
Performance of sFlt-1/PIGF Ratio for the Prediction of Perinatal Outcome in Obese Pre-Eclamptic Women

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Ethical Approval
3. Results
3.1. Baseline Characteristics and Perinatal Outcome
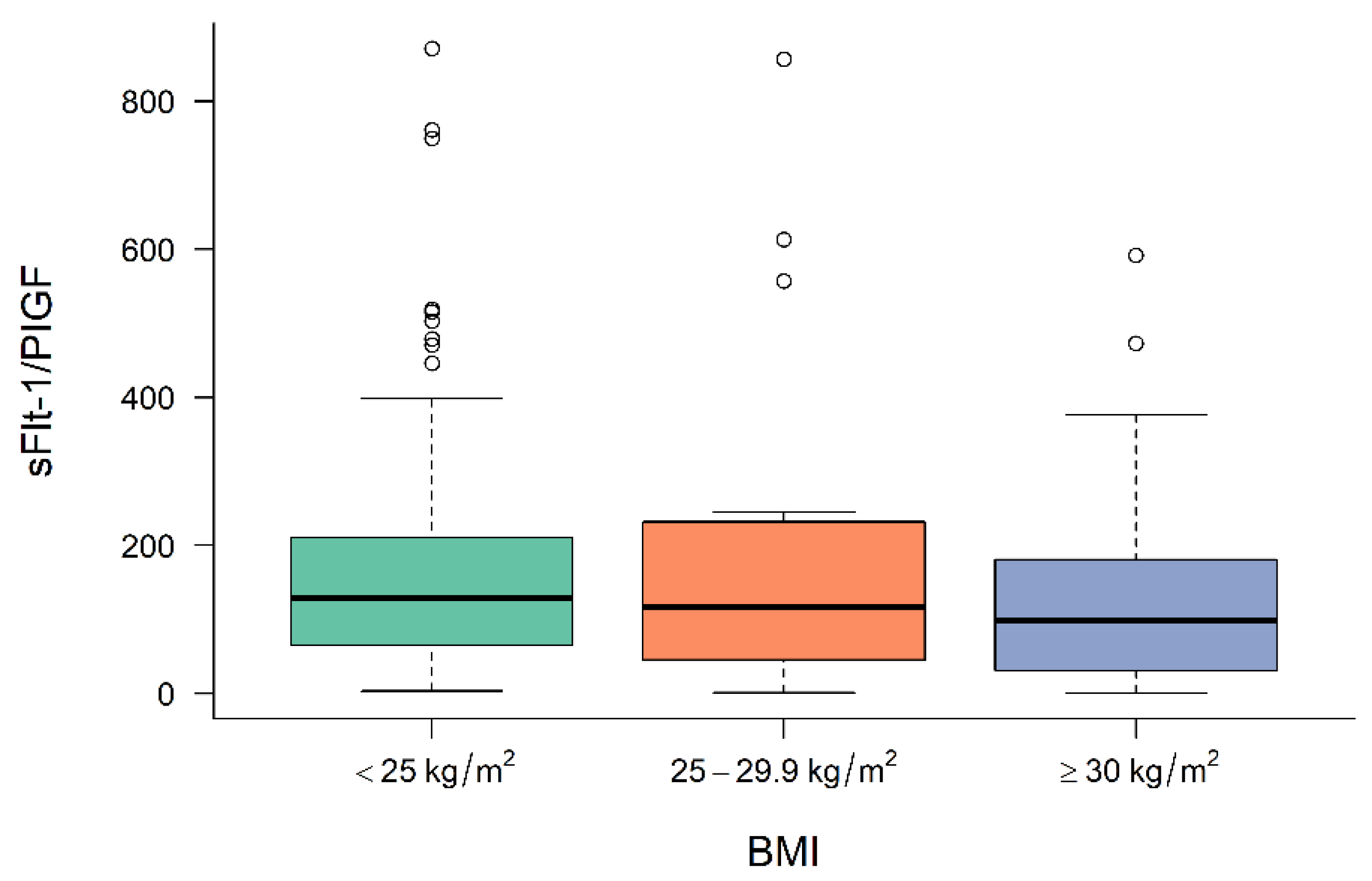
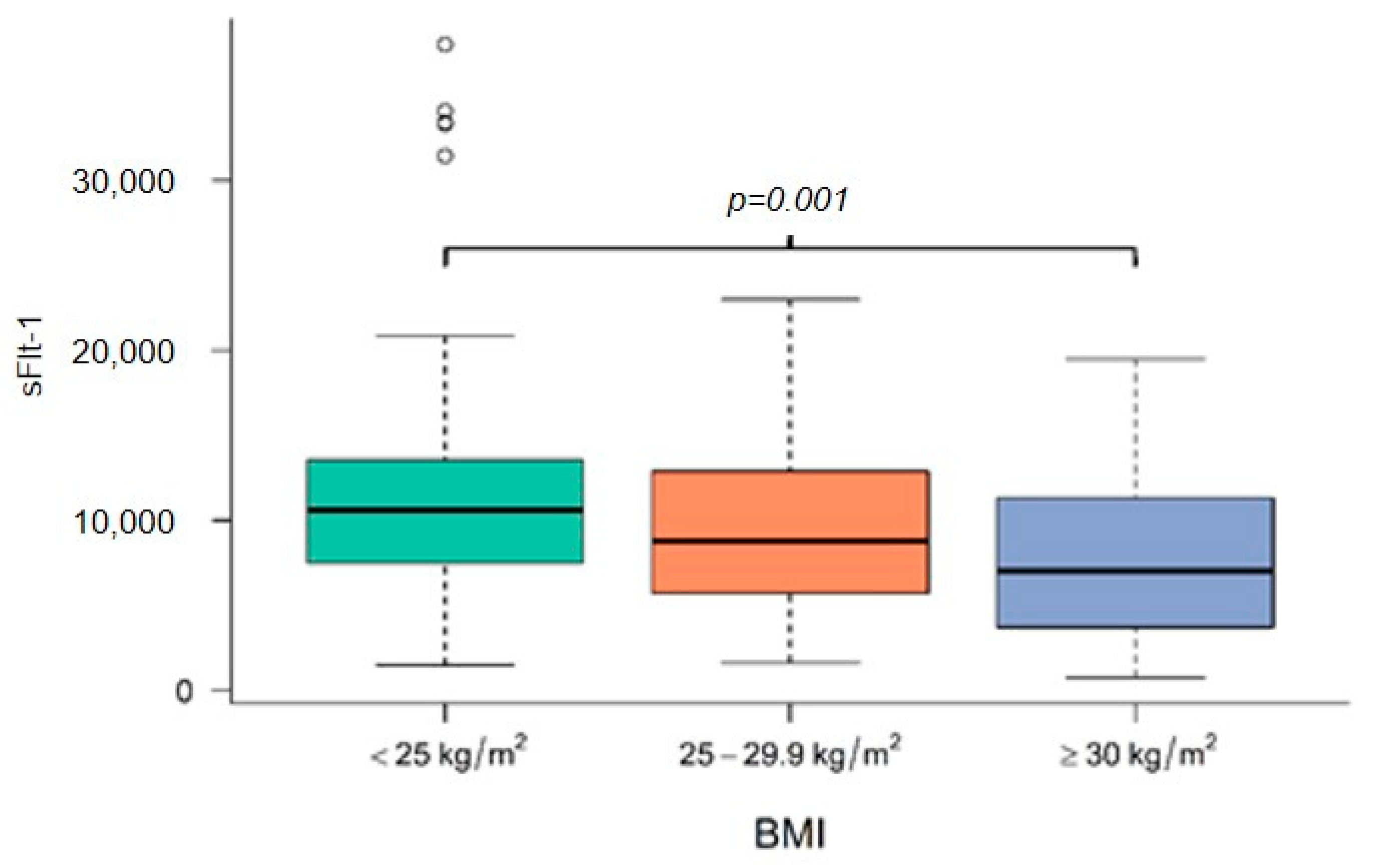
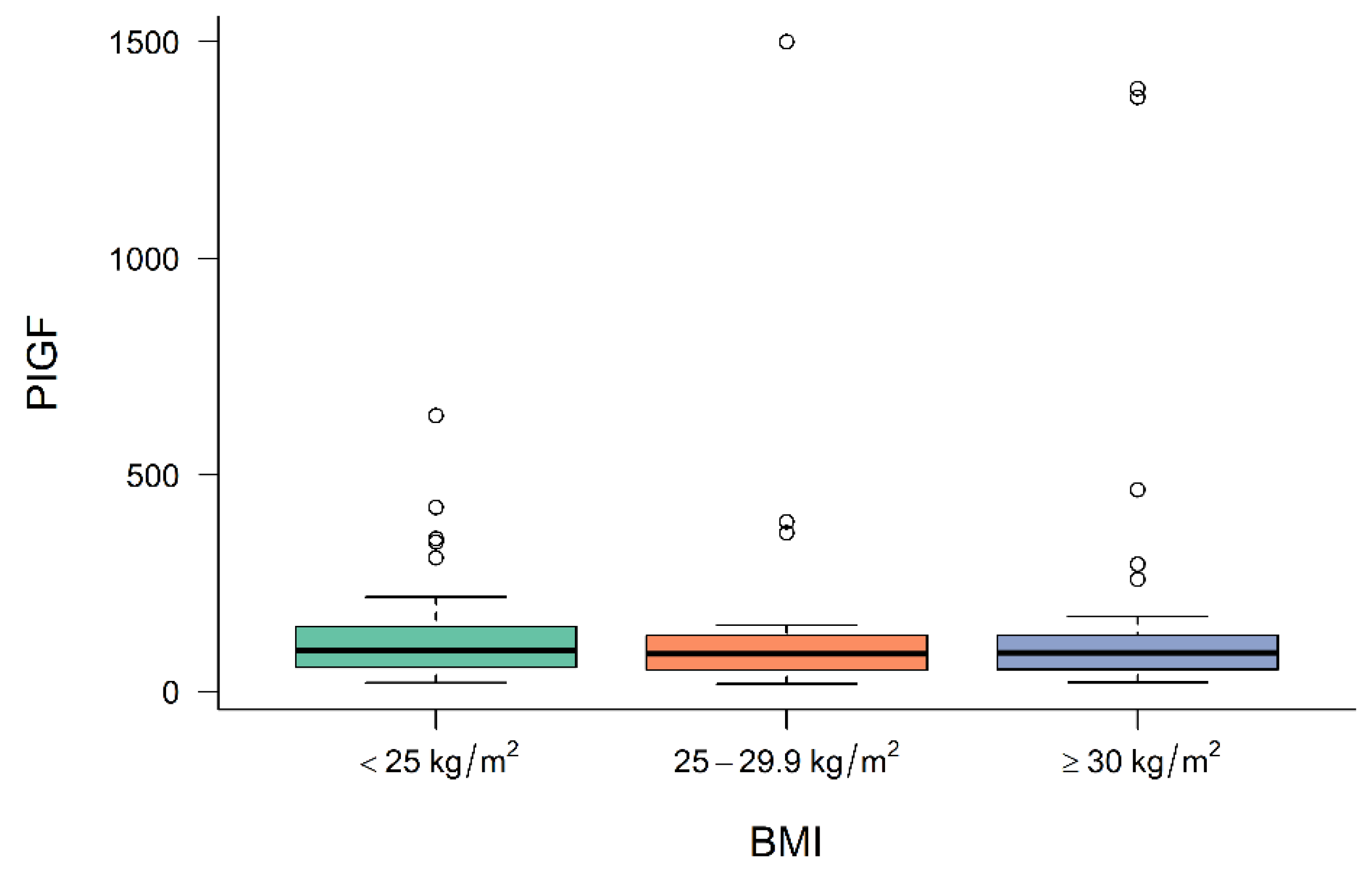
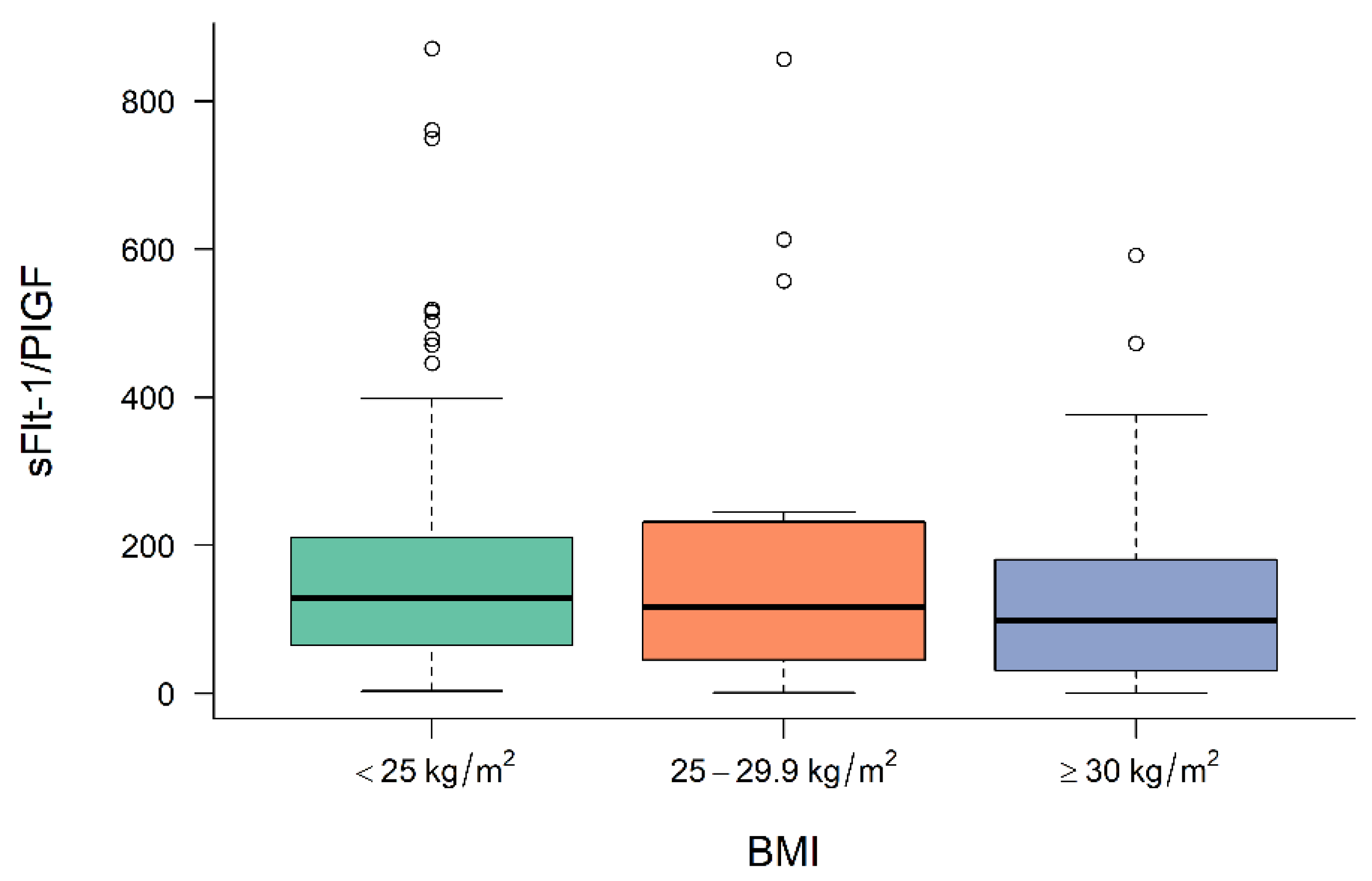
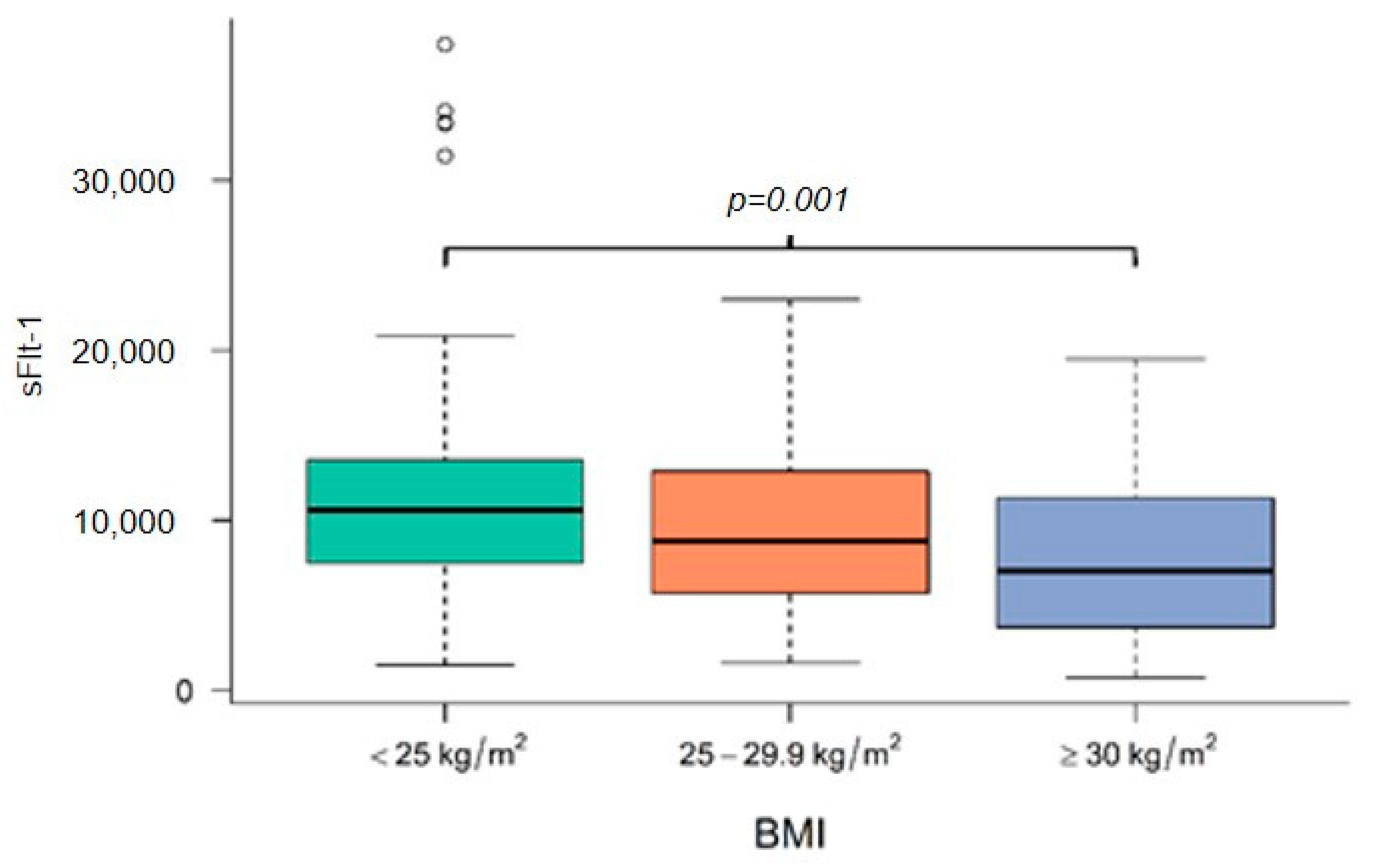
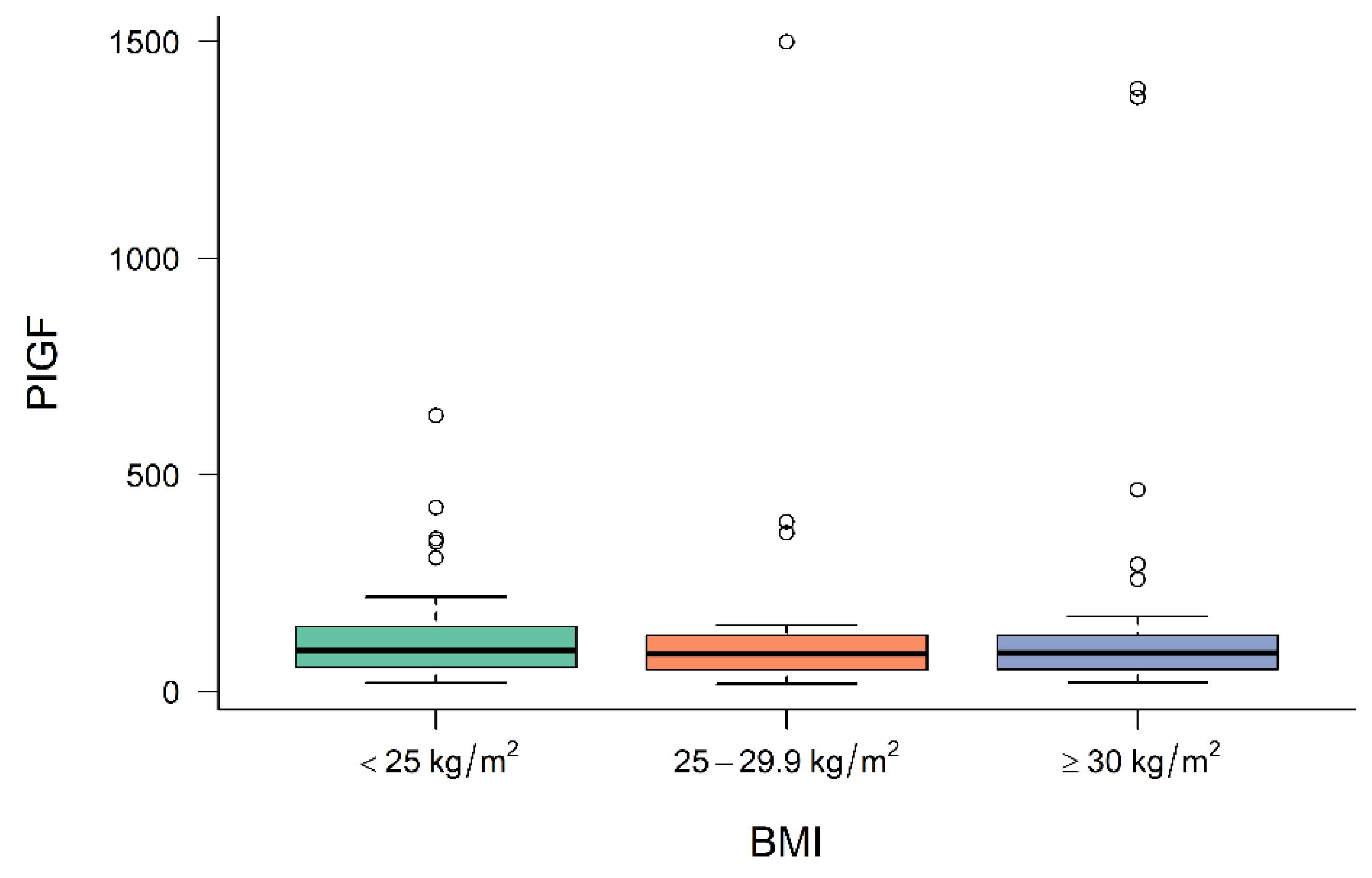
3.2. Levels of Angiogenic Factors in Preeclamptic Women Depending on BMI
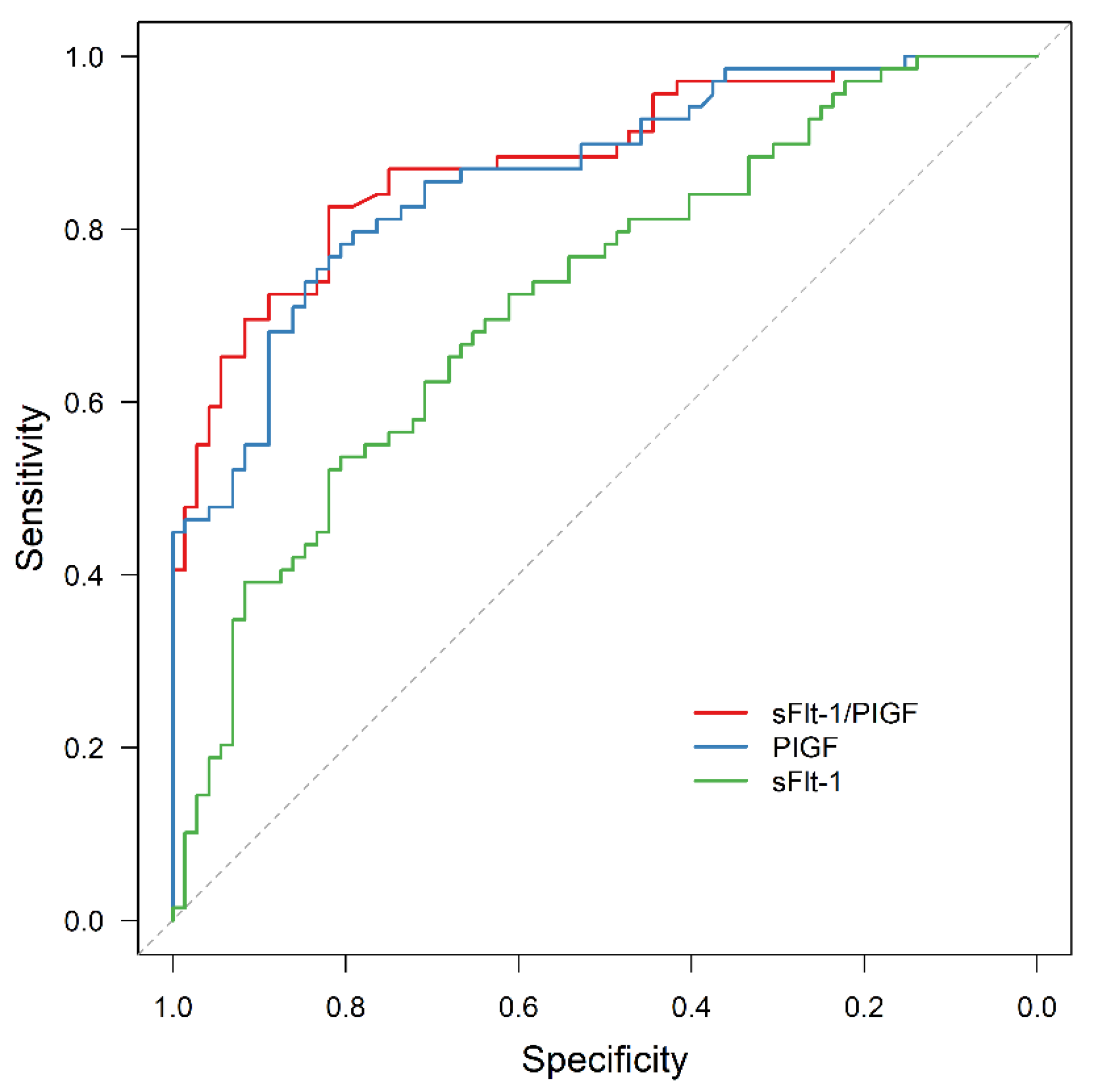
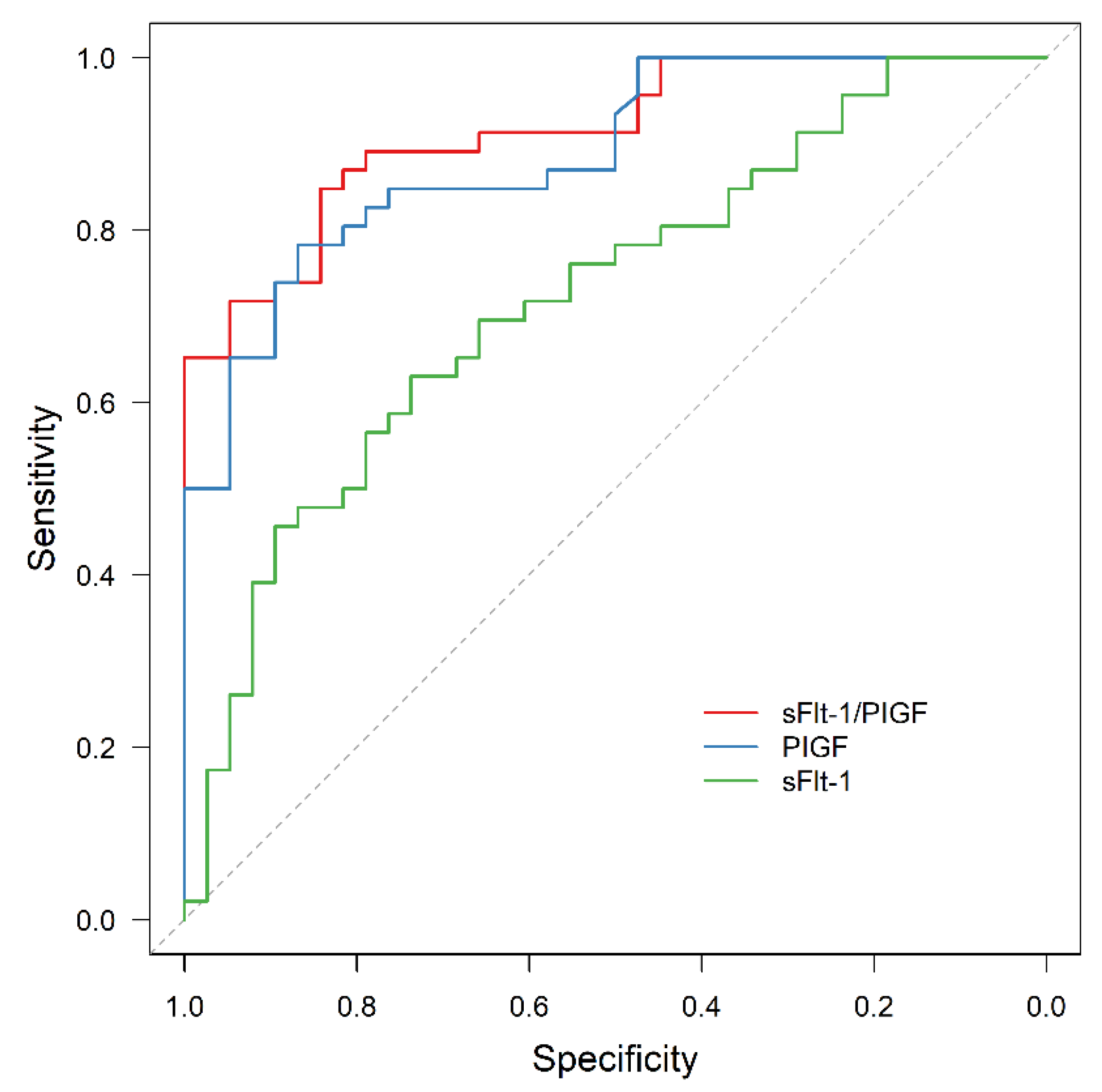
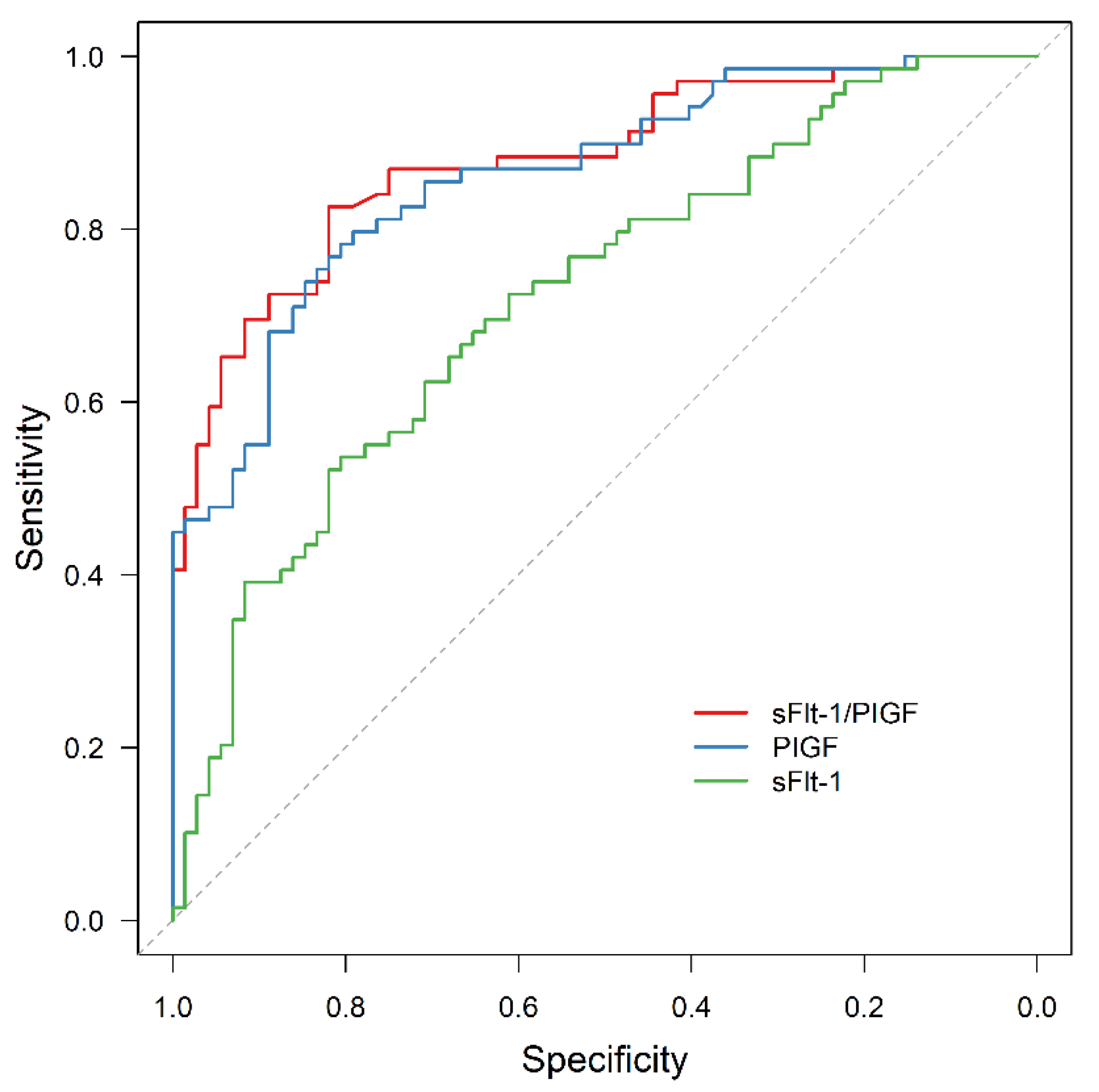
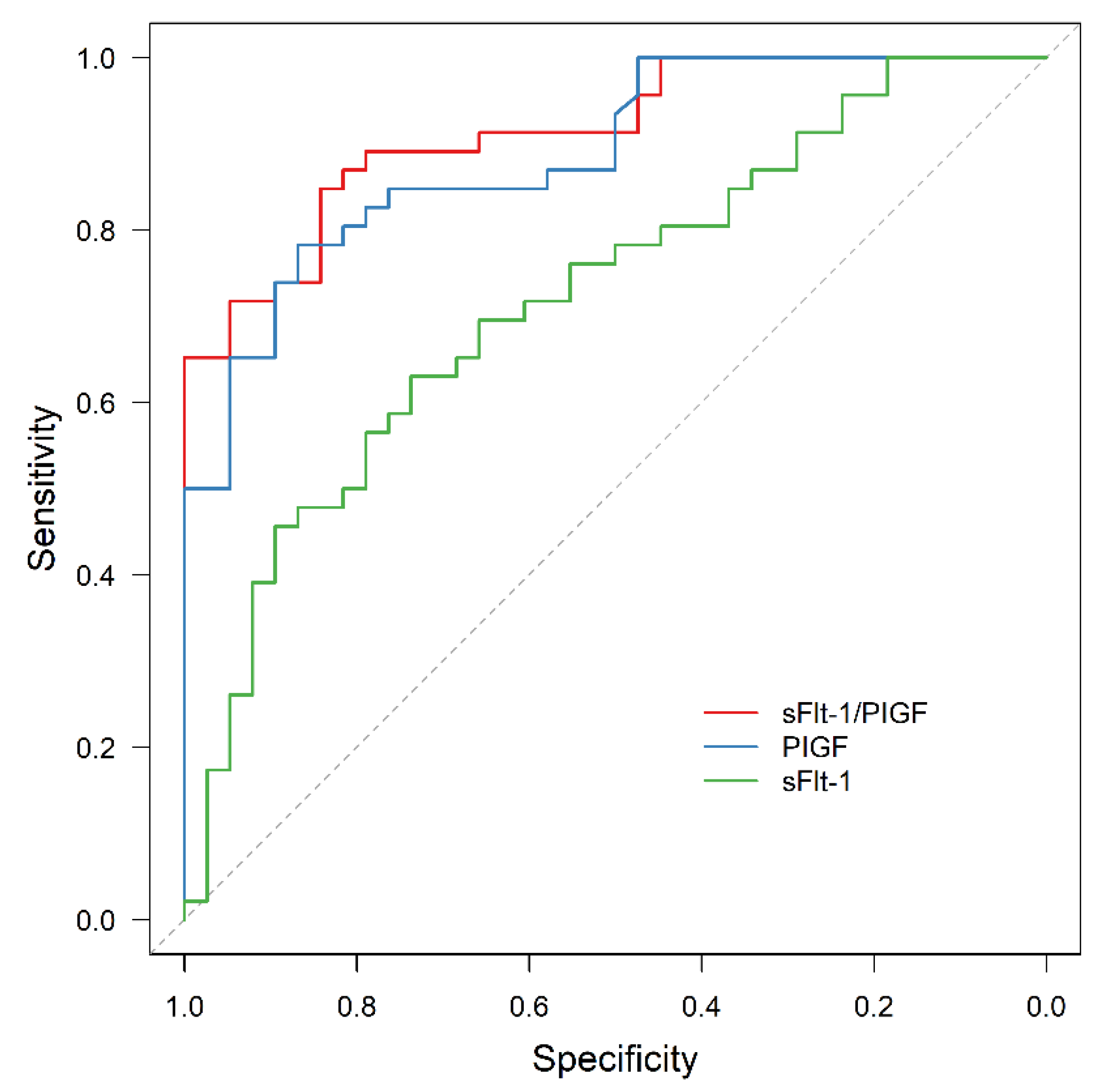
3.3. APO Prediction by sFlt-1/PlGF
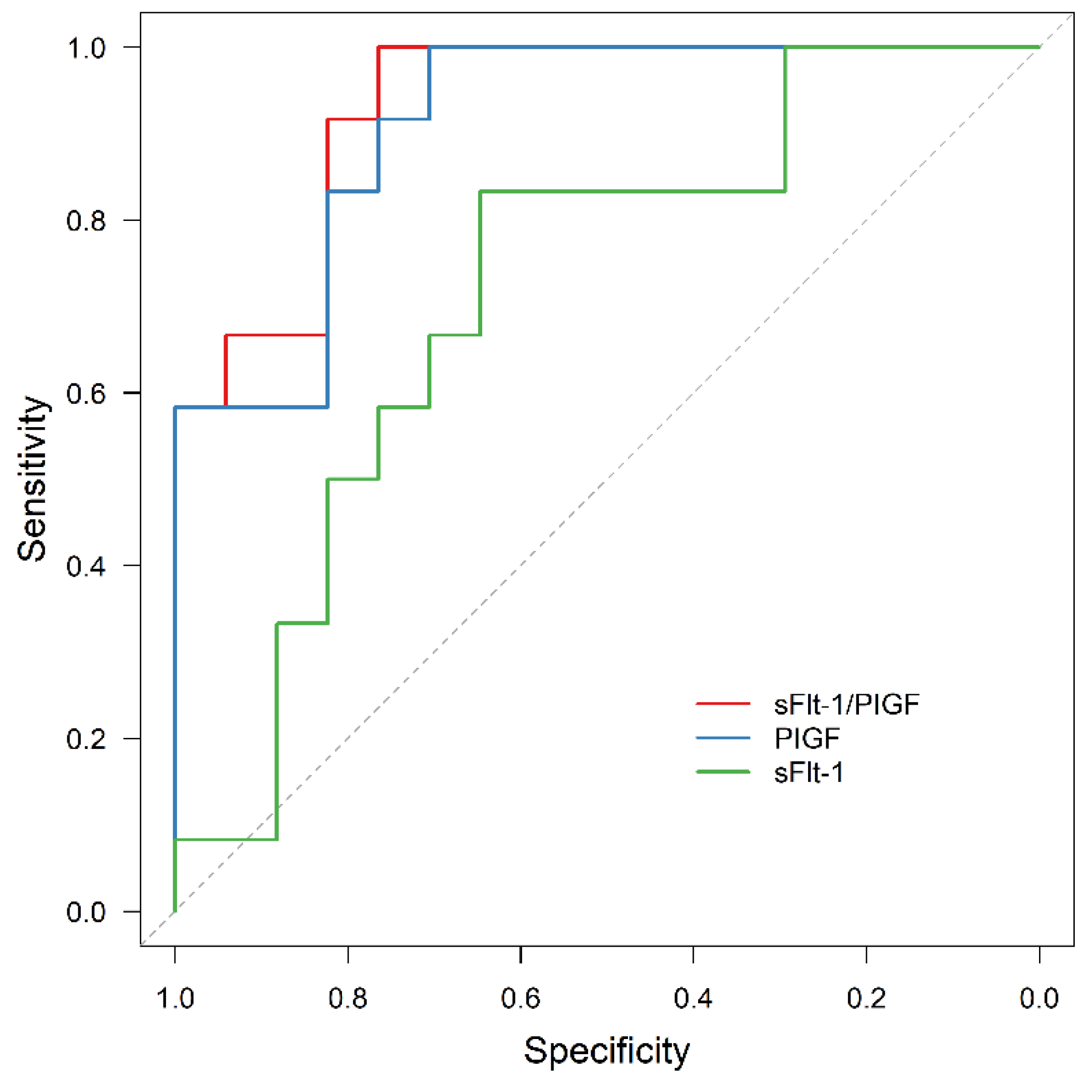
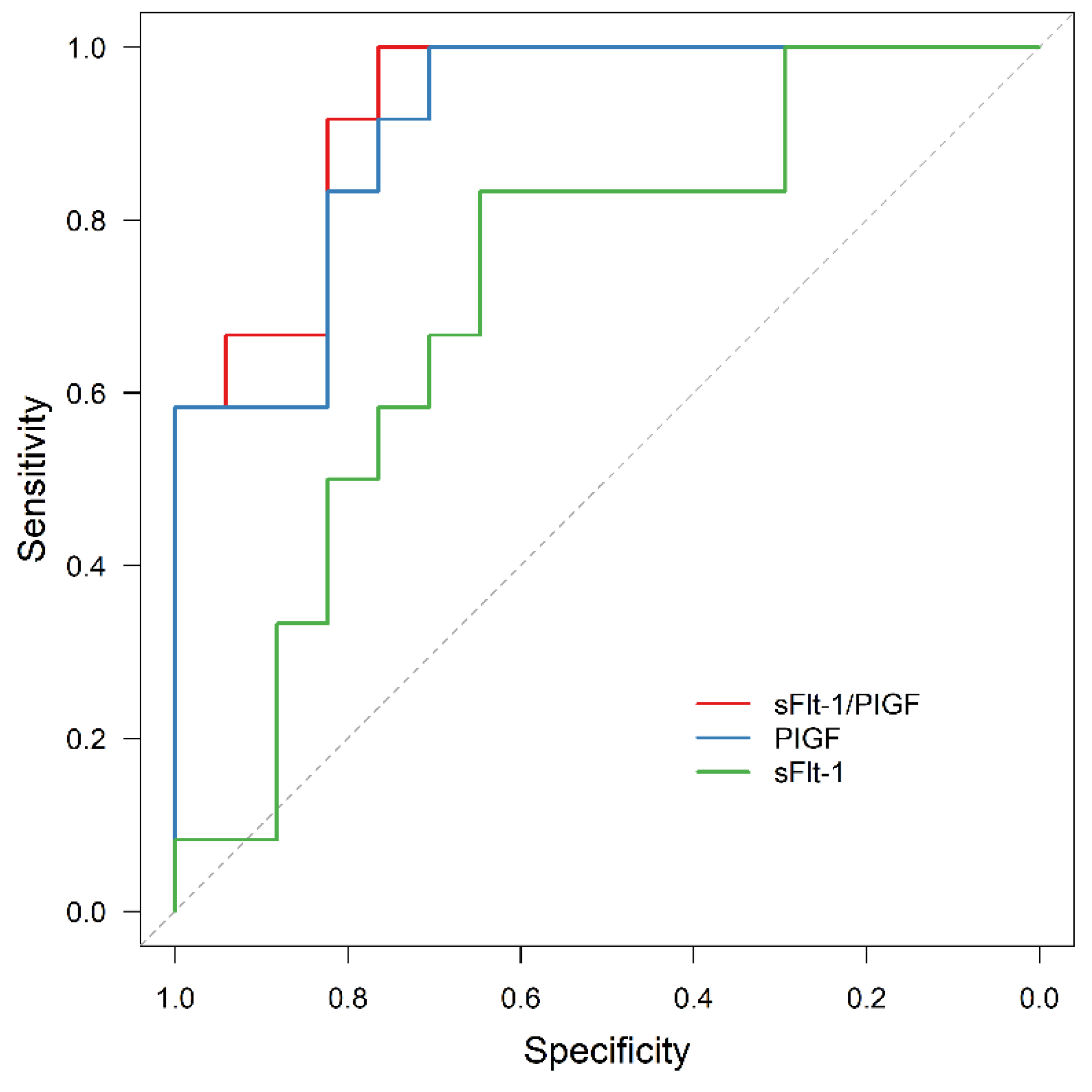
3.4. AMO Prediction by sFlt-1/PIGF
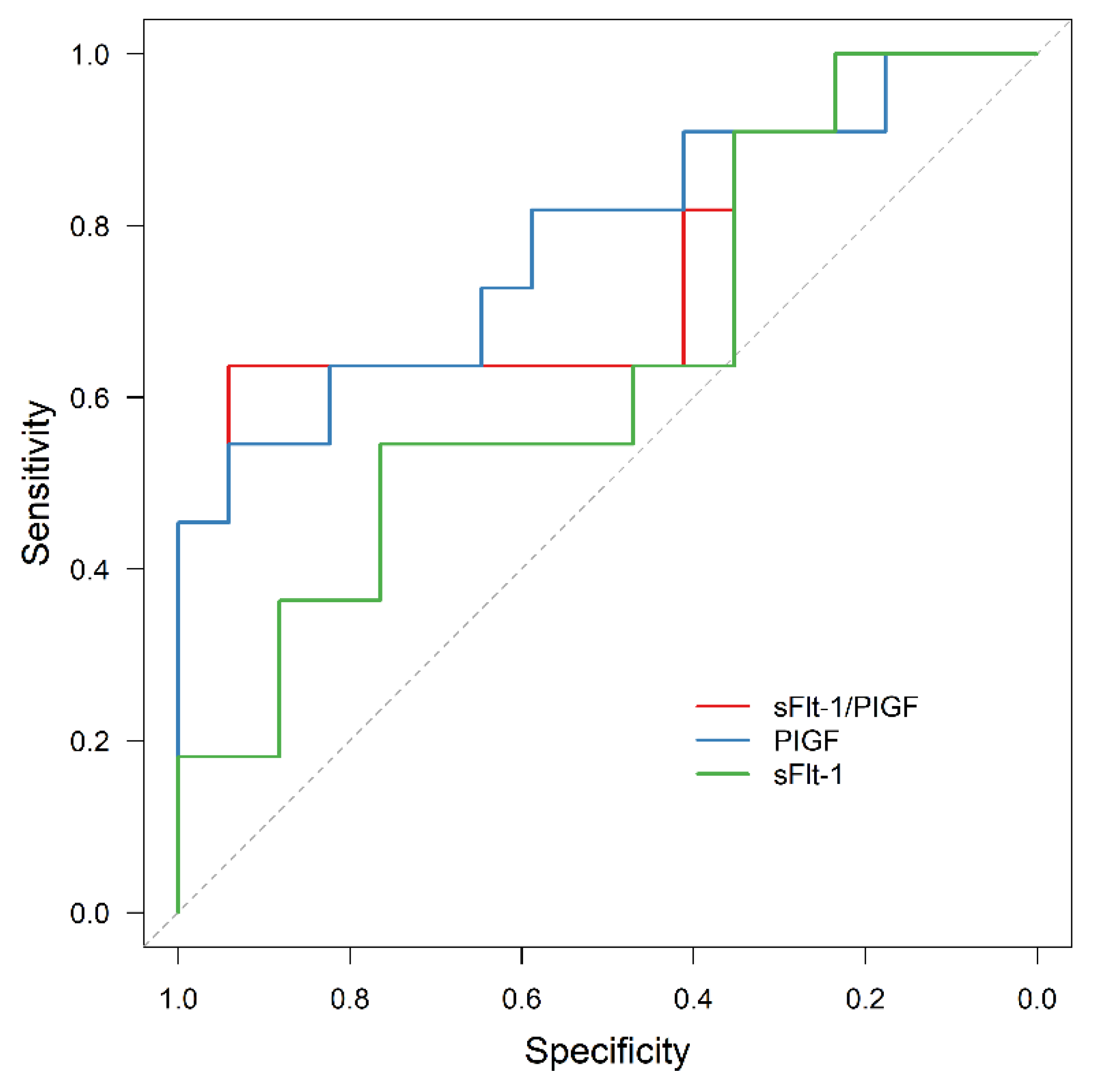
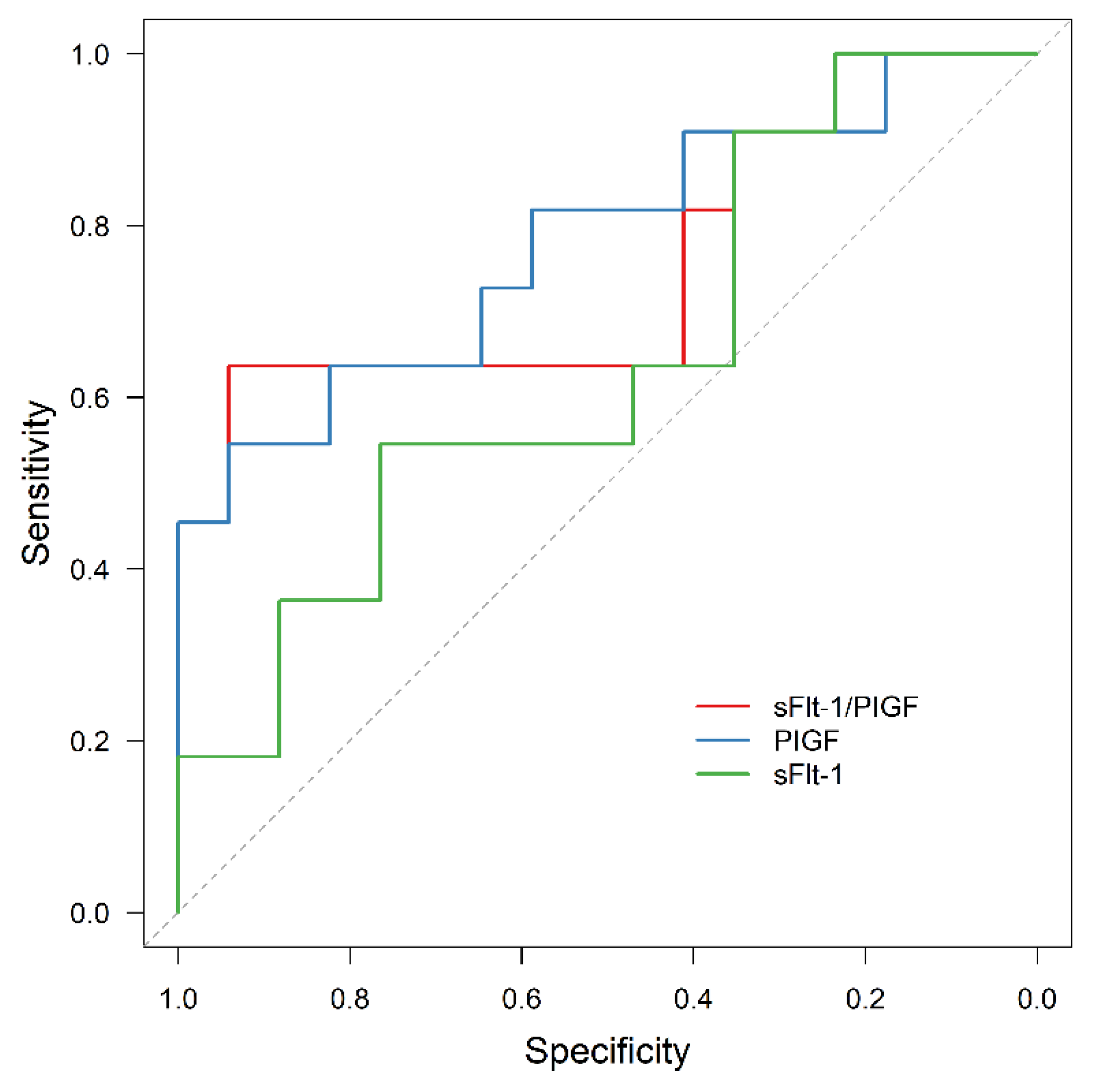
3.5. Exclusion of APO by sFlt-1/PIGF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, K.S.; Wojdyla, D.; Say, L.; Gülmezoglu, A.M.; Van Look, P.F. WHO analysis of causes of maternal death: A systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar] [CrossRef]
- van Esch, J.J.A.; van Heijst, A.F.; de Haan, A.F.J.; van der Heijden, O.W.H. Early-onset preeclampsia is associated with perinatal mortality and severe neonatal morbidity. J. Matern. Fetal Neonatal Med. 2017, 30, 2789–2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Guidelines Approved by the Guidelines Review Committee. In WHO Recommendations: Policy of Interventionist versus Expectant Management of Severe Pre-Eclampsia before Term; World Health Organization: Geneva, Switzerland, 2018.
- Tomimatsu, T.; Mimura, K.; Endo, M.; Kumasawa, K.; Kimura, T. Pathophysiology of preeclampsia: An angiogenic imbalance and long-lasting systemic vascular dysfunction. Hypertens. Res. 2017, 40, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Verlohren, S.; Herraiz, I.; Lapaire, O.; Schlembach, D.; Moertl, M.; Zeisler, H.; Calda, P.; Holzgreve, W.; Galindo, A.; Engels, T.; et al. The sFlt-1/PlGF ratio in different types of hypertensive pregnancy disorders and its prognostic potential in preeclamptic patients. Am. J. Obstet. Gynecol. 2012, 206, 58.e1–58.e8. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, R. Maternal obesity during pregnancy and cardiovascular development and disease in the offspring. Eur. J. Epidemiol. 2015, 30, 1141–1152. [Google Scholar] [CrossRef] [Green Version]
- Schaefer-Graf, U.; Ensenauer, R.; Gembruch, U.; Groten, T.; Flothkötter, M.; Hennicke, J.; Köhrle, J.; Möhler, J.; Kühnert, M.; Schmittendorf, A.; et al. Obesity and Pregnancy. Guideline of the German Society of Gynecology and Obstetrics (S3-Level, AWMF Registry No. 015-081, June 2019). Geburtshilfe Frauenheilkd 2021, 81, 279–303. [Google Scholar] [CrossRef]
- Strauss, A.; Rochow, N.; Kunze, M.; Hesse, V.; Dudenhausen, J.W.; Voigt, M. Obesity in pregnant women: A 20-year analysis of the German experience. Eur. J. Clin. Nutr. 2021, 75, 1757–1763. [Google Scholar] [CrossRef]
- Schummers, L.; Hutcheon, J.A.; Bodnar, L.M.; Lieberman, E.; Himes, K.P. Risk of Adverse Pregnancy Outcomes by Prepregnancy Body Mass Index. Obstet. Gynecol. 2015, 125, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Kwaifa, I.K.; Bahari, H.; Yong, Y.K.; Noor, S.M. Endothelial Dysfunction in Obesity-Induced Inflammation: Molecular Mechanisms and Clinical Implications. Biomolecules 2020, 10, 291. [Google Scholar] [CrossRef] [Green Version]
- Hypertensive Pregnancy Disorders: Diagnosis and Therapy. Guideline of the German Society of Gynecology and Obstetrics (S2k-Level, AMWF Registry No. 015/018, March 2019). Available online: http://www.awmf.org/leitlinien/detail/II/015-018.html (accessed on 27 April 2022).
- Verlohren, S.; Herraiz, I.; Lapaire, O.; Schlembach, D.; Zeisler, H.; Calda, P.; Sabria, J.; Markfeld-Erol, F.; Galindo, A.; Schoofs, K.; et al. New Gestational Phase–Specific Cutoff Values for the Use of the Soluble fms-Like Tyrosine Kinase-1/Placental Growth Factor Ratio as a Diagnostic Test for Preeclampsia. Hypertension 2014, 63, 346–352. [Google Scholar] [CrossRef]
- Rana, S.; Salahuddin, S.; Mueller, A.; Berg, A.H.; Thadhani, R.I.; Karumanchi, S.A. Angiogenic biomarkers in triage and risk for preeclampsia with severe features. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2018, 13, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-S.; Chen, C.-N.; Jeng, S.-F.; Su, Y.-N.; Chen, C.-Y.; Chou, H.-C.; Tsao, P.-N.; Hsieh, W.-S. The sFlt-1/PlGF ratio as a predictor for poor pregnancy and neonatal outcomes. Pediatr. Neonatol. 2017, 58, 529–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herraiz, I.; Llurba, E.; Verlohren, S.; Galindo, A.; on behalf of the Spanish Group for the Study of Angiogenic Markers in Preeclampsia. Update on the Diagnosis and Prognosis of Preeclampsia with the Aid of the sFlt-1/PlGF Ratio in Singleton Pregnancies. Fetal Diagn. Ther. 2018, 43, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karge, A.; Beckert, L.; Moog, P.; Haller, B.; Ortiz, J.U.; Lobmaier, S.M.; Abel, K.; Flechsenhar, S.; Kuschel, B.; Graupner, O. Role of sFlt-1/PIGF ratio and uterine Doppler in pregnancies with chronic kidney disease suspected with Pre-eclampsia or HELLP syndrome. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2020, 22, 160–166. [Google Scholar] [CrossRef]
- Gómez-Arriaga, P.I.; Herraiz, I.; López-Jiménez, E.A.; Escribano, D.; Denk, B.; Galindo, A. Uterine artery Doppler and sFlt-1/PlGF ratio: Prognostic value in early-onset pre-eclampsia. Ultrasound Obstet. Gynecol. 2014, 43, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Graupner, O.; Lobmaier, S.M.; Ortiz, J.U.; Karge, A.; Kuschel, B. sFlt-1/PlGF ratio for the prediction of the time of delivery. Arch. Gynecol. Obstet. 2018, 298, 567–577. [Google Scholar] [CrossRef]
- Karge, A.; Seiler, A.; Flechsenhar, S.; Haller, B.; Ortiz, J.U.; Lobmaier, S.M.; Axt-Fliedner, R.; Enzensberger, C.; Abel, K.; Kuschel, B.; et al. Prediction of adverse perinatal outcome and the mean time until delivery in twin pregnancies with suspected pre-eclampsia using sFlt-1/PIGF ratio. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2021, 24, 37–43. [Google Scholar] [CrossRef]
- Lobmaier, S.M.; Figueras, F.; Mercade, I.; Perello, M.; Peguero, A.; Crovetto, F.; Ortiz, J.U.; Crispi, F.; Gratacos, E. Angiogenic factorsvsDoppler surveillance in the prediction of adverse outcome among late-pregnancy small-for- gestational-age fetuses. Ultrasound Obstet. Gynecol. 2014, 43, 533–540. [Google Scholar] [CrossRef]
- Dröge, L.; Herraiz, I.; Zeisler, H.; Schlembach, D.; Stepan, H.; Küssel, L.; Henrich, W.; Galindo, A.; Verlohren, S. Maternal serum sFlt-1/PlGF ratio in twin pregnancies with and without pre-eclampsia in comparison with singleton pregnancies. Ultrasound Obstet. Gynecol. 2015, 45, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Jääskeläinen, T.; Finnpec, F.T.; Heinonen, S.; Hämäläinen, E.; Pulkki, K.; Romppanen, J.; Laivuori, H. Impact of obesity on angiogenic and inflammatory markers in the Finnish Genetics of Pre-eclampsia Consortium (FINNPEC) cohort. Int. J. Obes. 2019, 43, 1070–1081. [Google Scholar] [CrossRef] [Green Version]
- Zera, C.A.; Seely, E.W.; Wilkins-Haug, L.E.; Lim, K.-H.; Parry, S.I.; McElrath, T.F. The association of body mass index with serum angiogenic markers in normal and abnormal pregnancies. Am. J. Obstet. Gynecol. 2014, 211, 247.e1–247.e7. [Google Scholar] [CrossRef] [PubMed]
- Graupner, O.; Karge, A.; Flechsenhar, S.; Seiler, A.; Haller, B.; Ortiz, J.U.; Lobmaier, S.M.; Axt-Fliedner, R.; Enzensberger, C.; Abel, K.; et al. Role of sFlt-1/PlGF ratio and feto-maternal Doppler for the prediction of adverse perinatal outcome in late-onset pre-eclampsia. Arch. Gynecol. Obstet. 2020, 301, 375–385. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstet. Gynecol. 2019, 133, e1–e25. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar] [CrossRef]
- Weinstein, L. Syndrome of hemolysis, elevated liver enzymes, and low platelet count: A severe consequence of hypertension in pregnancy. Am. J. Obstet. Gynecol. 1982, 142, 159–167. [Google Scholar] [CrossRef]
- Von Dadelszen, P.; Magee, L.A.; Roberts, J.M. Subclassification of Preeclampsia. Hypertens. Pregnancy 2003, 22, 143–148. [Google Scholar] [CrossRef]
- Duffy, J.M.; Cairns, A.E.; Richards-Doran, D.; Hooft, J.V.; Gale, C.; Brown, M.; Chappell, L.; Grobman, W.A.; Fitzpatrick, R.; Karumanchi, S.A.; et al. A core outcome set for pre-eclampsia research: An international consensus development study. BJOG 2020, 127, 1516–1526. [Google Scholar] [CrossRef]
- Voigt, M.; Rochow, N.; Schneider, K.T.M.; Hagenah, H.-P.; Scholz, R.; Hesse, V.; Wittwer-Backofen, U.; Straube, S.; Olbertz, D. New percentile values for the anthropometric dimensions of singleton neonates: Analysis of perinatal survey data of 2007–2011 from all 16 states of Germany. Z. Geburtshilfe Neonatol. 2014, 218, 210–217. [Google Scholar] [CrossRef]
- Stepan, H.; Herraiz, I.; Schlembach, D.; Verlohren, S.; Brennecke, S.; Chantraine, F.; Klein, E.; Lapaire, O.; Llurba, E.; Ramoni, A.; et al. Implementation of the sFlt-1/PlGF ratio for prediction and diagnosis of pre-eclampsia in singleton pregnancy: Implications for clinical practice. Ultrasound Obstet. Gynecol. 2015, 45, 241–246. [Google Scholar] [CrossRef]
- WHO. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO Technical Report Series; WHO: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating charac-teristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Graupner, O.; Enzensberger, C. Prediction of Adverse Pregnancy Outcome Related to Placental Dysfunction Using the sFlt-1/PlGF Ratio: A Narrative Review. Geburtshilfe Frauenheilkd. 2021, 81, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Saleh, L.; Alblas, M.M.; Nieboer, D.; Neuman, R.I.; Vergouwe, Y.; Brussé, I.A.; Duvekot, J.J.; Steyerberg, E.W.; Versendaal, H.J.; Danser, A.H.J.; et al. Prediction of pre-eclampsia-related complications in women with suspected or confirmed pre-eclampsia: Development and internal validation of clinical prediction model. Ultrasound Obstet. Gynecol. 2021, 58, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Stolz, M.; Zeisler, H.; Heinzl, F.; Binder, J.; Farr, A. An sFlt-1:PlGF ratio of 655 is not a reliable cut-off value for predicting perinatal outcomes in women with preeclampsia. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2018, 11, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Simón, E.; Permuy, C.; Sacristán, L.; Zamoro-Lorenci, M.J.; Villalaín, C.; Galindo, A.; Herraiz, I. sFlt-1/PlGF ratio for the prediction of delivery within 48 hours and adverse outcomes in expectantly managed early-onset preeclampsia. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2020, 22, 17–23. [Google Scholar] [CrossRef]
- Saleh, L.; Tahitu, S.I.; Danser, A.J.; Meiracker, A.H.V.D.; Visser, W. The predictive value of the sFlt-1/PlGF ratio on short-term absence of preeclampsia and maternal and fetal or neonatal complications in twin pregnancies. Pregnancy Hypertens. Int. J. Women’s Cardiovasc. Health 2018, 14, 222–227. [Google Scholar] [CrossRef]
- Zeisler, H.; Llurba, E.; Chantraine, F.; Vatish, M.; Staff, A.C.; Sennström, M.; Olovsson, M.; Brennecke, S.P.; Stepan, H.; Allegranza, D.; et al. Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia. N. Engl. J. Med. 2016, 374, 13–22. [Google Scholar] [CrossRef]
- Suwaki, N.; Masuyama, H.; Nakatsukasa, H.; Masumoto, A.; Sumida, Y.; Takamoto, N.; Hiramatrsu, Y. Hypoadiponectinemia and circulating angiogenic factors in overweight patients complicated with pre-eclampsia. Am. J. Obstet. Gynecol. 2006, 195, 1687–1692. [Google Scholar] [CrossRef]
- Mijal, R.S.; Holzman, C.B.; Rana, S.; Karumanchi, S.A.; Wang, J.; Sikorskii, A. Midpregnancy levels of angiogenic markers in relation to maternal characteristics. Am. J. Obstet. Gynecol. 2011, 204, 244.e1–244.e12. [Google Scholar] [CrossRef] [Green Version]
- Faupel-Badger, J.M.; Staff, A.C.; Thadhani, R.; Powe, C.E.; Potischman, N.; Hoover, R.N.; Troisi, R. Maternal angiogenic profile in pregnancies that remain normotensive. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 158, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Heimberger, S.; Mueller, A.; Ratnaparkhi, R.; Perdigao, J.L.; Rana, S. Angiogenic factor abnormalities and risk of peripartum complications and prematurity among urban predominantly obese parturients with chronic hypertension. Pregnancy Hypertens. Int. J. Women Cardiovasc. Health 2020, 20, 124–130. [Google Scholar] [CrossRef]
- Spradley, F.T.; Palei, A.C.; Granger, J.P. Obese melanocortin-4 receptor-deficient rats exhibit augmented angiogenic balance and vasorelaxation during pregnancy. Physiol. Rep. 2013, 1, e00081. [Google Scholar] [CrossRef] [PubMed]
- Spradley, F.T.; Palei, A.C.; Granger, J.P. Increased risk for the development of preeclampsia in obese pregnancies: Weighing in on the mechanisms. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R1326–R1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herse, F.; Fain, J.N.; Janke, J.; Engeli, S.; Kuhn, C.; Frey, N.; Weich, H.A.; Bergmann, A.; Kappert, K.; Karumanchi, S.A.; et al. Adipose Tissue-Derived Soluble Fms-Like Tyrosine Kinase 1 Is an Obesity-Relevant Endogenous Paracrine Adipokine. Hypertension 2011, 58, 37–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariman, E.C.M.; Wang, P. Adipocyte extracellular matrix composition, dynamics and role in obesity. Cell. Mol. Life Sci. 2010, 67, 1277–1292. [Google Scholar] [CrossRef] [Green Version]
- Lisonkova, S.; Razaz, N.; Sabr, Y.; Muraca, G.M.; Boutin, A.; Mayer, C.; Joseph, K.; Kramer, M.S. Maternal risk factors and adverse birth outcomes associated with HELLP syndrome: A population-based study. BJOG 2020, 127, 1189–1198. [Google Scholar] [CrossRef]
- Rana, S.; Schnettler, W.T.; Powe, C.; Wenger, J.; Salahuddin, S.; Cerdeira, A.S.; Verlohren, S.; Perschel, F.H.; Arany, Z.; Lim, K.-H.; et al. Clinical characterization and outcomes of preeclampsia with normal angiogenic profile. Hypertens. Pregnancy 2013, 32, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Mbah, A.K.; Kornosky, J.L.; Kristensen, S.; August, E.M.; Alio, A.P.; Marty, P.J.; Belogolovkin, V.; Bruder, K.; Salihu, H.M. Super-obesity and risk for early and late pre-eclampsia. BJOG 2010, 117, 997–1004. [Google Scholar] [CrossRef]
- Klein, E.; Schlembach, D.; Ramoni, A.; Langer, E.; Bahlmann, F.; Grill, S.; Schaffenrath, H.; van der Does, R.; Messinger, D.; Verhagen-Kamerbeek, W.D.; et al. Influence of the sFlt-1/PlGF Ratio on Clinical Decision-Making in Women with Sus-pected Preeclampsia. PLoS ONE 2016, 11, e0156013. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | BMI < 25 kg/m2 n = 84 | BMI > 25–29.9 kg/m2 n = 29 | BMI ≥ 30 kg/m2 n = 28 | p-Value |
|---|---|---|---|---|
| Age at diagnosis | 33.5 (±5.4) | 34.1 (±5.7) | 33.2 (±4.6) | 0.608 |
| BMI | 21.2 (±1.8) | 27.3 (±1.5) | 34.1 (±3.9) | <0.001 *** |
| Weight gain during pregnancy (in kg) | 13.5 (±6.1) | 12.6 (±5.4) | 10.9 (±7.0) | 0.216 |
| Gestational age at diagnosis | 34.8 (±3.8) | 34.8 (±3.9) | 34.5 (±3.3) | 0.680 |
| sFlt-1/PIGF level at diagnosis | 125.1 (IQR: 64.4–213.1) | 116.0 (IQR: 45.3–233.0) | 99.30 (IQR: 30.36–187.0) | 0.275 |
| PIGF level at diagnosis | 93.9 (IQR: 54.6–93.9) | 86.3 (IQR: 46.1–130.4) | 89.35 (IQR: 51.0–130.9) | 0.810 |
| sFlt-1 level at diagnosis | 12,024.8 (IQR: 7472.0–13,544.8) | 8756.0 (IQR: 5708.5–13,040.0) | 7014.0 (IQR: 3668.6–11,347.3) | 0.003 ** |
| Gestational age at delivery | 35.5 (±3.3) | 35.7 (±3.9) | 35.9 (±3.0) | 0.684 |
| Nullipara | 57 (68%) | 17 (58%) | 17 (61%) | 0.396 |
| ASS prophylaxis | 10 (12%) | 11 (38%) | 9 (32%) | 0.005 * |
| Chronic hypertension | 8 (10%) | 3 (10%) | 3 (11%) | 0.844 |
| Early-onset PE/HELLP | 24/84 (29%) | 10/28 (36%) | 10/29 (35%) | 0.430 |
| Late-onset PE/HELLP | 60 (71%) | 19 (66%) | 17 (61%) | 0.272 |
| RDS Prophylaxis | 27 (32%) | 8 (28%) | 11 (39%) | 0.637 |
| Status after PE/HELLP/FGR | 16 (19%) | 9 (31%) | 8 (29%) | 0.205 |
| Magnesium sulfate prophylaxis | 44 (52%) | 16 (55%) | 15 (54%) | 0.868 |
| Perinatal Outcome | BMI < 25n = 84 | BMI > 25–29.9 kg/m2 n = 29 | BMI ≥ 30 kg/m2n = 28 | p-Value |
|---|---|---|---|---|
| APO | 46/84 (55%) | 12/29 (41%) | 11/28 (39%) | 0.110 |
| Respiratory support | 27/84 (33%) | 8/29 (28%) | 7/28 (25%) | 0.421 |
| Admission to NICU | 34/84 (41%) | 10/29 (35%) | 11/28 (39%) | 0.764 |
| Birthweight (g) | 2243.2 (±48.4) | 2422.1 (±932.5) | 2456.3 (±841.3) | 0.404 |
| Birthweight < 3. centile | 9/84 (11%) | 2/29 (7%) | 2/28 (7%) | 0.751 |
| Neonatal mortality | 0/84 (0%) | 0/29 (0%) | 1/28 (4%) | 0.080 |
| Fetal growth restriction | 24/84 (29%) | 7/29 (24%) | 5/28 (18%) | 0.257 |
| Seizures | 1/84 (1%) | 2/29 (7%) | 0/28 (0%) | 0.167 |
| AMO | 29/84 (35%) | 3/29 (10%) | 4/28 (14%) | 0.010 * |
| Early-onset HELLP | 8/84 (10%) | 0/29 (0%) | 2/28 (7%) | 0.406 |
| Late-onset HELLP | 7/84 (8%) | 1/29 (3%) | 1/28 (4%) | 0.297 |
| Postpartum haemorrhage | 1/84 (1%) | 0/29 (0%) | 1/28 (4%) | 0.005 * |
| Eclampsia | 0/84 (0%) | 1/29 (3%) | 0/28 (0%) | 0.619 |
| Acute kidney injury | 12/84 (14%) | 2/29 (7%) | 1/28 (4%) | 0.085 |
| Abruption | 3/84 (4%) | 0/29 (0%) | 0/28 (0%) | 0.187 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karge, A.; Desing, L.; Haller, B.; Ortiz, J.U.; Lobmaier, S.M.; Kuschel, B.; Graupner, O. Performance of sFlt-1/PIGF Ratio for the Prediction of Perinatal Outcome in Obese Pre-Eclamptic Women. J. Clin. Med. 2022, 11, 3023. https://doi.org/10.3390/jcm11113023
Karge A, Desing L, Haller B, Ortiz JU, Lobmaier SM, Kuschel B, Graupner O. Performance of sFlt-1/PIGF Ratio for the Prediction of Perinatal Outcome in Obese Pre-Eclamptic Women. Journal of Clinical Medicine. 2022; 11(11):3023. https://doi.org/10.3390/jcm11113023
Chicago/Turabian StyleKarge, Anne, Linus Desing, Bernhard Haller, Javier U. Ortiz, Silvia M. Lobmaier, Bettina Kuschel, and Oliver Graupner. 2022. "Performance of sFlt-1/PIGF Ratio for the Prediction of Perinatal Outcome in Obese Pre-Eclamptic Women" Journal of Clinical Medicine 11, no. 11: 3023. https://doi.org/10.3390/jcm11113023
APA StyleKarge, A., Desing, L., Haller, B., Ortiz, J. U., Lobmaier, S. M., Kuschel, B., & Graupner, O. (2022). Performance of sFlt-1/PIGF Ratio for the Prediction of Perinatal Outcome in Obese Pre-Eclamptic Women. Journal of Clinical Medicine, 11(11), 3023. https://doi.org/10.3390/jcm11113023