
Patient-Centered Treatment Outcomes with Full-Arch PEEK Rehabilitation Supported on Four Immediate or Conventionally Loaded Implants. A Randomized Clinical Trial

 ,
,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
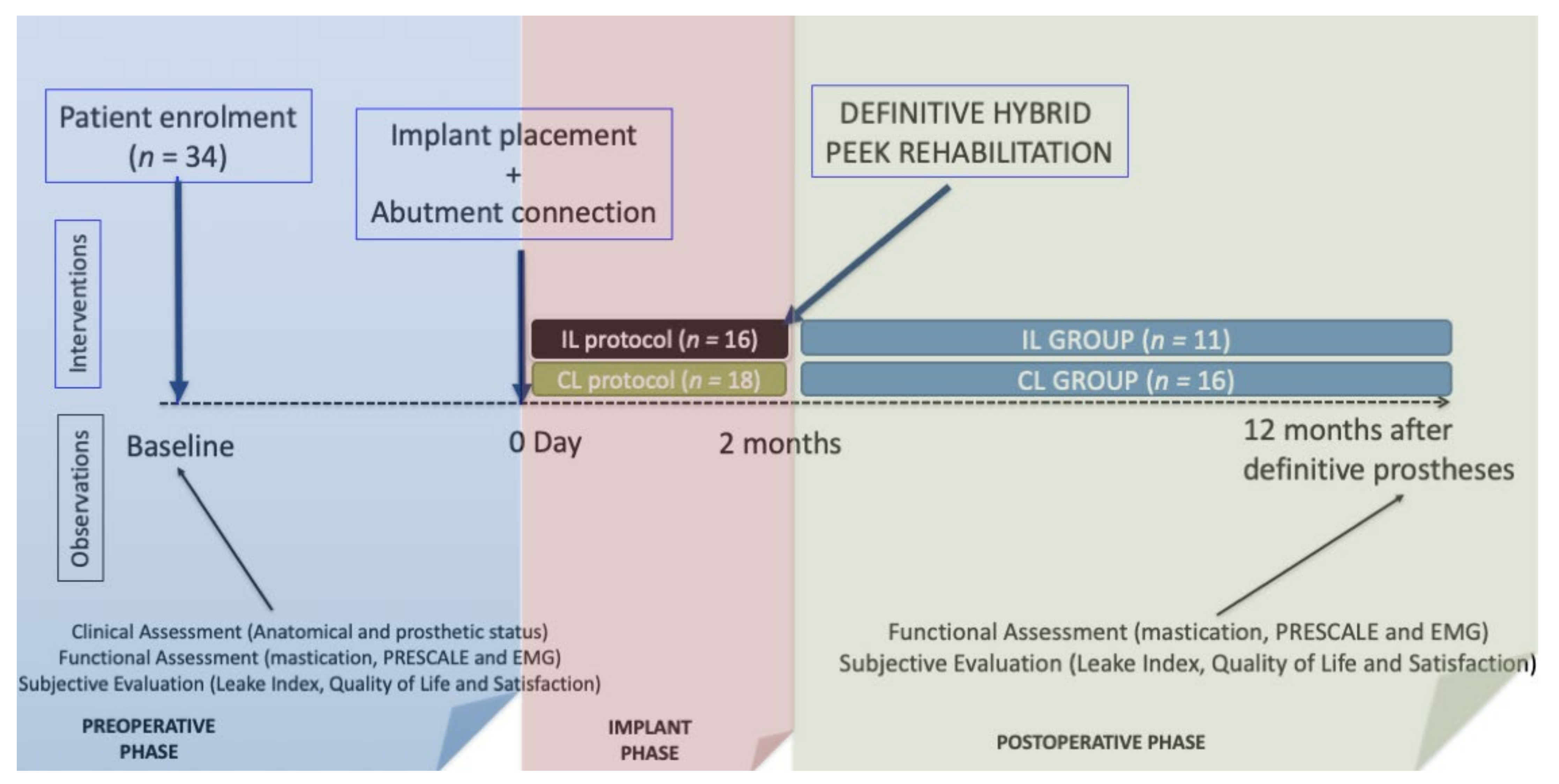
2.1. Study Design
2.2. Preoperative Assessments
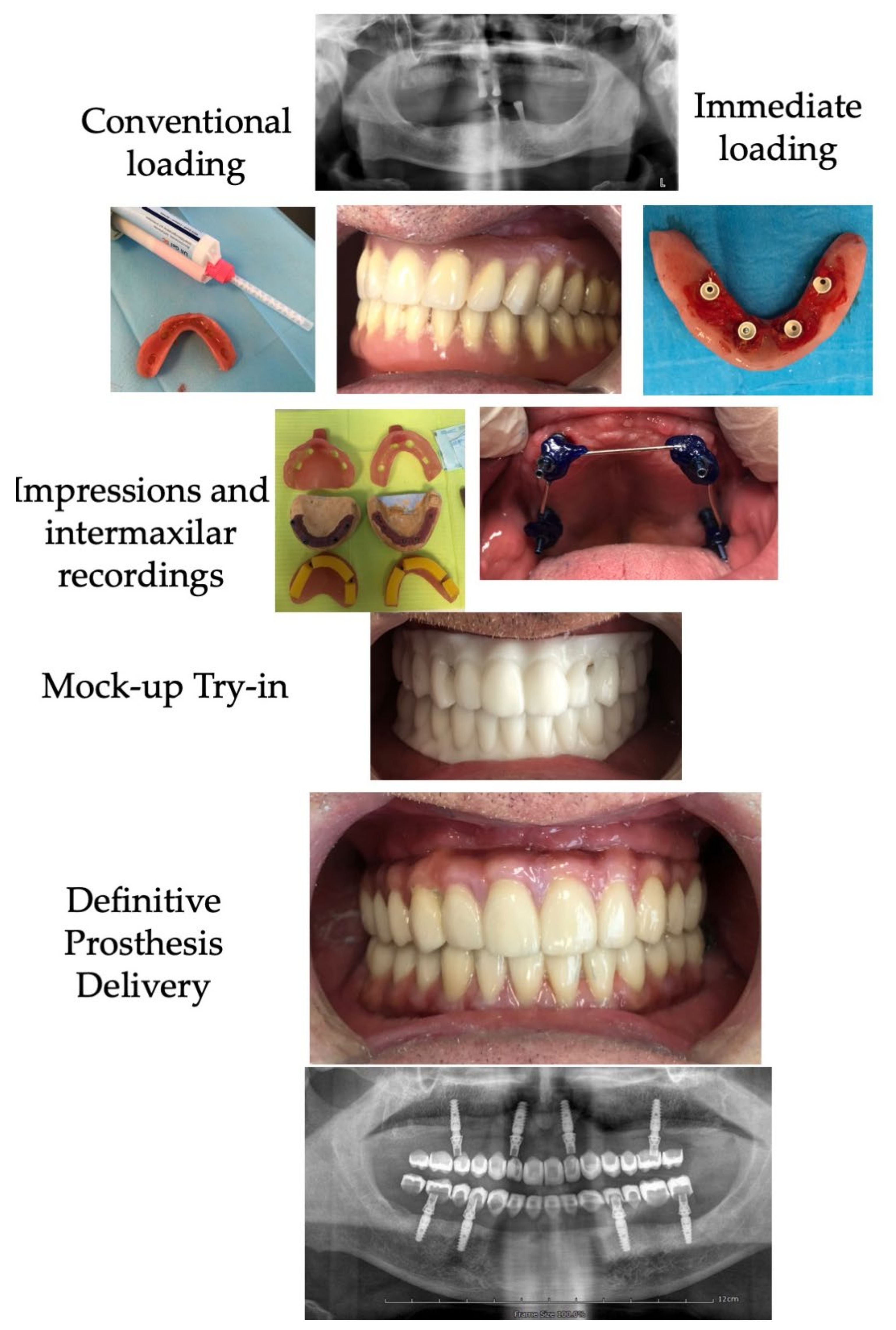
2.3. Surgical and Prosthetic Treatment Protocol
2.4. Postoperative Assessments
Data Analysis
3. Results
3.1. Sample Description
3.2. Baseline Anatomical Conditions
3.3. Type of Rehabilitation and Distribution of Implant and Abutment Sizes
3.4. Change in the Occlusal Parameters after Prosthetic Treatments
3.5. Change of the EMG Muscular Activity after PEEK-Hybrid Rehabilitation
3.6. Change in Chewing Ability by Leake Index
3.7. Change in Self-Rated Satisfaction One Year after Prosthetic Treatments
3.8. Change in Oral Health-Related Quality of Life after Prosthetic Treatments
3.9. Retrospective Self-Assessment of the Wellbeing Change by Global Transitional Items
3.10. Changes in Masticatory Performance by Mixing Ability Tests
3.11. Predictors of Patient-Centered Treatment Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pérez, M.; Almerich Silla, J.M.; Canorea Díaz, E.; Casal Peidro, E.; Cortés Martinicorea, F.J.; Expósito Delgado, A.J.; Gómez Santos, G.; Hidalgo Olivares, G.; Lamas Oliveira, M.; Martínez Beneyto, Y.; et al. Encuesta de Salud Oral en España. 2020. Available online: https://rcoe.es/articulo/115/encuesta-de-salud-oral-en-espaa-2020 (accessed on 20 September 2020).
- Montero, J.; Bravo, M.; Vicente, M.-P.; Galindo, M.-P.; Lopez-Valverde, A.; Casals, E.; Cortes-Martinicorena, F.-J.; Llodra, J.-C. Oral pain and eating problems in Spanish adults and elderly in the Spanish National Survey performed in 2005. J. Orofac. Pain 2011, 25, 141–152. [Google Scholar]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Brånemark, P.I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Thomason, J.M.; Feine, J.; Exley, C.; Moynihan, P.; Müller, F.; Naert, I.; Ellis, J.; Barclay, C.; Butterworth, C.; Scott, B.; et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients—The York Consensus Statement. Br. Dent. J. 2009, 207, 185–186. [Google Scholar] [CrossRef]
- Attard, N.; Wei, X.; Laporte, A.; Zarb, G.A.; Ungar, W.J. A cost minimization analysis of implant treatment in mandibular edentulous patients. Int. J. Prosthodont. 2003, 16, 271–276. [Google Scholar]
- Müller, F.; Hernandez, M.; Grütter, L.; Aracil-Kessler, L.; Weingart, D.; Schimmel, M. Masseter muscle thickness, chewing efficiency and bite force in edentulous patients with fixed and removable implant-supported prostheses: A cross-sectional multicenter study. Clin. Oral Implant. Res. 2011, 23, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Borges, G.A.; Barbin, T.; Dini, C.; Maia, L.C.; Magno, M.B.; Barão, V.A.R.; Mesquita, M.F. Patient-reported outcome measures and clinical assessment of implant-supported overdentures and fixed prostheses in mandibular edentulous patients: A systematic review and meta-analysis. J. Prosthet. Dent. 2020. [Google Scholar] [CrossRef]
- Brennan, M.; Houston, F.; O’Sullivan, M.; O’Connell, B. Patient satisfaction and oral health-related quality of life outcomes of implant overdentures and fixed complete dentures. Int. J. Oral Maxillofac. Implant. 2010, 25, 791–800. [Google Scholar]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 22–38. [Google Scholar] [CrossRef]
- Drago, C.; Howell, K. Concepts for Designing and Fabricating Metal Implant Frameworks for Hybrid Implant Prostheses. J. Prosthodont. 2012, 21, 413–424. [Google Scholar] [CrossRef]
- Qamheya, A.H.A.; Yeniyol, S.; Arısan, V. Full Mouth Oral Rehabilitation by Maxillary Implant Supported Hybrid Denture Employing a Fiber Reinforced Material Instead of Conventional PMMA. Case Rep. Dent. 2015, 2015, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Stawarczyk, B.; Beuer, F.; Wimmer, T.; Jahn, D.; Sener, B.; Roos, M.; Schmidlin, P.R. Polyetheretherketone—A suitable material for fixed dental prostheses? J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1209–1216. [Google Scholar] [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Guedes, C.M.; Almeida, R.; Silva, A.; Sereno, N.; Legatheaux, J. Short-term report of an ongoing prospective cohort study evaluating the outcome of full-arch implant-supported fixed hybrid polyetheretherketone-acrylic resin prostheses and the All-on-Four concept. Clin. Implant. Dent. Relat. Res. 2018, 20, 692–702. [Google Scholar] [CrossRef]
- De Araújo Nobre, M.; Mouda Guedes, C.; Almeida, R.; Silva, A.; Sereno, N. Hybrid Polyetheretherketone (PEEK)–Acrylic Resin Prostheses and the All-on-4 Concept: A Full-Arch Implant-Supported Fixed Solution with 3 Years of Follow-Up. J. Clin. Med. 2020, 9, 2187. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H. Interventions for replacing missing teeth: Different times for loading dental implants. Cochrane Database Syst. Rev. 2013, 28, CD003878. [Google Scholar] [CrossRef] [Green Version]
- Kittur, N.; Oak, R.; Dekate, D.; Jadhav, S.; Dhatrak, P. Dental implant stability and its measurements to improve osseointegration at the bone-implant interface: A review. Mater. Today 2020, 43, 1064–1070. [Google Scholar] [CrossRef]
- Montero, J.; Macedo, C.; Lopez-Valverde, A.; Bravo, M. Validation of the oral health impact profile (OHIP-20sp) for Spanish edentulous patients. Med. Oral. Patol. Oral. Cir. Bucal 2012, 17, e469–e476. [Google Scholar] [CrossRef] [Green Version]
- Montero, J.; Leiva, L.A.; Martín-Quintero, I.; Barrios-Rodríguez, R. Chewing Performance Calculator: An interactive clinical method for quantifying masticatory performance. J. Prosthet. Dent. 2021, 125, 82–88. [Google Scholar] [CrossRef]
- Leake, J.L. An Index of Chewing Ability. J. Public Health Dent. 1990, 50, 262–267. [Google Scholar] [CrossRef]
- Montero, J.; Bravo, M.; Albaladejo, A. Validation of two complementary oral-health related quality of life indicators (OIDP and OSS 0-10) in two qualitatively distinct samples of the Spanish population. Health Qual. Life Outcomes 2008, 6, 101. [Google Scholar] [CrossRef] [Green Version]
- Lekholm, U.; Zarb, G.A. Patient Selection and Preparation. In Tissue-Integrated Prostheses: Osseointegration in Clinical Dentistry; Branemark, P.I., Zarb, G.A., Albrektsson, T., Eds.; Quintessence: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Montero, J. A Review of the Major Prosthetic Factors Influencing the Prognosis of Implant Prosthodontics. J. Clin. Med. 2021, 10, 816. [Google Scholar] [CrossRef]
- Montero, J.; Dib, A. The effect of age and prosthodontic status on the clinical and electromyographic assessment of the interocclusal rest space. J. Prosthet. Dent. 2019, 121, 791–796. [Google Scholar] [CrossRef]
- Locker, D.; Jokovic, A.; Clarke, M. Assessing the responsiveness of measures of oral health-related quality of life. Community Dent. Oral Epidemiol. 2004, 32, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.E.; Sprangers, M.A. Methodological approaches for assessing response shift in longitudinal health-related quality-of-life research. Soc. Sci. Med. 1999, 48, 1531–1548. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis of the Behavioural Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdadle, NJ, USA, 1988. [Google Scholar]
- Montero, J.; Dib, A.; Guadilla, Y.; Flores, J.; Pardal-Peláez, B.; Quispe-López, N.; Gómez-Polo, C. Functional and Patient-Centered Treatment Outcomes with Mandibular Overdentures Retained by Two Immediate or Conventionally Loaded Implants: A Randomized Clinical Trial. J. Clin. Med. 2021, 10, 3477. [Google Scholar] [CrossRef] [PubMed]
- Baca, E.; Yengin, E.; Gökçen-Röhlig, B.; Sato, S. In Vivo evaluation of occlusal contact area and maximum bite force in patients with various types of implant-supported prostheses. Acta Odontol. Scand. 2013, 71, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kumagai, H.; Yoshitomi, N.; McGlumphy, E.A. Occlusal contacts of edentulous patients with mandibular hybrid dentures opposing maxillary complete dentures. Int. J. Oral Maxillofac. Implant. 1999, 14, 504–509. [Google Scholar]
- Iwaki, M.; Kanazawa, M.; Sato, D.; Miyayasu, A.; Minakuchi, S. Masticatory Function of Immediately Loaded Two-Implant Mandibular Overdentures: A 5-year Prospective Study. Int. J. Oral Maxillofac. Implant. 2019, 34, 1434–1440. [Google Scholar] [CrossRef]
- Suzuki, T.; Kumagai, H.; Watanabe, T.; Uchida, T.; Nagao, M. Evaluation of complete denture occlusal contacts using pressure-sensitive sheets. Int. J. Prosthodont. 1997, 10, 386–391. [Google Scholar]
- Von Der Gracht, I.; Derks, A.; Haselhuhn, K.; Wolfart, S. EMG correlations of edentulous patients with implant overdentures and fixed dental prostheses compared to conventional complete dentures and dentates: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2016, 28, 765–773. [Google Scholar] [CrossRef]
- Giannakopoulos, N.N.; Corteville, F.; Kappel, S.; Rammelsberg, P.; Schindler, H.J.; Eberhard, L. Functional adaptation of the masticatory system to implant-supported mandibular overdentures. Clin. Oral Implant. Res. 2017, 28, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Boven, G.C.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Improving masticatory performance, bite force, nutritional state and patient’s satisfaction with implant overdentures: A systematic review of the literature. J. Oral Rehabil. 2015, 42, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Yadav, H.; Pathak, A.; Bhatnagar, A.; Kumar, V. Comparative evaluation of biting force and chewing efficiency of all-on-four treatment concept with other treatment modalities in completely edentulous individuals. J. Indian Prosthodont. Soc. 2020, 20, 312–320. [Google Scholar] [CrossRef]
- Carlsson, G.E.; Lindquist, L.W. Ten-year longitudinal study of masticatory function in edentulous patients treated with fixed complete dentures on osseointegrated implants. Int. J. Prosthodont. 1994, 7, 448–453. [Google Scholar]
- Fueki, K.; Kimoto, K.; Ogawa, T.; Garrett, N.R. Effect of implant-supported or retained dentures on masticatory performance: A systematic review. J. Prosthet. Dent. 2007, 98, 470–477. [Google Scholar] [CrossRef]
- Prithviraj, D.R.; Madan, V.; Harshamayi, P.; Kumar, C.G.; Vashisht, R. A comparison of masticatory efficiency in conventional dentures, implant retained or supported overdentures and implant supported fixed prostheses: A literature review. J. Dent. Implant. 2014, 4, 153–157. [Google Scholar] [CrossRef]
- Preciado, A.; Del Río, J.; Lynch, C.D.; Castillo-Oyagüe, R. A new, short, specific questionnaire (QoLIP-10) for evaluating the oral health-related quality of life of implant-retained overdenture and hybrid prosthesis wearers. J. Dent. 2013, 41, 753–763. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Sridharan, K. Comparison of implant supported mandibular overdentures and conventional dentures on quality of life: A systematic review and meta-analysis of randomized controlled studies. Aust. Dent. J. 2016, 61, 482–488. [Google Scholar] [CrossRef]
- Schuster, A.J.; Marcello-Machado, R.M.; Bielemann, A.M.; Possebon, A.P.D.R.; Chagas Junior, O.L.; Faot, F. Immediate vs. conventional loading of Facility-Equator system in mandibular overdenture wearers: 1-year RCT with clinical, biological, and functional evaluation. Clin. Implant. Dent. Relat. Res. 2020, 22, 270–280. [Google Scholar] [CrossRef]
- De Kok, I.J.; Chang, K.H.; Lu, T.S.; Cooper, L.F. Comparison of three-implant-supported fixed dentures and two-implant-retained overdentures in the edentulous mandible: A pilot study of treatment efficacy and patient satisfaction. Int. J. Oral Maxillofac. Implant. 2011, 26, 415–426. [Google Scholar]
- Omura, Y.; Kanazawa, M.; Sato, D.; Kasugai, S.; Minakuchi, S. Comparison of patient-reported outcomes between immediately and conventionally loaded mandibular two-implant overdentures: A preliminary study. J. Prosthodont. Res. 2016, 60, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erkapers, M.; Ekstrand, K.; Baer, R.A.; Toljanic, J.A.; Thor, A. Patient satisfaction following dental implant treatment with immediate loading in the edentulous atrophic maxilla. Int. J. Oral Maxillofac. Implant. 2011, 26, 356–364. [Google Scholar]
- Papathanasiou, I.; Kamposiora, P.; Papavasiliou, G.; Ferrari, M. The use of PEEK in digital prosthodontics: A narrative review. BMC Oral Health 2020, 20, 217. [Google Scholar] [CrossRef]
- Zoidis, P. The all-on-4 modified polyetheretherketone treatment approach: A clinical report. J. Prosthet. Dent. 2018, 119, 516–521. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Sociodemographic | All Patients (n = 34; 100%) | IL Group (n = 16; 47.1%) | CL Group (n = 18; 52.9%) | |||
|---|---|---|---|---|---|---|
| Age Interval | N | % | N | % | N | % |
| 40–59 yrs | 8 | 23.5 | 5 | 21.3 | 3 | 16.7 |
| 60–70 yrs | 17 | 50.0 | 7 | 43.8 | 10 | 55.6 |
| >70 yrs | 9 | 26.5 | 4 | 25.0 | 5 | 27.8 |
| Mean | SD | Mean | SD | Mean | SD | |
| Age (yrs) | 65.0 | 10.0 | 62.8 | 11.9 | 67.0 | 7.8 |
| Gender | N | % | N | % | N | % |
| Female | 15 | 44.1 | 7 | 43.8 | 8 | 44.4 |
| Male | 19 | 55.9 | 9 | 56.3 | 10 | 55.6 |
| Socio-occupational class | N | % | N | % | N | % |
| Low | 19 | 55.9 | 10 | 62.5 | 9 | 50.0 |
| Medium | 15 | 44.1 | 6 | 37.5 | 9 | 50.0 |
| Place of residence | N | % | N | % | N | % |
| Urban | 21 | 61.8 | 10 | 62.5 | 11 | 61.1 |
| Peri-urban | 3 | 8.8 | 2 | 12.5 | 1 | 5.6 |
| Rural | 10 | 29.4 | 4 | 25.0 | 6 | 33.3 |
| Behavioral | ||||||
| Brushing habits | N | % | N | % | N | % |
| 2–3 times a day | 7 | 20.6 | 3 | 18.8 | 4 | 22.2 |
| Once a day | 16 | 47.1 | 6 | 37.5 | 10 | 55.6 |
| Less than once a day | 11 | 32.4 | 7 | 43.8 | 4 | 22.2 |
| Smoking habits | N | % | N | % | N | % |
| Non-smoker | 17 | 50.0 | 7 | 43.8 | 10 | 55.6 |
| Current smoker | 10 | 29.4 | 5 | 31.2 | 5 | 27.8 |
| Past Smoker | 7 | 20.6 | 4 | 25.0 | 3 | 16.6 |
| Mean | Sd | Mean | Sd | Mean | Sd | |
| Cigarettes/day in smokers | 13.5 | 5.3 | 12.8 | 5.1 | 14.3 | 5.9 |
| All Patients (n = 34; 100%) | IL Group (n = 16; 47.1%) | CL Group (n = 18; 52.9%) | ||||
|---|---|---|---|---|---|---|
| Bone Quality in Maxilla according to Leckholm and Zarb (n = 28 patients) | ||||||
| N | % | N | % | N | % | |
| Type I | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Type II | 2 | 7.1 | 1 | 7.1 | 1 | 7.1 |
| Intermediate | 8 | 28.6 | 7 | 50.0 | 1 | 7.1 |
| Type III | 11 | 39.3 | 4 | 28.6 | 7 | 50.0 |
| Intermediate | 3 | 10.7 | 1 | 7.1 | 2 | 14.3 |
| Type IV | 4 | 14.3 | 1 | 7.1 | 3 | 21.4 |
| Total | 28 | 100.0 | 14 | 100.0 | 18 | 100 |
| Bone Quality in the mandible according to Leckholm and Zarb (n = 22 patients) | ||||||
| Type I | 1 | 4.5 | 0 | 0.0 | 1 | 9.1 |
| Type II | 8 | 36.4 | 4 | 36.4 | 4 | 36.4 |
| Intermediate | 10 | 45.5 | 5 | 45.5 | 5 | 45.5 |
| Type III | 3 | 13.6 | 2 | 18.2 | 1 | 9.1 |
| Intermediate | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Type IV | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Total | 22 | 100 | 11 | 100 | 11 | 100 |
| Gingival Biotype in MAXILLA | ||||||
| Gingival Biotype | N | % | N | % | N | % |
| fine | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| medium | 14 | 50.0 | 7 | 50.0 | 7 | 50.0 |
| thick | 14 | 50.0 | 7 | 50.0 | 7 | 50.0 |
| Gingival Biotype in MANDIBLE | ||||||
| Gingival Biotype | N | % | N | % | N | % |
| fine | 5 | 22.7 | 3 | 27.3 | 2 | 18.2 |
| medium | 14 | 63.6 | 6 | 54.5 | 8 | 72.7 |
| thick | 3 | 13.6 | 2 | 18.2 | 1 | 9.1 |
| Mean | Sd | Mean | Sd | Mean | Sd | |
| Implant-Related Variables | All Patients (n = 34 Patients with 210 Implants) | IL Group (n = 16 Patients with 96 Implants) | CL Group (n = 18 Patients with 114 Implants) | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Type of hybrid PEEK-NFC Rehabilitation | ||||||
| Lower PEEK | 6 | 17.6 | 2 | 12.5 | 4 | 22.2 |
| Upper PEEK | 11 | 32.4 | 5 | 31.3 | 6 | 33.3 |
| Bimaxilar PEEK | 17 | 50.0 | 9 | 56.3 | 8 | 44.4 |
| Type of Antagonist | ||||||
| Partial Denture | 3 | 8.8 | 0 | 0.0 | 3 | 16.7 |
| Fixed implant-supported prosthesis | 10 | 29.4 | 4 | 25.0 | 6 | 33.3 |
| Fixed tooth-supported denture/Natural | 21 | 61.8 | 12 | 75.0 | 9 | 50.0 |
| Number of Implants | Mean | Sd | Mean | Sd | Mean | Sd |
| Total | 6.3 | 2.3 | 6.8 | 2.5 | 5.8 | 2.1 |
| Postextractive implants | 1.4 | 1.3 | 1.8 | 1.3 | 1.1 | 1.2 |
| N | % | N | % | N | % | |
| Baseline Records | All Patients (n = 34 Patients at Baseline; n = 27 at Follow-Up) | IL Group (n = 16 at Baseline; n = 11 at Follow-Up) | CL Group (n = 18 Patients at Baseline; n = 16 at Follow-Up) | |||
|---|---|---|---|---|---|---|
| Full Arch | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 13.5 a | 10.6 | 13.6 a | 9.8 | 13.4 a | 11.5 |
| Average Pressure (MPa) | 12.2 a | 13.7 | 13.0 a | 4.8 | 11.5 a | 2.4 |
| Maximal Pressure (MPa) | 35.4 a | 7.1 | 36.6 a | 9.4 | 34.3 a | 4.2 |
| Occlusal Load (Nw) | 188.4 a | 201.0 | 224.6 a | 256.8 | 156.2 a | 133.8 |
| Anterior Region | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 6.3 a | 4.4 | 6.0 a | 4.1 | 6.5 a | 4.7 |
| Average Pressure (MPa) | 11.1 a | 3.0 | 11.5 a | 3.2 | 10.7 a | 2.9 |
| Maximal Pressure (MPa) | 31.9 a | 11.5 | 33.7 a | 13.9 | 30.3 a | 9.0 |
| Occlusal Load (Nw) | 80.2 a | 73.3 | 79.6 a | 89.1 | 80.7 a | 58.5 |
| Right Side | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 4.2 a | 4.3 | 4.3 a | 4.6 | 4.2 a | 4.1 |
| Average Pressure (MPa) | 9.9 a | 4.2 | 10.7 a | 5.6 | 9.2 a | 2.4 |
| Maximal Pressure (MPa) | 25.4 a | 11.5 | 27.1 a | 13.4 | 23.9 a | 9.6 |
| Occlusal Load (Nw) | 50.4 a | 56.2 | 56.8 a | 65.1 | 44.7 a | 48.1 |
| Left Side | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 4.1 a | 4.1 | 4.7 a | 5.0 | 3.6 a | 3.0 |
| Average Pressure (MPa) | 10.0 a | a 3.3 | 9.9 a | 4.2 | 10.0 a | 2.5 |
| Maximal Pressure (MPa) | 25.3 a | 11.0 | 27.4 a | 12.3 | 23.4 a | 9.8 |
| Occlusal Load (Nw) | 45.4 a | 43.3 | 52.4 a | 52.7 | 39.1 | 33.2 |
| Postoperative Records (One Year After Treatment) | ||||||
| Full-Arch | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 31.6 b | 9.7 | 35.2 b | 9.3 | 29.1 b | 9.4 |
| Average Pressure (MPa) * | 15.4 b | 4.2 | 18.3 b | 4.5 | 13.4 b | 2.3 |
| Maximal Pressure (MPa) * | 42.9 b | 10.7 | 47.4 b | 13.9 | 39.8 b | 6.7 |
| Occlusal Load (Nw) * | 483.0 b | 280.1 | 606.5 b | 364.1 | 398.2 b | 171.0 |
| Anterior Region | ||||||
| Contact Area (mm) | 10.2 b | 7.8 | 9.6 b | 7.3 | 10.6 b | 8.4 |
| Average Pressure (MPa) | 13.0 b | 4.6 | 14.2 a | 6.4 | 12.2 a | 2.8 |
| Maximal Pressure (MPa) | 37.9 a | 22.0 | 43.3 a | 31.0 | 34.1 a | 12.6 |
| Occlusal Load (Nw) | 160.0 b | 174.5 | 182.0 b | 245.3 | 144.8 b | 109.8 |
| Right Side | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 13.9 b | 4.3 | 15.3 b | 4.9 | 12.9 b | 3.7 |
| Average Pressure (MPa) | 15.0 b | 4.3 | 15.7 a | 3.6 | 14.4 b | 4.7 |
| Maximal Pressure (MPa) | 36.7 b | 7.8 | 39.6 b | 8.2 | 34.6 b | 7.1 |
| Occlusal Load (Nw) | 207.9 b | 89.6 | 244.1 b | 104.6 | 182.9 b | 70.7 |
| Left Side | Mean | SD | Mean | SD | Mean | SD |
| Contact Area (mm) | 14.4 b | 5.5 | 15.6 b | 6.4 | 13.6 b | 4.9 |
| Average Pressure (MPa) | 15.1 b | 4.1 | 15.8 b | 4.4 | 14.6 b | 3.9 |
| Maximal Pressure (MPa) | 38.6 b | 12.2 | 42.9 b | 16.8 | 35.7 b | 6.9 |
| Occlusal Load (Nw) | 201.4 b | 110.2 | 249.0 b | 144.8 | 194.1 b | 75.9 |
| EMG Maximal Force (μv) | All Patients (n = 34 Patients at Baseline; n = 27 at Follow-Up) | IL Group (n = 16 at Baseline; n = 11 at Follow-Up) | CL Group (n = 18 Patients at Baseline; n = 16 at Follow-Up) | |||
|---|---|---|---|---|---|---|
| Preoperative | Mean | SD | Mean | SD | Mean | SD |
| Masseter Right | 26.6 a | 15.1 | 29.8 a | 18.6 | 23.8 a | 10.9 |
| Masseter Left | 23.5 a | 11.9 | 24.3 a | 13.4 | 22.8 a | 10.7 |
| Temporal Right | 22.9 a | 14.0 | 22.6 a | 14.2 | 23.3 a | 14.3 |
| Temporal Left | 21.7 a | 13.1 | 19.5 a | 10.3 | 23.6 a | 15.2 |
| Postoperative | ||||||
| Masseter Right | 33.4 b | 16.4 | 36.4 a | 19.8 | 31.3 b | 13.9 |
| Masseter Left | 30.6 b | 14.5 | 33.6 b | 16.3 | 28.5 b | 13.3 |
| Temporal Right | 24.9 a | 14.3 | 24.9 a | 16.0 | 24.9 a | 13.6 |
| Temporal Left | 22.7 a | 11.3 | 21.8 a | 7.8 | 23.3 a | 13.4 |
| All Patients | Carrot | Salads | Meat | Vegetables | Apple | Number of Foods Easily Chewed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline a | N | % | N | % | N | % | N | % | N | % | Mean | SD |
| Easy | 0 | 0.0 | 6 | 17.6 | 1 | 2.9 | 28 | 82.4 | 0 | 0.0 | 1.0 a | 0.7 |
| A bit difficult | 4 | 11.8 | 19 | 55.9 | 14 | 41.2 | 6 | 17.6 | 6 | 17.6 | ||
| Very difficult | 30 | 88.2 | 9 | 26.5 | 19 | 55.9 | 0 | 0.0 | 28 | 82.4 | ||
| 12 months after implant hybrid PEEK b | ||||||||||||
| Easy | 23 | 85.2 | 27 | 100.0 | 26 | 96.3 | 27 | 100.0 | 18 | 66.7 | 3.6 b | 1.9 |
| A bit difficult | 4 | 14.8 | 0 | 0.0 | 1 | 3.7 | 0 | 0.0 | 9 | 33.3 | ||
| Very difficult | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| IL Group | ||||||||||||
| Baseline a | N | % | N | % | N | % | N | % | N | % | Mean | SD |
| Easy | 0 | 0.0 | 2 | 12.5 | 1 | 6.3 | 14 | 87.5 | 0 | 0.0 | 1.1 a | 0.7 |
| A bit difficult | 3 | 18.8 | 11 | 68.8 | 6 | 37.5 | 2 | 12.5 | 4 | 25.0 | ||
| Very difficult | 13 | 81.3 | 3 | 18.8 | 9 | 56.3 | 0 | 0.0 | 12 | 75.0 | ||
| 12 months after implant hybrid PEEK b | ||||||||||||
| Easy | 11 | 100.0 | 11 | 100.0 | 10 | 90.9 | 11 | 100.0 | 9 | 81.8 | 3.3 b | 2.3 |
| A bit difficult | 0 | 0.0 | 0 | 0.0 | 1 | 9.1 | 0 | 0.0 | 2 | 18.2 | ||
| Very difficult | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| CL Group | ||||||||||||
| Baseline a | N | % | N | % | N | % | N | % | N | % | Mean | SD |
| Easy | 0 | 0 | 4 | 22.2 | 0 | 0.0 | 14 | 77.8 | 0 | 0.0 | 1.0 a | 0.7 |
| A bit difficult | 1 | 5.6 | 8 | 44.4 | 8 | 44.4 | 4 | 22.2 | 2 | 11.1 | ||
| Very difficult | 17 | 94.4 | 6 | 33.3 | 10 | 55.6 | 0 | 0.0 | 16 | 88.9 | ||
| 12 months after implant hybrid PEEK b | ||||||||||||
| Easy | 12 | 75.0 | 16 | 100.0 | 16 | 100.0 | 16 | 100.0 | 9 | 56.3 | 3.8 b | 1.4 |
| A bit difficult | 4 | 25.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 7 | 43.7 | ||
| Very difficult | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||
| Satisfaction (0–10 Range) | All Patients (n = 34 Patients at Baseline; n = 27 at Follow-Up) | IL Group (n = 16 at Baseline; n = 11 at Follow-Up) | CL Group (n = 18 Patients at Baseline; n = 16 at Follow-Up) | |||
|---|---|---|---|---|---|---|
| Preoperative | Mean | SD | Mean | SD | Mean | SD |
| Global | 4.2 a | 1.5 | 3.9 a | 1.5 | 4.4 a | 1.4 |
| Aesthetic | 4.3 a | 1.7 | 4.2 a | 2.0 | 4.4 a | 1.5 |
| Chewing | 3.4 a | 1.1 | 3.1 a | 1.0 | 3.6 a | 1.2 |
| Postoperative | ||||||
| Global * | 9.1 b | 0.7 | 9.5 b | 0.6 | 8.8 b | 0.7 |
| Aesthetic * | 9.0 b | 1.1 | 9.5 b | 0.7 | 8.7 b | 1.2 |
| Chewing * | 9.1 b | 0.5 | 9.6 b | 0.7 | 9.1 b | 0.5 |
| Oral Health-Related Quality of Life OHIP-20 | All Patients (n = 34 Patients at Baseline; n = 27 at Follow-Up) | IL Group (n = 16 at Baseline; n = 11 at Follow-Up) | CL Group (n = 18 Patients at Baseline; n = 16 at Follow-Up) | |||
|---|---|---|---|---|---|---|
| Preoperative Scores | Mean | SD | Mean | SD | Mean | SD |
| Functional limitation | 2.5 a | 0.7 | 2.5 a | 0.7 | 2.4 a | 0.7 |
| Pain | 3.2 a | 1.0 | 3.1 a | 1.1 | 3.2 a | 0.9 |
| Psychological Discomfort | 1.5 a | 0.8 | 1.6 a | 0.7 | 1.4 a | 0.8 |
| Physical Disability | 2.9 a | 1.4 | 3.0 a | 1.5 | 2.9 a | 1.5 |
| Psychological Disability | 1.3 a | 0.9 | 1.6 a | 0.8 | 1.0 a | 0.9 |
| Social Disability | 0.7 a | 0.9 | 0.8 a | 0.9 | 0.6 a | 0.9 |
| Handicap | 0.1 a | 0.4 | 0.1 a | 0.5 | 0.1 a | 0.2 |
| Total | 12.1 a | 3.7 | 12.6 a | 3.9 | 11.6 a | 3.6 |
| Postoperative Scores | Mean | SD | Mean | SD | Mean | SD |
| Functional limitation | 0.4 b | 0.7 | 0.4 b | 0.7 | 0.5 b | 0.7 |
| Pain | 0.0 b | 0.2 | 0.0 b | 0.0 | 0.1 b | 0.2 |
| Psychological Discomfort | 0.0 b | 0.2 | 0.0 b | 0.0 | 0.1 b | 0.3 |
| Physical Disability | 0.0 b | 0.0 | 0.0 b | 0.0 | 0.0 b | 0.0 |
| Psychological Disability | 0.1 b | 0.3 | 0.1 b | 0.3 | 0.1 b | 0.3 |
| Social Disability | 0.0 b | 0.0 | 0.0 b | 0.0 | 0.0 b | 0.0 |
| Handicap | 0.1 b | 0.3 | 0.0 b | 0.0 | 0.0 b | 0.2 |
| Total | 0.6 b | 1.0 | 0.6 b | 0.9 | 0.7 b | 1.1 |
| Effect Sizes | Mean | SD | Mean | SD | Mean | SD |
| Functional limitation | 3.1 | 1.2 | 3.5 | 1.0 | 2.8 | 1.3 |
| Pain | 3.3 | 1.1 | 3.2 | 1.1 | 3.3 | 1.0 |
| Psychological Discomfort | 1.9 | 1.0 | 2.2 | 0.9 | 1.8 | 1.1 |
| Physical Disability | 2.1 | 1.0 | 2.2 | 1.0 | 2.0 | 1.1 |
| Psychological Disability | 1.2 | 1.0 | 1.6 | 0.9 | 0.9 | 1.0 |
| Social Disability | 0.6 | 1.0 | 0.7 | 1.0 | 0.5 | 1.0 |
| Handicap | 0.2 | 1.3 | 0.2 | 1.8 | 0.2 | 0.7 |
| Total | 3.1 | 1.0 | 3.4 | 1.0 | 2.9 | 1.0 |
| Effect of Prosthetic Treatment | Much Worse | Worse | Equal | Better | Much Better |
|---|---|---|---|---|---|
| All Patients (n = 27 at follow-up) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Pronouncing words * | 0 (0.0) | 0 (0.0) | 18 (66.7) | 3 (11.1) | 6 (22.2) |
| Taste and smell | 0 (0.0) | 0 (0.0) | 12 (44.4) | 11 (40.7) | 4 (14.8) |
| Painful aching in the mouth | 0 (0.0) | 0 (0.0) | 1 (3.7) | 16 (59.3) | 10 (37.0) |
| Oral hygiene | 0 (0.0) | 3 (11.1) | 5 (18.5) | 14 (59.1) | 5 (18.5) |
| Chewing Ability | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (7.4) | 25 (92.6) |
| Feeding satisfaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (11.1) | 24 (88.9) |
| Mouth comfortability | 0 (0.0) | 1 (3.7) | 0 (0.0) | 7 (25.9) | 19 (70.4) |
| Appealing Smile | 0 (0.0) | 0 (0.0) | 0 (0.0) | 9 (33.3) | 18 (66.7) |
| Social relations | 0 (0.0) | 0 (0.0) | 8 (29.6) | 16 (59.3) | 3 (11.1) |
| IL Group (n = 11 at follow-up) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Pronouncing words | 0 (0.0) | 0 (0.0) | 5 (45.5) | 1 (9.1) | 5 (45.5) |
| Taste and smell | 0 (0.0) | 0 (0.0) | 4 (36.4) | 4 (36.4) | 3 (27.3) |
| Painful aching in the mouth | 0 (0.0) | 0 (0.0) | 0 (0.0) | 4 (36.4) | 7 (63.6) |
| Oral hygiene | 0 (0.0) | 0 (0.0) | 2 (18.2) | 7 (63.6) | 2 (18.2) |
| Chewing Ability | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 11 (100) |
| Feeding satisfaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (9.1) | 10 (90.9) |
| Mouth comfortability | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (18.2) | 9 (81.8) |
| Appealing Smile | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (18.2) | 9 (81.8) |
| Social relations | 0 (0.0) | 0 (0.0) | 2 (18.2) | 8 (72.7) | 1 (9.1) |
| CL Group (n = 16 at follow-up) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Pronouncing words | 0 (0.0) | 0 (0.0) | 13 (81.3) | 2 (12.5) | 1 (6.3) |
| Taste and smell | 0 (0.0) | 0 (0.0) | 8 (50.0) | 7 (43.8) | 1 (6.3) |
| Painful aching in the mouth | 0 (0.0) | 0 (0.0) | 1 (6.3) | 12 (75.0) | 3 (18.8) |
| Oral hygiene | 0 (0.0) | 3 (18.8) | 3 (18.8) | 7 (43.8) | 3 (18.8) |
| Chewing Ability | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (12.5) | 14 (87.5) |
| Feeding satisfaction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (12.5) | 14 (87.5) |
| Mouth comfortability | 0 (0.0) | 1 (6.3) | 0 (0.0) | 5 (31.3) | 10 (62.5) |
| Appealing Smile | 0 (0.0) | 0 (0.0) | 0 (0.0) | 7 (43.8) | 9 (56.3) |
| Social relations | 0 (0.0) | 0 (0.0) | 6 (37.5) | 8 (50.0) | 2 (12.5) |
| Masticatory Performance by Mixing Ability Tests (https://studio.chewing.app/) | All Patients (n = 34 Patients at Baseline; n = 27 at Follow-Up) | IL Group (n = 16 at Baseline; n = 11 at Follow-Up) | CL Group (n = 18 Patients at Baseline; n = 16 at Follow-Up) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Preoperative Scores | 19.7 a | 9.0 | 21.0 a | 10.6 | 18.6 a | 7.6 |
| Postoperative Scores | 67.8 b | 6.5 | 68.2 b | 4.6 | 67.5 b | 7.7 |
| Dependent Predictors | Β | Error | T | p-Value | Lower CI 95% | Upper CI 95% |
|---|---|---|---|---|---|---|
| Masticatory Performance a | ||||||
| Postoperative easily chewed foods | 3.9 | 0.03 | 2.3 | 0.03 | 0.34 | 7.52 |
| Foods Chewed Easily b | ||||||
| Postoperative masticatory performance | 0.05 | 0.02 | 2.8 | 0.01 | 0.01 | 0.09 |
| Global Satisfaction c | ||||||
| Loading Cohort | 0.67 | 0.26 | 2.6 | 0.02 | 0.2 | 1.2 |
| Final Impact on Quality of Life d | ||||||
| Foods easily chewed after treatment | −0.63 | 0.28 | −2.3 | 0.03 | −0.06 | −1.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montero, J.; Guadilla, Y.; Flores, J.; Pardal-Peláez, B.; Quispe-López, N.; Gómez-Polo, C.; Dib, A. Patient-Centered Treatment Outcomes with Full-Arch PEEK Rehabilitation Supported on Four Immediate or Conventionally Loaded Implants. A Randomized Clinical Trial. J. Clin. Med. 2021, 10, 4589. https://doi.org/10.3390/jcm10194589
Montero J, Guadilla Y, Flores J, Pardal-Peláez B, Quispe-López N, Gómez-Polo C, Dib A. Patient-Centered Treatment Outcomes with Full-Arch PEEK Rehabilitation Supported on Four Immediate or Conventionally Loaded Implants. A Randomized Clinical Trial. Journal of Clinical Medicine. 2021; 10(19):4589. https://doi.org/10.3390/jcm10194589
Chicago/Turabian StyleMontero, Javier, Yasmina Guadilla, Javier Flores, Beatriz Pardal-Peláez, Norberto Quispe-López, Cristina Gómez-Polo, and Abraham Dib. 2021. "Patient-Centered Treatment Outcomes with Full-Arch PEEK Rehabilitation Supported on Four Immediate or Conventionally Loaded Implants. A Randomized Clinical Trial" Journal of Clinical Medicine 10, no. 19: 4589. https://doi.org/10.3390/jcm10194589
APA StyleMontero, J., Guadilla, Y., Flores, J., Pardal-Peláez, B., Quispe-López, N., Gómez-Polo, C., & Dib, A. (2021). Patient-Centered Treatment Outcomes with Full-Arch PEEK Rehabilitation Supported on Four Immediate or Conventionally Loaded Implants. A Randomized Clinical Trial. Journal of Clinical Medicine, 10(19), 4589. https://doi.org/10.3390/jcm10194589