
Thrombophilia Impact on Treatment Decisions, Subsequent Venous or Arterial Thrombosis and Pregnancy-Related Morbidity: A Retrospective Single-Center Cohort Study

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Thrombophilia Testing
2.3. Classification of Thrombophilia and Risk Factors
2.4. Follow-Up and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Study Cohort
3.2. Prevalence of Thrombophilia in the Cohort Study
3.3. Impact of Thrombophilia Testing on Treatment Decisions
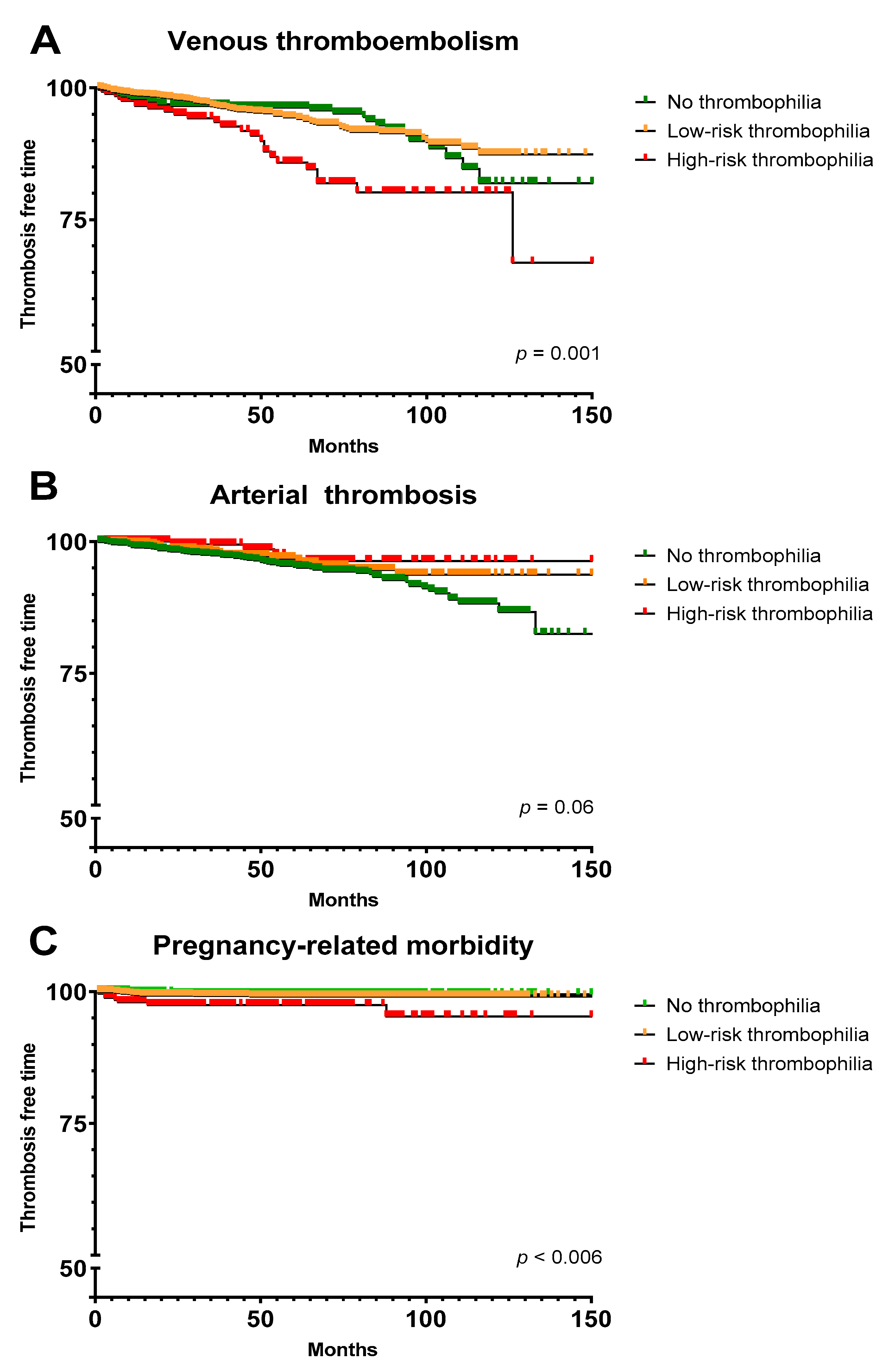
3.4. Association between Thrombophilia and Thromboembolic Events or Pregnancy-Related Morbidity during Follow-Up
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Middeldorp, S. Inherited thrombophilia: A double-edged sword. Hematol. Am. Soc. Hematol. Educ. Program. 2016, 2016, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.M. Thrombophilia Testing and Venous Thrombosis. N. Engl. J. Med. 2017, 377, 1177–1187. [Google Scholar] [CrossRef] [PubMed]
- Ulas, T.; Dal, M.S. Should we screen hereditary thrombophilia testing in patients with provoked/unprovoked venous thromboembolism? Int. J. Cardiol. 2018, 271, 323. [Google Scholar] [CrossRef]
- Khan, F.; Le Gal, G.; Rodger, M.A. The authors respond to “Thrombophilia testing in venous thromboembolism”. CMAJ 2018, 190, E172. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, V.; Rossi, E. Testing for inherited thrombophilia and consequences for antithrombotic prophylaxis in patients with venous thromboembolism and their relatives. A review of the Guidelines from Scientific Societies and Working Groups. Thromb. Haemost. 2013, 110, 697–705. [Google Scholar] [PubMed]
- Gaddh, M.; Cheng, E.; Elsebaie, M.A.; Bodó, I. Clinical Utilization and Cost of Thrombophilia Testing in Patients with Venous Thromboembolism. TH Open 2020, 4, e153–e162. [Google Scholar] [CrossRef]
- Garcia-Horton, A.; Kovacs, M.J.; Abdulrehman, J.; Taylor, J.E.; Sharma, S.; Lazo-Langner, A. Impact of thrombophilia screening on venous thromboembolism management practices. Thromb. Res. 2017, 149, 76–80. [Google Scholar] [CrossRef]
- Reitter-Pfoertner, S.; Waldhoer, T.; Mayerhofer, M.; Eigenbauer, E.; Ay, C.; Mannhalter, C.; Kyrle, P.A.; Pabinger, I. The influence of thrombophilia on the long-term survival of patients with a history of venous thromboembolism. Thromb. Haemost. 2013, 109, 79–84. [Google Scholar] [CrossRef]
- Coppens, M.; Reijnders, J.H.; Middeldorp, S.; Doggen, C.J.M.; Rosendaal, F.R. Testing for inherited thrombophilia does not reduce the recurrence of venous thrombosis. J. Thromb. Haemost. 2008, 6, 1474–1477. [Google Scholar] [CrossRef]
- Lian, T.-Y.; Lu, D.; Yan, X.-X.; Tan, J.-S.; Peng, F.-H.; Zhu, Y.-J.; Wei, Y.-P.; Wu, T.; Sun, K.; Jiang, X.; et al. Association between congenital thrombophilia and outcomes in pulmonary embolism patients. Blood Adv. 2020, 4, 5958–5965. [Google Scholar] [CrossRef]
- Baglin, T.; Luddington, R.; Brown, K.; Baglin, C. Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: Prospective cohort study. Lancet 2003, 362, 523–526. [Google Scholar] [CrossRef]
- Christiansen, S.C.; Cannegieter, S.C.; Koster, T.; Vandenbroucke, J.P.; Rosendaal, F.R. Thrombophilia, Clinical Factors, and Recurrent Venous Thrombotic Events. JAMA 2005, 293, 2352–2361. [Google Scholar] [CrossRef] [PubMed]
- Colucci, G.; Tsakiris, D.A. Thrombophilia screening revisited: An issue of personalized medicine. J. Thromb. Thrombolysis 2020, 49, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, N.; Visweshwar, N.; Jaglal, M.; Sokol, L.; Laber, D. Evolving paradigm in thrombophilia screening. Blood Coagul. Fibrinolysis 2019, 30, 249–252. [Google Scholar] [CrossRef] [PubMed]
- McCormack, T.; Harrisingh, M.C.; Horner, D.; Bewley, S. Venous thromboembolism in adults: Summary of updated NICE guidance on diagnosis, management, and thrombophilia testing. BMJ 2020, 369, m1565. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.M.; Woller, S.C.; Bauer, K.A.; Kasthuri, R.; Cushman, M.; Streiff, M.; Lim, W.; Douketis, J.D. Guidance for the evaluation and treatment of hereditary and acquired thrombophilia. J. Thromb. Thrombolysis 2016, 41, 154–164. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef]
- Kwon, A.J.; Roshal, M.; DeSancho, M.T. Clinical adherence to thrombophilia screening guidelines at a major tertiary care hospital. J. Thromb. Haemost. 2016, 14, 982–986. [Google Scholar] [CrossRef]
- Meyer, M.R.; Witt, D.M.; Delate, T.; Johnson, S.G.; Fang, M.; Go, A.; Clark, N.P. Thrombophilia testing patterns amongst patients with acute venous thromboembolism. Thromb. Res. 2015, 136, 1160–1164. [Google Scholar] [CrossRef][Green Version]
- Virparia, R.; Brunetti, L.; Vigdor, S.; Adams, C.D. Appropriateness of thrombophilia testing in patients in the acute care setting and an evaluation of the associated costs. J. Thromb. Thrombolysis 2019, 49, 108–112. [Google Scholar] [CrossRef]
- Alakbarzade, V.; Taylor, A.; Scully, M.; Simister, R.; Chandratheva, A. Utility of current thrombophilia screening in young patients with stroke and TIA. Stroke Vasc. Neurol. 2018, 3, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.; Jacob, G.P. Thrombophilia testing in pregnancy: Should we agree to disagree? J. Perinat Med. 2015, 43, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Hiedemann, B.; Vernon, E.; Bowie, B.H. Re-Examining Genetic Screening and Oral Contraceptives: A Patient-Centered Review. J. Pers. Med. 2019, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Turrini, M.; Bourgain, C. Appraising screening, making risk in/visible. The medical debate over Non-Rare Thrombophilia (NRT) testing before prescribing the pill. Sociol. Health Illn. 2021, 43, 1627–1642. [Google Scholar] [CrossRef]
- Cohn, D.M.; Middeldorp, S. Early termination of the multicentre randomised clinical trial to evaluate the benefit of testing for thrombophilia following a first venous thromboembolism: The NOSTRADAMUS study. Ned. Tijdschr. Geneeskd. 2008, 152, 2093–2094. [Google Scholar]
- Wilbur, J.; Shian, B. Diagnosis of deep venous thrombosis and pulmonary embolism. Am. Fam. Physician 2012, 86, 913–919. [Google Scholar]
- Hasan, T.F.; Rabinstein, A.A.; Middlebrooks, E.H.; Haranhalli, N.; Silliman, S.L.; Meschia, J.F.; Tawk, R.G. Diagnosis and Management of Acute Ischemic Stroke. Mayo Clin. Proc. 2018, 93, 523–538. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute Myocardial Infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef]
- Firnhaber, J.M.; Powell, C.S. Lower Extremity Peripheral Artery Disease: Diagnosis and Treatment. Am. Fam. Physician 2019, 99, 362–369. [Google Scholar]
- Rajesh, S.; Mukund, A.; Arora, A. Imaging Diagnosis of Splanchnic Venous Thrombosis. Gastroenterol. Res. Pr. 2015, 2015, 1–29. [Google Scholar] [CrossRef]
- Karaosmanoglu, A.D.; Uysal, A.; Akata, D.; Ozmen, M.N.; Karcaaltincaba, M. Role of imaging in visceral vascular emergencies. Insights Imaging 2020, 11, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Ghoneim, A.; Straiton, J.; Pollard, C.; Macdonald, K.; Jampana, R. Imaging of cerebral venous thrombosis. Clin. Radiol. 2020, 75, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Davenport, W.B.; Kutteh, W.H. Inherited thrombophilias and adverse pregnancy outcomes: A review of screening patterns and recommendations. Obstet. Gynecol. Clin. N. Am. 2014, 41, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Feinberg, B.; Burwick, R. Thrombotic microangiopathies of pregnancy: Differential diagnosis. Pregnancy Hypertens. 2018, 12, 29–34. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Kearon, C.; Ageno, W.; Cannegieter, S.C.; Cosmi, B.; Geersing, G.-J.; Kyrle, P.A. Categorization of patients as having provoked or unprovoked venous thromboembolism: Guidance from the SSC of ISTH. J. Thromb. Haemost. 2016, 14, 1480–1483. [Google Scholar] [CrossRef]
- Lu, H.; Yang, Q.; Yang, L.; Qu, K.; Tian, B.; Xiao, Q.; Xin, X.; Lv, Y.; Zheng, X. The risk of venous thromboembolism associated with midline catheters compared with peripherally inserted central catheters: A systematic review and meta-analysis. Nurs. Open 2021, 9, 1873–1882. [Google Scholar] [CrossRef]
- Harbin, M.M.; Lutsey, P.L. May-Thurner syndrome: History of understanding and need for defining population prevalence. J. Thromb. Haemost. 2019, 18, 534–542. [Google Scholar] [CrossRef]
- Chandra, D.; Parisini, E.; Mozaffarian, D. Meta-analysis: Travel and risk for venous thromboembolism. Ann. Intern. Med. 2009, 151, 180–190. [Google Scholar] [CrossRef]
- Enga, K.F.; Braekkan, S.K.; Hansen-Krone, I.J.; le Cessie, S.; Rosendaal, F.R.; Hansen, J.-B. Cigarette smoking and the risk of venous thromboembolism: The Tromsø Study. J. Thromb. Haemost. 2012, 10, 2068–2074. [Google Scholar] [CrossRef]
- ACOG Practice Bulletin No. 197: Inherited Thrombophilias in Pregnancy: Correction. Obstet. Gynecol. 2018, 132, 1069.
- Kahn, S.R.; Lim, W.; Dunn, A.S.; Cushman, M.; Dentali, F.; Akl, E.A.; Cook, J.K.; Balekian, A.A.; Klein, C.R.; Le, H.; et al. Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e195S–e226S. [Google Scholar] [CrossRef]
- George, M.G. Risk Factors for Ischemic Stroke in Younger Adults: A Focused Update. Stroke 2020, 51, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Crous-Bou, M.; Harrington, L.B.; Kabrhel, C. Environmental and Genetic Risk Factors Associated with Venous Thromboembolism. Semin. Thromb. Hemost. 2016, 42, 808–820. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.K.; Minissian, M.; Merz, C.N.B. Adverse pregnancy outcomes and cardiovascular risk factor management. Semin. Perinatol. 2015, 39, 268–275. [Google Scholar] [CrossRef]
- Gaddh, M.; Rosovsky, R.P. Venous Thromboembolism: Genetics and Thrombophilias. Semin Resp Crit Care Med. 2021, 42, 271–283. [Google Scholar] [CrossRef]
- Shen, Y.-M.; Tsai, J.; Taiwo, E.; Gavva, C.; Yates, S.G.; Patel, V.; Frenkel, E.; Sarode, R. Analysis of Thrombophilia Test Ordering Practices at an Academic Center: A Proposal for Appropriate Testing to Reduce Harm and Cost. PLoS ONE 2016, 11, e0155326. [Google Scholar] [CrossRef]
- Khan, S.; Dickerman, J.D. Hereditary thrombophilia. Thromb. J. 2006, 4, 15. [Google Scholar] [CrossRef][Green Version]
- Omran, S.S.; Lerario, M.P.; Gialdini, G.; Merkler, A.E.; Moya, A.; Chen, M.L.; Kamel, H.; DeSancho, M.; Navi, B.B. Clinical Impact of Thrombophilia Screening in Young Adults with Ischemic Stroke. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2019, 28, 882–889. [Google Scholar] [CrossRef]
- May, J.E.; Martin, K.D.; Taylor, L.J.; Gangaraju, R.; Lin, C. Current Practice and Clinical Utility of Thrombophilia Testing in Hospitalized Patients with Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105209. [Google Scholar] [CrossRef]
- Vossen, C.Y.; Conard, J.; Fontcuberta, J.; Makris, M.; van der Meer, F.J.M.; Pabinger, I.; Palareti, G.; Preston, F.E.; Scharrer, I.; Souto, J.C.; et al. Risk of a first venous thrombotic event in carriers of a familial thrombophilic defect. The European Prospective Cohort on Thrombophilia (EPCOT). J. Thromb. Haemost. 2005, 3, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, I. Thrombophilia and its impact on pregnancy11Adapted from Pabinger I, Thrombophilia and its impact on pregnancy. Thromb. Res. 2009, 123, S16–S21. [Google Scholar] [CrossRef]
- Stefanski, A.-L.; Specker, C.; Fischer-Betz, R.; Henrich, W.; Schleussner, E.; Dörner, T. Maternal Thrombophilia and Recurrent Miscarriage—Is There Evidence That Heparin is Indicated as Prophylaxis against Recurrence? Geburtshilfe Frauenheilkd. 2018, 78, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Chen, Y.; Ye, C.; Xing, D.; Wu, R.; Li, F.; Chen, L.; Wang, T. Hereditary thrombophilia and recurrent pregnancy loss: A systematic review and meta-analysis. Hum. Reprod. 2021, 36, 1213–1229. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Meleth, S.; Catellier, D.; Crowther, M.; Erkan, D.; Fortin, P.R.; Garcia, D.; Haywood, N.; Kosinski, A.S.; Levine, S.R.; et al. Recurrent thrombosis in patients with antiphospholipid antibodies and an initial venous or arterial thromboembolic event: A systematic review and meta-analysis. J. Thromb. Haemost. 2020, 18, 2274–2286. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No influence on treatment | Anticoagulation therapy or prophylaxis should have been initiated irrespective of thrombophilia testing result | |
| Positive or potential positive influence | Appropriate decision | Decision to extend, intensify or initiate any type of anticoagulation based on a thrombophilia testing result |
| Result not considered/overlooked | Thrombophilia testing result not considered in treatment decision, although it should have been | |
| Negative influence | Decision to undertreat | Decision to withhold or not initiate any type of anticoagulation because thrombophilia testing result was not in accordance with guidelines |
| Decision to overtreat | Decision to extend or initiate any type of anticoagulation based on a thrombophilia testing result not in accordance with guidelines |
| Characteristic | Tested Patients n= 3550 | Negative Work-Up n = 2358 (66) | Positive Work-Up n = 1192 (34) | p-Value |
|---|---|---|---|---|
| Age, year, mean (±SD) * | 42 (15) | 43 (15) | 39 (15) | |
| Sex, n (%) | <0.001 | |||
| Female | 2118 (60) | 1358 (58) | 760 (64) | |
| Indication for consulting, n (%) | <0.001 | |||
| Arterial thrombosis | 583 (16) | 455 (19) | 128 (11) | |
| VTE | 2343 (66) | 1587 (67) | 756 (63) | |
| Pregnancy-related morbidity | 120 (3.4) | 59 (2.5) | 61 (5.1) | |
| Asymptomatic patients | 504 (14) | 257 (11) | 247 (21) | |
| Provoking factors of VTE †, n (%) | 0.026 | |||
| Unprovoked VTE | 683 (19) | 460 (20) | 223 (19) | |
| Provoked VTE, minor risk factor | 1242 (35) | 821 (35) | 421 (35) | |
| Provoked VTE, major risk factor | 415 (12) | 303 (13) | 112 (9.4) | |
| Referral for recurrent VTE †, n (%) | 0.009 | |||
| Yes | 571 (16) | 365 (15) | 206 (17) | |
| Number of co-morbidities *, n (%) | <0.001 | |||
| 0 | 1999 (56) | 1231 (52) | 768 (64) | |
| 1 | 814 (23) | 569 (24) | 245 (21) | |
| 2 or more | 737 (21) | 558 (24) | 179 (15) | |
| Number of risk factors for thromboembolism *, n (%) | <0.001 | |||
| 0 | 1259 (35) | 783 (33) | 467 (40) | |
| 1 | 1189 (33) | 791 (34) | 398 (33) | |
| 2 or more | 1102 (31) | 784 (33) | 318 (27) | |
| Family history of VTE in first-degree relatives †, n (%) | <0.001 | |||
| Positive | 1106 (31) | 643 (27) | 463 (39) | |
| Family history of VTE in second-degree relatives †, n (%) | <0.001 | |||
| Positive | 523 (15) | 315 (13) | 208 (17) | |
| Total | No Influence on Therapy | Positive and Potential Positive Influence | Negative Influence | p-Value | |||
|---|---|---|---|---|---|---|---|
| Appropriate Decision | Overlooked Results | Decision to Overtreat | Decision to Undertreat | ||||
| n = 3550 | n = 3050 (85.9) | n = 211 (5.7) | n = 82 (2.2) | n = 11 (0.3) | n = 184 (5.1) | <0.001 | |
| Negative thrombophilia work-up, n (%) | 2358 (66) | 2171 (71) | 0 | 0 | 1 (9.1) | 181 (98) | |
| Hereditary low-risk thrombophilia, n (%) | 826 (23) | 675 (22) | 111 (53) | 25 (30) | 7 (64) | 3 (1.6) | |
| Hereditary high-risk thrombophilia, n (%) | 247 (6.3) | 157 (5.1) | 50 (24) | 36 (44) | 2 (18) | 0 | |
| Antiphospholipid antibody syndrome, n (%) | 119 (3.4) | 47 (1.5) | 50 (24) | 21 (26) | 1 (9.1) | 0 | |
| Type of Thrombophilia | OR (95% CI) |
|---|---|
| Heterozygous factor V Leiden mutation | 1 (ref) |
| Antiphospholipid antibody syndrome | 8.26 (5.40–12.62) |
| Antithrombin < 70% | 5.15 (2.84–9.34) |
| Homozygous factor V Leiden mutation | 3.93 (2.10–7.34) |
| Protein S < 59% | 1.99 (1.21–3.27) |
| Heterozygous prothrombin 20210G>A mutation | 1.89 (1.24–2.90) |
| Homozygous prothrombin 20210G>A mutation | 2.79 (0.25–31.07) |
| Protein C < 69% | 2.17 (0.88–5.33) |
| Crude HR (95% CI) | Adjusted HR (95% CI) | |
|---|---|---|
| Venous thromboembolism | ||
| Negative work-up | 1 (ref.) | 1 (ref.) |
| Hereditary low-risk thrombophilia | 1.02 (0.66–1.56) | 1.08 (0.70–1.67) |
| Hereditary high-risk thrombophilia | 1.99 (1.18–3.36) | 2.55 (1.49–4.35) |
| APS | 2.33 (1.13–4.84) | 2.50 (1.20–5.19) |
| Arterial thrombosis | ||
| Negative work-up | 1 (ref.) | 1 (ref.) |
| Hereditary low-risk thrombophilia | 0.69 (0.40–1.18) | 0.86 (0.50–1.50) |
| Hereditary high-risk thrombophilia | 0.27 (0.07– 1.11) | 0.38 (0.09–1.58) |
| APS | 0.70 (0.17–2.85) | 0.82 (0.20–3.37) |
| Pregnancy-related morbidity | ||
| Negative work-up | 1 (ref.) | 1 (ref.) |
| Hereditary low-risk thrombophilia | 0.76 (0.21–2.69) | 0.57 (0.16–2.04) |
| Hereditary high-risk thrombophilia | 3.23 (1.04–10.00) | 1.93 (0.62–6.05) |
| APS | 4.49 (1.27–15.96) | 3.86 (1.07–13.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vrotniakaite-Bajerciene, K.; Tritschler, T.; Jalowiec, K.A.; Broughton, H.; Brodard, J.; Porret, N.A.; Haynes, A.; Rovo, A.; Kremer Hovinga, J.A.; Aujesky, D.; et al. Thrombophilia Impact on Treatment Decisions, Subsequent Venous or Arterial Thrombosis and Pregnancy-Related Morbidity: A Retrospective Single-Center Cohort Study. J. Clin. Med. 2022, 11, 4188. https://doi.org/10.3390/jcm11144188
Vrotniakaite-Bajerciene K, Tritschler T, Jalowiec KA, Broughton H, Brodard J, Porret NA, Haynes A, Rovo A, Kremer Hovinga JA, Aujesky D, et al. Thrombophilia Impact on Treatment Decisions, Subsequent Venous or Arterial Thrombosis and Pregnancy-Related Morbidity: A Retrospective Single-Center Cohort Study. Journal of Clinical Medicine. 2022; 11(14):4188. https://doi.org/10.3390/jcm11144188
Chicago/Turabian StyleVrotniakaite-Bajerciene, Kristina, Tobias Tritschler, Katarzyna Aleksandra Jalowiec, Helen Broughton, Justine Brodard, Naomi Azur Porret, Alan Haynes, Alicia Rovo, Johanna Anna Kremer Hovinga, Drahomir Aujesky, and et al. 2022. "Thrombophilia Impact on Treatment Decisions, Subsequent Venous or Arterial Thrombosis and Pregnancy-Related Morbidity: A Retrospective Single-Center Cohort Study" Journal of Clinical Medicine 11, no. 14: 4188. https://doi.org/10.3390/jcm11144188
APA StyleVrotniakaite-Bajerciene, K., Tritschler, T., Jalowiec, K. A., Broughton, H., Brodard, J., Porret, N. A., Haynes, A., Rovo, A., Kremer Hovinga, J. A., Aujesky, D., & Angelillo-Scherrer, A. (2022). Thrombophilia Impact on Treatment Decisions, Subsequent Venous or Arterial Thrombosis and Pregnancy-Related Morbidity: A Retrospective Single-Center Cohort Study. Journal of Clinical Medicine, 11(14), 4188. https://doi.org/10.3390/jcm11144188