
Clinical Outcomes between Stand-Alone Zero-Profile Spacers and Cervical Plate with Cage Fixation for Anterior Cervical Discectomy and Fusion: A Retrospective Analysis of 166 Patients


 , ,
, , 
Abstract
:1. Introduction
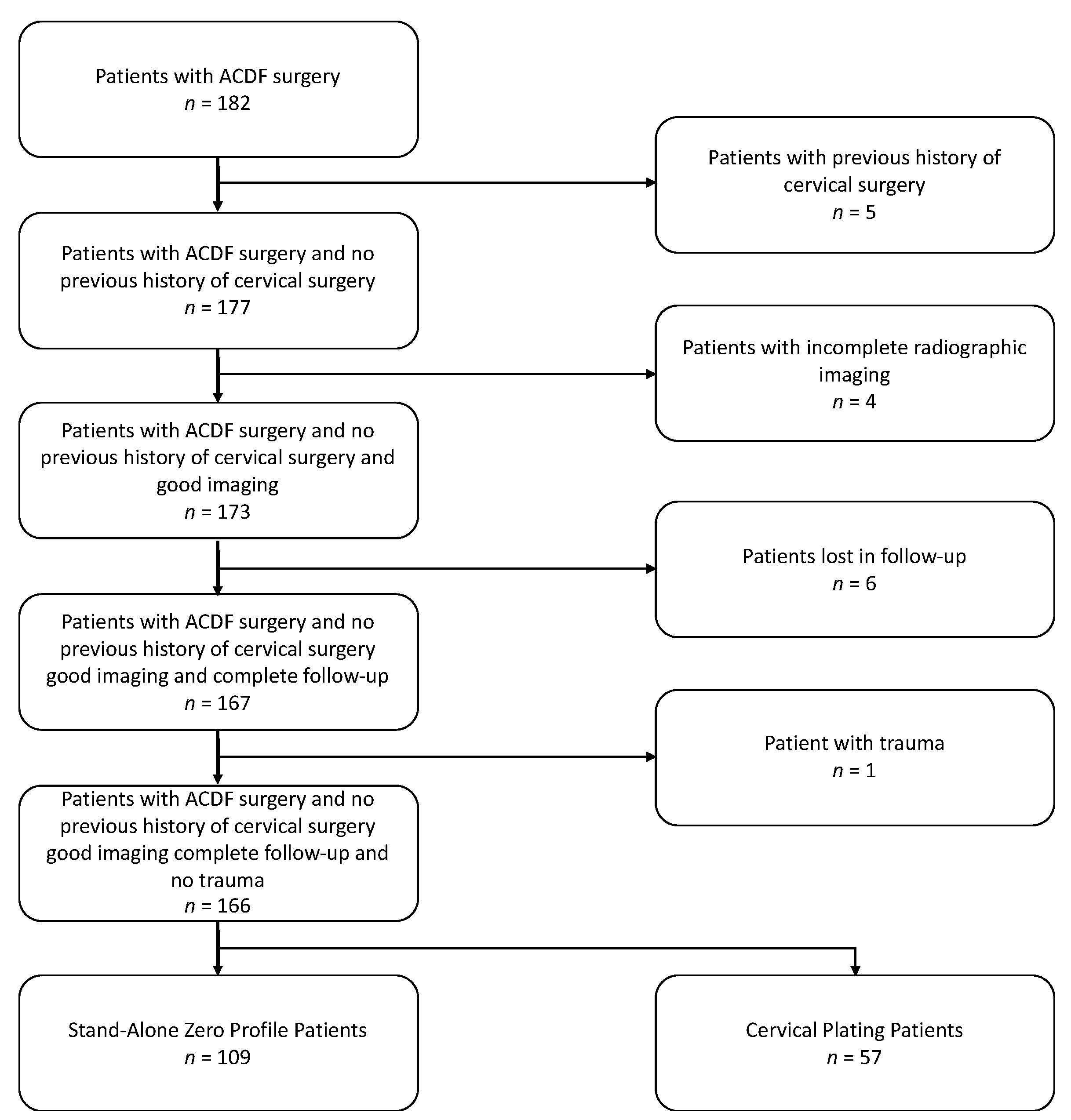
2. Materials and Methods
2.1. Surgical Procedure
2.2. Clinical Measures
2.3. Statistical Analysis
3. Results
3.1. Demographics
3.2. Clinical Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M. Degenerative Cervical Myelopathy. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Martin, A.R.; Nater, A.; Witiw, C.D.; Kato, S.; Tetreault, L.; Reihani-Kermani, H.; Santaguida, C.; Fehlings, M.G. Influence of Magnetic Resonance Imaging Features on Surgical Decision-Making in Degenerative Cervical Myelopathy: Results from a Global Survey of AOSpine International Members. World Neurosurg. 2017, 105, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Angevine, P.D.; Arons, R.R.; McCormick, P.C. National and Regional Rates and Variation of Cervical Discectomy with and Without Anterior Fusion, 1990–1999. Spine 2003, 28, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Korinth, M.C. Treatment of Cervical Degenerative Disc Disease–Current Status and Trends. Cent. Eur. Neurosurg. Zent. Neurochir. 2008, 69, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Z.B.; Gidumal, S.; White, S.; Shin, J.; Phan, K.; Osman, N.; Bronheim, R.; Vargas, L.; Kim, J.; Cho, S.K. Comparison of Anterior Cervical Discectomy and Fusion with a Stand-Alone Interbody Cage Versus a Conventional Cage-Plate Technique: A Systematic Review and Meta-Analysis. Glob. Spine J. 2018, 9, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, G.M.V.; Romano, D.; Certo, F.; Milone, P.; Albanese, V. Zero-P: A new zero-profile cage-plate device for single and multilevel ACDF. A single Institution series with four years maximum follow-up and review of the literature on zero-profile devices. Eur. Spine J. 2013, 22, 868–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matz, P.G.; Pritchard, P.R.; Hadley, M.N. Anterior cervical approach for the treatment of cervical myelopathy. Neurosurgery 2007, 60, S1–S64. [Google Scholar] [CrossRef] [PubMed]
- Bible, J.E.; Kang, J.D. Anterior cervical discectomy and fusion: Surgical indications and outcomes. Semin. Spine Surg. 2016, 28, 80–83. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, H.; Wu, X.; Wang, X.; Lin, W.; Yuan, W. Comparative analysis of clinical outcomes between zero-profile implant and cages with plate fixation in treating multilevel cervical spondilotic myelopathy: A three-year follow-up. Clin. Neurol. Neurosurg. 2016, 144, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Song, K.-J.; Taghavi, C.E.; Lee, K.-B.; Song, J.-H.; Eun, J.-P. The Efficacy of Plate Construct Augmentation Versus Cage Alone in Anterior Cervical Fusion. Spine 2009, 34, 2886–2892. [Google Scholar] [CrossRef] [PubMed]
- Yun, D.-J.; Lee, S.-J.; Park, S.-J.; Oh, H.S.; Lee, Y.J.; Oh, H.M. Use of a Zero-Profile Device for Contiguous 2-Level Anterior Cervical Diskectomy and Fusion: Comparison with Cage with Plate Construct. World Neurosurg. 2017, 97, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Liu, Z.-D.; Li, X.-F.; Qian, L.; Zhong, G.-B.; Chen, F.-J. Comparison of plate-cage construct and stand-alone anchored spacer in the surgical treatment of three-level cervical spondylotic myelopathy: A preliminary clinical study. Spine J. 2015, 15, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Vaněk, P.; Bradáč, O.; DeLacy, P.; Lacman, J.; Beneš, V. Anterior Interbody Fusion of the Cervical Spine with Zero-P Spacer. Spine 2013, 38, E792–E797. [Google Scholar] [CrossRef] [PubMed]
- Bazaz, R.; Lee, M.J.; Yoo, J.U. Incidence of Dysphagia after Anterior Cervical Spine Surgery. Spine 2002, 27, 2453–2458. [Google Scholar] [CrossRef] [PubMed]
- Fountas, K.N.; Kapsalaki, E.Z.; Nikolakakos, L.G.; Smisson, H.F.; Johnston, K.W.; Grigorian, A.A.; Lee, G.P.; Robinson, J.S. Anterior Cervical Discectomy and Fusion Associated Complications. Spine 2007, 32, 2310–2317. [Google Scholar] [CrossRef] [PubMed]
- Gabr, M.A.; Touko, E.; Yadav, A.P.; Karikari, I.; Goodwin, C.R.; Groff, M.W.; Ramirez, L.; Abd-El-Barr, M.M. Improved Dysphagia Outcomes in Anchored Spacers Versus Plate-Screw Systems in Anterior Cervical Discectomy and Fusion: A Systematic Review. Glob. Spine J. 2020, 10, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Boer, L.F.R.; Zorzetto, E.; Yeh, F.; Wajchenberg, M.; Martins, D.E. Degenerative Cervical Disorder—Stand-alone Cage Versus Cage and Cervical Plate: A Systematic Review. Glob. Spine J. 2021, 11, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fogel, G.R.; McDonnell, M.F. Surgical treatment of dysphagia after anterior cervical interbody fusion. Spine J. 2005, 5, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-H.; Hyun, S.-J.; Kim, M.J.; Yeom, J.S.; Kim, W.H.; Kim, K.-J.; Jahng, T.-A.; Kim, H.-J.; Yoon, S.H. Comparative Analysis of 3 Different Construct Systems for Single-level Anterior Cervical Discectomy and Fusion. J. Spinal Disord. Tech. 2013, 26, 112–118. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Covariate | All Patients n = 166 | Stand Alone n = 109 | Cervical Plate n = 57 | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age, n (SD) | 53 (13) | 52 (14) | 54 (13) | 0.50 |
| Female, n (%) | 92 (55) | 66 (61) | 26 (46) | 0.07 |
| Medical Comorbidities | ||||
| BMI, mean (SD) | 29 (9) | 28 (6) | 30 (6) | 0.05 |
| Diabetes Mellitus, n (%) | 24 (14) | 15 (14) | 9 (16) | 0.73 |
| Current Smoker, n (%) | 45 (27) | 30 (28) | 15 (26) | 0.87 |
| Former Smoker, n (%) | 47 (28) | 24 (22) | 23 (40) | 0.03 |
| Osteoporosis, n (%) | 3 (2) | 3 (3) | 0 | 0.08 |
| Treatments, n (%) | ||||
| Number of Medication, mean (SD) | 6 (4) | 6 (4) | 6 (4) | 0.72 |
| 1 opioid | 50 (30) | 32 (29) | 18 (32) | 0.77 |
| 2+ opioids | 11 (7) | 8 (7) | 3 (5) | 0.60 |
| 1 depression medication | 44 (27) | 33 (30) | 11 (19) | 0.11 |
| 2+ depression medications | 10 (6) | 7 (6) | 3 (5) | 0.76 |
| Pregabalin or Gabapentin | 40 (24) | 30 (28) | 10 (18) | 0.17 |
| Chronic NSAID | 58 (35) | 40 (37) | 18 (32) | 0.44 |
| Chronic Steroid | 13 (8) | 10 (9) | 3 (5) | 0.60 |
| Physical Therapy | 98 (59) | 67 (61) | 31 (54) | 0.52 |
| Epidural Steroid Injection | 22 (13) | 17 (16) | 5 (9) | 0.25 |
| Clinical presentation, n (%) | ||||
| Radiculopathy | 92 (55) | 66 (61) | 26 (46) | 0.07 |
| Myelopathy | 37 (22) | 15 (14) | 22 (39) | 0.001 |
| Myeloradiculopathy | 37 (22) | 28 (26) | 9 (16) | 0.13 |
| Covariate | All Patients | Stand Alone | Cervical Plate | p-Value |
|---|---|---|---|---|
| Number of Levels of Surgery | ||||
| 1 | 85 (51) | 59 (54) | 26 (46) | 0.30 |
| 2 | 65 (39) | 37 (34) | 28 (49) | 0.63 |
| 3 | 16 (10) | 13 (12) | 3 (5) | 0.13 |
| Levels of Surgery, n | ||||
| C2-C3 | 25 | 13 | 12 | 0.15 |
| C3-C4 | 66 | 42 | 24 | 0.66 |
| C4-C5 | 133 | 88 | 45 | 0.79 |
| C5-C6 | 133 | 89 | 44 | 0.51 |
| C6-C7 | 68 | 48 | 20 | 0.26 |
| C7-T1 | 52 | 35 | 17 | 0.76 |
| Total number of levels | 477 | 315 | 162 | |
| Length of Surgery, mean (SD) | 150 min (64) | 126 min (46) | 194 min (69) | <0.001 |
| Blood Loss, n (%) | ||||
| 0–50 mL | 132 (80) | 85 (78) | 47 (82) | 0.49 |
| 51–100 mL | 30 (18) | 24 (22) | 6 (10) | 0.05 |
| >100 mL | 4 (2) | 0 | 4 (7) | 0.05 |
| CSF leak, n (%) | 1 (1) | 0 | 1 (2) | 0.32 |
| Length of stay, mean (SD) | 1.7 (1) | 1.5 (1) | 2.1 (2) | 0.006 |
| Dysphagia at 3 months, n (%) | ||||
| None | 79 (96) | 52 (98) | 27 (93) | 0.34 |
| Mild | 3 (4) | 1 (2) | 2 (7) | 0.34 |
| Moderate | 0 | 0 | 0 | N/A |
| Steroid use, n (%) | 10 (6) | 9 (8) | 1 (2) | 0.07 |
| Patient Group | All Patients (n = 74) | Stand Alone (n = 43) | Cervical Plate (n = 31) | |||
|---|---|---|---|---|---|---|
| Nurick Score | Baseline | Last Follow-Up | Baseline | Last Follow-Up | Baseline | Last Follow-Up |
| 0 | 0 | 55 (74) | 0 | 36 (84) | 0 | 19 (61) |
| 1 | 21 (28) | 12 (16) | 11 (26) | 3 (7) | 10 (32) | 9 (29) |
| 2 | 41 (55) | 5 (7) | 25 (58) | 4 (9) | 16 (52) | 1 (3) |
| 3 | 8 (11) | 1 (1) | 6 (14) | 0 | 2 (7) | 1 (3) |
| 4 | 3 (4) | 0 | 1 (2) | 0 | 2 (7) | 0 |
| 5 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6 | 1 (1) | 1 (1) | 0 | 0 | 1 (3) | 1 (3) |
| Covariates | OR (95% CI) | p-Value |
|---|---|---|
| Patient Characteristics | ||
| Age | 0.99 (0.97–1.04) | 0.79 |
| Sex (Female) | 1.21 (0.27–2.30) | 0.71 |
| Diabetes | 0.44 (0.12–1.23) | 0.14 |
| Surgery Characteristics | ||
| Stand-Alone Zero Profile | 0.67 (0.14–1.61) | 0.49 |
| Length of Stay | 0.5 (0.35–0.85) | 0.003 |
| Number of levels of Surgery | ||
| 1 level | 1 | NA |
| 2 levels | 1.99 (0.15–1.70) | 0.22 |
| 3 levels | 3.56 (0.77–21) | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sommaruga, S.; Camara-Quintana, J.; Patel, K.; Nouri, A.; Tessitore, E.; Molliqaj, G.; Panchagnula, S.; Robinson, M.; Virojanapa, J.; Sun, X.; et al. Clinical Outcomes between Stand-Alone Zero-Profile Spacers and Cervical Plate with Cage Fixation for Anterior Cervical Discectomy and Fusion: A Retrospective Analysis of 166 Patients. J. Clin. Med. 2021, 10, 3076. https://doi.org/10.3390/jcm10143076
Sommaruga S, Camara-Quintana J, Patel K, Nouri A, Tessitore E, Molliqaj G, Panchagnula S, Robinson M, Virojanapa J, Sun X, et al. Clinical Outcomes between Stand-Alone Zero-Profile Spacers and Cervical Plate with Cage Fixation for Anterior Cervical Discectomy and Fusion: A Retrospective Analysis of 166 Patients. Journal of Clinical Medicine. 2021; 10(14):3076. https://doi.org/10.3390/jcm10143076
Chicago/Turabian StyleSommaruga, Samuel, Joaquin Camara-Quintana, Kishan Patel, Aria Nouri, Enrico Tessitore, Granit Molliqaj, Shreyas Panchagnula, Michael Robinson, Justin Virojanapa, Xin Sun, and et al. 2021. "Clinical Outcomes between Stand-Alone Zero-Profile Spacers and Cervical Plate with Cage Fixation for Anterior Cervical Discectomy and Fusion: A Retrospective Analysis of 166 Patients" Journal of Clinical Medicine 10, no. 14: 3076. https://doi.org/10.3390/jcm10143076
APA StyleSommaruga, S., Camara-Quintana, J., Patel, K., Nouri, A., Tessitore, E., Molliqaj, G., Panchagnula, S., Robinson, M., Virojanapa, J., Sun, X., Melnikov, F., Kolb, L., Schaller, K., Abbed, K., & Cheng, J. (2021). Clinical Outcomes between Stand-Alone Zero-Profile Spacers and Cervical Plate with Cage Fixation for Anterior Cervical Discectomy and Fusion: A Retrospective Analysis of 166 Patients. Journal of Clinical Medicine, 10(14), 3076. https://doi.org/10.3390/jcm10143076