
The Relationship between Platelet Indices and Ultrasound, Clinical, Laboratory Parameters of Disease Activity in Patients with Rheumatoid Arthritis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical and Laboratory Findings
2.3. Ultrasound Imaging of Joints
- Semi-quantitative grey scale (GS) for grading synovial hypertrophy (0–3) in each joint:
- -
- Grade 0: normal joint with no synovial hypertrophy;
- -
- Grade 1: synovial hypertrophy up to the level of the horizontal line connecting the bone surfaces of an examined joint;
- -
- Grade 2: synovial hypertrophy extending beyond the joint line but with the upper surface flat to the underlying bones;
- -
- Grade 3: synovial hypertrophy extending beyond the joint line but with the upper surface convex to the underlying bones.
- Power Doppler ultrasound (PDUS) semi-quantitative scale (0–3) in each joint:
- -
- Grade 0: no Doppler activity;
- -
- Grade 1: up to three single Doppler spots, or up to one confluent spot and two single spots, or up to two confluent spots;
- -
- Grade 2: greater than grade 1 but <50% Doppler signals in the total GS background;
- -
- Grade 3: greater than grade 2 and >50% Doppler signals of the GS background [27].
2.4. Statistical Analysis
3. Results
3.1. Demographic and Disease-Related Variables in RA Patients
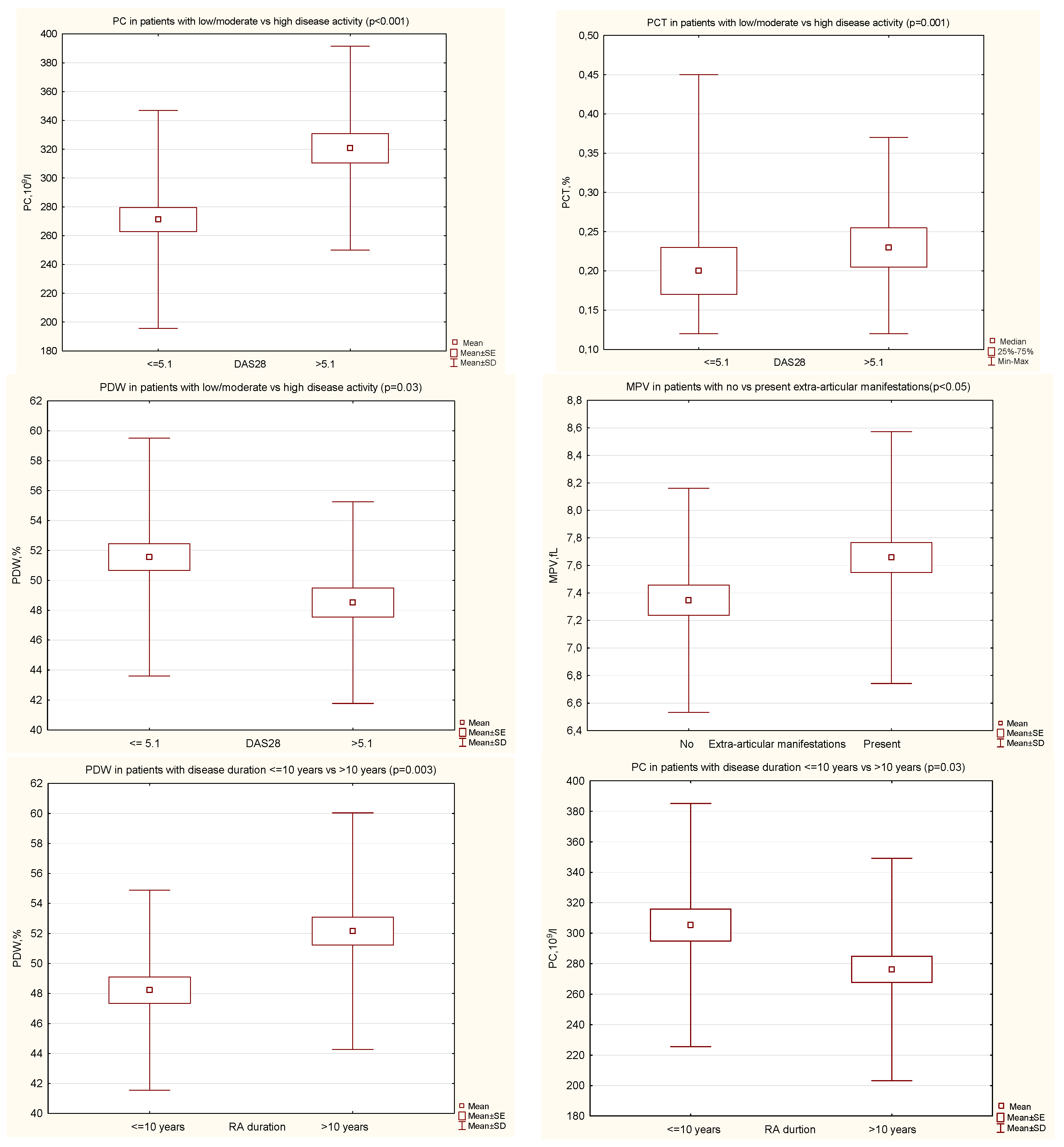
3.2. Comparison of PIs in Certain Groups of Patients with RA
3.3. The Relationship between PIs (PC, MPV, PCT, PDW) and the Clinical Disease Activity Markers, and the Disease Duration, and Treatment Used
3.4. The Relationship between PIs (PC, MPV, PCT, PDW) and Laboratory Disease Activity Markers
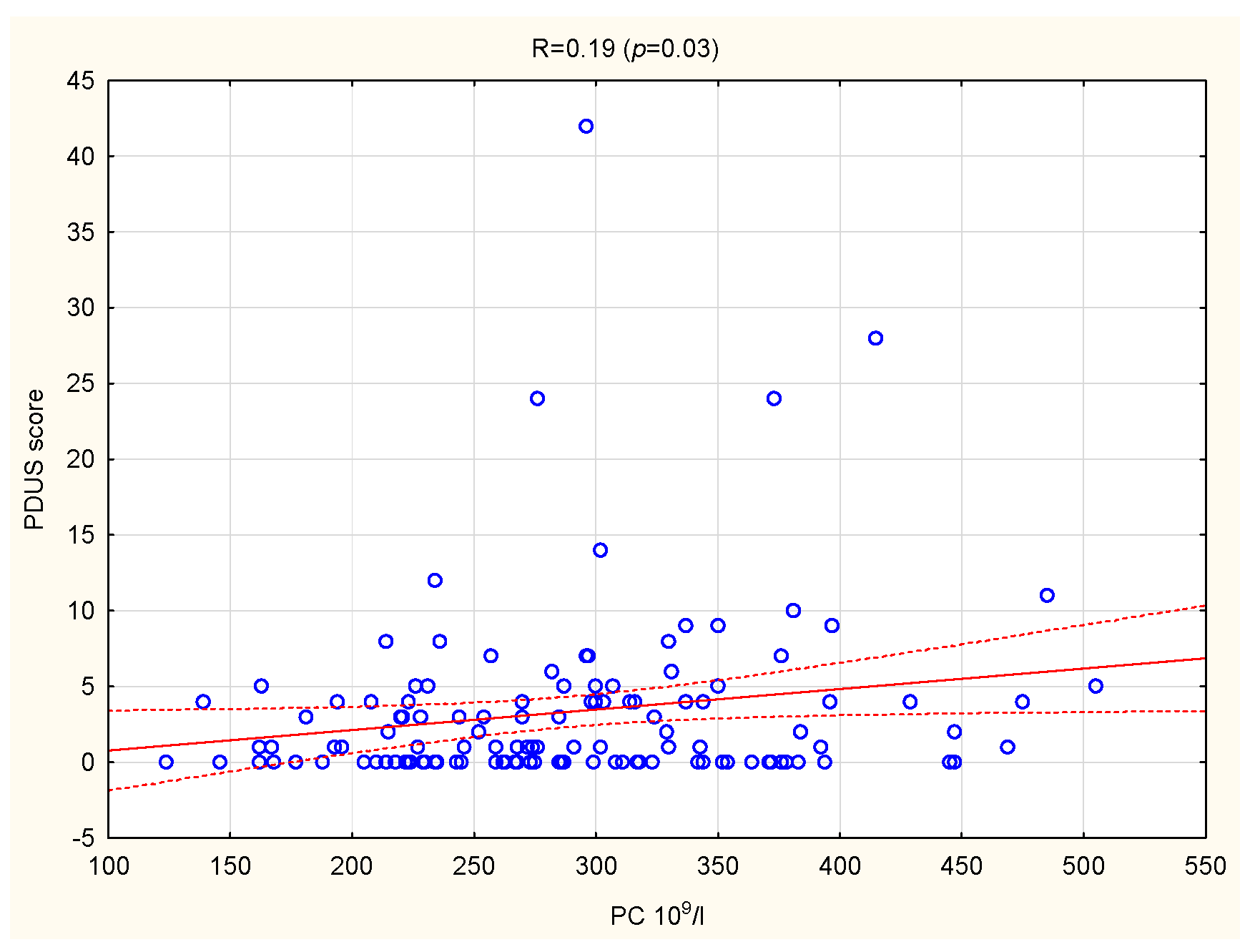
3.5. The Relationship between PIs and US Parameters in the Group of 131 Patients with RA
3.6. The Relationship between PIs and US Parameters in Certain Groups of Patients with RA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khaled, S.A.A.; NasrEldin, E.; Makarem, Y.S.; Mahmoud, H.F.F. Value of Platelet Distribution Width and Mean Platelet Volume in Disease Activity Score of Rheumatoid Arthritis. J. Inflamm. Res. 2020, 3, 595–606. [Google Scholar] [CrossRef]
- Kisacik, B.; Tufan, A.; Kalyoncu, U.; Karadag, O.; Akdogan, A.; Ozturk, M.A.; Kiraz, S.; Ertenli, I.; Calguneri, M. Mean platelet volume (MPV) as an inflammatory marker in ankylosing spondylitis and rheumatoid arthritis. Jt. Bone Spine 2008, 75, 291–294. [Google Scholar] [CrossRef]
- Prevoo, M.L.; van’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts: Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 1995, 38, 44–48. [Google Scholar] [CrossRef]
- Quin, K.; Madhoun, H.M. Ultrasound as a Biomarker in Rheumatic Diseases. Diagnostics 2020, 10, 933. [Google Scholar] [CrossRef]
- Nam, S.W.; Kang, T. A Pragmatic Application of Ultrasonography for the Assessment of Disease Activity in Patients with Early Inflammatory Arthritis. J. Clin. Med. 2021, 10, 283. [Google Scholar] [CrossRef] [PubMed]
- Harifi, G.; Sibilia, J. Pathogenic role of platelets in rheumatoid arthritis and systemic autoimmune diseases. Perspectives and therapeutic aspects. Saudi Med. J. 2016, 37, 354–360. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Stavropoulos-Kalinoglou, A.; Mikhailidis, D.P.; Douglas, K.M.; Kitas, G.D. Platelet function in rheumatoid arthritis: Arthritic and cardiovascular implications. Rheumatol. Int. 2011, 31, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Pogorzelska, K.; Krętowska, A.; Krawczuk-Rybak, M.; Sawicka-Żukowska, M. Characteristics of platelet indices and their prognostic significance in selected medical condition—A systematic review. Adv. Med. Sci. 2020, 65, 310–315. [Google Scholar] [CrossRef]
- Korniluk, A.; Koper-Lenkiewicz, O.M.; Kamińska, J.; Kemona, H.; Dymicka-Piekarska, V. Mean Platelet Volume (MPV): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions. Mediat. Inflamm. 2019, 2019, 9213074. [Google Scholar] [CrossRef] [PubMed]
- Waghale, R.M.; Khot, R.S.; Joshi, P.P. Platelet volume indices: Markers of carotid atherosclerosis in type 2 diabetes mellitus? Clin. Diabetol. 2020, 9, 103–111. [Google Scholar] [CrossRef]
- Xu, F.; Qu, S.; Wang, L.; Qin, Y. Mean platelet volume (MPV): New diagnostic indices for co-morbidity of tuberculosis and diabetes mellitus. BMC Infect. Dis. 2021, 21, 461. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.G.; Becker, R.C.; Berger, P.B.; Bhatt, D.L.; Eikelboom, J.W.; Konkle, B.; Mohler, E.R.; Reilly, M.P.; Berger, J.S. Mean platelet volume as a predictor of cardiovascular risk: A systematic review and meta-analysis. J. Thromb. Haemost. 2010, 8, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Schmoeller, D.; Picarelli, M.M.; Paz Munhoz, T.; Poli de Figueiredo, C.E.; Staub, H.L. Mean Platelet Volume and Immature Platelet Fraction in Autoimmune Disorders. Front. Med. 2017, 4, 146. [Google Scholar] [CrossRef]
- Budak, Y.U.; Polat, M.; Huysal, K. The use of platelet indices, plateletcrit, mean platelet volume and platelet distribution width in emergency non-traumatic abdominal surgery: A systematic review. Biochem. Med. 2016, 26, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.A.; Kim, T.Y. Controversies over the interpretation of changes of mean platelet volume in rheumatoid arthritis. Platelets 2011, 22, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Tekeoğlu, İ.; Gürol, G.; Harman, H.; Karakeçe, E.; Çiftçi, İ.H. Overlooked hematological markers of disease activity in rheumatoid arthritis. Int. J. Rheum. Dis. 2016, 19, 1078–1082. [Google Scholar] [CrossRef]
- Mathew, R.; Kumar, S. Association of platelet indices with disease activity in rheumatoid arthritis. J. Evid. Based Med. Healthc. 2018, 5, 95–100. [Google Scholar] [CrossRef]
- Shuba, N.; Praba, V.; Prithiviraaj, P. Association of platelet indices with disease activity in rheumatoid arthritis. J. Evol. Med. Dent. Sci. 2018, 7, 3940–3945. [Google Scholar]
- Gasparyan, A.Y.; Sandoo, A.; Stavropoulos-Kalinoglou, A.; Kitas, G.D. Mean platelet volume in patients with rheumatoid arthritis: The effect of anti-TNF-α therapy. Rheumatol. Int. 2010, 30, 1125–1129. [Google Scholar] [CrossRef]
- Yazici, S.; Yazici, M.; Erer, B.; Erer, B.; Calik, Y.; Ozhan, H.; Ataoglu, S. The platelet indices in patients with rheumatoid arthritis: Mean platelet volume reflects disease activity. Platelets 2010, 21, 122–125. [Google Scholar] [CrossRef]
- Yıldırım, A.; Karabiber, M.; Surucu, G.; Türkbeyler, I.; Karakoyun, A.; Selkuc, M.Y.; Zengin, O. The changes of mean platelet volume and platelet distribution width in patients with rheumatoid arthritis and their correlation with disease activity. Acta Med. Mediter. 2015, 31, 1105–1111. [Google Scholar]
- Işık, M.; Şahin, H.; Hüseyin, E. New platelet indices as inflammatory parameters for patients with rheumatoid arthritis. Eur. J. Rheumatol. 2014, 1, 144–146. [Google Scholar] [CrossRef]
- Zhou, Z.; Chen, H.; Ju, H.; Sun, M.; Jin, H. Platelet indices in patients with chronic inflammatory arthritis: A systematic review and meta-analysis. Platelets 2020, 31, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerek, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Pincus, T.; Sokka, T.; Kautiainen, H. Further development of a physical function scale on a MDHAQ [corrected] for standard care of patients with rheumatic diseases. J. Rheumatol. 2005, 32, 1432–1439. [Google Scholar]
- Van der Heijde, D. How to read radiographs according to the Sharp/van der Heijde method. J. Rheumatol. 2000, 27, 261–263. [Google Scholar] [PubMed]
- D’Agostino, M.-A.; Terslev, L.; Aegerter, P.; Backhaus, M.; Balint, P.; Bruyn, G.A.; Filippucci, E.; Grassi, W.; Iagnocco, A.; Jousse-Joulin, S.; et al. Scoring ultrasound synovitis in rheumatoid arthritis: A EULAR-OMERACT ultrasound taskforce-Part 1: Definition and development of a standardised, consensus-based scoring system. Rheum. Musculoskelet. Dis. Open 2017, 3, e000428. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, M.; Burmester, G.R.; Gerber, T.; Grassi, W.; Machold, K.P.; Swen, W.A.; Wakefield, R.; Manger, B. Guidelines for musculoskeletal ultrasound in rheumatology. Ann. Rheum. Dis. 2001, 60, 641–649. [Google Scholar] [CrossRef]
- Iagnocco, A.; Finucci, A.; Ceccarelli, F.; Perricone, C.; Iorgoveanu, V.; Valesini, G. Power Doppler ultrasound monitoring of response to anti-tumour necrosis factor alpha treatment in patient with rheumatoid arthritis. Rheumatology 2015, 54, 1890–1896. [Google Scholar] [CrossRef][Green Version]
- Hammer, H.B.; Michelsen, B.; Sexton, J.; Haugen, I.K.; Provan, S.A.; Haavardsholm, E.A.; Uhlig, T.; Kvien, T.K. Swollen, but not tender joints, are independently associated with ultrasound synovitis: Results from a longitudinal observational study of patients with established rheumatoid arthritis. Ann. Rheum. Dis. 2019, 78, 1179–1185. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef]
- Le Blanc, J.; Lordkipanidzé, M. Platelet Function in Aging. Front. Cardiovasc. Med. 2019, 6, 109. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data | Results (n = 131) |
|---|---|
| Age, years | 54.0 (±11.9) |
| Gender, female/male (n, %) | 104 (79.4)/27 (20.6) |
| Disease duration, years | 14.2 (±10.9) |
| Disease duration > 10 years | 73 (55.7) |
| Positive RF-IgM (n, %) | 112 (85.5) |
| Positive anti-CCP (n, %) | 108 (82.4) |
| Extra-articular manifestations (n, %) | 71 (54.2) |
| Erosions (hands/feet) (n, %) | 123 (93.9) |
| Current synthetic DMARD used (n, %) | 128 (97.8) |
| MTX | 119 (90.8) |
| Anti-malarial drug | 51 (38.9) |
| Leflunomide | 14 (10.7) |
| Other | 14 (10.7) |
| Current biological DMARD used (n, %) | 64 (48.9) |
| Anti-TNF | 31 (23.7) |
| Other | 33 (25.2) |
| Current low dose glucocorticoid use (n, %) | 86 (65.6) |
| Data | Results (n = 131) |
|---|---|
| Laboratory results: | |
| Hemoglobin, g/dL | 12.8 (±1.4) |
| WBC, 109/L | 7.0 (±2.7) |
| PC,109/L | 289.1 (±77.2) |
| PCT, % | 0.21 (0.18–0.24) |
| MPV, fl | 7.5 (±0.9) |
| PDW, % | 50.4 (±7.6) |
| CRP, mg/L | 9.3 (2.0–19.0) |
| ESR, mm/h | 27 (14–51) |
| Clinical parameters of RA activity: | |
| TJC | 4 (1–10) |
| SJC | 2 (0–6) |
| PGA (VAS), mm | 38.2 (±26.0) |
| Morning stiffness, minutes | 30.0 (10–75) |
| DAS28 | 4.24 (±1.8) |
| High Disease Activity (DAS28 > 5.1) (n, %) | 48 (36.6) |
| Remission/Low Disease Activity (DAS28 < 3.2) (n, %) | 46 (35.1) |
| M-HAQ | 1.4 (±0.8) |
| US parameters of RA activity: | |
| GSUS score (hypertrophy) | 9 (3–19) |
| PDUS score | 1 (0–4) |
| Global score | 10.5 (4–23) |
| Global score = 0 (n, %) | 15 (12.1) |
| Data/p Value/R | PC | PCT | MPV | PDW |
|---|---|---|---|---|
| DAS28 | <0.001 | <0.001 | NS | 0.02 |
| 0.42 | 0.32 | −0.22 | ||
| TJC | <0.001 | 0.01 | NS | NS |
| 0.29 | 0.23 | |||
| SJC | <0.001 | 0.002 | NS | 0.008 |
| 0.34 | 0.27 | −0.23 | ||
| PGA | 0.005 | 0.02 | 0.02 | NS |
| 0.26 | 0.22 | −0.21 | ||
| Morning stiffness | <0.001 | <0.001 | NS | NS |
| 0.33 | 0.32 | |||
| M-HAQ | 0.05 | NS | NS | NS |
| 0.19 | ||||
| Disease duration | 0.008 | NS | 0.02 | 0.02 |
| −0.23 | 0.21 | 0.21 | ||
| CRP | <0.001 | <0.001 | NS | 0.03 |
| 0.35 | 0.33 | −0.2 | ||
| ESR | <0.001 | <0.001 | NS | <0.001 |
| 0.43 | 0.42 | −0.33 | ||
| WBC | 0.002 | 0.004 | NS | NS |
| 0.29 | 0.25 | |||
| Hb | 0.02 | <0.001 | NS | NS |
| −0.22 | −0.29 |
| Data/p Value/R | GSUS Score | PDUS Score | Global Score |
|---|---|---|---|
| Patients anti-CCP positive: | |||
| PC | NS | 0.02 | NS |
| 0.22 | |||
| PCT | NS | 0.03 | NS |
| 0.22 | |||
| Patients RF-IgM positive: | |||
| PC | 0.04 | 0.001 | 0.02 |
| 0.20 | 0.32 | 0.23 | |
| PCT | NS | 0.009 | 0.04 |
| 0.26 | 0.20 | ||
| Patients with extra-articular symptoms: | |||
| PC | 0.002 | <0.001 | <0.001 |
| 0.36 | 0.44 | 0.39 | |
| PCT | 0.03 | 0.01 | 0.02 |
| 0.32 | 0.30 | 0.28 | |
| Patients with RA duration < 10 years | |||
| PDW | 0.04 | 0.03 | NS |
| −0.28 | −0.29 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Targońska-Stępniak, B.; Grzechnik, K.; Zwolak, R. The Relationship between Platelet Indices and Ultrasound, Clinical, Laboratory Parameters of Disease Activity in Patients with Rheumatoid Arthritis. J. Clin. Med. 2021, 10, 5259. https://doi.org/10.3390/jcm10225259
Targońska-Stępniak B, Grzechnik K, Zwolak R. The Relationship between Platelet Indices and Ultrasound, Clinical, Laboratory Parameters of Disease Activity in Patients with Rheumatoid Arthritis. Journal of Clinical Medicine. 2021; 10(22):5259. https://doi.org/10.3390/jcm10225259
Chicago/Turabian StyleTargońska-Stępniak, Bożena, Krzysztof Grzechnik, and Robert Zwolak. 2021. "The Relationship between Platelet Indices and Ultrasound, Clinical, Laboratory Parameters of Disease Activity in Patients with Rheumatoid Arthritis" Journal of Clinical Medicine 10, no. 22: 5259. https://doi.org/10.3390/jcm10225259
APA StyleTargońska-Stępniak, B., Grzechnik, K., & Zwolak, R. (2021). The Relationship between Platelet Indices and Ultrasound, Clinical, Laboratory Parameters of Disease Activity in Patients with Rheumatoid Arthritis. Journal of Clinical Medicine, 10(22), 5259. https://doi.org/10.3390/jcm10225259