

Association between SGLT2 Inhibitors and Cardiac Rehabilitation Outcomes in Patients with Cardiovascular Disease and Type 2 Diabetes Mellitus
 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. SGLT2 Inhibitors
2.3. Physical Function
2.4. Endpoints
2.5. Cardiac Rehabilitation Program
2.6. Statistical Analysis
3. Results
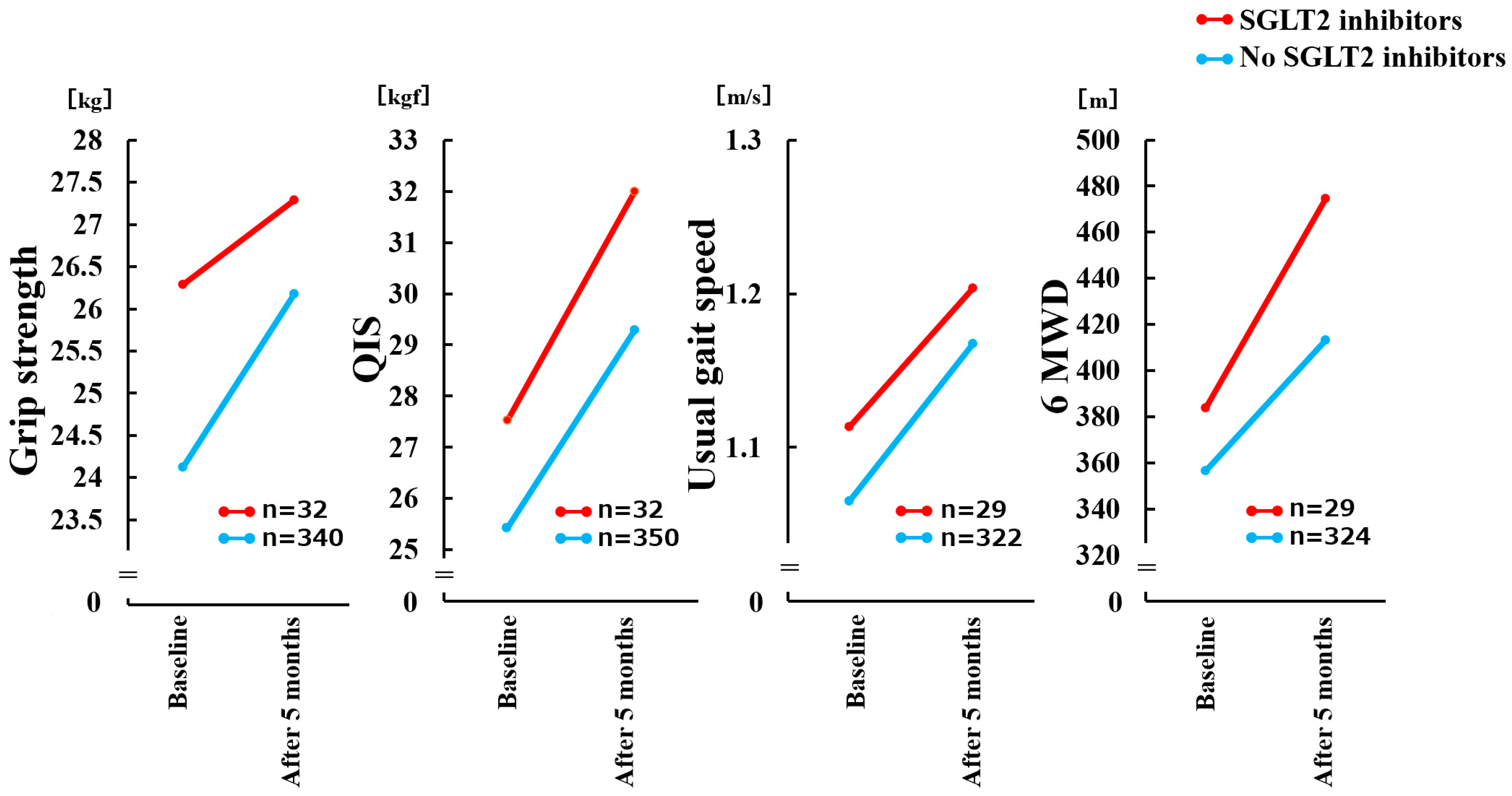
3.1. Association between SGLT2 Inhibitor Use and Change in Physical Function
3.2. Association between SGLT2 Inhibitor Use and Change in Body Weight
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 1, Cd003331. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.C., Jr.; Benjamin, E.J.; Bonow, R.O.; Braun, L.T.; Creager, M.A.; Franklin, B.A.; Gibbons, R.J.; Grundy, S.M.; Hiratzka, L.F.; Jones, D.W.; et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: A guideline from the American Heart Association and American College of Cardiology Foundation. Circulation 2011, 124, 2458–2473. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Gliflozins in the Management of Cardiovascular Disease. N. Engl. J. Med. 2022, 386, 2024–2034. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; DeMets, D.L.; Inzucchi, S.E.; Kober, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Bengtsson, O.; Ponikowski, P.; Sabatine, M.S.; et al. A trial to evaluate the effect of the sodium-glucose co-transporter 2 inhibitor dapagliflozin on morbidity and mortality in patients with heart failure and reduced left ventricular ejection fraction (DAPA-HF). Eur. J. Heart Fail 2019, 21, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Fitchett, D.; Inzucchi, S.E.; Cannon, C.P.; McGuire, D.K.; Scirica, B.M.; Johansen, O.E.; Sambevski, S.; Kaspers, S.; Pfarr, E.; George, J.T.; et al. Empagliflozin Reduced Mortality and Hospitalization for Heart Failure Across the Spectrum of Cardiovascular Risk in the EMPA-REG OUTCOME Trial. Circulation 2019, 139, 1384–1395. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Cefalu, W.T.; Leiter, L.A.; Yoon, K.H.; Arias, P.; Niskanen, L.; Xie, J.; Balis, D.A.; Canovatchel, W.; Meininger, G. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet 2013, 382, 941–950. [Google Scholar] [CrossRef]
- Koike, Y.; Shirabe, S.I.; Maeda, H.; Yoshimoto, A.; Arai, K.; Kumakura, A.; Hirao, K.; Terauchi, Y. Effect of canagliflozin on the overall clinical state including insulin resistance in Japanese patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2019, 149, 140–146. [Google Scholar] [CrossRef]
- Sasaki, T.; Sugawara, M.; Fukuda, M. Sodium-glucose cotransporter 2 inhibitor-induced changes in body composition and simultaneous changes in metabolic profile: 52-week prospective LIGHT (Luseogliflozin: The Components of Weight Loss in Japanese Patients with Type 2 Diabetes Mellitus) Study. J. Diabetes Investig. 2019, 10, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, H.; Yokomizo, H.; Nakamura, S.; Izumi, Y.; Takahashi, M.; Obara, S.; Nakao, M.; Ikeda, Y.; Sato, N.; Sakamoto, R.; et al. Differential effect of canagliflozin, a sodium-glucose cotransporter 2 (SGLT2) inhibitor, on slow and fast skeletal muscles from nondiabetic mice. Biochem. J. 2022, 479, 425–444. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Ito, S.; Uemura, O.; Kato, T.; Kimura, G.; Nakao, T.; Hattori, M.; Fukagawa, M.; Horio, M.; Mitarai, T.; et al. CKD Clinical Practice Guidebook. The essence of treatment for CKD patients. Clin. Exp. Nephrol. 2009, 13, 191–248. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Maekawa, E.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; Masuda, T.; et al. Incremental Value of Objective Frailty Assessment to Predict Mortality in Elderly Patients Hospitalized for Heart Failure. J. Card. Fail 2018, 24, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Masuda, T.; Tanaka, S.; Hamazaki, N.; Matsue, Y.; Mezzani, A.; Matsuzawa, R.; Nozaki, K.; Maekawa, E.; Noda, C.; et al. Quadriceps Strength as a Predictor of Mortality in Coronary Artery Disease. Am. J. Med. 2015, 128, 1212–1219. [Google Scholar] [CrossRef]
- Ueno, K.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Uchida, S.; Noda, T.; Maekawa, E.; Yamaoka-Tojo, M.; et al. Usefulness of measuring maximal gait speed in conjunction with usual gait speed for risk stratification in patients with cardiovascular disease. Exp. Gerontol. 2022, 164, 111810. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Izawa, H.; Yoshida, T.; Ikegame, T.; Izawa, K.P.; Ito, Y.; Okamura, H.; Osada, N.; Kinugawa, S.; Kubozono, T.; Kono, Y.; et al. Standard Cardiac Rehabilitation Program for Heart Failure. Circ. J. 2019, 83, 2394–2398. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Murray, E.M.; Whellan, D.J.; Chen, H.; Bertoni, A.G.; Duncan, P.; Pastva, A.M.; Kitzman, D.W.; Mentz, R.J. Physical Rehabilitation in Older Patients Hospitalized with Acute Heart Failure and Diabetes: Insights from REHAB-HF. Am. J. Med. 2022, 135, 82–90. [Google Scholar] [CrossRef]
- Santos-Gallego, C.G.; Vargas-Delgado, A.P.; Requena-Ibanez, J.A.; Garcia-Ropero, A.; Mancini, D.; Pinney, S.; Macaluso, F.; Sartori, S.; Roque, M.; Sabatel-Perez, F.; et al. Randomized Trial of Empagliflozin in Nondiabetic Patients With Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2021, 77, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Nassif, M.E.; Windsor, S.L.; Borlaug, B.A.; Kitzman, D.W.; Shah, S.J.; Tang, F.; Khariton, Y.; Malik, A.O.; Khumri, T.; Umpierrez, G.; et al. The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: A multicenter randomized trial. Nat. Med. 2021, 27, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Petrie, M.C.; Verma, S.; Docherty, K.F.; Inzucchi, S.E.; Anand, I.; Belohlavek, J.; Bohm, M.; Chiang, C.E.; Chopra, V.K.; de Boer, R.A.; et al. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA 2020, 323, 1353–1368. [Google Scholar] [CrossRef] [PubMed]
- Post, A.; Groothof, D.; Eisenga, M.F.; Bakker, S.J.L. Sodium-Glucose Cotransporter 2 Inhibitors and Kidney Outcomes: True Renoprotection, Loss of Muscle Mass or Both? J. Clin. Med. 2020, 9, 1603. [Google Scholar] [CrossRef] [PubMed]
- Bolinder, J.; Ljunggren, Ö.; Kullberg, J.; Johansson, L.; Wilding, J.; Langkilde, A.M.; Sugg, J.; Parikh, S. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J. Clin. Endocrinol. Metab. 2012, 97, 1020–1031. [Google Scholar] [CrossRef]
- Nambu, H.; Takada, S.; Fukushima, A.; Matsumoto, J.; Kakutani, N.; Maekawa, S.; Shirakawa, R.; Nakano, I.; Furihata, T.; Katayama, T.; et al. Empagliflozin restores lowered exercise endurance capacity via the activation of skeletal muscle fatty acid oxidation in a murine model of heart failure. Eur. J. Pharmacol. 2020, 866, 172810. [Google Scholar] [CrossRef]
- Bamba, R.; Okamura, T.; Hashimoto, Y.; Majima, S.; Senmaru, T.; Ushigome, E.; Nakanishi, N.; Asano, M.; Yamazaki, M.; Takakuwa, H.; et al. Extracellular lipidome change by an SGLT2 inhibitor, luseogliflozin, contributes to prevent skeletal muscle atrophy in db/db mice. J. Cachexia Sarcopenia Muscle 2022, 13, 574–588. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker For Older Adults. Clin. Interv. Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Maekawa, E.; Reed, J.L.; Noda, C.; et al. Quadriceps Strength and Mortality in Older Patients With Heart Failure. Can. J. Cardiol. 2021, 37, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Mezzani, A.; Hotta, K.; Shimizu, R.; Kamekawa, D.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; Masuda, T. Quadriceps isometric strength as a predictor of exercise capacity in coronary artery disease patients. Eur. J. Prev. Cardiol. 2014, 21, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Hamazaki, N.; Matsue, Y.; Mezzani, A.; Corrà, U.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Maekawa, E.; Noda, C.; et al. Gait speed has comparable prognostic capability to six-minute walk distance in older patients with cardiovascular disease. Eur. J. Prev. Cardiol. 2018, 25, 212–219. [Google Scholar] [CrossRef]
- Tabata, M.; Shimizu, R.; Kamekawa, D.; Kato, M.; Kamiya, K.; Akiyama, A.; Kamada, Y.; Tanaka, S.; Noda, C.; Masuda, T. Six-minute walk distance is an independent predictor of hospital readmission in patients with chronic heart failure. Int. Heart J. 2014, 55, 331–336. [Google Scholar] [CrossRef]
- Sato, A.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Uchida, S.; Maekawa, E.; Yamaoka-Tojo, M.; Matsunaga, A.; et al. Gait speed and 6-minute walking distance are useful for identifying difficulties in activities of daily living in patients with cardiovascular disease. Heart Lung 2022, 51, 46–51. [Google Scholar] [CrossRef]
- Linden, M.A.; Ross, T.T.; Beebe, D.A.; Gorgoglione, M.F.; Hamilton, K.L.; Miller, B.F.; Braun, B.; Esler, W.P. The combination of exercise training and sodium-glucose cotransporter-2 inhibition improves glucose tolerance and exercise capacity in a rodent model of type 2 diabetes. Metabolism 2019, 97, 68–80. [Google Scholar] [CrossRef]
- Saeidi, M.; Mostafavi, S.; Heidari, H.; Masoudi, S. Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. ARYA Atheroscler. 2013, 9, 179–185. [Google Scholar] [CrossRef]
- Paneroni, M.; Scalvini, S.; Corrà, U.; Lovagnini, M.; Maestri, R.; Mazza, A.; Raimondo, R.; Agostoni, P.; La Rovere, M.T. The Impact of Cardiac Rehabilitation on Activities of Daily Life in Elderly Patients With Heart Failure. Front. Physiol. 2021, 12, 785501. [Google Scholar] [CrossRef]
- Adachi, T.; Iritani, N.; Kamiya, K.; Iwatsu, K.; Kamisaka, K.; Iida, Y.; Yamada, S. Prognostic Effects of Cardiac Rehabilitation in Patients With Heart Failure (from a Multicenter Prospective Cohort Study). Am. J. Cardiol. 2022, 164, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Uchida, S.; Kamiya, K.; Hamazaki, N.; Nozaki, K.; Ichikawa, T.; Nakamura, T.; Yamashita, M.; Maekawa, E.; Reed, J.L.; Yamaoka-Tojo, M.; et al. Prognostic utility of dynapenia in patients with cardiovascular disease. Clin. Nutr. 2021, 40, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Slomski, A. Dapagliflozin Safe and Effective for Heart Failure with Frailty. JAMA 2022, 327, 1950. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Overall | SGLT2 Inhibitors | Non SGLT2 Inhibitors | p-Value |
|---|---|---|---|---|
| n = 402 | n = 32 | n = 370 | ||
| Age [years] | 69 [60–76] | 64 [52–68] | 69 [61–76] | 0.002 |
| Older (≥65), n (%) | 262 (65.2) | 14 (43.8) | 248 (67.0) | 0.011 |
| Males, n (%) | 274 (68.2) | 21 (65.6) | 253 (68.4) | 0.843 |
| body weight [kg] | 59.2 [50.3–67.7] | 60.7 [50.9–69.5] | 59.2 [50.1–67.4] | 0.525 |
| BMI [kg/m2] | 22.6 [20.2–25.1] | 23.2 [20.1–25.8] | 22.6 [20.2–25.0] | 0.569 |
| LVEF [%] | 54.2 [42.7–64.5] | 42.0 [29.0–58.8] | 55.0 [44.0–65.0] | 0.009 |
| The total number of outpatient CR [times] | 4.0 [3.0–8.0] | 3.0 [2.0–6.5] | 4.5 [3.0–8.0] | 0.059 |
| Diagnosis, n (%) | ||||
| ACS | 128 (31.8) | 12 (37.5) | 116 (31.4) | 0.553 |
| HF | 123 (30.6) | 16 (50.0) | 107 (28.9) | 0.017 |
| Others | 151 (37.6) | 4 (12.5) | 147 (39.7) | 0.002 |
| History of HF hospitalization, n (%) | 74 (18.4) | 6 (18.8) | 68 (18.4) | 1.000 |
| History of AMI, n (%) | 70 (17.4) | 2 (6.2) | 68 (18.4) | 0.09 |
| Hb [g/dL] | 12.3 [10.6–14.0] | 14.2 [12.5–15.4] | 12.2 [10.5–13.7] | <0.001 |
| BNP [pg/mL] | 177 [62–512] | 268 [79–741] | 176 [58–476] | 0.221 |
| eGFR [mL/min/1.73 m2] | 57 [39–71] | 60 [48–74] | 57 [38–71] | 0.285 |
| Baseline Physical function | ||||
| grip strength [kg] | 23.4 [16.1–30.7] | 27.8 [19.0–31.0] | 22.9 [16.1–30.5] | 0.143 |
| QIS [kgf] | 23.8 [15.5–33.5] | 27.1 [16.9–35.7] | 23.6 [15.5–33.2] | 0.321 |
| usual gait speed [m/s] | 1.10 [0.91–1.26] | 1.15 [0.98–1.34] | 1.08 [0.90–1.26] | 0.334 |
| 6 MWD [m] | 422 [310–498] | 440 [360–500] | 418 [308–495] | 0.476 |
| Medications, n (%) | ||||
| ACE Inhibitor | 159 (39.6) | 18 (56.2) | 141 (38.1) | 0.058 |
| ARB | 182 (45.3) | 11 (34.4) | 171 (46.2) | 0.267 |
| Beta-Blocker | 310 (77.1) | 28 (87.5) | 282 (76.2) | 0.189 |
| Variables | Δ Grip Strength | Δ QIS | Δ Usual Gait Speed | Δ 6 MWD | ||||
|---|---|---|---|---|---|---|---|---|
| β | p-Value | β | p-Value | β | p-Value | β | p-Value | |
| SGLT2 inhibitors use | 0.148 | 0.061 | 0.018 | 0.830 | 0.129 | 0.161 | 0.020 | 0.822 |
| Age | −0.416 | <0.001 | −0.359 | <0.001 | −0.225 | 0.023 | −0.460 | <0.001 |
| Male | −0.409 | <0.001 | −0.238 | 0.007 | 0.062 | 0.497 | −0.042 | 0.626 |
| BMI | 0.168 | 0.021 | 0.122 | 0.131 | 0.059 | 0.466 | −0.042 | 0.594 |
| NYHA class ≥ III | −0.055 | 0.463 | −0.077 | 0.312 | −0.057 | 0.503 | −0.043 | 0.602 |
| LVEF | −0.096 | 0.231 | 0.063 | 0.457 | −0.111 | 0.252 | 0.035 | 0.699 |
| HF | 0.082 | 0.271 | 0.017 | 0.832 | 0.156 | 0.079 | 0.112 | 0.186 |
| Hb | 0.045 | 0.604 | 0.261 | 0.004 | 0.084 | 0.413 | 0.098 | 0.317 |
| Year of hospitalization (≥2014) | −0.118 | 0.106 | −0.042 | 0.587 | −0.051 | 0.548 | −0.163 | 0.048 |
| Baseline each physical function | −0.700 | <0.001 | −0.472 | <0.001 | −0.376 | 0.001 | −0.462 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashima, A.; Kamiya, K.; Hamazaki, N.; Ueno, K.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Uchida, S.; Noda, T.; Hotta, K.; et al. Association between SGLT2 Inhibitors and Cardiac Rehabilitation Outcomes in Patients with Cardiovascular Disease and Type 2 Diabetes Mellitus. J. Clin. Med. 2022, 11, 5956. https://doi.org/10.3390/jcm11195956
Kashima A, Kamiya K, Hamazaki N, Ueno K, Nozaki K, Ichikawa T, Yamashita M, Uchida S, Noda T, Hotta K, et al. Association between SGLT2 Inhibitors and Cardiac Rehabilitation Outcomes in Patients with Cardiovascular Disease and Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2022; 11(19):5956. https://doi.org/10.3390/jcm11195956
Chicago/Turabian StyleKashima, Ayuko, Kentaro Kamiya, Nobuaki Hamazaki, Kensuke Ueno, Kohei Nozaki, Takafumi Ichikawa, Masashi Yamashita, Shota Uchida, Takumi Noda, Kazuki Hotta, and et al. 2022. "Association between SGLT2 Inhibitors and Cardiac Rehabilitation Outcomes in Patients with Cardiovascular Disease and Type 2 Diabetes Mellitus" Journal of Clinical Medicine 11, no. 19: 5956. https://doi.org/10.3390/jcm11195956
APA StyleKashima, A., Kamiya, K., Hamazaki, N., Ueno, K., Nozaki, K., Ichikawa, T., Yamashita, M., Uchida, S., Noda, T., Hotta, K., Maekawa, E., Yamaoka-Tojo, M., Matsunaga, A., & Ako, J. (2022). Association between SGLT2 Inhibitors and Cardiac Rehabilitation Outcomes in Patients with Cardiovascular Disease and Type 2 Diabetes Mellitus. Journal of Clinical Medicine, 11(19), 5956. https://doi.org/10.3390/jcm11195956