
Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy

 , , ,
, , , 

Abstract
1. Introduction
2. Current UK Management of Locally Advanced Pancreatic Cancer (LAPC)
2.1. Chemotherapy in Unresectable Locally Advanced Pancreatic Cancer (LAPC)
2.2. IRE Treatment for Locally Advanced Pancreas Cancer
2.3. Immunotherapy in Pancreatic Cancer
3. Systematic Review of IRE in Human Pancreas Cancer
4. Clinical Outcomes of IRE for LAPC
5. Complications of Pancreas IRE Therapy
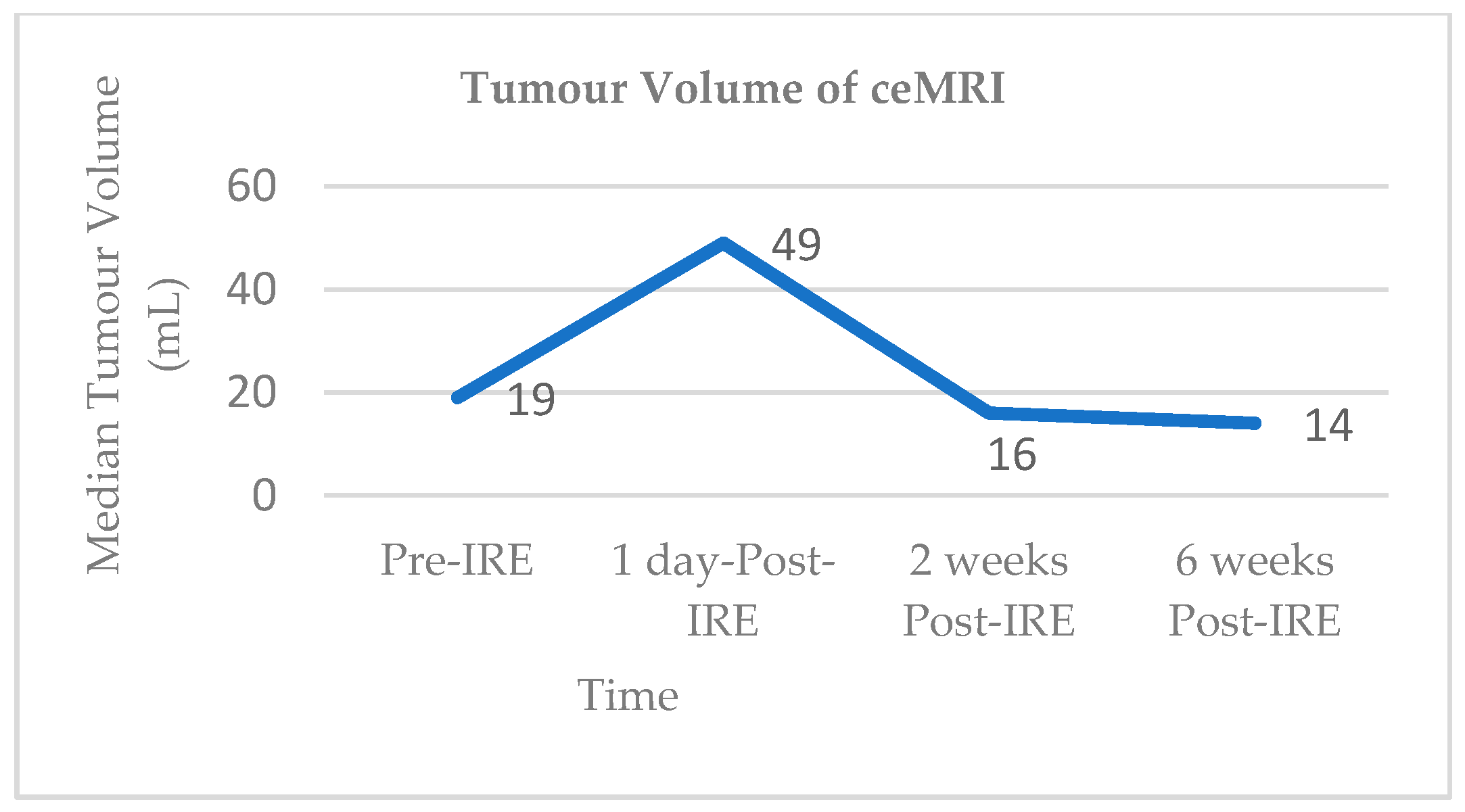
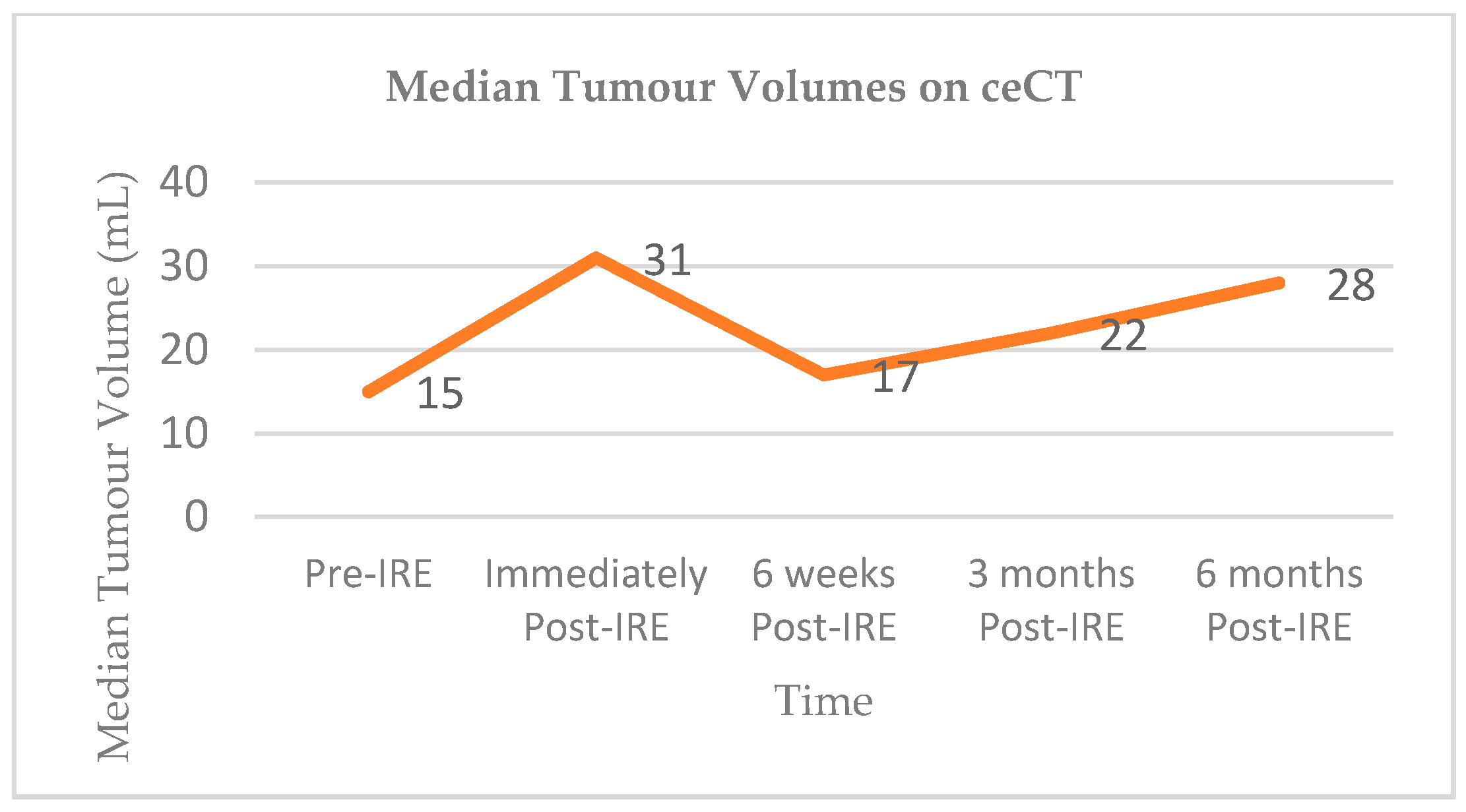
6. Radiological Response to Pancreas IRE
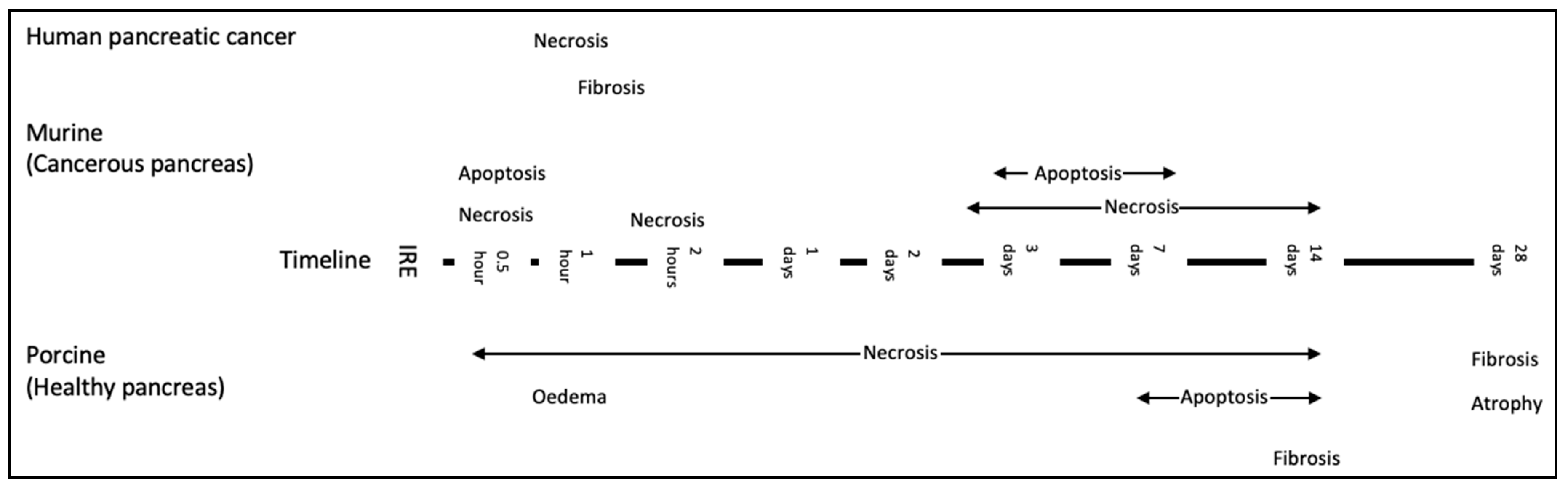
7. Pathological Response to Pancreas IRE Therapy and Mechanism of Action
7.1. IRE Studies Involving Normal Porcine Pancreas
7.2. IRE in Animal Models of Pancreas Cancer
7.3. Human Models and IRE
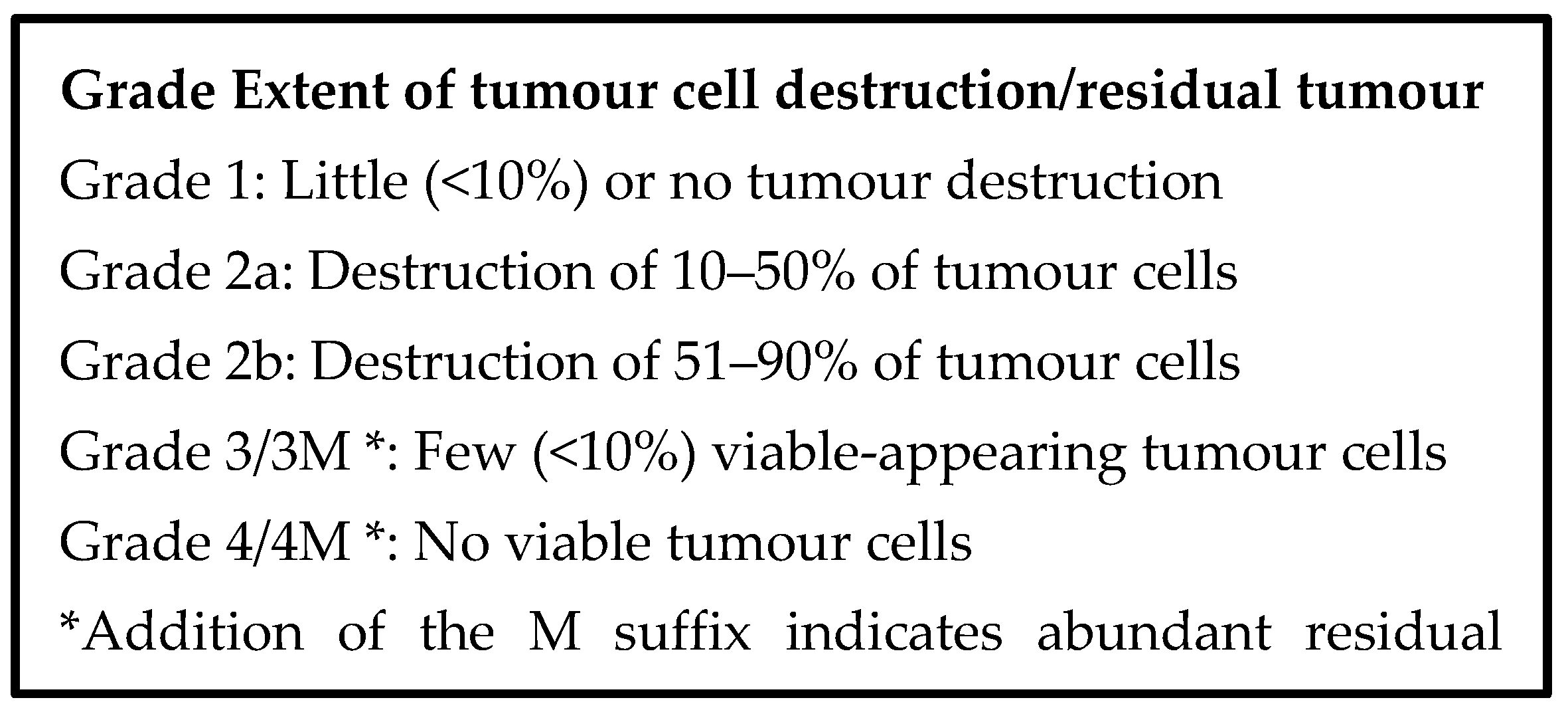
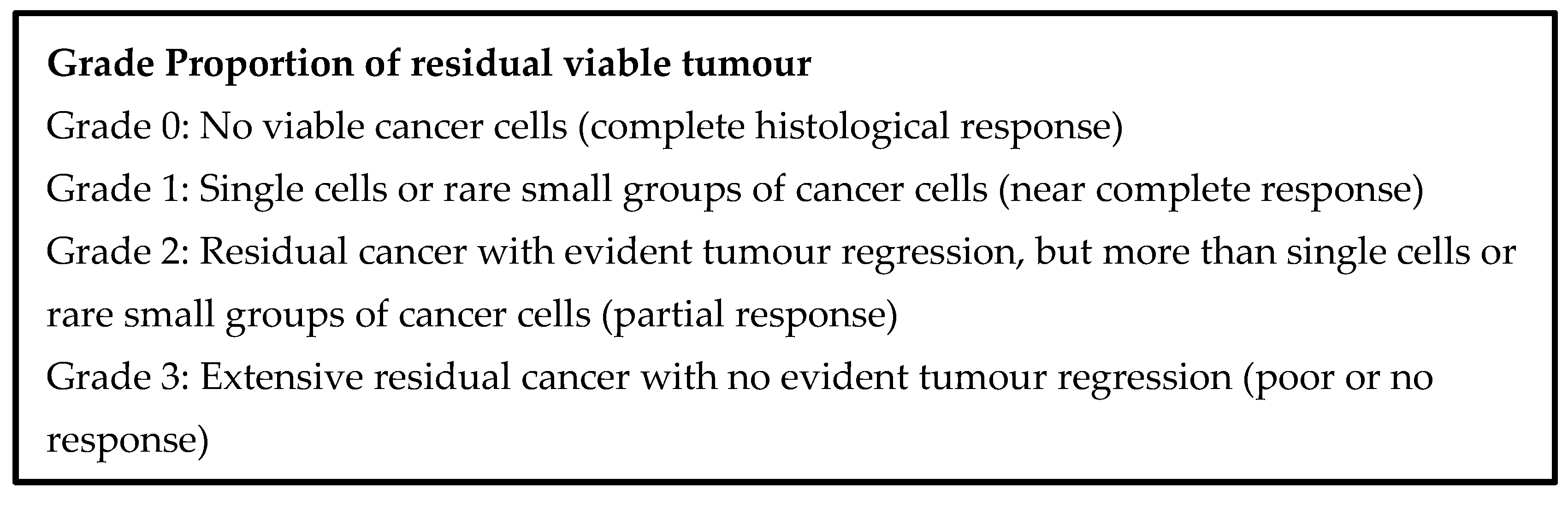
8. Pathological Changes in Human Pancreas Cancer Following IRE
9. New Approaches to Pancreas IRE
9.1. EUS Guided Pancreas IRE
9.2. Paddles Rather Than Electrodes for IRE Therapy
10. Chemosensitisation Following Electroporation
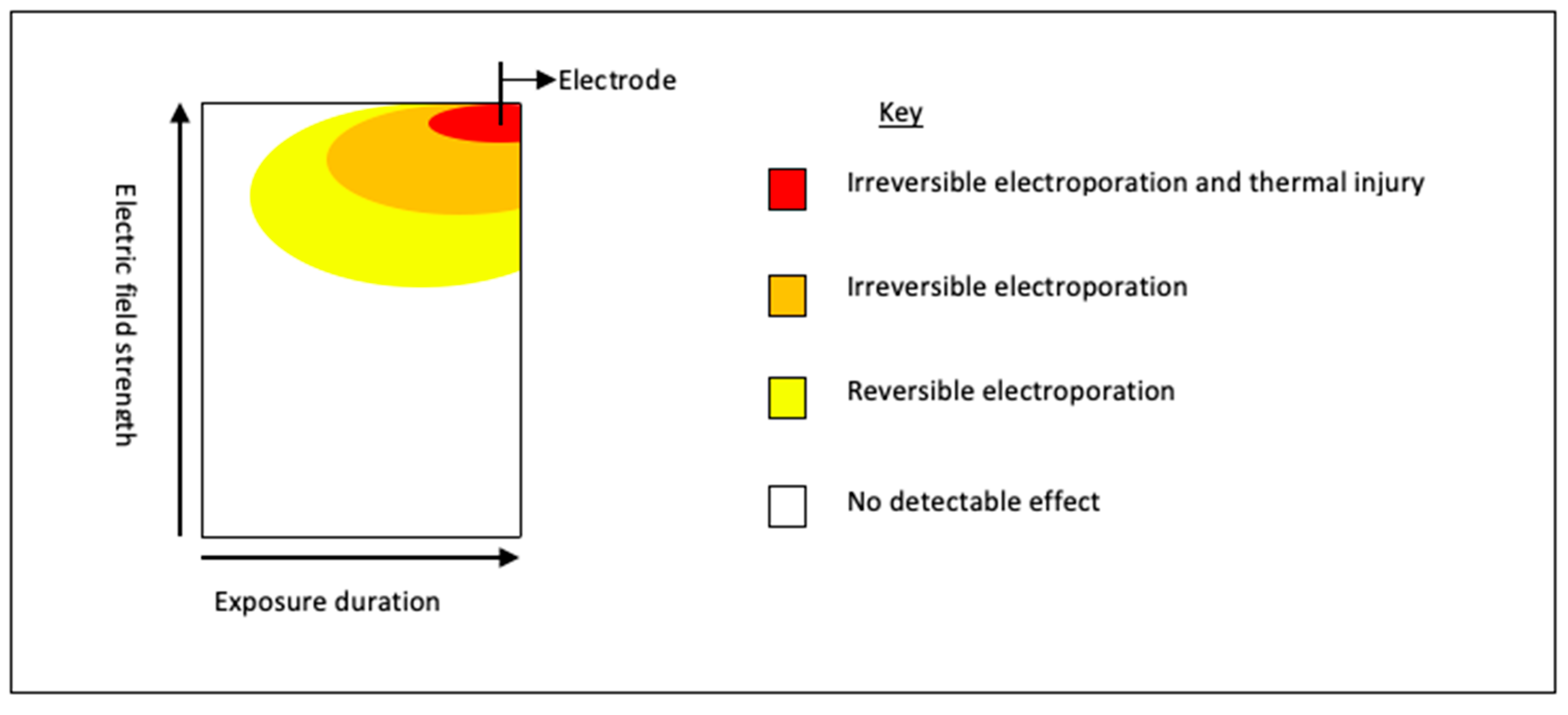
10.1. Reversible Electroporation
10.2. Irreversible Electroporation
11. Immune Landscape in the Pancreas, in Health and Disease
12. Altering the Systemic Immune Response to Pancreatic Cancer with IRE
13. Combination Therapies for Pancreatic Cancer: Combining Immunotherapeutic Approaches with IRE
14. Discussion and Future Directions
14.1. Clinical Outcomes of IRE for LAPC
14.2. Radiological Response to Pancreas IRE
14.3. Pathological Changes Following Pancreas IRE Treatment
14.4. New Approaches to Pancreas IRE
14.5. IRE Synergy with Chemotherapy
14.6. Immunological Response to IRE and Synergy with Immunotherapy
15. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lafranceschina, S.; Brunetti, O.; DelVecchio, A.; Conticchio, M.; Ammendola, M.; Currò, G.; Piardi, T.; De’Angelis, N.; Silvestris, N.; Memeo, R. Systematic Review of Irreversible Electroporation Role in Management of Locally Advanced Pancreatic Cancer. Cancers 2019, 11, 1718. [Google Scholar] [CrossRef]
- Geboers, B.; Scheffer, H.J.; Graybill, P.M.; Ruarus, A.H.; Nieuwenhuizen, S.; Puijk, R.S.; Tol, P.M.V.D.; Davalos, R.V.; Rubinsky, B.; De Gruijl, T.D.; et al. High-Voltage Electrical Pulses in Oncology: Irreversible Electroporation, Electrochemotherapy, Gene Electrotransfer, Electrofusion, and Electroimmunotherapy. Radiology 2020, 295, 254–272. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Reese, T. Changes in membrane structure induced by electroporation as revealed by rapid-freezing electron microscopy. Biophys. J. 1990, 58, 1–12. [Google Scholar] [CrossRef]
- Lee, E.W.; Wong, D.; Prikhodko, S.V.; Perez, A.; Tran, C.; Loh, C.T.; Kee, S.T. Electron Microscopic Demonstration and Evaluation of Irreversible Electroporation-Induced Nanopores on Hepatocyte Membranes. J. Vasc. Interv. Radiol. 2012, 23, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Choi, H.S.; Kim, E.S.; Keum, B.; Seo, Y.S.; Jeen, Y.T.; Lee, H.S.; Chun, H.J.; Um, S.H.; Kim, C.D. Characterization of irreversible electroporation on the stomach: A feasibility study in rats. Sci. Rep. 2019, 9, 9094. [Google Scholar] [CrossRef] [PubMed]
- Faroja, M.; Ahmed, M.; Appelbaum, L.; Ben-David, E.; Moussa, M.; Sosna, J.; Nissenbaum, I.; Goldberg, S.N. Irreversible Electroporation Ablation: Is All the Damage Nonthermal? Radiology 2013, 266, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Ferri, K.F.; Kroemer, G. Mitochondria-the suicide organelles. BioEssays 2001, 23, 111–115. [Google Scholar] [CrossRef]
- Lambert, A.; Schwarz, L.; Borbath, I.; Henry, A.; Van Laethem, J.-L.; Malka, D.; Ducreux, M.; Conroy, T. An update on treatment options for pancreatic adenocarcinoma. Ther. Adv. Med Oncol. 2019, 11. [Google Scholar] [CrossRef]
- Maor, E.; Ivorra, A.; Rubinsky, B. Non Thermal Irreversible Electroporation: Novel Technology for Vascular Smooth Muscle Cells Ablation. PLoS ONE 2009, 4, e4757. [Google Scholar] [CrossRef]
- Maor, E.; Ivorra, A.; Leor, J.; Rubinsky, B. The Effect of Irreversible Electroporation on Blood Vessels. Technol. Cancer Res. Treat. 2007, 6, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.W.; Loh, C.T.; Kee, S.T. Imaging Guided Percutaneous Irreversible Electroporation: Ultrasound and Immunohistological Correlation. Technol. Cancer Res. Treat. 2007, 6, 287–294. [Google Scholar] [CrossRef]
- Li, Y.; Brown, R.E.; Martin, R.C. Incomplete thermal ablation of hepatocellular carcinoma: Effects on tumor proliferation. J. Surg. Res. 2013, 181, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Rowan, N.; MacGregor, S.; Anderson, J.; Fouracre, R.; Farish, O. Pulsed electric field inactivation of diarrhoeagenic Bacillus cereus through irreversible electroporation. Lett. Appl. Microbiol. 2000, 31, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Xie, X.; Zhao, W.; Yao, J.; Kong, D.; Boehm, A.B.; Cui, Y. Static Electricity Powered Copper Oxide Nanowire Microbicidal Electroporation for Water Disinfection. Nano Lett. 2014, 14, 5603–5608. [Google Scholar] [CrossRef] [PubMed]
- Sale, A.; Hamilton, W. Effects of high electric fields on micro-organisms. 3. Lysis of erythrocytes and protoplasts. Biochim. Biophys. Acta 1968, 163, 37–43. [Google Scholar] [CrossRef]
- Sugar, I.P.; Neumann, E. Stochastic model for electric field-induced membrane pores. Electroporation. Biophys. Chem. 1984, 19, 211–225. [Google Scholar] [CrossRef]
- Rosazza, C.; Meglic, S.H.; Zumbusch, A.; Rols, M.P.; Miklavcic, D. Gene Electrotransfer: A Mechanistic Perspective. Curr. Gene Ther. 2016, 16, 98–129. [Google Scholar] [CrossRef]
- Orlowski, S.; Belehradek, J.; Paoletti, C.; Mir, L.M. Transient electropermeabilization of cells in culture. Biochem. Pharmacol. 1988, 37, 4727–4733. [Google Scholar] [CrossRef]
- Davalos, R.V.; Mir, L.M.; Rubinsky, B. Tissue ablation with irreversible electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef]
- Al-Sakere, B.; André, F.; Bernat, C.; Connault, E.; Opolon, P.; Davalos, R.V.; Rubinsky, B.; Mir, L.M. Tumor Ablation with Irreversible Electroporation. PLoS ONE 2007, 2, e1135. [Google Scholar] [CrossRef]
- Lee, E.W.; Wong, D.; Tafti, B.A.; Prieto, V.; Totonchy, M.; Hilton, J.; Dry, S.; Cho, S.; Loh, C.T.; Kee, S.T. Irreversible Electroporation in Eradication of Rabbit VX2 Liver Tumor. J. Vasc. Interv. Radiol. 2012, 23, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Leor, J.; Rubinsky, B. Cancer Cells Ablation with Irreversible Electroporation. Technol. Cancer Res. Treat. 2005, 4, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, K.P.; Wolf, F.; Noble, L.; Winn, B.; Resnick, M.; Dupuy, D.E. Irreversible electroporation of the pancreas in swine: A pilot study. HPB 2010, 12, 348–351. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fritz, S.; Sommer, C.M.; Vollherbst, D.; Wachter, M.F.; Longerich, T.; Sachsenmeier, M.; Knapp, J.; Radeleff, B.A.; Werner, J. Irreversible Electroporation of the Pancreas Is Feasible and Safe in a Porcine Survival Model. Pancreas 2015, 44, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Au, J.T.; Kingham, T.; Jun, K.; Haddad, D.; Gholami, S.; Mojica, K.; Monette, S.; Ezell, P.; Fong, Y. Irreversible electroporation ablation of the liver can be detected with ultrasound B-mode and elastography. Surgery 2013, 153, 787–793. [Google Scholar] [CrossRef]
- Choi, Y.-S.; Kim, H.B.; Chung, J.; Kim, H.S.; Yi, J.H.; Park, J.K. Preclinical Analysis of Irreversible Electroporation on Rat Liver Tissues Using a Microfabricated Electroporator. Tissue Eng. Part C Methods 2010, 16, 1245–1253. [Google Scholar] [CrossRef]
- Sommer, C.M.; Fritz, S.; Wachter, M.F.; Vollherbst, D.; Stampfl, U.; Bellemann, N.; Gockner, T.; Mokry, T.; Gnutzmann, D.; Schmitz, A.; et al. Irreversible Electroporation of the Pig Kidney with Involvement of the Renal Pelvis: Technical Aspects, Clinical Outcome, and Three-dimensional CT Rendering for Assessment of the Treatment Zone. J. Vasc. Interv. Radiol. 2013, 24, 1888–1897. [Google Scholar] [CrossRef]
- Martin, R.C., 2nd; McFarland, K.; Ellis, S.; Velanovich, V. Irreversible electroporation therapy in the management of locally advanced pancreatic adenocarcinoma. J. Am. Coll. Surg. 2012, 215, 361–369. [Google Scholar] [CrossRef]
- Belfiore, M.P.; Ronza, F.M.; Romano, F.; Ianniello, G.P.; De Lucia, G.; Gallo, C.; Marsicano, C.; Di Gennaro, T.L.; Belfiore, G. Percutaneous CT-guided irreversible electroporation followed by chemotherapy as a novel neoadjuvant protocol in locally advanced pancreatic cancer: Our preliminary experience. Int. J. Surg. 2015, 21 (Suppl. S1), S34–S39. [Google Scholar] [CrossRef]
- Flak, R.V.; Stender, M.T.; Jensen, T.M.; Andersen, K.L.; Henriksen, S.D.; Mortensen, P.B.; Sall, M.; Thorlacius-Ussing, O. Treatment of locally advanced pancreatic cancer with irreversible electroporation–A Danish single center study of safety and feasibility. Scand. J. Gastroenterol. 2019, 54, 252–258. [Google Scholar] [CrossRef]
- Holland, M.M.; Bhutiani, N.; Kruse, E.J.; Weiss, M.J.; Christein, J.D.; White, R.R.; Huang, K.-W.; Martin, R.C. A prospective, multi-institution assessment of irreversible electroporation for treatment of locally advanced pancreatic adenocarcinoma: Initial outcomes from the AHPBA pancreatic registry. HPB 2019, 21, 1024–1031. [Google Scholar] [CrossRef]
- Kluger, M.D.; Epelboym, I.; Schrope, B.A.; Mahendraraj, K.; Hecht, E.M.; Susman, J.; Weintraub, J.L.; Chabot, J.A. Single-Institution Experience with Irreversible Electroporation for T4 Pancreatic Cancer: First 50 Patients. Ann. Surg. Oncol. 2016, 23, 1736–1743. [Google Scholar] [CrossRef]
- Leen, E.; Picard, J.; Stebbing, J.; Abel, M.; Dhillon, T.; Wasan, H. Percutaneous irreversible electroporation with systemic treatment for locally advanced pancreatic adenocarcinoma. J. Gastrointest. Oncol. 2018, 9, 275–281. [Google Scholar] [CrossRef]
- Månsson, C.; Bergenfeldt, M.; Brahmstaedt, R.; Karlson, B.-M.; Nygren, P.; Nilsson, A. Safety and preliminary efficacy of ultrasound-guided percutaneous irreversible electroporation for treatment of localized pancreatic cancer. Anticancer. Res. 2014, 34, 289–293. [Google Scholar]
- Månsson, C.; Brahmstaedt, R.; Nilsson, A.; Nygren, P.; Karlson, B.-M. Percutaneous irreversible electroporation for treatment of locally advanced pancreatic cancer following chemotherapy or radiochemotherapy. Eur. J. Surg. Oncol. 2016, 42, 1401–1406. [Google Scholar] [CrossRef]
- Månsson, C.; Brahmstaedt, R.; Nygren, P.; Nilsson, A.; Urdzik, J.; Karlson, B.-M. Percutaneous Irreversible Electroporation as First-line Treatment of Locally Advanced Pancreatic Cancer. Anticancer. Res. 2019, 39, 2509–2512. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., 2nd; Kwon, D.; Chalikonda, S.; Sellers, M.; Kotz, E.; Scoggins, C.; McMasters, K.M.; Watkins, K. Treatment of 200 locally advanced (stage III) pancreatic adenocarcinoma patients with irreversible electroporation: Safety and efficacy. Ann. Surg. 2015, 262, 486–494; discussion 92–94. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., 2nd; McFarland, K.; Ellis, S.; Velanovich, V. Irreversible electroporation in locally advanced pancreatic cancer: Potential improved overall survival. Ann. Surg. Oncol. 2013, 20 (Suppl. S3), S443–S449. [Google Scholar] [CrossRef]
- Narayanan, G.; Hosein, P.J.; Arora, G.; Barbery, K.J.; Froud, T.; Livingstone, A.S.; Franceschi, D.; Lima, C.M.R.; Yrizarry, J. Percutaneous Irreversible Electroporation for Downstaging and Control of Unresectable Pancreatic Adenocarcinoma. J. Vasc. Interv. Radiol. 2012, 23, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Hosein, P.J.; Beulaygue, I.C.; Froud, T.; Scheffer, H.J.; Venkat, S.R.; Echenique, A.M.; Hevert, E.C.; Livingstone, A.S.; Rocha-Lima, C.M.; et al. Percutaneous Image-Guided Irreversible Electroporation for the Treatment of Unresectable, Locally Advanced Pancreatic Adenocarcinoma. J. Vasc. Interv. Radiol. 2017, 28, 342–348. [Google Scholar] [CrossRef]
- Paiella, S.; Butturini, G.; Frigerio, I.; Salvia, R.; Armatura, G.; Bacchion, M.; Fontana, M.; D’’Onofrio, M.; Martone, E.; Bassi, C. Safety and Feasibility of Irreversible Electroporation (IRE) in Patients with Locally Advanced Pancreatic Cancer: Results of a Prospective Study. Dig. Surg. 2015, 32, 90–97. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Vroomen, L.G.P.H.; De Jong, M.C.; Melenhorst, M.C.A.M.; Zonderhuis, B.M.; Daams, F.; Vogel, J.A.; Besselink, M.G.H.; Van Kuijk, C.; Witvliet, J.; et al. Ablation of Locally Advanced Pancreatic Cancer with Percutaneous Irreversible Electroporation: Results of the Phase I/II PANFIRE Study. Radiology 2017, 282, 585–597. [Google Scholar] [CrossRef]
- Yan, L.; Chen, Y.-L.; Su, M.; Liu, T.; Xu, K.; Liang, F.; Gu, W.-Q.; Lu, S.-C. A Single-institution Experience with Open Irreversible Electroporation for Locally Advanced Pancreatic Carcinoma. Chin. Med. J. 2016, 129, 2920–2925. [Google Scholar] [CrossRef] [PubMed]
- Ruarus, A.H.; Barabasch, A.; Catalano, O.; Leen, E.; Narayanan, G.; Nilsson, A.; Padia, S.A.; Wiggermann, P.; Scheffer, H.J.; Meijerink, M.R. Irreversible Electroporation for Hepatic Tumors: Protocol Standardization Using the Modified Delphi Technique. J. Vasc. Interv. Radiol. 2020, 31, 1765–1771.e15. [Google Scholar] [CrossRef]
- Martin, R.C., 2nd; Durham, A.N.; Besselink, M.G.; Iannitti, D.; Weiss, M.J.; Wolfgang, C.L.; Huang, K.W. Irreversible electroporation in locally advanced pancreatic cancer: A call for standardization of energy delivery. J. Surg. Oncol. 2016, 114, 865–871. [Google Scholar] [CrossRef] [PubMed]
- van Suylichem, P.T.; van Deijnen, J.E.; Wolters, G.H.; van Schilfgaarde, R. Amount and distribution of collagen in pancreatic tissue of different species in the perspective of islet isolation procedures. Cell Transplant. 1995, 4, 609–614. [Google Scholar] [CrossRef]
- Beitel-White, N.; Bhonsle, S.; Martin, R.C.G.; Davalos, R.V. Electrical Characterization of Human Biological Tissue for Irreversible Electroporation Treatments. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 4170–4173. [Google Scholar] [PubMed]
- Thomas, D.; Radhakrishnan, P. Tumor-stromal crosstalk in pancreatic cancer and tissue fibrosis. Mol. Cancer 2019, 18, 14. [Google Scholar] [CrossRef]
- Chen, S.; Chen, X.; Shan, T.; Ma, J.; Lin, W.; Li, W.; Kang, Y. MiR-21-mediated Metabolic Alteration of Cancer-associated Fibroblasts and Its Effect on Pancreatic Cancer Cell Behavior. Int. J. Biol. Sci. 2018, 14, 100–110. [Google Scholar] [CrossRef]
- Yarmush, M.L.; Golberg, A.; Serša, G.; Kotnik, T.; Miklavčič, D. Electroporation-Based Technologies for Medicine: Principles, Applications, and Challenges. Annu. Rev. Biomed. Eng. 2014, 16, 295–320. [Google Scholar] [CrossRef]
- He, C.; Wang, J.; Sun, S.; Zhang, Y.; Lin, X.; Lao, X.; Cui, B.; Li, S. Irreversible electroporation versus radiotherapy after induction chemotherapy on survival in patients with locally advanced pancreatic cancer: A propensity score analysis. BMC Cancer 2019, 19, 394. [Google Scholar]
- Lambert, L.; Hořejš, J.; Krška, Z.; Hoskovec, D.; Petruzelka, L.; Krechler, T.; Kriz, P.; Bříza, J. Treatment of locally advanced pancreatic cancer by percutaneous and intraoperative irreversible electroporation: General hospital cancer center experience. Neoplasma 2016, 63, 269–273. [Google Scholar] [CrossRef]
- Sedrakyan, A.; Campbell, B.; Merino, J.G.; Kuntz, R.; Hirst, A.; McCulloch, P. IDEAL-D: A rational framework for evaluating and regulating the use of medical devices. BMJ 2016, 353, i2372. [Google Scholar] [CrossRef] [PubMed]
- Avery, K.; Blazeby, J.; Wilson, N.; Macefield, R.; Cousins, S.; Main, B.; Blencowe, N.S.; Zahra, J.; Elliott, D.; Hinchliffe, R.; et al. Development of reporting guidance and core outcome sets for seamless, standardised evaluation of innovative surgical procedures and devices: A study protocol for content generation and a Delphi consensus process (COHESIVE study). BMJ Open 2019, 9, e029574. [Google Scholar] [CrossRef]
- Manas, D.; UK IRE Users Group, UK. Unpublished work. 2017.
- Are, C.; Chowdhury, S.; Ahmad, H.; Ravipati, A.; Song, T.; Shrikandhe, S.; Smith, L. Predictive global trends in the incidence and mortality of pancreatic cancer based on geographic location, socio-economic status, and demographic shift. J. Surg. Oncol. 2016, 114, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Ghaneh, P.; Costello, E.; Neoptolemos, J.P. Biology and management of pancreatic cancer. Postgrad. Med. J. 2008, 84, 478–497. [Google Scholar] [CrossRef]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Balaban, E.P.; Mangu, P.B.; Khorana, A.A.; Shah, M.A.; Mukherjee, S.; Crane, C.H.; Javle, M.M.; Eads, J.R.; Allen, P.; Ko, A.H.; et al. Locally Advanced, Unresectable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 2654–2668. [Google Scholar] [CrossRef]
- Middleton, G.; Silcocks, P.; Cox, T.; Valle, J.; Wadsley, J.; Propper, D.; Coxon, F.; Ross, P.; Madhusudan, S.; Roques, T.; et al. Gemcitabine and capecitabine with or without telomerase peptide vaccine GV1001 in patients with locally advanced or metastatic pancreatic cancer (TeloVac): An open-label, randomised, phase 3 trial. Lancet Oncol. 2014, 15, 829–840. [Google Scholar] [CrossRef]
- Rahib, L.; Fleshman, J.M.; Matrisian, L.M.; Berlin, J.D. Evaluation of Pancreatic Cancer Clinical Trials and Benchmarks for Clinically Meaningful Future Trials: A Systematic Review. JAMA Oncol. 2016, 2, 1209–1216. [Google Scholar] [CrossRef]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; E Faris, J.; A Mellon, E.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for locally advanced pancreatic cancer: A systematic review and patient-level meta-analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Excellence NIfHaC. Overview|Pancreatic Cancer in Adults: Diagnosis and Management|Guidance|NICE: NICE; 2020. Available online: https://www.nice.org.uk/guidance/ng85 (accessed on 14 January 2021).
- Excellence NIfHaC. Recommendations|Pancreatic Cancer in Adults: Diagnosis and Management|Guidance|NICE: NICE; 2020. Available online: https://www.nice.org.uk/guidance/ng85/chapter/Recommendations#managing-resectable-and-borderline-resectable-pancreatic-cancer (accessed on 14 January 2021).
- Pavillard, V.; Formento, P.; Rostagno, P.; Formento, J.; Fischel, J.; Francoual, M.; Etienne, M.; Milano, G. Combination of irinotecan (CPT11) and 5-fluorouracil with an analysis of cellular determinants of drug activity. Biochem. Pharmacol. 1998, 56, 1315–1322. [Google Scholar] [CrossRef]
- Ducreux, M.; Mitry, E.; Ould-Kaci, M.; Boige, V.; Seitz, J.F.; Bugat, R.; Breau, J.L.; Bouché, O.; Etienne, P.L.; Tigaud, J.M.; et al. Randomized phase II study evaluating oxaliplatin alone, oxaliplatin combined with infusional 5-FU, and infusional 5-FU alone in advanced pancreatic carcinoma patients. Ann. Oncol. 2004, 15, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Vogel, J.A.; Besselink, M.G.; Busch, O.R.C.; Wilmink, J.W.; Daams, J.G.; van Eijck, C.H.J.; Koerkamp, B.G.; Rasch, C.R.N.; van Tienhoven, G. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br. J. Surg. 2018, 105, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Marchegiani, G.; Andrianello, S.; Nessi, C.; Sandini, M.; Maggino, L.; Malleo, G.; Paiella, S.; Polati, E.; Bassi, C.; Salvia, R. Neoadjuvant Therapy Versus Upfront Resection for Pancreatic Cancer: The Actual Spectrum and Clinical Burden of Postoperative Complications. Ann. Surg. Oncol. 2018, 25, 626–637. [Google Scholar] [CrossRef]
- Cheng, T.Y.; Sheth, K.; White, R.R.; Ueno, T.; Hung, C.F.; Clary, B.M.; Pappas, T.N.; Tyler, U.S. Effect of Neoadjuvant Chemoradiation on Operative Mortality and Morbidity for Pancreaticoduodenectomy. Ann. Surg. Oncol. 2006, 13, 66–74. [Google Scholar] [CrossRef]
- Yamada, S.; Takami, H.; Sonohara, F.; Hayashi, M.; Fujii, T.; Kodera, Y. Effects of duration of initial treatment on postoperative complications in pancreatic cancer. J. Hepatobiliary Pancreat. Sci. 2019, 26, 235–241. [Google Scholar] [CrossRef]
- Janssen, Q.P.; Buettner, S.; Suker, M.; Beumer, B.R.; Addeo, P.; Bachellier, P.; Bahary, N.; Bekaii-Saab, T.; A Bali, M.; Besselink, M.G.; et al. Neoadjuvant FOLFIRINOX in Patients With Borderline Resectable Pancreatic Cancer: A Systematic Review and Patient-Level Meta-Analysis. J. Natl. Cancer Inst. 2019, 111, 782–794. [Google Scholar] [CrossRef]
- Hurt, C.N.; Falk, S.; Crosby, T.; Macdonald, A.; Ray, R.; Joseph, G.; Staffurth, J.; A Abrams, R.; Griffiths, G.; Maughan, T.; et al. Long-term results and recurrence patterns from SCALOP: A phase II randomised trial of gemcitabine- or capecitabine-based chemoradiation for locally advanced pancreatic cancer. Br. J. Cancer 2017, 116, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Fitzsimmons, D.; Johnson, C.D. Quality of life after treatment of pancreatic cancer. Langenbecks Arch. Surg. 1998, 383, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Field, W.; Rostas, J.W.; Martin, R.C. Quality of life assessment for patients undergoing irreversible electroporation (IRE) for treatment of locally advanced pancreatic cancer (LAPC). Am. J. Surg. 2019, 218, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Tuveson, D.A.; Neoptolemos, J.P. Understanding Metastasis in Pancreatic Cancer: A Call for New Clinical Approaches. Cell 2012, 148, 21–23. [Google Scholar] [CrossRef]
- Yang, Y. Cancer immunotherapy: Harnessing the immune system to battle cancer. J. Clin. Investig. 2015, 125, 3335–3337. [Google Scholar] [CrossRef]
- Royal, R.E.; Levy, C.; Turner, K.; Mathur, A.; Hughes, M.; Kammula, U.S.; Sherry, R.M.; Topalian, S.L.; Yang, J.C.; Lowy, I.; et al. Phase 2 Trial of Single Agent Ipilimumab (Anti-CTLA-4) for Locally Advanced or Metastatic Pancreatic Adenocarcinoma. J. Immunother. 2010, 33, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Dougan, S.K. The Pancreatic Cancer Microenvironment. Cancer J. 2017, 23, 321–325. [Google Scholar] [CrossRef]
- Erkan, M.; Hausmann, S.; Michalski, C.W.; Fingerle, A.A.; Dobritz, M.; Kleeff, J.; Friess, H. The role of stroma in pancreatic cancer: Diagnostic and therapeutic implications. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, G.S.; Poutahidis, T.; Erdman, S.E.; Kirsch, R.; Riddell, R.H.; Diamandis, E.P. Cancer-Associated Fibroblasts Drive the Progression of Metastasis through both Paracrine and Mechanical Pressure on Cancer Tissue. Mol. Cancer Res. 2012, 10, 1403–1418. [Google Scholar] [CrossRef]
- Kleeff, J.; Beckhove, P.; Esposito, I.; Herzig, S.; Huber, P.E.; Löhr, J.M.; Friess, H. Pancreatic cancer microenvironment. Int. J. Cancer 2007, 121, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G.J.; Blaydorn, L.; Beck, J.; Bornemann-Kolatzki, K.; Urnovitz, H.; Schütz, E.; Khemka, V. Phase Ib/II study of gemcitabine, nab-paclitaxel, and pembrolizumab in metastatic pancreatic adenocarcinoma. Investig. New Drugs 2018, 36, 96–102. [Google Scholar] [CrossRef]
- He, C.; Wang, J.; Zhang, Y.; Lin, X.; Li, S. Irreversible electroporation after induction chemotherapy versus chemotherapy alone for patients with locally advanced pancreatic cancer: A propensity score matching analysis. Pancreatology 2020, 20, 477–484. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- van Veldhuisen, E.; Vroomen, L.G.; Ruarus, A.H.; Derksen, T.C.; Busch, O.R.; de Jong, M.C.; Kazemier, G.; Puijk, R.S.; Sorgedrager, N.S.; Vogel, J.A.; et al. Value of CT-Guided Percutaneous Irreversible Electroporation Added to FOLFIRINOX Chemotherapy in Locally Advanced Pancreatic Cancer: A Post Hoc Comparison. J. Vasc. Interv. Radiol. 2020, 31, 1600–1608. [Google Scholar] [CrossRef] [PubMed]
- Ruarus, A.H.; Vroomen, L.G.P.H.; Geboers, B.; Van Veldhuisen, E.; Puijk, R.S.; Nieuwenhuizen, S.; Besselink, M.G.; Zonderhuis, B.M.; Kazemier, G.; De Gruijl, T.D.; et al. Percutaneous Irreversible Electroporation in Locally Advanced and Recurrent Pancreatic Cancer (PANFIRE-2): A Multicenter, Prospective, Single-Arm, Phase II Study. Radiology 2020, 294, 212–220. [Google Scholar] [CrossRef]
- Liu, S.; Qin, Z.; Xu, J.; Zeng, J.; Chen, J.; Niu, L.; Xu, M. Irreversible electroporation combined with chemotherapy for unresectable pancreatic carcinoma: A prospective cohort study. OncoTargets Ther. 2019, 12, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Moriyasu, F.; Tsuchiya, T.; Nagakawa, Y.; Hosokawa, Y.; Saito, K.; Tsuchida, A.; Itoi, T. Irreversible Electroporation for Nonthermal Tumor Ablation in Patients with Locally Advanced Pancreatic Cancer: Initial Clinical Experience in Japan. Intern. Med. 2018, 57, 3225–3231. [Google Scholar] [CrossRef]
- Huang, K.-W.; Yang, P.-C.; Pua, U.; Kim, M.-D.; Li, S.-P.; Qiu, Y.-D.; Song, T.-Q.; Liang, P.-C. The efficacy of combination of induction chemotherapy and irreversible electroporation ablation for patients with locally advanced pancreatic adenocarcinoma. J. Surg. Oncol. 2018, 118, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.A.; Rombouts, S.J.; de Rooij, T.; van Delden, O.M.; Dijkgraaf, M.G.; van Gulik, T.M.; van Hooft, J.E.; van Laarhoven, H.W.; Martin, R.C.; Schoorlemmer, A.; et al. Induction Chemotherapy Followed by Resection or Irreversible Electroporation in Locally Advanced Pancreatic Cancer (IMPALA): A Prospective Cohort Study. Ann. Surg. Oncol. 2017, 24, 2734–2743. [Google Scholar] [CrossRef]
- Zhang, Y.; Shi, J.; Zeng, J.; Alnagger, M.; Zhou, L.; Fang, G.; Pan, Z.; Li, Y.; Chen, J.; Xu, K.; et al. Percutaneous Irreversible Electroporation for Ablation of Locally Advanced Pancreatic Cancer: Experience From a Chinese Institution. Pancreas 2017, 46, e12–e14. [Google Scholar] [CrossRef]
- Savic, L.J.; Chapiro, J.; Hamm, B.; Gebauer, B.; Collettini, F. Irreversible Electroporation in Interventional Oncology: Where We Stand and Where We Go. Rofo 2016, 188, 735–745. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Timmer, F.E.; Geboers, B.; Ruarus, A.H.; Schouten, E.A.; Nieuwenhuizen, S.; Puijk, R.S.; De Vries, J.J.; Meijerink, M.R.; Scheffer, H.J. Irreversible Electroporation for Locally Advanced Pancreatic Cancer. Tech. Vasc. Interv. Radiol. 2020, 23, 100675. [Google Scholar] [CrossRef]
- Wu, L.M.; Zhang, L.L.; Chen, X.H.; Zheng, S.S. Is irreversible electroporation safe and effective in the treatment of hepatobiliary and pancreatic cancers? Hepatobiliary Pancreat. Dis. Int. 2019, 18, 117–124. [Google Scholar] [CrossRef]
- Akinwande, O.; Ahmad, S.S.; Van Meter, T.; Schulz, B.; Martin, R.C.G. CT Findings of Patients Treated with Irreversible Electroporation for Locally Advanced Pancreatic Cancer. J. Oncol. 2015, 2015, 680319. [Google Scholar] [CrossRef] [PubMed]
- Vroomen, L.G.P.H.; Scheffer, H.J.; Melenhorst, M.C.A.M.; De Jong, M.C.; Bergh, J.E.V.D.; Van Kuijk, C.; Van Delft, F.; Kazemier, G.; Meijerink, M.R. MR and CT imaging characteristics and ablation zone volumetry of locally advanced pancreatic cancer treated with irreversible electroporation. Eur. Radiol. 2017, 27, 2521–2531. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, T.; Srimathveeravalli, G.; Gutta, N.; Ezell, P.C.; Monette, S.; Kingham, T.P.; Maybody, M.; Durack, J.C.; Fong, Y.; Solomon, S.B. Comparison of Simulation-based Treatment Planning with Imaging and Pathology Outcomes for Percutaneous CT-guided Irreversible Electroporation of the Porcine Pancreas: A Pilot Study. J. Vasc. Interv. Radiol. 2013, 24, 1709–1718. [Google Scholar] [CrossRef] [PubMed]
- José, A.; Sobrevals, L.; Ivorra, A.; Fillat, C. Irreversible electroporation shows efficacy against pancreatic carcinoma without systemic toxicity in mouse models. Cancer Lett. 2012, 317, 16–23. [Google Scholar] [CrossRef]
- Su, J.J.; Xu, K.; Wang, P.F.; Zhang, H.Y.; Chen, Y.L. Histological analysis of human pancreatic carcinoma following irreversible electroporation in a nude mouse model. World J. Gastrointest. Oncol. 2018, 10, 476–486. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, W.; Procissi, D.; Tyler, P.; A Omary, R.; Larson, A.C. Rapid dramatic alterations to the tumor microstructure in pancreatic cancer following irreversible electroporation ablation. Nanomedicine 2014, 9, 1181–1192. [Google Scholar] [CrossRef] [PubMed]
- Allera, C.; Lazzarini, G.; Patrone, E.; Alberti, I.; Barboro, P.; Sanna, P.; Melchiori, A.; Parodi, S.; Balbi, C. The Condensation of Chromatin in Apoptotic Thymocytes Shows a Specific Structural Change. J. Biol. Chem. 1997, 272, 10817–10822. [Google Scholar] [CrossRef]
- Siriwardana, P.N.; Singh, S.; Johnston, E.W.; Watkins, J.; Bandula, S.; Illing, R.O.; Davidson, B.R. Effect of Hepatic Perfusion on Microwave Ablation Zones in an Ex Vivo Porcine Liver Model. J. Vasc. Interv. Radiol. 2017, 28, 732–739. [Google Scholar] [CrossRef]
- Singh, S.; Siriwardana, P.N.; Johnston, E.W.; Watkins, J.; Bandula, S.; Illing, R.; Davidson, B.R. Perivascular extension of microwave ablation zone: Demonstrated using an ex vivo porcine perfusion liver model. Int. J. Hyperth. 2018, 34, 1114–1120. [Google Scholar] [CrossRef]
- Singh, S.; Siriwardana, P.N.; Johnston, E.W.; Bandula, S.; Davidson, B.R.; Illing, R.O. Perivascular parenchymal extension of the ablation zone following liver microwave ablation. BMJ Case Rep. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.; McFarland, K.; Velanovich, V.; Martin, R.C., 2nd. Borderline and locally advanced pancreatic adenocarcinoma margin accentuation with intraoperative irreversible electroporation. Surgery 2014, 156, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Marsanic, P.; Mellano, A.; Sottile, A.; De Simone, M. Irreversible electroporation as treatment of locally advanced and as margin accentuation in borderline resectable pancreatic adenocarcinoma. Med Biol. Eng. Comput. 2017, 55, 1123–1127. [Google Scholar] [CrossRef]
- Papoulas, M.; Abdul-Hamid, S.; Peddu, P.; Cotoi, C.; Heaton, N.; Menon, K. Irreversible electroporation in borderline resectable pancreatic adenocarcinoma for margin accentuation. J. Surg. Case Rep. 2018, 2018, rjy127. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Choi, H.S.; Chun, H.J.; Kim, E.S.; Keum, B.; Seo, Y.S.; Jeen, Y.T.; Lee, H.S.; Um, S.H.; Kim, C.D.; et al. EUS-guided irreversible electroporation using endoscopic needle-electrode in porcine pancreas. Surg. Endosc. 2019, 33, 658–662. [Google Scholar] [CrossRef]
- Rombouts, S.J.E.; van Dijck, W.P.M.; Nijkamp, M.W.; Derksen, T.C.; Brosens, L.A.A.; Hoogwater, F.J.H.; van Leeuwen, M.S.; Rinkes, I.H.M.B.; van Hillegersberg, R.; Wittkampf, F.H.; et al. Clinical and pathological outcomes after irreversible electroporation of the pancreas using two parallel plate electrodes: A porcine model. HPB 2017, 19, 1058–1065. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D. Electrochemotherapy–An easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur. J. Cancer Suppl. 2006, 4, 3–12. [Google Scholar] [CrossRef]
- Di Monta, G.; Caracò, C.; Benedetto, L.; La Padula, S.; Marone, U.; Tornesello, M.L.; Buonaguro, F.M.; Simeone, E.; Ascierto, P.A.; Mozzillo, N. Electrochemotherapy as “new standard of care” treatment for cutaneous Kaposi’s sarcoma. Eur. J. Surg. Oncol. 2014, 40, 61–66. [Google Scholar] [CrossRef]
- Overview|Electrochemotherapy for Primary Basal Cell Carcinoma and Primary Squamous Cell Carcinoma|Guidance|NICE: NICE; 2021. Available online: https://www.nice.org.uk/guidance/ipg478 (accessed on 14 January 2021).
- Jaroszeski, M.J.; Dang, V.; Pottinger, C.; Hickey, J.; Gilbert, R.; Heller, R. Toxicity of anticancer agents mediated by electroporation in vitro. Anticancer Drugs 2000, 11, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Mir, L.M.; Gehl, J.; Sersa, G.; Collins, C.G.; Garbay, J.R.; Billard, V.; Geertsen, P.F.; Rudolf, Z.; O’Sullivan, G.C.; Marty, M. Standard operating procedures of the electrochemotherapy: Instructions for the use of bleomycin or cisplatin administered either systemically or locally and electric pulses delivered by the CliniporatorTM by means of invasive or non-invasive electrodes. Eur. J. Cancer Suppl. 2006, 4, 14–25. [Google Scholar] [CrossRef]
- Jaroszeski, M.J.; Illingworth, P.; Pottinger, C.; Hyacinthe, M.; Heller, R. Electrically mediated drug delivery for treating subcutaneous and orthotopic pancreatic adenocarcinoma in a hamster model. Anticancer. Res. 1999, 19, 989–994. [Google Scholar] [PubMed]
- Girelli, R.; Prejanò, S.; Cataldo, I.; Corbo, V.; Martini, L.; Scarpa, A.; Claudio, B. Feasibility and safety of electrochemotherapy (ECT) in the pancreas: A pre-clinical investigation. Radiol. Oncol. 2015, 49, 147–154. [Google Scholar] [CrossRef]
- Casadei, R.; Ricci, C.; Ingaldi, C.; Alberici, L.; Di Marco, M.; Guido, A.; Minni, F.; Serra, C. Intraoperative electrochemotherapy in locally advanced pancreatic cancer: Indications, techniques and results—A single-center experience. Updat. Surg. 2020, 72, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Piccirillo, M.; Palaia, R.; Petrillo, A.; Lastoria, S.; Izzo, F. Electrochemotherapy in locally advanced pancreatic cancer: Preliminary results. Int. J. Surg. 2015, 18, 230–236. [Google Scholar] [CrossRef]
- Bhutiani, N.; Agle, S.; Li, Y.; Li, S.; Martin, R.C., 2nd. Irreversible electroporation enhances delivery of gemcitabine to pancreatic adenocarcinoma. J. Surg. Oncol. 2016, 114, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Batra, S.K. Pancreatic cancer metastasis: Are we being pre-EMTed? Curr. Pharm. Des. 2015, 21, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Dev, S.B.; Rabussay, D.P.; Widera, G.; Hofmann, G.A. Medical applications of electroporation. IEEE Trans. Plasma Sci. 2000, 28, 206–223. [Google Scholar] [CrossRef]
- Bhutiani, N.; Pulliam, Z.R.; Zheng, Q.; Pandit, H.; Shi, X.; Chen, Y.; Yu, Y.; Bs, Z.R.P.; Tan, M.; Martin, R.C.G. Electrochemotherapy with Irreversible Electroporation and FOLFIRINOX Improves Survival in Murine Models of Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2020, 27, 4348–4359. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, V.P.; Łuksza, M.; Zhao, J.N.; Makarov, V.; Moral, J.A.; Remark, R.; Herbst, B.; Askan, G.; Bhanot, U.; Senbabaoglu, Y.; et al. Identification of unique neoantigen qualities in long-term survivors of pancreatic cancer. Nature 2017, 551, 512–516. [Google Scholar] [CrossRef]
- Ene–Obong, A.; Clear, A.J.; Watt, J.; Wang, J.; Fatah, R.; Riches, J.C.; Marshall, J.F.; Chin–Aleong, J.; Chelala, C.; Gribben, J.G.; et al. Activated Pancreatic Stellate Cells Sequester CD8+ T Cells to Reduce Their Infiltration of the Juxtatumoral Compartment of Pancreatic Ductal Adenocarcinoma. Gastroenterology 2013, 145, 1121–1132. [Google Scholar] [CrossRef]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A guide to cancer immunotherapy: From T cell basic science to clinical practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Winograd, R.; Byrne, K.T.; Evans, R.A.; Odorizzi, P.M.; Meyer, A.R.L.; Bajor, D.L.; Clendenin, C.; Stanger, B.Z.; Furth, E.E.; Wherry, E.J.; et al. Induction of T-cell Immunity Overcomes Complete Resistance to PD-1 and CTLA-4 Blockade and Improves Survival in Pancreatic Carcinoma. Cancer Immunol. Res. 2015, 3, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Bosch, N.; Vinaixa, J.; Navarro, P. Immune Evasion in Pancreatic Cancer: From Mechanisms to Therapy. Cancers 2018, 10, 6. [Google Scholar] [CrossRef]
- Razzaque, S.; Ashraf, N.; Chavez, J.C.; Malafa, M.P.; Coppola, D.; Springett, G.M.; Helm, J.; Kim, R.D. Expression of programmed death ligand 1 (PD-L1) in malignant and nonmalignant pancreatic tissue. J. Clin. Oncol. 2013, 31, 215. [Google Scholar] [CrossRef]
- Geng, L.; Huang, D.; Liu, J.; Qian, Y.; Deng, J.; Li, D.; Hu, Z.; Zhang, J.; Jiang, G.; Zheng, S. B7-H1 up-regulated expression in human pancreatic carcinoma tissue associates with tumor progression. J. Cancer Res. Clin. Oncol. 2008, 134, 1021–1027. [Google Scholar] [CrossRef]
- Nomi, T.; Sho, M.; Akahori, T.; Hamada, K.; Kubo, A.; Kanehiro, H.; Nakamura, S.; Enomoto, K.; Yagita, H.; Azuma, M.; et al. Clinical Significance and Therapeutic Potential of the Programmed Death-1 Ligand/Programmed Death-1 Pathway in Human Pancreatic Cancer. Clin. Cancer Res. 2007, 13, 2151–2157. [Google Scholar] [CrossRef]
- PPark, S.L.; Gebhardt, T.; Mackay, L.K. Tissue-Resident Memory T Cells in Cancer Immunosurveillance. Trends Immunol. 2019, 40, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; Carpenter, D.J.; Chait, M.; Dogra, P.; Gartrell-Corrado, R.D.; Chen, A.X.; Campbell, S.; Liu, W.; Saraf, P.; Snyder, M.E.; et al. Tissue-Resident Memory T Cells Mediate Immune Homeostasis in the Human Pancreas through the PD-1/PD-L1 Pathway. Cell Rep. 2019, 29, 3916–3932.e5. [Google Scholar] [CrossRef] [PubMed]
- Daley, D.; Zambirinis, C.P.; Seifert, L.; Akkad, N.; Mohan, N.; Werba, G.; Barilla, R.; Torres-Hernandez, A.; Hundeyin, M.; Mani, V.R.K.; et al. gammadelta T Cells Support Pancreatic Oncogenesis by Restraining alphabeta T Cell Activation. Cell 2016, 166, 1485–1499 e15. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Wang, J.; Sun, S.; Zhang, Y.; Li, S. Immunomodulatory Effect after Irreversible Electroporation in Patients with Locally Advanced Pancreatic Cancer. J. Oncol. 2019, 2019, 9346017. [Google Scholar] [CrossRef]
- Gabrilovich, D.I.; Nagaraj, S. Myeloid-derived suppressor cells as regulators of the immune system. Nat. Rev. Immunol. 2009, 9, 162–174. [Google Scholar] [CrossRef]
- Pandit, H.; Hong, Y.K.; Li, Y.; Rostas, J.; Pulliam, Z.; Li, S.P.; Martin, R.C.G. Evaluating the Regulatory Immunomodulation Effect of Irreversible Electroporation (IRE) in Pancreatic Adenocarcinoma. Ann. Surg. Oncol. 2019, 26, 800–806. [Google Scholar] [CrossRef]
- Tanaka, A.; Sakaguchi, S. Targeting Treg cells in cancer immunotherapy. Eur. J. Immunol. 2019, 49, 1140–1146. [Google Scholar] [CrossRef]
- Zhao, J.; Wen, X.; Tian, L.; Li, T.; Xu, C.; Wen, X.; Melancon, M.P.; Gupta, S.; Shen, B.; Peng, W.; et al. Irreversible electroporation reverses resistance to immune checkpoint blockade in pancreatic cancer. Nat. Commun. 2019, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Mucciolo, G.; Roux, C.; Scagliotti, A.; Brugiapaglia, S.; Novelli, F.; Cappello, P. The dark side of immunotherapy: Pancreatic cancer. Cancer Drug Resist. 2020, 3, 491–520. [Google Scholar] [CrossRef]
- Kawaoka, T.; Oka, M.; Takashima, M.; Ueno, T.; Yamamoto, K.; Yahara, N.; Yoshino, S.; Hazama, S. Adoptive immunotherapy for pancreatic cancer: Cytotoxic T lymphocytes stimulated by the MUC1-expressing human pancreatic cancer cell line YPK-1. Oncol. Rep. 2008, 20, 155–163. [Google Scholar] [CrossRef]
- Lin, M.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L.; Xu, K. Short-term clinical efficacy of percutaneous irreversible electroporation combined with allogeneic natural killer cell for treating metastatic pancreatic cancer. Immunol. Lett. 2017, 186, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Pan, Q.; Hu, C.; Fan, Y.; Wang, Y.; Li, R.; Hu, X. Efficacy of irreversible electroporation ablation combined with natural killer cells in treating locally advanced pancreatic cancer. J. BUON 2020, 25, 1643–1649. [Google Scholar] [PubMed]
- SDS. DIRECT Clinical Study for Stage III Pancreatic Cancer. 2021. Available online: http://research.angiodynamics.com/studies/direct-study/ (accessed on 14 January 2021).
- Yoshioka, M.; Sato, T.; Furuya, T.; Shibata, S.; Andoh, H.; Asanuma, Y.; Hatazawa, J.; Shimosegawa, E.; Koyama, K.; Yamamoto, Y. Role of positron emission tomography with 2-deoxy-2-[18F]fluoro-d-glucose in evaluating the effects of arterial infusion chemotherapy and radiotherapy on pancreatic cancer. J. Gastroenterol. 2004, 39, 50–55. [Google Scholar] [CrossRef]
- Rashid, M.F.; Hecht, E.M.; Steinman, J.A.; Kluger, M.D. Irreversible electroporation of pancreatic adenocarcinoma: A primer for the radiologist. Abdom. Radiol. 2017, 43, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.B.; Rich, T.A.; Byrd, D.R.; Cleary, K.R.; Connelly, J.H.; Levin, B.; Charnsangavej, C.; Fenoglio, C.J.; Ames, F.C. Preoperative Chemoradiation and Pancreaticoduodenectomy for Adenocarcinoma of the Pancreas. Arch. Surg. 1992, 127, 1335–1339. [Google Scholar] [CrossRef]
- Washington, K.; Berlin, J.; Branton, P.; Burgart, L.J.; Carter, D.K.; Compton, C.C.; Fitzgibbons, P.; Frankel, W.L.; Jessup, J.; Kakar, S.; et al. Protocol for the Examination of Specimens from Patients with Carcinoma of the Exocrine Pancreas; College of American Pathologists: Northfield, IL, USA, 2016. [Google Scholar]
- Chatterjee, D.; Katz, M.H.; Rashid, A.; Varadhachary, G.R.; Wolff, R.A.; Wang, H.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Crane, C.; et al. Histologic grading of the extent of residual carcinoma following neoadjuvant chemoradiation in pancreatic ductal adenocarcinoma: A predictor for patient outcome. Cancer 2012, 118, 3182–3190. [Google Scholar] [CrossRef] [PubMed]
- Janssen, B.V.; Tutucu, F.; Van Roessel, S.; Adsay, V.; Basturk, O.; Campbell, F.; Doglioni, C.; Esposito, I.; Feakins, R. Amsterdam International Consensus Meeting: Tumor response scoring in the pathology assessment of resected pancreatic cancer after neoadjuvant therapy. Mod. Pathol. 2021, 34, 4–12. [Google Scholar] [CrossRef]
- Campbell, F.; Cairns, A.; Duthie, F.; Feakins, R.M. Dataset for Histopathological Reporting of Carcinomas of the Pancreas, Ampulla of Vater and Common Bile Duct, 2nd ed.; Royal College of Pathologists: London, UK, 2019. [Google Scholar]
- Nielsen, K.; Scheffer, H.J.; Vieveen, J.M.; Van Tilborg, A.A.J.M.; Meijer, S.; Van Kuijk, C.; Tol, M.P.V.D.; Meijerink, M.R.; Bouwman, R.A. Anaesthetic management during open and percutaneous irreversible electroporation. Br. J. Anaesth. 2014, 113, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.J.; Chien, H.-L.; Weiss, M.J.; He, J.; Wolfgang, C.L.; Cameron, J.L.; Pawlik, T.M.; Makary, M.A. Minimally invasive versus open surgery in the Medicare population: A comparison of post-operative and economic outcomes. Surg. Endosc. 2018, 32, 3874–3880. [Google Scholar] [CrossRef] [PubMed]
- Joines, W.T.; Zhang, Y.; Li, C.; Jirtle, R.L. The measured electrical properties of normal and malignant human tissues from 50 to 900 MHz. Med. Phys. 1994, 21, 547–550. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Komar, C.A.; Bengsch, F.; Graham, K.; Beatty, G.L. Genetically Engineered Mouse Models of Pancreatic Cancer: The KPC Model (LSL-Kras(G12D/+); LSL-Trp53(R172H/+); Pdx-1-Cre), Its Variants, and Their Application in Immuno-oncology Drug Discovery. Curr. Protoc. Pharmacol. 2016, 73, 14–39. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Date | n | Cancer Stage and Size | Median OS (Months) | Location | Type of Study |
|---|---|---|---|---|---|---|
| Veldhuisen et al. [86] | 2020 | 52 | LAPC ≤ 4.5 cm | 17.2 | The Netherlands | Comparative |
| Ruarus et al. [87] | 2020 | 50 | LAPC ≤ 4.6 cm (n = 40) Post-surgical local recurrence (n = 10) | LAPC: 17 Post-surgery local recurrence: 16 | The Netherlands | Prospective single arm |
| He et al. [84] | 2020 | 32 | LAPC > 4 cm included | 24 | China | Propensity Score Matched analysis |
| Holland et al. [31] | 2019 | 152 | LAPC ≤ 5.5 cm | 30 | Multi-national | Prospective observational using patient registry |
| Liu et al. [88] | 2019 | 54 | LAPC (n = 28) metastatic PC (n = 24) | LAPC: 20 metastatic PC: 14 | China | Prospective |
| Flak et al. [30] | 2019 | 33 | LAPC ≤ 5 cm | 18 | Denmark | Prospective single arm |
| Mansson et al. [36] | 2019 | 24 | LAPC ≤ 3.5 cm | 13 | Sweden | Prospective |
| Leen et al. [33] | 2018 | 75 | LAPC ≤ 5 cm | 27 | United Kingdom | Prospective |
| Sugimoto et al. [89] | 2018 | 8 | LAPC ≤ 5 cm | 24 | Japan | Prospective |
| Huang et al. [90] | 2018 | 70 | LAPC≤ 5 cm | 22 | Taiwan | Retrospective |
| Vogel et al. [91] | 2017 | 15 | LAPC ≤ 5.5 cm | 16 | The Netherlands | Prospective |
| Scheffer et al. [42] | 2017 | 25 | LAPC ≤ cm | 17 | The Netherlands | Prospective |
| Narayanan et al. [40] | 2016 | 50 | LAP > 3 cm included | 27 | United States of America | Retrospective |
| Mansson et al. [35] | 2016 | 24 | LAPC ≤ 4.5 cm | 17.9 | Sweden | Prospective |
| Lambert et al. [52] | 2016 | 21 | LAPC ≤ 6.5 cm | 10 | Czech Republic | Retrospective |
| Martin et al. [37] | 2015 | 200 | LAPC | 24.9 | United States of America | Prospective |
| Kluger et al. [32] | 2015 | 50 | LAPC < 3 cm | 12 | United States of America | Prospective |
| Paeilla et al. [41] | 2015 | 10 | LAPC | 17 | Italy | Prospective |
| Martin et al. [38] | 2013 | 54 | LAPC | 20 | United States of America | Prospective with Propensity Score analysis |
| Study | Date | Sample Size | Method of IRE Delivery | All Complications | Severe Complications |
|---|---|---|---|---|---|
| Veldhuisen et al. [86] | 2020 | 52 | Percutaneous | 37% | - |
| Ruarus et al. [87] | 2020 | 50 | Percutaneous | 58% | 42% |
| Liu et al. [88] | 2019 | 54 | Open (16/54) | 19% | 1% |
| Liu et al. | 2019 | 54 | Percutaneous (38/54) | 44% | 3% |
| Holland et al. [31] | 2019 | 152 | Percutaneous | 18% | 13% |
| Flak et al. [30] | 2019 | 33 | Percutaneous | 33% | 21% |
| Mansson et al. [36] | 2019 | 24 | Percutaneous | 33% | 25% |
| Huang et al. [90] | 2018 | 70 | Open | 23% | 4% |
| Leen et al. [33] | 2018 | 75 | Percutaneous | 25% | 8% |
| Zhang et al. [92] | 2017 | 21 | Percutaneous | 19% | 0% |
| Sheffer et al. [42] | 2017 | 25 | Percutaneous | 48% | - |
| Vogel et al. [91] | 2017 | 15 | Percutaneous | 53% | - |
| Narayanan et al. [40] | 2016 | 50 | Percutaneous | 62% | 20% |
| Mansson et al. [35] | 2016 | 24 | Percutaneous | 46% | 13% |
| Lambert et al. [52] | 2016 | 21 | Percutaneous | 24% | - |
| Yan et al. [43] | 2016 | 25 | Open | 36% | 8% |
| Paiella et al. [41] | 2015 | 10 | Open | 10% | 0% |
| Belfiore et al. [29] | 2015 | 20 | Percutaneous | 10% | 0% |
| Martin et al. [37] | 2015 | 200 | Open + resection (50/200) | 40% | - |
| Martin et al. | 2015 | 200 | In situ (150/200) | 36% | - |
| Kluger et al. [32] | 2015 | 50 | Open | 46% | 20% |
| Martin et al. [38] | 2013 | 54 | Open | 39% | - |
| Martin et al. [28] | 2012 | 27 | Open | 25% | 7% |
| Time | Electrode Type | Probe No | Inter-Electrode Distance (mm) | Pulse No | Pulse Length (ms) | Voltage (Volts) | Ablation Zone (mm2) | Histology |
|---|---|---|---|---|---|---|---|---|
| 1 h | Monopolar | 2 | 10 | 90 | 90 | 1900 | Not stated | Oedema Necrosis |
| 2 h | Monopolar | 2 | 10 | 90 | 100 | 1500 | 240 | Necrosis |
| 24 h | Monopolar | 2 | 10 | 70 | 70 | 2000 | 134 | Necrosis |
| 24 h | Bipolar | 1 | 7 | 90 | 70 | 2100 | 271 | Necrosis |
| 48 h | Monopolar | 2 | 9 | 90 | 100 | 1500 | 252 | Necrosis |
| 72 h | Monopolar | 2 | 20 | 90 | 100 | 3000 | Not stated | Necrosis |
| 7 days | Monopolar | 2 | 10 | 90 | 90 | 1900 | Not stated |
Apoptosis Necrosis |
| 7 days | Monopolar | 2 | 15 | 90 | 70 | 2700 | Not stated | Necrosis |
| 14 days | Monopolar | 2 | 10 | 90 | 100 | 1500 | <100 | Fibrosis |
| 14 days | Monopolar | 2 | 15 | 90 | 100 | 1500 | Not seen | No changes |
| 14 days | Monopolar | 2 | 15 | 70 | 100 | 2250 | Not seen | No changes |
| 14 days | Monopolar | 2 | 10 | 70 | 70 | 2000 | Not seen | No changes |
| 14 days | Not specified | - | Not specified | 100 | 100 | 2500 | Not stated | Necrosis |
| 14 days | Monopolar | 2 | 15 | 90 | 100 | 2300 | Not stated | Necrosis Apoptosis |
| 28 days | Monopolar | 2 | 15 | 90 | 100 | 2500 | 21 |
Atrophy Fibrosis |
| 28 days | Bipolar | 1 | 7 | 90 | 70 | 2400 | 207 |
Atrophy Fibrosis |
| Time | Electrode Type | Probe No | Inter-Electrode Distance (mm) | Pulse No |
Pulse Length (ms) | Voltage (Volts/cm) | Ablation Zone (mm2) | Histology |
|---|---|---|---|---|---|---|---|---|
| 0.5 h | Not specified | - | Not specified | 64 | 100 | 1250 | Not stated |
Necrosis Apoptosis |
| 24 h | Not specified | - | Not specified | 100 | 100 | 2500 | Not stated | Necrosis No evidence of apoptosis |
| 24 h | Not specified | - | 5 | 90 | 100 | 800 | Not stated | Necrosis Apoptosis |
| 72 h | Not specified | - | 5 | 90 | 100 | 800 | Not stated | Necrosis Apoptosis |
| 7 days | Not specified | - | Not specified | 100 | 100 | 2500 | Not stated | Necrosis No evidence of apoptosis |
| 7 days | Not specified | - | 5 | 90 | 100 | 800 | Not stated | Necrosis Apoptosis |
| 14 days | Not specified | - | Not specified | 100 | 100 | 2500 | Not stated | Necrosis No evidence of apoptosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rai, Z.L.; Feakins, R.; Pallett, L.J.; Manas, D.; Davidson, B.R. Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy. J. Clin. Med. 2021, 10, 1609. https://doi.org/10.3390/jcm10081609
Rai ZL, Feakins R, Pallett LJ, Manas D, Davidson BR. Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy. Journal of Clinical Medicine. 2021; 10(8):1609. https://doi.org/10.3390/jcm10081609
Chicago/Turabian StyleRai, Zainab L., Roger Feakins, Laura J. Pallett, Derek Manas, and Brian R. Davidson. 2021. "Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy" Journal of Clinical Medicine 10, no. 8: 1609. https://doi.org/10.3390/jcm10081609
APA StyleRai, Z. L., Feakins, R., Pallett, L. J., Manas, D., & Davidson, B. R. (2021). Irreversible Electroporation (IRE) in Locally Advanced Pancreatic Cancer: A Review of Current Clinical Outcomes, Mechanism of Action and Opportunities for Synergistic Therapy. Journal of Clinical Medicine, 10(8), 1609. https://doi.org/10.3390/jcm10081609