
Association of the KDIGO Risk Classification with the Prevalence of Heart Failure in Patients with Type 2 Diabetes

 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.2. Patients
2.3. Primary Dependent Variable
2.4. Variables Obtained at Inclusion
2.5. Statistical Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [PubMed] [Green Version]
- Shah, A.D.; Langenberg, C.; Rapsomaniki, E.; Denaxas, S.; Rodriguez, M.P.; Gale, C.P.; Deanfield, J.; Smeeth, L.; Timmis, A.; Hemingway, H. Type 2 diabetes and incidence of cardiovascular diseases: A cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015, 3, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Rawshani, A.; Rawshani, A.; Franzén, S.; Sattar, N.; Eliasson, B.; Svensson, A.M.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; Gudbjörnsdottir, S.; et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2018, 379, 633–644. [Google Scholar] [CrossRef]
- Bell, D.S.H.; Goncalves, E. Heart failure in the patient with diabetes: Epidemiology, aetiology, prognosis, therapy and the effect of glucose-lowering medications. Diabetes Obes. Metab. 2019, 21, 1277–1290. [Google Scholar] [CrossRef] [Green Version]
- Jia, G.; Whaley-Connell, A.; Sowers, J.R. Diabetic cardiomyopathy: A hyperglycaemia- and insulin-resistance-induced heart disease. Diabetologia 2018, 61, 21–28. [Google Scholar] [CrossRef]
- Horton, W.B.; Barrett, E.J. Microvascular Dysfunction in Diabetes Mellitus and Cardiometabolic Disease. Endocr. Rev. 2021, 42, 29–55. [Google Scholar] [CrossRef]
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef]
- Kidney Disease Improving Global Outcomes (KDIGO) Chronic Kidney Disease Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2013, 3 (Suppl. 3), 1–150. [Google Scholar]
- Kalyani, R.R. Glucose-Lowering Drugs to Reduce Cardiovascular Risk in Type 2 Diabetes. N. Engl. J. Med. 2021, 384, 1248–1260. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2019, 63, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M. Heart Failure: The Most Important, Preventable, and Treatable Cardiovascular Complication of Type 2 Diabetes. Diabetes Care 2017, 41, 11–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, E.D.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2019, 41, 255–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Addendum. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 44, 125–150. [Google Scholar]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes:Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Pieske, B.; Riley, J.P.; Rosano, G.M.C.; Ruilope, L.M.; et al. 2016 ESC Guidelines for the diagnosis and treat-ment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [PubMed]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure inci-dence: A population-based study of 4 million individuals. Lancet 2018, 391, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; Deswal, A.; Dickson, V.V.; Kosiborod, M.N.; Lekavich, C.L.; et al. American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and the Heart Failure Society of America. Type 2 Diabetes Mellitus and Heart Failure: A Scientific Statement from the American Heart Association and the Heart Failure Society of America: This statement does not represent an update of the 2017 ACC/AHA/HFSA heart failure guideline update. Circulation 2019, 140, e294–e324. [Google Scholar] [CrossRef]
- Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). The survival of patients with heart failure with pre-served or reduced left ventricular ejection fraction: An individual patient data meta-analysis. Eur. Heart J. 2012, 33, 1750–1757. [Google Scholar] [CrossRef] [Green Version]
- Sacre, J.W.; Magliano, D.J.; Shaw, J.E. Incidence of Hospitalization for Heart Failure Relative to Major Atherosclerotic Events in Type 2 Diabetes: A Meta-analysis of Cardiovascular Outcomes Trials. Diabetes Care 2020, 43, 2614–2623. [Google Scholar] [CrossRef]
- Drager, L.F.; McEvoy, R.D.; Barbe, F.; Lorenzi-Filho, G.; Redline, S.; INCOSACT Initiative (International Collaboration of Sleep Apnea Cardiovascular Trialists). Sleep Apnea and Cardiovascular Disease. Lessons from recent trials and need for team science. Circulation 2017, 136, 1840–1850. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. American Heart Association Coun-cil on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiol-ogy; Council on Epidemiology and Prevention; and Stroke Council. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [PubMed]
- Kullo, I.J.; Rooke, T.W. CLINICAL PRACTICE. Peripheral Artery Disease. N. Engl. J. Med. 2016, 374, 861–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonaca, M.P.; Wiviott, S.D.; Zelniker, T.A.; Mosenzon, O.; Bhatt, D.L.; Leiter, L.A.; McGuire, D.K.; Goodrich, E.L.; Furtado, R.H.D.M.; Wilding, J.P.; et al. Dapagliflozin and Cardiac, Kidney, and Limb Outcomes in Patients With and Without Peripheral Artery Disease in DECLARE-TIMI 58. Circulation 2020, 142, 734–747. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Nault, P.; Giugliano, R.P.; Keech, A.C.; Pineda, A.L.; Kanevsky, E.; Kuder, J.; Murphy, S.A.; Jukema, J.W.; Lewis, B.S.; et al. Low-Density Lipoprotein Cholesterol Lowering With Evolocumab and Outcomes in Patients With Peripheral Artery Disease: Insights From the FOURIER Trial (Further Cardiovascular Outcomes Research With PCSK9 Inhibition in Subjects With Elevated Risk). Circulation 2018, 137, 338–350. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.; Mazer, C.D.; Inzucchi, S.E.; Wanner, C.; Ofstad, A.P.; Johansen, O.E.; Zwiener, I.; George, J.T.; Butler, J.; Zinman, B. Impact of polyvascular disease with and without co-existent kidney dysfunction on cardiovascular outcomes in diabetes: A post hoc analysis of EMPA-REG OUTCOME. Diabetes Obes. Metab. 2021, 23, 1173–1181. [Google Scholar] [CrossRef]
- Neuen, B.L.; Ohkuma, T.; Neal, B.; Matthews, D.R.; de Zeeuw, D.; Mahaffey, K.W.; Fulcher, G.; Blais, J.; Li, M.Q.; Jardine, M.J.; et al. Relative and Absolute Risk Reductions in Cardiovascular and Kidney Outcomes With Canagliflozin Across KDIGO Risk Categories: Findings From the CANVAS Program. Am. J. Kidney Dis. 2021, 77, 23–34.e1. [Google Scholar] [CrossRef]
- House, A.A.; Wanner, C.; Sarnak, M.J.; Piña, I.L.; McIntyre, C.W.; Komenda, P.; Kasiske, B.L.; Deswal, A.; Defilippi, C.R.; Cleland, J.G.F.; et al. Heart failure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 1304–1317. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Kim, K.J.; Chung, T.; Bae, J.; Lee, Y.; Lee, B.; Cha, B.; Yun, M.; Kang, E.S. Nonalcoholic fatty liver disease, diastolic dysfunction, and impaired myocardial glucose uptake in patients with type 2 diabetes. Diabetes Obes. Metab. 2021, 23, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Lomonaco, R.; Leiva, E.G.; Bril, F.; Shrestha, S.; Mansour, L.; Budd, J.; Romero, J.P.; Schmidt, S.; Chang, K.-L.; Samraj, G.; et al. Advanced Liver Fibrosis Is Common in Patients With Type 2 Diabetes Followed in the Outpatient Setting: The Need for Systematic Screening. Diabetes Care 2021, 44, 399–406. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Total Group n = 1497 | No Heart Failure n = 943 | Heart Failure n = 554 | p | OR | 95% CI | |
|---|---|---|---|---|---|---|---|
| Age (years) | 67.3 (10.1) | 65.9 (9.9) | 69.8 (9,9) | <0.001 | 1.04 | 1.03–1.05 | |
| Gender (% female) | 501 (33) | 320 (33.9) | 169 (30.5) | 0.17 | 0.86 | 0.68–1.07 | |
| Current smoking (%) | 164 (10.8) | 116 (12.3) | 46 (8.3) | 0.12 | 0.74 | 0.51–1.08 | |
| Hypertension (%) | 1244 (81.9) | 763 (80.9) | 466 (84.1) | 0.12 | 1.25 | 0.94–1.65 | |
| Chronic obstructive pulmonary disease (%) | 166 (10.9) | 79 (8.4) | 85 (15.3) | <0.001 | 1.98 | 1.43–2.75 | |
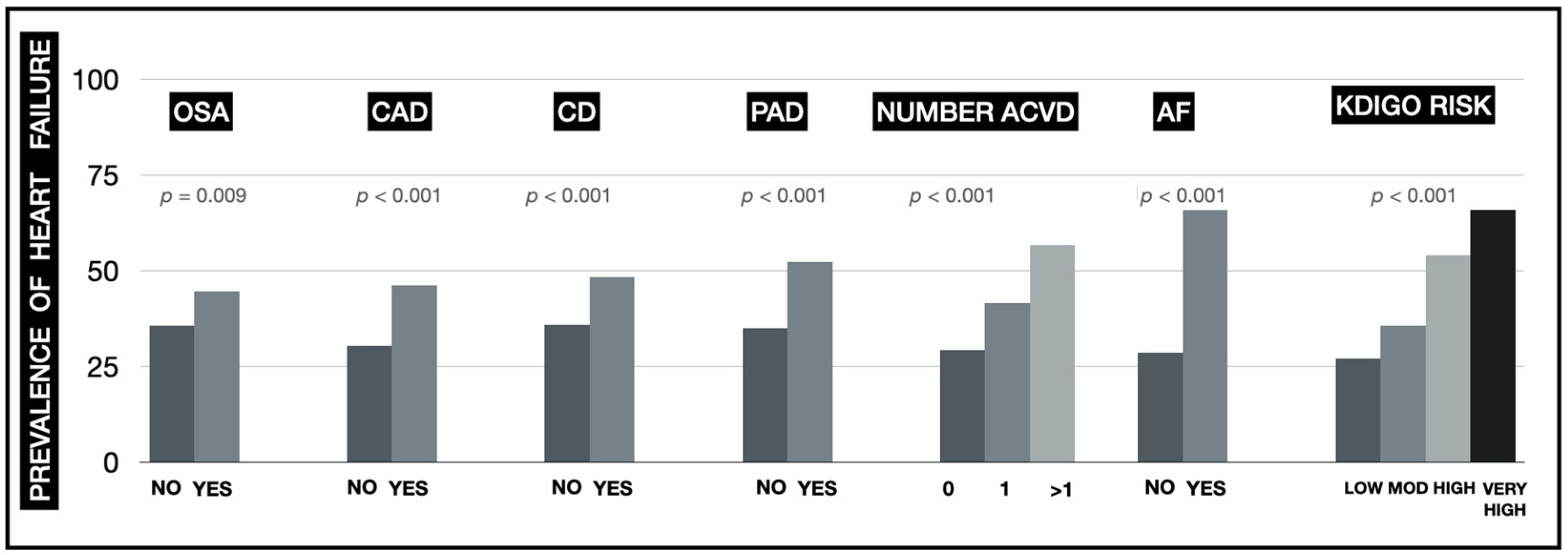
| Obstructive sleep apnoea (%) | 232 (15.3) | 126 (13.4) | 102 (18.4) | 0.009 | 1.46 | 1.10–1.95 | |
| Fatty liver disease (%) | 181 (12.1) | 132 (14.2) | 43 (7.8) | <0.001 | 0.51 | 0.35–0.73 | |
| Auricular fibrillation (%) | 327 (21.6) | 108 (11.4) | 217 (39.2) | <0.001 | 4.98 | 3.83–6.48 | |
| Coronary artery disease (%) | 633 (41.9) | 339 (36) | 291 (52.5) | <0.001 | 1.97 | 1.59–2.44 | |
| Cerebrovascular disease (%) | 128 (8.5) | 66 (7) | 62 (11.2) | <0.001 | 1.67 | 1.16–2.41 | |
| Peripheral artery disease (%) | 164 (10.8) | 78 (8.3) | 86 (15.5) | <0.001 | 2.04 | 1.47–2.82 | |
| Atherosclerotic cardiovascular disease (%) | 741 (49) | 406 (43) | 332 (59.9) | <0.001 | 1.98 | 1.60–2.45 | |
| Number of vascular territories affected | 0 (%) | 771 (51) | 537 (57) | 222 (40.1) | <0.001 | 1 | - |
| 1 (%) | 577 (38.2) | 335 (35.5) | 239 (43.1) | 1.73 | 1.37–2.17 | ||
| >1 (%) | 164 (10.8) | 71 (7.5) | 93 (16.8) | 3.17 | 2.24–4.48 | ||
| Charlson index (points) | 0.62 (0.88) | 0.52 (0.8) | 0,81 (0.98) | <0.001 | 1.44 | 1.28–1.62 | |
| Retinopathy | Simple (%) | 114 (7.6) | 77 (8.2) | 32 (5.8) | 0.29 | 0.69 | 0.45–1.05 |
| Proliferative (%) | 74 (4.9) | 45 (4.8) | 29 (5.2) | 1.07 | 0.66–1.72 | ||
| Body mass index (Kg/m2) | 30.3 (5.2) | 30.3 (5.1) | 30.1 (5.4) | 0.57 | 1.00 | 0.98–1.02 | |
| Systolic blood pressure (mmHg) | 135 (19.4) | 138 (18) | 129 (21) | <0.001 | 0.98 | 0.97–0.98 | |
| Diastolic blood pressure (mmHg) | 76 (11.5) | 77 (11) | 73 (11) | <0.001 | 0.96 | 0.95–0.97 | |
| Diabetes duration (years) | 14 (11.1) | 13.7 (9.9) | 14.7 (12.9) | 0.14 | 1.01 | 1.00–1.02 | |
| HbA1c (%) | 7.3 (1.3) | 7.3 (1.3) | 7.2 (1.3) | 0.12 | 0.94 | 0.86–1.02 | |
| Non-HDL cholesterol (mg/dL) | 109 (34.1) | 110 (34) | 107 (35) | 0.04 | 0.99 | 0.99–1.00 | |
| Triglycerides (mg/dL) * | 133 (85) | 129 (87) | 136 (82) | 0.55 | 1.00 | 0.99–1.00 | |
| Haemoglobin (g/dL) | 14 (1.8) | 14.3 (1.7) | 13.6 (1.9) | <0.001 | 0.82 | 0.77–0.87 | |
| NT-proBNP (pg/mL) * | 243 (782) | 127 (245) | 851 (1958) | <0.001 | 1.001 | 1.000–1.002 | |
| Glomerular filtration rate (mL/min/1.73 m2) | 73.1 (22.7) | 77.9(20.8) | 64.6 (23.5) | <0.001 | 0.97 | 0.96–0.98 | |
| Urinary albumin excretion (mg/g) | 87 (393) | 62 (201) | 132 (603) | 0.017 | 1.001 | 1.000–1.001 | |
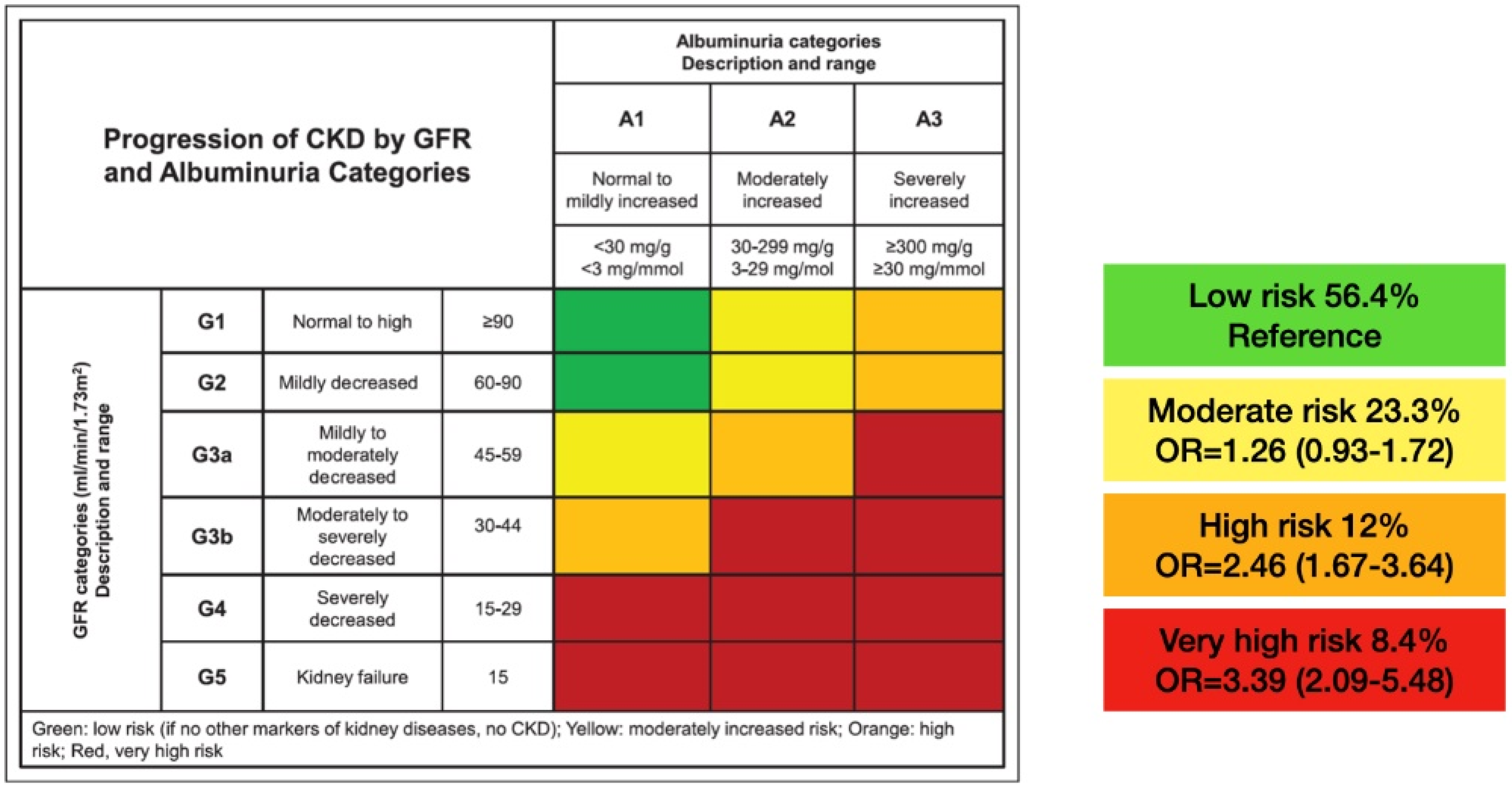
| KDIGO risk | Low (%) | 715 (56.4) | 518 (63.6) | 194 (43) | <0.001 | 1 | - |
| Moderate (%) | 295 (23.3) | 190 (23.4) | 105 (23.3) | 1.48 | 1.10–1.97 | ||
| High (%) | 152 (12) | 70 (8.6) | 82 (18.2) | 3.13 | 2.18–4.48 | ||
| Very high (%) | 106 (8.4) | 36 (4.4) | 70 (15.5) | 5.19 | 3.36–8.02 | ||
| Variable | Total Group n = 1497 | Group 1: No Heart Failure n = 943 | Group 2: HF with EF < 40% n = 240 | Group 3: HF with EF ≥ 40% n = 314 | p | p Group 2 vs 3 | |
|---|---|---|---|---|---|---|---|
| Age (years) | 67.3 (10.1) | 65.9 (9.9) | 68.1 (9.9) | 71.1 (9.7) | <0.001 | <0.001 | |
| Gender (% female) | 501 (33) | 320 (33.9) | 52 (21.7) | 117 (37.2) | <0.001 | <0.001 | |
| Current smoking (%) | 164 (10.8) | 116 (12.3) | 27 (11.2) | 19 (6.1) | <0.001 | 0.017 | |
| Hypertension (%) | 1244 (81.9) | 763 (80.9) | 188 (78.3) | 278 (88.5) | 0.002 | 0.001 | |
| Chronic obstructive pulmonary disease (%) | 166 (10.9) | 79 (8.4) | 39 (16.2) | 46 (14.6) | <0.001 | 0.60 | |
| Obstructive sleep apnoea (%) | 232 (15.3) | 126 (13.4) | 37 (15.4) | 65 (20.7) | 0.007 | 0.11 | |
| Fatty liver disease (%) | 181 (12.1) | 132 (14.2) | 14 (5.9) | 29 (9.3) | <0.001 | 0.14 | |
| Auricular fibrillation (%) | 327 (21.6) | 108 (11.4) | 92 (38.3) | 125 (39.8) | <0.001 | 0.72 | |
| Coronary artery disease (%) | 633 (41.9) | 339 (36) | 148 (61.6) | 143 (45.5) | <0.001 | <0.001 | |
| Cerebrovascular disease (%) | 128 (8.5) | 66 (7) | 28 (11.7) | 34 (10.8) | 0.019 | 0.76 | |
| Peripheral artery disease (%) | 164 (10.8) | 78 (8.3) | 37 (15.4) | 49 (15.6) | <0.001 | 0.95 | |
| Atherosclerotic cardiovascular disease (%) | 741 (49) | 406 (43) | 164 (68.3) | 168 (53.5) | <0.001 | <0.001 | |
| Number of vascular territories affected | 0 | 771 (51) | 537 (57) | 76 (31.7) | 146 (46.5) | <0.001 | 0.002 |
| 1 | 577 (38.2) | 335 (35.5) | 120 (50) | 119 (37.9) | |||
| >1 | 164 (10.8) | 71 (7.5) | 44 (18.3) | 49 (15.6) | |||
| Charlson index (points) | 0.62 (0.88) | 0.52 (0.8) | 0.78 (0.95) | 0.83 (1.00) | <0.001 | 0.50 | |
| Retinopathy | Simple (%) | 114 (7.6) | 77 (8.2) | 14 (5.8) | 18 (5.7) | 0.64 | 0.88 |
| Proliferative (%) | 74 (4.9) | 45 (4.8) | 13 (5.4) | 16 (5.1) | |||
| Body mass index (Kg/m2) | 30.3 (5.2) | 30.3 (5.1) | 29.4 (5.3) | 30.7 (5.4) | 0.012 | 0.005 | |
| Systolic blood pressure (mmHg) | 135 (19.4) | 138 (18) | 126 (19.8) | 132 (19.8) | <0.001 | <0.001 | |
| Diastolic blood pressure (mmHg) | 76 (11.5) | 77 (11) | 72 (11.8) | 73 (11.2) | <0.001 | 0.10 | |
| Diabetes duration (years) | 14 (11.1) | 13.7 (9.9) | 15.4 (15.3) | 14.1 (10.7) | 0.1 | 0.46 | |
| HbA1c (%) | 7.3 (1.3) | 7.3 (1.3) | 7.2 (1.2) | 7.3 (1.3) | 0.26 | 0.58 | |
| Non-HDL cholesterol (mg/dL) | 109 (34.1) | 110 (34) | 104 (34) | 109 (35) | 0.026 | 0.09 | |
| Triglycerides (mg/dL) * | 133 (85) | 129 (87) | 134 (82) | 138 (84) | 0.33 | 0.16 | |
| Haemoglobin (g/dL) | 14 (1.8) | 14.3 (1.7) | 13.9 (1.9) | 13.4 (1.8) | <0.001 | 0.004 | |
| NT-proBNP (pg/mL) * | 243 (782) | 127 (245) | 1089(2661) | 627 (1563) | <0.001 | 0.038 | |
| Ejection Fraction (%) | 54.9 (13.4) | 61.5 (7.6) | 32.8 (7.9) | 54 (10.4) | <0.001 | <0.001 | |
| Glomerular filtration rate (mL/min/1.73 m2) | 73.1 (22.7) | 77.9 (20.8) | 66.3 (23.1) | 66.3 (23.8) | <0.001 | 0.14 | |
| Urinary albumin excretion (mg/g) | 87 (393) | 62 (201) | 165 (825) | 112 (404) | 0.004 | 0.36 | |
| KDIGO risk | Low (%) | 715 (56.4) | 518 (63.6) | 73 (41.7) | 121 (43.8) | <0.001 | 0.97 |
| Moderate (%) | 295 (23.3) | 190 (23.4) | 42 (24) | 63 (22.8) | |||
| High (%) | 152 (12) | 70 (8.6) | 33 (18.9) | 49 (17.7) | |||
| Very high (%) | 106 (8.4) | 36 (4.4) | 27 (15.4) | 43 (15.6) | |||
| Variable | OR | 95% CI | p | |
|---|---|---|---|---|
| Age (years) | 1.02 | 1.01–1.03 | 0.006 | |
| Obstructive sleep apnoea | 1.61 | 1.14–2.25 | 0.006 | |
| Fatty liver disease | 0.59 | 0.39–0.91 | 0.016 | |
| Coronary artery disease | 1.66 | 1.31–2.11 | <0.001 | |
| Peripheral artery disease | 1.53 | 1.06-2.23 | 0.025 | |
| Number of vascular territories affected | 0 | 1 | - | |
| 1 | 1.38 | 1.05–1.81 | 0.02 | |
| >1 | 2.39 | 1.59–3.60 | <0.001 | |
| Systolic blood pressure (mmHg) | 0.98 | 0.97–0.99 | <0.001 | |
| Haemoglobin (g/dL) | 0.86 | 0.80–0.93 | <0.001 | |
| Glomerular filtration rate (mL/min/1.73 m2) | 0.976 | 0.97–0.98 | <0.001 | |
| KDIGO risk | Low | 1 | - | |
| Moderate | 1.26 | 0.93–1.72 | 0.14 | |
| High | 2.46 | 1.67–3.64 | <0.001 | |
| Very high | 3.39 | 2.09–5.48 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gimeno-Orna, J.A.; Rodríguez-Padial, L.; Anguita-Sánchez, M.; Barrios, V.; Muñiz, J.; Pérez, A. Association of the KDIGO Risk Classification with the Prevalence of Heart Failure in Patients with Type 2 Diabetes. J. Clin. Med. 2021, 10, 4634. https://doi.org/10.3390/jcm10204634
Gimeno-Orna JA, Rodríguez-Padial L, Anguita-Sánchez M, Barrios V, Muñiz J, Pérez A. Association of the KDIGO Risk Classification with the Prevalence of Heart Failure in Patients with Type 2 Diabetes. Journal of Clinical Medicine. 2021; 10(20):4634. https://doi.org/10.3390/jcm10204634
Chicago/Turabian StyleGimeno-Orna, José Antonio, Luis Rodríguez-Padial, Manuel Anguita-Sánchez, Vivencio Barrios, Javier Muñiz, and Antonio Pérez. 2021. "Association of the KDIGO Risk Classification with the Prevalence of Heart Failure in Patients with Type 2 Diabetes" Journal of Clinical Medicine 10, no. 20: 4634. https://doi.org/10.3390/jcm10204634
APA StyleGimeno-Orna, J. A., Rodríguez-Padial, L., Anguita-Sánchez, M., Barrios, V., Muñiz, J., & Pérez, A. (2021). Association of the KDIGO Risk Classification with the Prevalence of Heart Failure in Patients with Type 2 Diabetes. Journal of Clinical Medicine, 10(20), 4634. https://doi.org/10.3390/jcm10204634