
The Relationship between Initial Tacrolimus Metabolism Rate and Recipients Body Composition in Kidney Transplantation

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
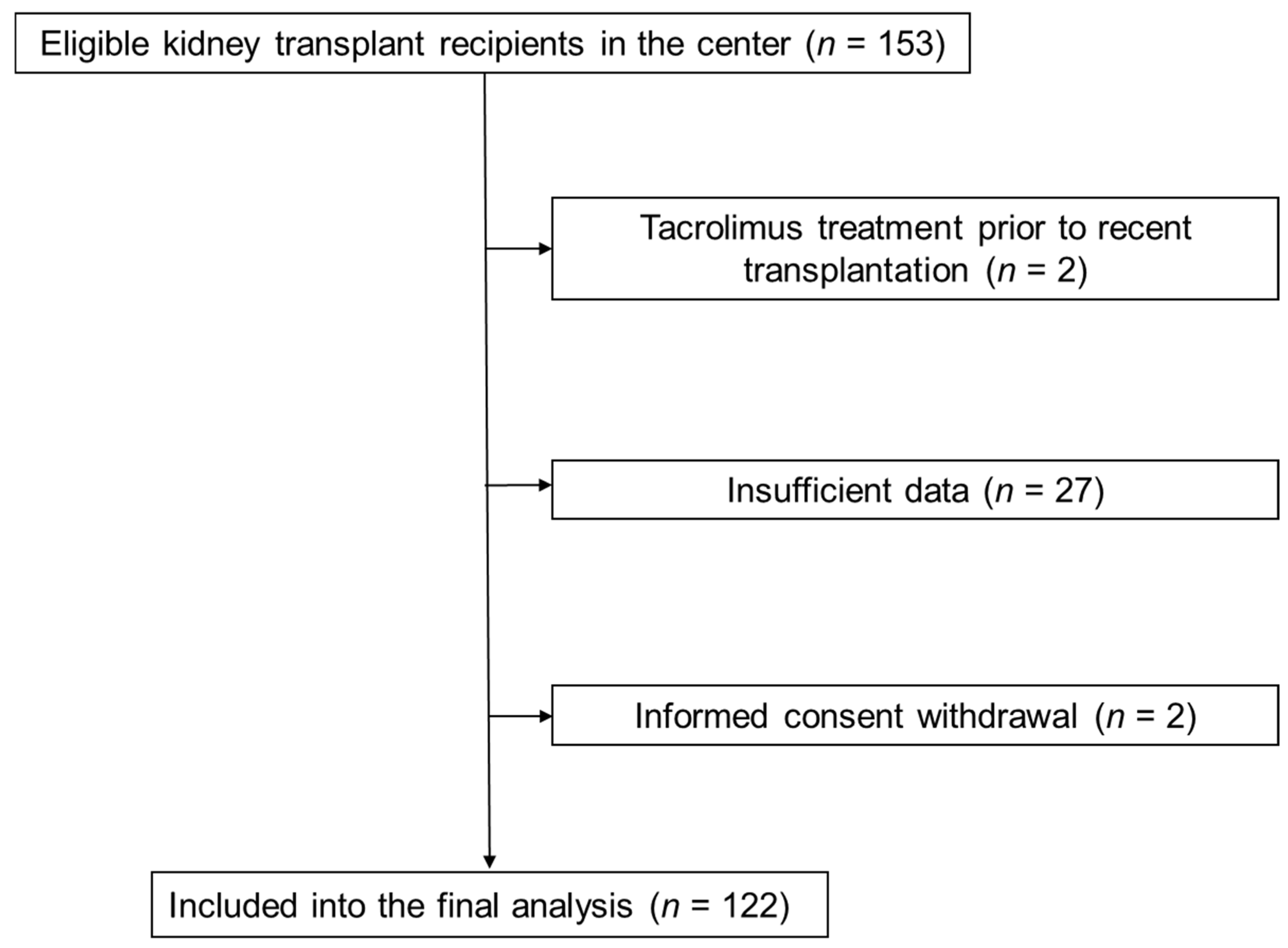
2.1. Study Group
2.2. Pre-Transplant BIA
2.3. Immunosuppression Protocol and Tacrolimus C/D Ratio Calculation
2.4. Statistical Analysis
3. Results
3.1. Study Group Characteristics
3.2. Body Composition Parameters in Slow and Fast Tacrolimus Metabolizers
3.3. Body Composition Parameters in Groups Depending on the LBMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentata, Y. Tacrolimus: 20 years of use in adult kidney transplantation. What we should know about its nephrotoxicity. Artif. Organs. 2020, 44, 140–152. [Google Scholar] [CrossRef] [PubMed]
- Saint-Marcoux, F.; Woillard, J.B.; Jurado, C.; Marquet, P. Lessons from routine dose adjustment of tacrolimus in renal transplant patients based on global exposure. Ther. Drug Monit. 2013, 35, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.E.; Tett, S.E. Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation. Clin. Pharmacokinet. 2004, 43, 623–653. [Google Scholar] [CrossRef] [PubMed]
- Stratta, P.; Quaglia, M.; Cena, T.; Antoniotti, R.; Fenoglio, R.; Menegotto, A.; Ferrante, D.; Genazzani, A.; Terrazzino, S.; Magnani, C. The interactions of age, sex, body mass index, genetics, and steroid weight-based doses on tacrolimus dosing requirement after adult kidney transplantation. Eur. J. Clin. Pharmacol. 2012, 68, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Krzyżowska, K.; Kolonko, A.; Giza, P.; Chudek, J.; Więcek, A. Which Kidney Transplant Recipients Can Benefit from the Initial Tacrolimus Dose Reduction? Biomed Res. Int. 2018, 30, 4573452. [Google Scholar] [CrossRef]
- Vavic, N.; Rancic, N.; Dragojevic-Simic, V.; Draskovic-Pavlovic, B.; Bokonjic, D.; Ignjatovic, L.; Mikov, M. The influence of comedication on tacrolimus blood concentration in patients subjected to kidney transplantation: A retrospective study. Eur. J. Drug Metab. Pharmacokinet. 2014, 39, 243–253. [Google Scholar] [CrossRef]
- Ro, H.; Jeong, J.C.; Kong, J.M.; Min, J.W.; Park, S.K.; Lee, J.; Koo, T.Y.; Yang, J.; Kim, M.S.; Hwang, S.; et al. The tacrolimus metabolism affect post-transplant outcome mediating acute rejection and delayed graft function: Analysis from Korean Organ Transplantation Registry data. Transpl. Int. 2021, 34, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, E.; de Cos, M.A.; Fernández-Fresnedo, G.; Sánchez, B.; Ruiz, J.C.; Piñera, C.; Palomar, R.; Cotorruelo, J.G.; Gómez-Alamillo, C.; de Castro, S.S.; et al. Higher initial tacrolimus blood levels and concentration-dose ratios in kidney transplant recipients who develop diabetes mellitus. Transpl. Proc. 2005, 37, 3819–3820. [Google Scholar] [CrossRef]
- Saito, M.; Satoh, S.; Kagaya, H.; Tsuruta, H.; Obara, T.; Kumazawa, T.; Inoue, T.; Inoue, K.; Miura, M.; Yuasa, T.; et al. Thrombotic microangiopathy developing in early stage after renal transplantation with a high trough level of tacrolimus. Clin. Exp. Nephrol. 2008, 12, 312–315. [Google Scholar] [CrossRef]
- Schiff, J.; Cole, E.; Cantarovich, M. Therapeutic monitoring of calcineurin inhibitors for the nephrologist. Clin. J. Am. Soc. Nephrol. 2007, 2, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Mao, Y.; Razo, J.; Zhou, X.; Wong, S.T.; Patel, S.; Elliott, E.; Shea, E.; Wu, A.H.; Gaber, A.O. Using genetic and clinical factors to predict tacrolimus dose in renal transplant recipients. Pharmacogenomics 2010, 11, 1389–1402. [Google Scholar] [CrossRef]
- Passey, C.; Birnbaum, A.K.; Brundage, R.C.; Oetting, W.S.; Israni, A.K.; Jacobson, P.A. Dosing equation for tacrolimus using genetic variants and clinical factors. Br. J. Clin. Pharmacol. 2011, 72, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Åsberg, A.; Midtvedt, K.; van Guilder, M.; Størset, E.; Bremer, S.; Bergan, S.; Jelliffe, R.; Hartmann, A.; Neely, M.N. Inclusion of CYP3A5 genotyping in a nonparametric population model improves dosing of tacrolimus early after transplantation. Transpl. Int. 2013, 26, 1198–1207. [Google Scholar] [CrossRef]
- Størset, E.; Åsberg, A.; Skauby, M.; Neely, M.; Bergan, S.; Bremer, S.; Midtvedt, K. Improved Tacrolimus Target Concentration Achievement Using Computerized Dosing in Renal Transplant Recipients—A Prospective, Randomized Study. Transplantation 2015, 99, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Boughton, O.; Borgulya, G.; Cecconi, M.; Fredericks, S.; Moreton-Clack, M.; MacPhee, I.A. A published pharmacogenetic algorithm was poorly predictive of tacrolimus clearance in an independent cohort of renal transplant recipients. Br. J. Clin. Pharmacol. 2013, 76, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, E.; de Cos, M.A.; Sánchez, B.; Ruiz, J.C.; Piñera, C.; Fernández-Fresnedo, G.; Palomar, R.; Pérez-Ceballos, M.A.; Cotorruelo, J.G.; Zubimendi, J.A.; et al. High initial blood levels of tacrolimus in overweight renal transplant recipients. Transpl. Proc. 2005, 37, 1453–1454. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Gallagher, D. Body composition changes with aging: The cause or the result of alterations in metabolic rate and macronutrient oxidation? Nutrition 2010, 26, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Kim, D.H.; Lee, S.M.; Han, N.Y.; Oh, J.M.; Ha, J.; Kim, Y.S. Pharmacokinetics of tacrolimus according to body composition in recipients of kidney transplants. Kidney Res. Clin. Pract. 2012, 31, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Fortmann, C.; Koch, R.; Gerth, H.U.; Pabst, D.; Pavenstadt, H.; Kabar, I.; Husing, A.; Wolters, H.; Reuter, S.; et al. The tacrolimus metabolism rate influences renal function after kidney transplantation. PLoS ONE 2014, 9, e111128. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, M.; Górska, M.; Nowicka, Z.; Edyko, K.; Edyko, P.; Wiślicki, S.; Zawiasa-Bryszewska, A.; Strzelczyk, J.; Matych, J.; Kurnatowska, I. Tacrolimus: Influcnce of the posttransplant concentration/dose ratio on kidney graft function in a two-year follow-up. Kidney Blood Press Res. 2019, 44, 1075–1088. [Google Scholar] [CrossRef]
- Schutte-Nutgen, K.; Tholking, G.; Steinke, J.; Pavenstadt, H.; Schmidt, R.; Suwelack, B.; Reuter, S. Fast Tac metabolizers at risk—It is time for a C/D ratio calculation. J. Clin. Med. 2019, 8, 587. [Google Scholar] [CrossRef] [PubMed]
- Suwelack, B.; Bunnapradist, S.; Meier-Kriesche, U.; Stevens, D.R.; Procaccianti, C.; Morganti, R.; Budde, K. Effect of concentration/dose ratio in de novo kidney transplant recipients receiving LCP-tacrolimus or immediate-release tacrolimus: Post hoc analysis of a phase 3 clinical trial. Ann. Transpl. 2020, 25, e923278. [Google Scholar] [CrossRef] [PubMed]
- Hilmi, M.; Jouinot, A.; Burns, R.; Pigneur, F.; Mounier, R.; Gondin, J.; Neuzillet, C.; Goldwasser, F. Body composition and sarcopenia: The next-generation of personalized oncology and pharmacology? Pharmacol. Ther. 2019, 196, 135–159. [Google Scholar] [CrossRef] [PubMed]
- Sjøblom, B.; Benth, J.Š.; Grønberg, B.H.; Baracos, V.E.; Sawyer, M.B.; Fløtten, Ø.; Hjermstad, M.J.; Aass, N.; Jordhøy, M. Drug Dose Per Kilogram Lean Body Mass Predicts Hematologic Toxicity from Carboplatin-Doublet Chemotherapy in Advanced Non-Small-Cell Lung Cancer. Clin. Lung Cancer. 2017, 18, e129–e136. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Cai, P.; Li, P.; Cao, C.; Zhou, J.; Dong, L.; Yang, Y.; Xuan, Q.; Wang, J.; Zhang, Q. Body Composition as a Predictor of Toxicity and Prognosis in Patients with Diffuse Large B-Cell Lymphoma Receiving R-CHOP Immunochemotherapy. Curr. Oncol. 2021, 23, 1325–1337. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Kim, T.H.; Tao, X.; Kinzig, M.; Landersdorfer, C.B.; Drescher, S.K.; Sutaria, D.S.; Moya, B.; Holzgrabe, U.; Sörgel, F.; et al. First population pharmacokinetic analysis showing increased quinolone metabolite formation and clearance in patients with cystic fibrosis compared to healthy volunteers. Eur. J. Pharm. Sci. 2018, 123, 416–428. [Google Scholar] [CrossRef]
- Ding, N.S.; Malietzis, G.; Lung, P.F.C.; Penez, L.; Yip, W.M.; Gabe, S.; Jenkins, J.T.; Hart, A. The body composition profile is associated with response to anti-TNF therapy in Crohn’s disease and may offer an alternative dosing paradigm. Aliment. Pharmacol. Ther. 2017, 46, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Krzyżowska, K.; Kolonko, A.; Giza, P.; Chudek, J.; Więcek, A. No Significant Influence of Reduced Initial Tacrolimus Dose on Risk of Underdosing and Early Graft Function in Older and Overweight Kidney Transplant Recipients. Transpl. Proc. 2018, 50, 1755–1759. [Google Scholar] [CrossRef] [PubMed]
- Nawaratne, S.; Brien, J.E.; Seeman, E.; Fabiny, R.; Zalcberg, J.; Cosolo, W.; Angus, P.; Morgan, D.J. Relationships among liver and kidney volumes, lean body mass and drug clearance. Br. J. Clin. Pharmacol. 1998, 46, 447–452. [Google Scholar] [CrossRef]
- McLeay, S.C.; Morrish, G.A.; Kirkpatrick, C.M.; Green, B. The relationship between drug clearance and body size: Systematic review and meta-analysis of the literature published from 2000 to 2007. Clin. Pharm. 2012, 51, 319–330. [Google Scholar] [CrossRef]
- Hartinger, J.M.; Šíma, M.; Hronová, K.; Halouzková, B.A.; Szonowská, B.; Polakovič, V.; Bednářová, V.; Hladinová, Z.; Tesař, V.; Slanař, O. Vancomycin pharmacokinetics in patients treated with intermittent haemodialysis based on therapeutic drug monitoring. J. Chemother. 2021, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- De Fijter, W.M.; de Fijter, C.W.; Oe, P.L.; Ter Wee, P.M.; Donker, A.J. Assessment of total body water and lean body mass from anthropometry, Watson formula, creatinine kinetics, and body electrical impedance compared with antipyrine kinetics in peritoneal dialysis patients. Nephrol Dial. Transpl. 1997, 12, 151–156. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Grenda, R.; Prokurat, S.; Ciechanowicz, A.; Piatosa, B.; Kaliciński, P. Evaluation of the genetic background of standard-immunosuppressant-related toxicity in a cohort of 200 paediatric renal allograft recipients—A retrospective study. Ann. Transpl. 2009, 14, 18–24. [Google Scholar]
- Pallet, N.; Etienne, I.; Buchler, M.; Bailly, E.; Hurault de Ligny, B.; Choukroun, G.; Colosio, C.; Thierry, A.; Vigneau, C.; Moulin, B.; et al. Long-Term Clinical Impact of Adaptation of Initial Tacrolimus Dosing to CYP3A5 Genotype. Am. J. Transpl. 2016, 16, 2670–2675. [Google Scholar] [CrossRef] [PubMed]
- Niioka, T.; Kagaya, H.; Saito, M.; Inoue, T.; Numakura, K.; Habuchi, T.; Satoh, S.; Miura, M. Capability of utilizing CYP3A5 polymorphisms to predict therapeutic dosage of tacrolimus at early stage post-renal transplantation. Int. J. Mol. Sci. 2015, 16, 1840–1854. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Tacrolimus C/D Ratio | p | |
|---|---|---|---|
| Slow Metabolizers ≥1.48 n = 61 | Fast Metabolizers <1.48 n = 61 | ||
| Patient | |||
| Age (years) | 51.6 (48.5–54.7) | 44.7 (41.6–47.9) | <0.01 |
| Sex (M/F) | 40/21 | 36/25 | 0.46 |
| BMI (kg/m2) | 25.6 (24.5–26.8) | 25.7 (24.6–26.8) | 0.95 |
| Dialysis vintage (months) * | 34 (25–55) | 31 (20–44) | 0.29 |
| Residual diuresis (mL) * | 300 (0–1000) | 500 (100–1500) | 0.35 |
| Transplant procedure | |||
| Retransplant (n, %) | 4 (6.6) | 10 (16.4) | 0.09 |
| HLA class I mismatch * | 2 (2–3) | 2 (2–3) | 0.48 |
| HLA class II mismatch * | 1 (0–1) | 1 (0–1) | 0.09 |
| CIT (h) | 18.7 (16.9–20.4) | 17.8 (16.2–19.4) | 0.46 |
| Induction therapy | |||
| IL-2RB (n, %) | 29 (47.5) | 46 (75.4) | <0.01 |
| ATG (n, %) | 32 (52.3) | 15 (24.6) | |
| DGF (n, %) | 19 (31.1) | 9 (14.8) | <0.05 |
| Early acute rejection (n, %) | 5 (8.2) | 5 (8.2) | 1.0 |
| Tacrolimus dosing and metabolism | |||
| Tacrolimus dose (mg/d) * | 7.0 (4.0–12.0) | 11.0 (8.0–13.0) | <0.001 |
| Tacrolimus dose per kg (mg/kg) * | 0.11 (0.06–0.14) | 0.14 (0.12–0.16) | <0.001 |
| Initial tacrolimus level (ng/mL) * | 15.5 (9.0–21.6) | 9.7 (6.4–12.0) | <0.001 |
| Initial tacrolimus level > 15 ng/mL (%) | 50.8 | 13.1 | <0.001 |
| Tacrolimus C/D ratio * | 2.00 (1.71–2.50) | 0.99 (0.74–1.24) | <0.001 |
| Parameter | Tacrolimus C/D Ratio | p | |
|---|---|---|---|
| Slow Metabolizers ≥1.48 n = 61 | Fast Metabolizers <1.48 n = 61 | ||
| Baseline body composition analysis | |||
| Weight (kg) | 74.9 (70.5–79.2) | 76.1 (72.4–79.7) | 0.67 |
| ICW (L) | 24.5 (23.1–25.9) | 25.5 (24.1–26.9) | 0.31 |
| ECW (L) | 15.7 (14.8–16.5) | 16.2 (15.3–17.0) | 0.42 |
| TBW (L) | 40.2 (37.9–42.5) | 41.7 (39.4–44.0) | 0.35 |
| ECW/TBW | 0.390 (0.387–0.393) | 0.388 (0.385–0.390) | 0.27 |
| Phase angle (o) | 5.0 (4.8–5.3) | 5.2 (5.0–5.4) | 0.32 |
| Visceral fat area (cm2) * | 93.6 (59.1–126.3) | 88.4 (51.5–129.9) | 0.60 |
| LBM (kg) | 51.5 (48.6–54.4) | 53.5 (50.5–56.4) | 0.34 |
| LBM (%) | 69.2 (67.0–71.4) | 70.5 (67.7–73.3) | 0.45 |
| LBMI (kg/m2) | 18.6 (17.9–19.3) | 18.8 (18.2–19.5) | 0.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolonko, A.; Pokora, P.; Słabiak-Błaż, N.; Czerwieńska, B.; Karkoszka, H.; Kuczera, P.; Piecha, G.; Więcek, A. The Relationship between Initial Tacrolimus Metabolism Rate and Recipients Body Composition in Kidney Transplantation. J. Clin. Med. 2021, 10, 5793. https://doi.org/10.3390/jcm10245793
Kolonko A, Pokora P, Słabiak-Błaż N, Czerwieńska B, Karkoszka H, Kuczera P, Piecha G, Więcek A. The Relationship between Initial Tacrolimus Metabolism Rate and Recipients Body Composition in Kidney Transplantation. Journal of Clinical Medicine. 2021; 10(24):5793. https://doi.org/10.3390/jcm10245793
Chicago/Turabian StyleKolonko, Aureliusz, Patrycja Pokora, Natalia Słabiak-Błaż, Beata Czerwieńska, Henryk Karkoszka, Piotr Kuczera, Grzegorz Piecha, and Andrzej Więcek. 2021. "The Relationship between Initial Tacrolimus Metabolism Rate and Recipients Body Composition in Kidney Transplantation" Journal of Clinical Medicine 10, no. 24: 5793. https://doi.org/10.3390/jcm10245793
APA StyleKolonko, A., Pokora, P., Słabiak-Błaż, N., Czerwieńska, B., Karkoszka, H., Kuczera, P., Piecha, G., & Więcek, A. (2021). The Relationship between Initial Tacrolimus Metabolism Rate and Recipients Body Composition in Kidney Transplantation. Journal of Clinical Medicine, 10(24), 5793. https://doi.org/10.3390/jcm10245793