaine Stage | Arterial Embolism/Thrombosis | Other | |||
|---|---|---|---|---|---|---|
| I/IIa | IIb | III | IV | |||
| n = 38,766 | n = 712,306 | n = 178,608 | n = 503,873 | n = 141,160 | n = 536,212 | |
| Age in years (median, Q1–Q3) | 68 (60–75) | 68 (60–75) | 71 (62–79) | 76 (68–83) | 74 (63–83) | 72 (64–79) |
| Male sex | 27,019 (70) | 479,908 (67) | 105,804 (59) | 313,052 (62) | 70,840 (50) | 367,149 (69) |
| Elixhauser Score (median, Q1–Q3) | 0 (0–5) | 0 (0–5) | 3 (0–8) | 7 (2–13) | 7 (2–13) | 7 (2–14) |
| Comorbidities | ||||||
| Chronic ischemic heart disease | 9166 (24) | 178,289 (25) | 51,078 (29) | 151,943 (30) | 32,731 (23) | 181,603 (34) |
| Hypertension | 26,589 (69) | 511,423 (72) | 129,352 (72) | 361,501 (72) | 92,389 (66) | 388,740 (73) |
| Chronic pulmonary disease | 2717 (7.0) | 67,720 (9.5) | 23,689 (13) | 60,150 (12) | 14,371 (10) | 60,889 (11) |
| Diabetes mellitus | 9820 (25) | 189,046 (27) | 52,480 (29) | 225,326 (45) | 36,813 (26) | 139,146 (26) |
| Renal disease | 5552 (14) | 113,884 (16) | 44,097 (25) | 196,752 (39) | 34,778 (25) | 201,008 (38) |
| Aortic Aneurysm | 453 (1.2) | 9373 (1.3) | 2806 (1.6) | 5231 (1.04) | 2653 (1.9) | 7963 (1.5) |
| Distance from residency to hospital | ||||||
| Linear distance in km (median, Q1–Q3) | 11.05 (4.9–22.0) | 9.88 (4.4–19.8) | 9.31 (4.1–18.8) | 9.38 (4.1–18.3) | 9.43 (4.1–19.0) | 9.59 (4.1–19.2) |
| Treating Department | ||||||
| Vascular surgery | 7958 (21) | 223,801 (31) | 59,956 (34) | 167,340 (33) | 49,528 (35) | 146,503 (27) |
| General surgery | 11,375 (29) | 237,547 (33) | 70,003 (39) | 225,302 (45) | 61,867 (44) | 232,107 (43) |
| Cardiology or Angiology | 6430 (17) | 68,629 (9.6) | 13,560 (7.6) | 26,495 (5.3) | 6858 (4.9) | 34,179 (6.4) |
| General internal medicine | 6074 (16) | 97,597 (14) | 22,383 (13) | 60,523 (12) | 15,936 (11) | 97,337 (18) |
| Others | 7420 (19) | 97,406 (14) | 21,757 (12) | 64,252 (13) | 19,143 (14) | 85,277 (16) |
| Outcomes | ||||||
| Length of stay in days (median, Q1–Q3) | 2 (1–4) | 3 (2–8) | 8 (4–15) | 14 (8–25) | 9 (6–16) | 15 (8–28) |
| Minor amputation | 203 (0.52) | 482 (0.07) | 873 (0.49) | 141,169 (28) | 2379 (1.7) | 157,618 (29) |
| Major amputation | 133 (0.34) | 518 (0.07) | 3812 (2.1) | 72,958 (15) | 9363 (6.6) | 59,965 (11) |
| In-hospital mortality | 150 (0.39) | 1690 (0.24) | 3687 (2.1) | 29,121 (5.8) | 14,297 (10) | 35,949 (6.7) |
| Main Diagnosis | Fontaine Stage | Arterial Embolism/Thrombosis | Other | |||
|---|---|---|---|---|---|---|
| I/IIa | IIb | III | IV | |||
| n = 38,766 | n = 712,306 | n = 178,608 | n = 503,873 | n = 141,160 | n = 536,212 | |
| Endovascular Procedures | ||||||
| Balloon Angioplasty | ||||||
| Aorta and iliac | 118 (0.30) | 3006 (0.42) | 467 (0.26) | 492 (0.10) | 659 (0.47) | 2617 (0.49) |
| Vascular Graft | 196 (0.51) | 2852 (0.4) | 1432 (0.8) | 2331 (0.46) | 946 (0.67) | 5925 (1.1) |
| Above knee | 28,590 (74) | 451,601 (63) | 78,971 (44) | 174,250 (35) | 29,009 (21) | 141,425 (26) |
| Below knee | 4869 (13) | 70,571 (9.9) | 29,625 (17) | 146,890 (29) | 15,614 (11) | 107,990 (20) |
| Stent Angioplasty | ||||||
| Aorta and iliac | 94 (0.24) | 2092 (0.29) | 339 (0.19) | 364 (0.07) | 485 (0.34) | 1440 (0.27) |
| Vascular Graft | 36 (0.09) | 546 (0.08) | 361 (0.20) | 405 (0.08) | 282 (0.20) | 1050 (0.20) |
| Above knee | 17,027 (44) | 274,732 (39) | 45,053 (25) | 80,506 (16) | 16,155 (11) | 66,768 (13) |
| Below knee | 838 (2.2) | 10,349 (1.5) | 4418 (2.5) | 16,409 (3.3) | 2785 (2.0) | 10,342 (1.9) |
| Open Surgical Procedures | ||||||
| Endarterectomy | ||||||
| Aorta and iliac | 1260 (3.3) | 49,815 (7.0) | 15,698 (8.8) | 22,912 (4.6) | 8107 (5.7) | 23,487 (4.4) |
| Above knee | 4010 (10) | 147,251 (21) | 50,291 (28) | 84,075 (17) | 39,324 (28) | 93,037 (17) |
| Below knee | 75 (0.19) | 2284 (0.32) | 4185 (2.3) | 8612 (1.71) | 4708 (3.3) | 9114 (1.7) |
| Bypass (distal anastomosis) | ||||||
| Iliac | 33 (0.09) | 1574 (0.22) | 427 (0.24) | 297 (0.06) | 469 (0.33) | 1349 (0.25) |
| Femoral | 585 (1.5) | 25,813 (3.6) | 13,151 (7.4) | 15,358 (3.1) | 7050 (5.0) | 20,686 (3.9) |
| Popliteal above knee | 781 (2.0) | 39,203 (5.5) | 10,188 (5.7) | 23,355 (4.6) | 2180 (1.5) | 13,764 (2.6) |
| Popliteal below knee | 276 (0.71) | 12,854 (1.8) | 10,612 (5.9) | 24,688 (4.9) | 3629 (2.6) | 16,758 (3.1) |
| Popliteal unspecified | 89 (0.23) | 3324 (0.47) | 1354 (0.76) | 2900 (0.58) | 436 (0.31) | 2089 (0.39) |
| Crural | 186 (0.48) | 5260 (0.74) | 12,458 (7.0) | 35,562 (7.1) | 4658 (3.3) | 22,128 (4.1) |
| Pedal | 10 (0.03) | 87 (0.01) | 486 (0.3) | 5289 (1.1) | 310 (0.22) | 3988 (0.74) |
| Major Amputation | ||||||
| Above knee and knee exarticulation | 101 (0.26) | 403 (0.06) | 3017 (1.7) | 50,862 (10) | 7687 (5.5) | 35,539 (6.6) |
| Below knee | 36 (0.09) | 151 (0.02) | 1080 (0.60) | 26,063 (5.2) | 2206 (1.6) | 27,754 (5.2) |
| Unspecified | 1 (0.00) | 6 (0.00) | 268 (0.05) | 16 (0.01) | 278 (0.05) | |
| Minor Amputation | ||||||
| Forefoot and midfoot | 40 (0.10) | 88 (0.01) | 278 (0.16) | 38,816 (7.7) | 902 (0.64) | 45,043 (8.4) |
| Toes | 164 (0.42) | 394 (0.06) | 635 (0.36) | 111,483 (22) | 1580 (1.1) | 121,216 (23) |
| Unspecified | 8 (0.02) | 11 (0.00) | 18 (0.01) | 2705 (0.54) | 48 (0.03) | 3679 (0.69) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trenner, M.; Knappich, C.; Bohmann, B.; Heuberger, S.; Eckstein, H.-H.; Kuehnl, A. Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data. J. Clin. Med. 2022, 11, 2116. https://doi.org/10.3390/jcm11082116
Trenner M, Knappich C, Bohmann B, Heuberger S, Eckstein H-H, Kuehnl A. Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data. Journal of Clinical Medicine. 2022; 11(8):2116. https://doi.org/10.3390/jcm11082116
Chicago/Turabian StyleTrenner, Matthias, Christoph Knappich, Bianca Bohmann, Simon Heuberger, Hans-Henning Eckstein, and Andreas Kuehnl. 2022. "Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data" Journal of Clinical Medicine 11, no. 8: 2116. https://doi.org/10.3390/jcm11082116
APA StyleTrenner, M., Knappich, C., Bohmann, B., Heuberger, S., Eckstein, H.-H., & Kuehnl, A. (2022). Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data. Journal of Clinical Medicine, 11(8), 2116. https://doi.org/10.3390/jcm11082116