
Modified Mini-Keystone Flaps for Coverage of Tiny Volar Pulp Defects of the Fingertips in Cases with Missing Amputation Skin Stumps: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
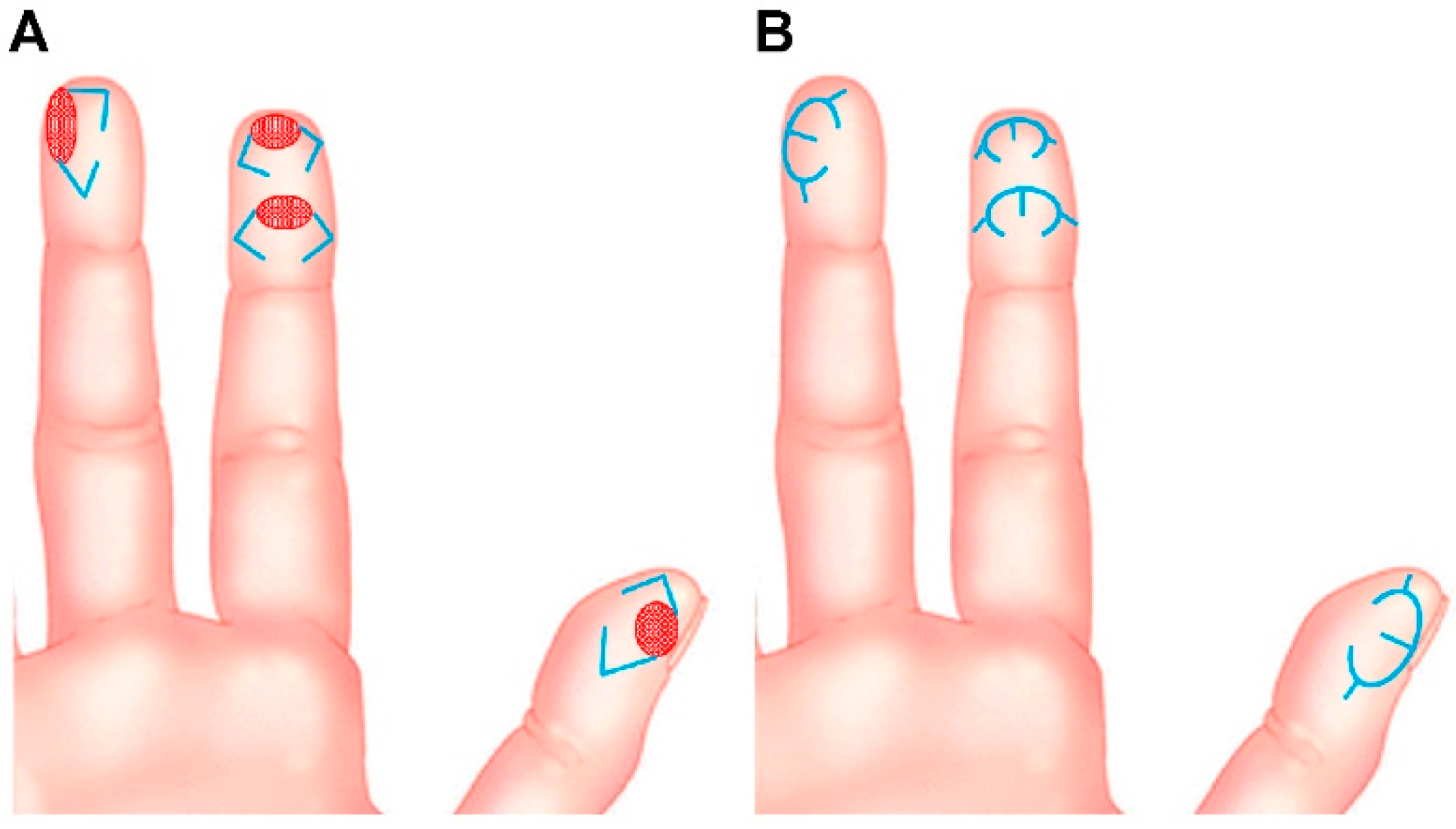
2.1. Surgical Techniques
2.2. Evaluation of Postoperative Functional Outcomes
2.3. Statistical Analysis
3. Results
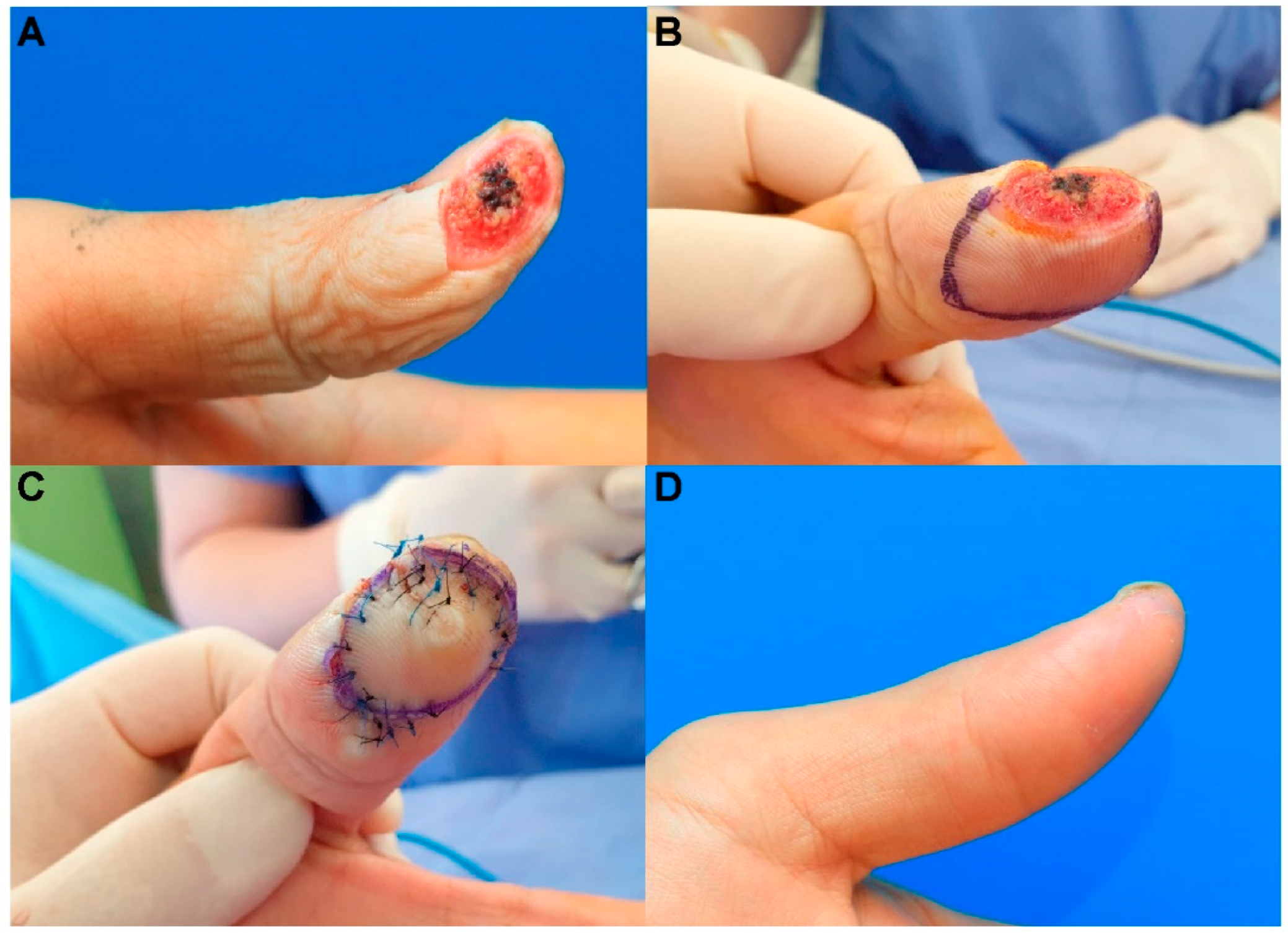
3.1. Case Presentations
3.1.1. Case 5
3.1.2. Case 6
3.1.3. Case 11
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozturk, M.B.; Barutca, S.A.; Aksan, T.; Atik, B. Pulp rotation flap for lateral oblique fingertip defects. Ann. Plast. Surg. 2016, 77, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Das De, S.; Sebastin, S.J. Soft tissue coverage of the digits and hand. Hand Clin. 2020, 36, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C.S.; Kim, S.I.; Kim, H.; Kim, K.N. Keystone-designed perforator island flaps for the coverage of traumatic pretibial defects in patients with comorbidities. Int. J. Low. Extrem. Wounds 2017, 16, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Yoon, C.S.; Lee, H.G.; Kim, K.N. Keystone design perforator island flap in facial defect reconstruction. World J. Clin. Cases 2020, 8, 1832–1847. [Google Scholar] [CrossRef] [PubMed]
- Behan, F.C.; Rozen, W.M.; Lo, C.H.; Findlay, M. The omega—Ω—variant designs (types A and B) of the keystone perforator island flap. ANZ J. Surg. 2011, 81, 650–652. [Google Scholar] [CrossRef] [PubMed]
- Moncrieff, M.D.; Bowen, F.; Thompson, J.F.; Saw, R.P.; Shannon, K.F.; Spillane, A.J.; Quinn, M.J.; Stretch, J.R. Keystone flap reconstruction of primary melanoma excision defects of the leg –the end of the skin graft? Ann. Surg. Oncol. 2008, 15, 2867–2873. [Google Scholar] [CrossRef]
- Lee, H.G.; Lim, S.Y.; Kim, Y.K.; Yoon, C.S.; Kim, K.N. Keystone design perforator island flaps for coverage of non-oncological periarticular defects surrounded by the zone of injury. J. Int. Med. Res. 2020, 48, 0300060520930152. [Google Scholar] [CrossRef]
- Lundborg, G.; Rosén, B. The two-point discrimination test–time for a re-appraisal? J. Hand Surg. Br. 2004, 29, 418–422. [Google Scholar] [CrossRef]
- Silva, P.G.; Jones, A.; Araujo, P.M.; Natour, J. Assessment of light touch sensation in the hands of systemic sclerosis patients. Clinics 2014, 69, 585–588. [Google Scholar] [CrossRef]
- Weber, R.A.; Breidenbach, W.C.; Brown, R.E.; Jabaley, M.E.; Mass, D.P. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast. Reconstr. Surg. 2000, 106, 1036–1045, discussion 1046. [Google Scholar] [CrossRef]
- Kawaiah, A.; Thakur, M.; Garg, S.; Kawasmi, S.H.; Hassan, A. Fingertip injuries and amputations: A review of the literature. Cureus 2020, 12, e8291. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.H.; Jung, S.N.; Kim, H.J.; Kwon, H.; Sohn, W.I.; Yoo, G.; Im, K.S. Treatment of posttraumatic fingertip pain using a great toe pulp graft. Ann. Plast. Surg. 2011, 67, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Gharb, B.B.; Rampazzo, A.; Armijo, B.S.; Eshraghi, Y.; Totonchi, A.S.; Teo, T.C.; Salgado, C.J. Tranquilli-Leali or Atasoy flap: An anatomical cadaveric study. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Lemmon, J.A.; Janis, J.E.; Rohrich, R.J. Soft-tissue injuries of the fingertip: Methods of evaluation and treatment. An algorithmic approach. Plast. Reconstr. Surg. 2008, 122, 105e–117e. [Google Scholar] [CrossRef] [Green Version]
- Sebastin, S.J.; Mendoza, R.T.; Chong, A.K.S.; Peng, Y.P.; Ono, S.; Chung, K.C.; Lim, A.Y.T. Application of the dorsal metacarpal artery perforator flap for resurfacing soft-tissue defects proximal to the fingertip. Plast. Reconstr. Surg. 2011, 128, 166e–178e. [Google Scholar] [CrossRef]
- Behan, F.C. The keystone design perforator island flap in reconstructive surgery. ANZ J. Surg. 2003, 73, 112–120. [Google Scholar] [CrossRef]
- Yoon, C.S.; Kim, H.B.; Kim, Y.K.; Kim, H.; Kim, K.N. Relaxed skin tension line–oriented keystone–designed perforator island flaps considering the facial aesthetic unit concept for the coverage of small to moderate facial defects. Medicine 2019, 98, e14167. [Google Scholar] [CrossRef]
- Yoon, C.S.; Kim, H.B.; Kim, Y.K.; Kim, H.; Kim, K.N. Keystone-design perforator island flaps for the management of complicated epidermoid cysts on the back. Sci. Rep. 2019, 9, 14699. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Chittoria, R.K.; Chavan, V.; Aggarwal, A.; Reddy, C.L.; Mohan, P.B.; Shijina, K.; Pathan, I. Role of keystone flap in finger reconstruction. Clin. Surg. J. 2019, 2, 11–15. [Google Scholar]
- Rajabtork Zadeh, O.; Rizzo, M.I.; Monarca, C. The versatility of keystone flap: Reconstructive option in ring finger. Plast. Reconstr. Surg. Glob. Open. 2020, 8, e2526. [Google Scholar] [CrossRef]
- Lee, D.H.; Mignemi, M.E.; Crosby, S.N. Fingertip injuries: An update on management. J. Am. Acad. Orthop. Surg. 2013, 21, 756–766. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Cause of the Defect | Defect Location | Defect Size (cm2) | Flap Size (cm2) | Flap Survival | Complications | Static 2-PDT (Affected Fingertip/Contralateral Normal Fingertip, mm) | Dynamic 2-PDT (Affected Fingertip/Contralateral Normal Fingertip, mm) | Follow-Up Period (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F/27 | Trauma caused by cutter knife | Rt. volar pulp of the thumb | 0.7 × 1.0 | 0.9 × 2.0 | Fully survived | None | 3/3 | 2/2 | 7 |
| 2 | F/59 | Trauma caused by kitchen knife | Lt. volar pulp of the fifth finger | 0.5 × 1.0 | 0.7 × 1.5 | Fully survived | None | 4/4 | 3/3 | 6 |
| 3 | M/61 | Trauma caused by cutter knife | Rt. volar pulp of the thumb | 1.0 × 1.5 | 1.5 × 3.0 | Fully survived | Distal margin maceration | 6/4 | 5/3 | 5 |
| 4 | M/34 | Trauma caused by cutter knife | Lt. volar pulp of the fourth finger | 0.7 × 0.9 | 0.9 × 1.6 | Fully survived | None | 3/3 | 2/2 | 7 |
| 5 | M/47 | Trauma caused by cutter knife | Rt. volar pulp of the second finger | 0.6 × 1.0 | 0.8 × 1.5 | Fully survived | None | 2/2 | 2/2 | 6 |
| 6 | M/36 | Trauma caused by cutter knife | Lt. volar pulp of the fifth finger | 0.6 × 1.5 | 0.8 × 2.5 | Fully survived | None | 4/4 | 3/3 | 6 |
| 7 | M/19 | Trauma caused by cutter knife | Rt. volar pulp of the thumb | 0.8 × 1.1 | 1.0 × 2.3 | Fully survived | None | 3/3 | 2/2 | 7 |
| 8 | M/41 | Trauma caused by kitchen knife | Lt. volar pulp of the second finger | 0.6 × 1.0 | 0.8 × 2.0 | Fully survived | None | 4/4 | 3/3 | 6 |
| 9 | M/58 | Trauma caused by cutter knife | Rt. volar pulp of the second finger | 0.9 × 1.5 | 1.3 × 2.5 | Fully survived | None | 4/4 | 4/4 | 5 |
| 10 | M/56 | Trauma caused by cutter knife | Lt. volar pulp of the second finger | 0.6 × 1.2 | 0.9 × 1.6 | Fully survived | None | 5/4 | 4/3 | 5 |
| 11 | M/30 | Trauma caused by kitchen knife | Lt. volar pulp of the thumb | 1.2 × 2.0 | 1.5 × 3.0 | Fully survived | None | 6/4 | 5/3 | 5 |
| 12 | M/31 | Trauma caused by kitchen knife | Lt. volar pulp of the second finger | 0.7 × 1.2 | 1.0 × 2.2 | Fully survived | None | 3/3 | 3/3 | 5 |
| 13 | F/42 | Trauma caused by cutter knife | Rt. volar pulp of the fifth finger | 0.6 × 1.1 | 0.8 × 1.7 | Fully survived | None | 4/4 | 4/4 | 5 |
| 14 | F/56 | Trauma caused by kitchen knife | Rt. volar pulp of the fourth finger | 0.7 × 1.3 | 1.1 × 1.8 | Fully survived | None | 4/4 | 3/3 | 5 |
| 15 | F/54 | Trauma caused by kitchen knife | Lt. volar pulp of the second finger | 0.8 × 1.0 | 1.2 × 2.0 | Fully survived | None | 5/4 | 4/3 | 6 |
| Static 2-PDT (Affected Fingertip) | Static 2-PDT (Contralateral Normal Fingertip) | Dynamic 2-PDT (Affected Fingertip) | Dynamic 2-PDT (Contralateral Normal Fingertip) | |
|---|---|---|---|---|
| Good (Static 2-PDT, <6 mm; dynamic 2-PDT, <4 mm) | 13 | 15 | 8 | 13 |
| Fair (Static 2-PDT, 6~10 mm; dynamic 2-PDT, 4~7 mm) | 2 | 0 | 7 | 2 |
| Poor (Static 2-PDT, >10 mm; dynamic 2-PDT, >7 mm) | 0 | 0 | 0 | 0 |
| Mean ± SD (mm) | 4.00 ± 1.13 | 3.60 ± 0.63 | 3.27 ± 1.03 | 2.87 ± 0.64 |
| Student’s t-test | p = 0.243 | p = 0.213 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, B.W.; Oh, S.; Kim, J.; Oh, K.S.; Shin, H.W.; Kim, K.N. Modified Mini-Keystone Flaps for Coverage of Tiny Volar Pulp Defects of the Fingertips in Cases with Missing Amputation Skin Stumps: A Retrospective Study. J. Clin. Med. 2022, 11, 3394. https://doi.org/10.3390/jcm11123394
Yoo BW, Oh S, Kim J, Oh KS, Shin HW, Kim KN. Modified Mini-Keystone Flaps for Coverage of Tiny Volar Pulp Defects of the Fingertips in Cases with Missing Amputation Skin Stumps: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(12):3394. https://doi.org/10.3390/jcm11123394
Chicago/Turabian StyleYoo, Byung Woo, Seungyoon Oh, Junekyu Kim, Kap Sung Oh, Hyun Woo Shin, and Kyu Nam Kim. 2022. "Modified Mini-Keystone Flaps for Coverage of Tiny Volar Pulp Defects of the Fingertips in Cases with Missing Amputation Skin Stumps: A Retrospective Study" Journal of Clinical Medicine 11, no. 12: 3394. https://doi.org/10.3390/jcm11123394
APA StyleYoo, B. W., Oh, S., Kim, J., Oh, K. S., Shin, H. W., & Kim, K. N. (2022). Modified Mini-Keystone Flaps for Coverage of Tiny Volar Pulp Defects of the Fingertips in Cases with Missing Amputation Skin Stumps: A Retrospective Study. Journal of Clinical Medicine, 11(12), 3394. https://doi.org/10.3390/jcm11123394