
Anti-S and Anti-N Antibody Responses of COVID-19 Vaccine Recipients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants, Setting, and Ethical Consideration
2.2. Demographic and Clinical Characteristics of Population Study
2.3. Sample Collection
2.4. Sample Analysis
2.5. Statistical Analysis
3. Results
3.1. Participants (Demographics)
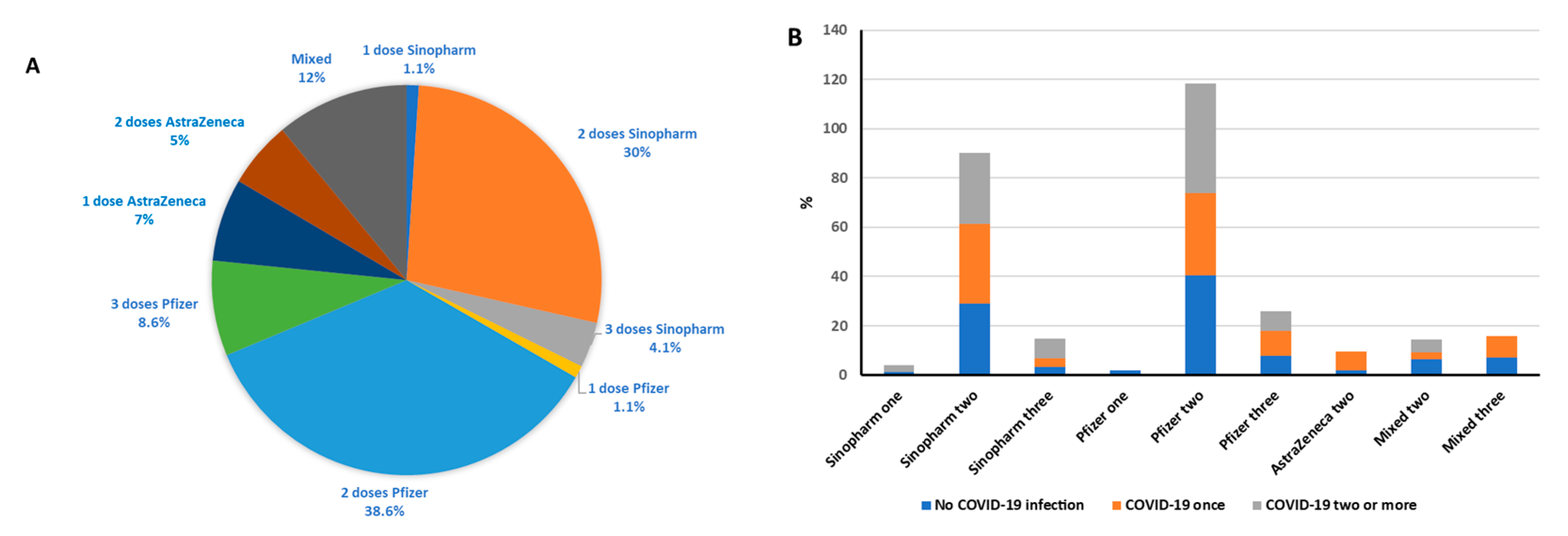
3.2. Participants’ Vaccination and COVID Infection History
3.3. Participants’ COVID-19 Immunoglobulin Responses to Vaccine
3.4. COVID-19 Vaccine Effects on Antibodies
3.5. COVID-19 Infection Effect on Anti-S IgG and Anti-N IgG Levels
3.6. Effect of Hybrid Immunity on Anti-S IgG and Anti-N IgG Levels
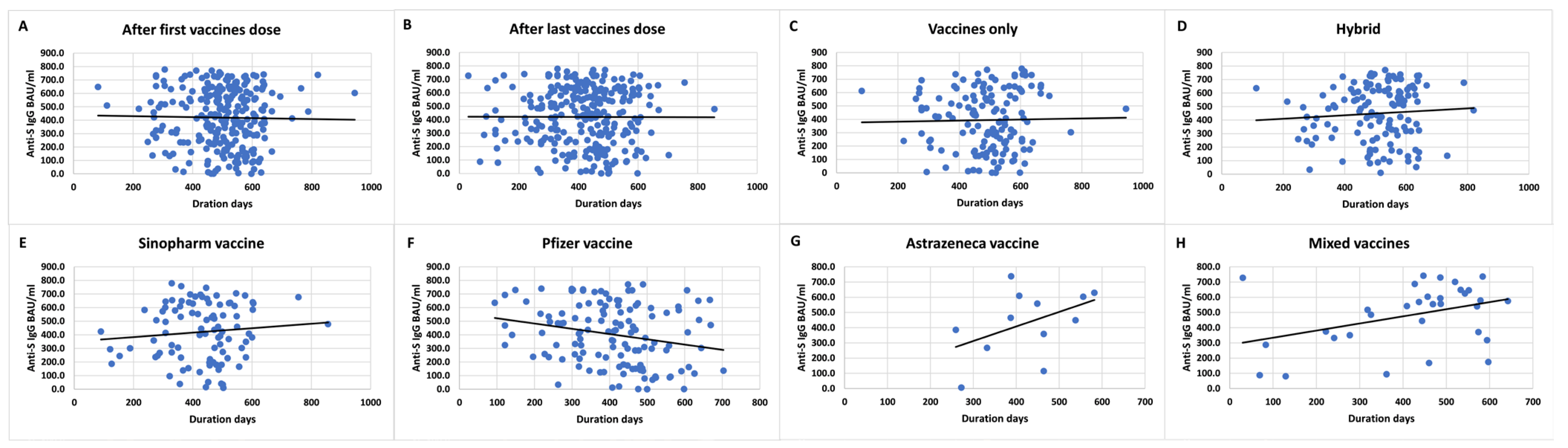
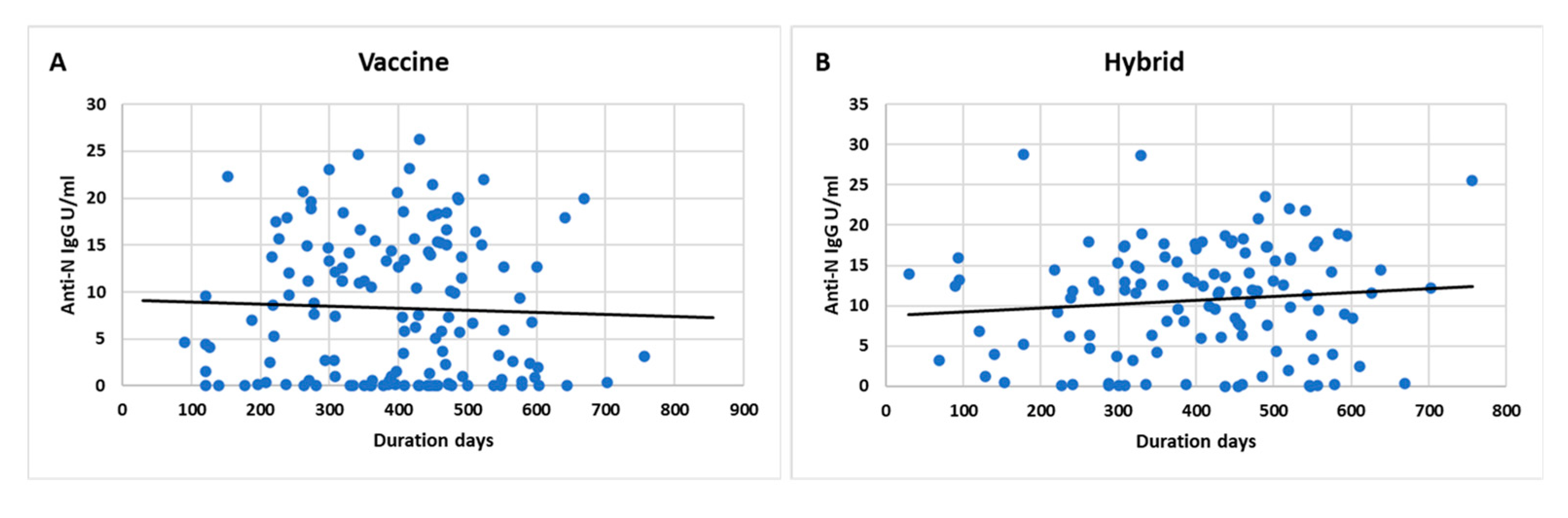
3.7. Effect of Time on Anti-S IgG and Anti-N IgG Levels
3.8. Effect of Age, Gender, BMI, Smoking, and Chronic Diseases on Anti-S IgG and Anti-N IgG Positivity and Titer Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef]
- WHO. Archived: WHO Timeline-COVID-19. Available online: https://www.who.int/news-room/detail/27-04-2020-who-timeline---covid-19 (accessed on 10 March 2023).
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]
- Yu, J.; Chai, P.; Ge, S.; Fan, X. Recent Understandings Toward Coronavirus Disease 2019 (COVID-19): From Bench to Bedside. Front. Cell Dev. Biol. 2020, 8, 476. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Mukherjee, S. Morbidity and mortality from COVID-19 post-vaccination breakthrough infections in association with vaccines and the emergence of variants in Bahrain. Biol. Sci. 2021. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef]
- Jordan-COVID-19 Overview-Johns Hopkins. Available online: https://coronavirus.jhu.edu/region/jordan (accessed on 20 April 2023).
- CDC. COVID Data Tracker: Vaccinations in the US. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-people-booster-percent-pop5 (accessed on 20 April 2023).
- Lippi, G.; Henry, B.M.; Plebani, M. Anti-SARS-CoV-2 Antibodies Testing in Recipients of COVID-19 Vaccination: Why, When, and How? Diagnostics 2021, 11, 941. [Google Scholar] [CrossRef]
- Rezaei, M.; Sadeghi, M.; Korourian, A.; Tabarsi, P.; Porabdollah, M.; Askari, E.; Mortaz, E.; Mahmoudi, S.; Marjani, M.; Velayati, A.A. Comparative evaluation of SARS-CoV-2 IgG assays against nucleocapsid and spike antigens. Hum. Antibodies 2021, 29, 109–113. [Google Scholar] [CrossRef]
- Azak, E.; Karadenizli, A.; Uzuner, H.; Karakaya, N.; Canturk, N.Z.; Hulagu, S. Comparison of an inactivated Covid19 vaccine-induced antibody response with concurrent natural Covid19 infection. Int. J. Infect. Dis. 2021, 113, 58–64. [Google Scholar] [CrossRef]
- Lee, N.; Jeong, S.; Lee, S.K.; Cho, E.-J.; Hyun, J.; Park, M.-J.; Song, W.; Kim, H.S. Quantitative Analysis of Anti-N and Anti-S Antibody Titers of SARS-CoV-2 Infection after the Third Dose of COVID-19 Vaccination. Vaccines 2022, 10, 1143. [Google Scholar] [CrossRef]
- Van Elslande, J.; Decru, B.; Jonckheere, S.; Van Wijngaerden, E.; Houben, E.; Vandecandelaere, P.; Indevuyst, C.; Depypere, M.; Desmet, S.; André, E.; et al. Antibody response against SARS-CoV-2 spike protein and nucleoprotein evaluated by four automated immunoassays and three ELISAs. Clin. Microbiol. Infect. 2020, 26, 1557.e1–1557.e7. [Google Scholar] [CrossRef]
- McBride, R.; Van Zyl, M.; Fielding, B.C. The Coronavirus Nucleocapsid Is a Multifunctional Protein. Viruses 2014, 6, 2991–3018. [Google Scholar] [CrossRef]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; Huang, H.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef]
- Vályi-Nagy, I.; Matula, Z.; Gönczi, M.; Tasnády, S.; Bekő, G.; Réti, M.; Ajzner, É.; Uher, F. Comparison of antibody and T cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. Geroscience 2021, 43, 2321–2331. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Omran, E.A.; Habashy, R.E.; Elarab, L.A.E.; Hashish, M.H.; El-Barrawy, M.A.; Abdelwahab, I.A.; Fekry, M.M. Anti-Spike and Neutralizing Antibodies after Two Doses of COVID-19 Sinopharm/BIBP Vaccine. Vaccines 2022, 10, 1340. [Google Scholar] [CrossRef]
- Aldridge, R.W.; Yavlinsky, A.; Nguyen, V.; Eyre, M.T.; Shrotri, M.; Navaratnam, A.M.D.; Beale, S.; Braithwaite, I.; Byrne, T.; Kovar, J.; et al. SARS-CoV-2 antibodies and breakthrough infections in the Virus Watch cohort. Nat. Commun. 2022, 13, 4869. [Google Scholar] [CrossRef]
- Matsuba, I.; Takuma, T.; Hatori, N.; Takai, M.; Watanabe, Y.; Takada, N.; Kishi, S.; Matsuzawa, Y.; Nishikawa, T.; Kunishima, T.; et al. The Proportion of Long-term Response to Anti-N Igg Antibody after 12 Months for COVID-19 Subclinical Infections and a Longitudinal Survey for COVID-19 Subclinical Infections in 2021. Intern. Med. 2022, 61, 3053–3062. [Google Scholar] [CrossRef]
- Chantasrisawad, N.; Puthanakit, T.; Tangsathapornpong, A.; Techasaensiri, C.; Phongsamart, W.; Suwanpakdee, D.; Jaruampornpan, P.; Sophonphan, J.; Suntarattiwong, P.; Chotpitayasunondh, T. Immunogenicity and Reactogenicity of mRNA BNT162b2 COVID-19 Vaccine among Thai Adolescents with Chronic Diseases. Vaccines 2022, 10, 871. [Google Scholar] [CrossRef]
- Bansal, D.; Atia, H.; Al Badr, M.; Nour, M.; Abdulmajeed, J.; Hasan, A.; Al-Hajri, N.; Ahmed, L.; Ibrahim, R.; Zamel, R.; et al. Dynamics of Anti-S IgG Antibodies Titers after the Second Dose of COVID-19 Vaccines in the Manual and Craft Worker Population of Qatar. Vaccines 2023, 11, 496. [Google Scholar] [CrossRef]
- Al-Rifai, R.H.; Alhosani, F.; Abuyadek, R.; Atef, S.; Donnelly, J.G.; Leinberger-Jabari, A.; Ahmed, L.A.; Altrabulsi, B.; Alatoom, A.; Alsuwaidi, A.R.; et al. Evaluation of post-vaccination immunoglobulin G antibodies and T-cell immune response after inoculation with different types and doses of SARS-CoV-2 vaccines: A retrospective cohort study. Front. Med. 2023, 9, 1092646. [Google Scholar] [CrossRef]
- Pourakbari, B.; Mirbeyk, M.; Mahmoudi, S.; Sadeghi, R.H.H.; Rezaei, N.; Ghasemi, R.; Esfandiari, F.; Mamishi, S. Evaluation of response to different COVID-19 vaccines in vaccinated healthcare workers in a single center in Iran. J. Med. Virol. 2022, 94, 5669–5677. [Google Scholar] [CrossRef]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.-E.; Alsmadi, H.; et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines 2021, 9, 1223. [Google Scholar] [CrossRef]
- Qaqish, A.; Abbas, M.M.; Al-Tamimi, M.; Abbas, M.A.; Al-Omari, M.; Alqassieh, R. SARS-CoV-2 Antinucleocapsid Antibody Response of mRNA and Inactivated Virus Vaccines Compared to Unvaccinated Individuals. Vaccines 2022, 10, 643. [Google Scholar] [CrossRef]
- Assaid, N.; Arich, S.; Charoute, H.; Akarid, K.; Ezzikouri, S.; Maaroufi, A.; Sarih, M. Anti-SARS-CoV-2 Antibody Responses 5 Months Post Complete Vaccination of Moroccan Healthcare Workers. Vaccines 2022, 10, 465. [Google Scholar] [CrossRef]
- Buhre, J.S.; Pongracz, T.; Künsting, I.; Lixenfeld, A.S.; Wang, W.; Nouta, J.; Lehrian, S.; Schmelter, F.; Lunding, H.B.; Dühring, L.; et al. mRNA vaccines against SARS-CoV-2 induce comparably low long-term IgG Fc galactosylation and sialylation levels but increasing long-term IgG4 responses compared to an adenovirus-based vaccine. Front. Immunol. 2023, 13, 1020844. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Number (%) | |||
|---|---|---|---|---|
| Age (years) | 0–20 21–40 41–60 Above 60 | 11 (4.1) 97 (36.3) 107 (40.1) 52 (19.5) | ||
| Gender | Male Female | 120 (44.9) 147 (55.1) | ||
| BMI | Underweight < 18.5 Normal 18.5–24.9 Overweight 25–29.9 Obese ≥ 30 | 9 (3.4) 81 (30.3) 102 (38.2) 75 (28.1) | ||
| Smoking | Yes No | 94 (35.2) 173 (64.8) | ||
| Chronic diseases | Yes Hypertension Diabetes mellitus Cardiac diseases Hyperlipidemia Thyroid diseases Asthma Others (cancer, kidney diseases, digestive diseases, lung diseases) | 156 (58.4) 72 (27.0) 65 (24.3) 39 (14.6) 34 (12.7) 35 (13.1) 13 (4.9) 46 (17.2) | ||
| COVID-19 Infection | Yes Confirmed by RT-PCR One Two Three Four After vaccine Before vaccine | 125 (46.8) 105 (39.3) 87 (32.6) 29 (10.9) 6 (2.2) 3 (1.1) 87 (32.6) 38 (14.2) | ||
| COVID-19 Vaccination | Yes One dose Two doses Three doses Four doses | 267 (100) 7 (2.6) 206 (77.2) 53 (19.9) 1 (0.4) | ||
| Type of vaccine | Sinopharm Pfizer AstraZeneca Sputnik No | First dose 112 (41.9) 133 (49.8) 20 (7.5) 2 (0.7) 0 (0.0) | Second dose 108 (40.4) 135 (50.6) 16 (6.0) 1 (0.4) 7 (2.6) | Third dose 11 (4.1) 43 (16.1) 0 (0.0) 0 (0.0) 213 (79.8) |
| Duration (days) 0–100 101–200 201–300 301–400 401–500 Above 500 Not available | First dose 1 (0.4) 1 (0.4) 19 (7.1) 30 (11.2) 74 (27.7) 142 (53.2) - | Second dose 4 (1.5) 8 (3.0) 17 (6.4) 35 (13.1) 108 (40.4) 86 (32.2) 9 (3.4) | Third dose 2 (0.7) 2 (0.7) 17 (6.4) 18 (6.7) 2 (0.7) 2 (0.7) 224 (83.9) | Last dose 6 (2.2) 12 (4.5) 36 (13.5) 58 (21.7) 90 (33.7) 65 (24.3) - |
| COVID-19 infection | ||||
| COVID-19 vaccine type and doses | Sinopharm one Sinopharm two Sinopharm three Pfizer one Pfizer two Pfizer three AstraZeneca two Mixed two Mixed three | No infection 2 (1.4) 41 (29.1) 5 (3.5) 3 (2.1) 57 (40.4) 11 (7.8) 3 (2.1) 9 (6.4) 10 (7.1) | Once 0 (0.0) 28 (32.2) 3 (3.4) 0 (0.0) 29 (33.3) 9 (10.3) 8 (7.6) 3 (2.9) 9 (8.6) | Two or more 1 (2.6) 11 (28.9) 3 (7.9) 0 (0.0) 17 (44.7) 3 (7.9) 0 (0.0) 1 (5.0) 0 (0.0) |
| Antibody | Variable | Category | Number (%) or Mean ± SD |
|---|---|---|---|
| Anti-S IgG antibodies | Number (%) | Positive Negative Not available | 257 (96.3) 7 (2.6) 3 (1.1) |
| Titer BAU/mL | Mean ± SD | 420.19 ± 213.65 | |
| Titer BAU/mL ranges | 0–100 101–200 201–300 301–400 401–500 Above 500 | 23 (8.6) 32 (12.0) 28 (10.5) 35 (13.1) 35 (13.1) 111 (41.6) | |
| Anti-N IgG antibodies | Number (%) | Positive Negative Not available | 202 (75.7) 56 (21.0) 9 (3.4) |
| Titer U/mL | Mean ± SD | 9.36 ± 7.30 | |
| Titer U/mL ranges | 0–10 10.1–20 20.1–30 | 137 (51.3) 105 (39.3) 16 (6.0) | |
| Anti-N IgM antibodies | Number (%) | Positive Negative Not available | 16 (6.0) 241 (90.3) 10 (3.7) |
| Titer U/mL | Mean ± SD | 0.48 ± 0.65 | |
| Titer U/mL ranges | ˂1 ≥1 | 241 (90.3) 16 (6.0) |
| Sinopharm Doses | Pfizer Doses | AstraZeneca Doses | Mixed Doses | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Antibody | Variable | 2 | 3 | 2 | 3 | 2 | 2 | 3 | |
| Anti-S IgG antibodies | Positive N (%) | 75 (93.8) | 11 (100) | 99 (99) | 23 (100) | 11 (100) | 13 (100) | 18 (100) | 0.020 |
| Negative N (%) | 5 (71.4) | 0 (0) | 1 (14.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| Titer BAU/mL Mean ± SD | 323.0 ± 212.9 | 320.9 ± 182.4 | 470.4 ± 189.85 | 531.5 ± 220.1 | 437.8 ± 207.1 | 374.7 ± 179.3 | 489.3 ± 202.8 | 0.000 | |
| Anti-N IgG antibodies | Positive N (%) | 71 (91) | 9 (90) | 72 (72.7) | 19 (82.6) | 7 (63.6) | 6 (50) | 13 (72.2) | 0.015 |
| Negative N (%) | 7 (12.7) | 1 (1.8) | 27 (49.1) | 4 (7.3) | 4 (7.3) | 6 (10.9) | 5 (9.1) | ||
| Titer U/mL Mean ± SD | 10.9 ± 6.3 | 12.3 ± 7.9 | 8.3 ± 7.1 | 10.7 ± 8.0 | 9.4 ± 9.0 | 6.5 ± 8.1 | 7.5 ± 8.2 | 0.000 | |
| Number of COVID-19 Infections That Individuals Have Experienced | Timing of Infection | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Antibody | Variable | 0 | 1 | 2 | 3 | 4 | p Value | Before | After | p Value |
| Anti-S IgG antibodies | Positive N (%) | 135 (52.5) | 84 (32.7) | 29 (11.3) | 6 (2.3) | 3 (1.2) | 0.532 | 38 (14.8) | 84 (32.7) | 0.206 |
| Titer BAU/mL Mean ± SD | 395.8 ± 218.9 | 420.7 ± 215.8 | 509.1 ± 168.1 | 469.9 ± 182.7 | 585.6 ± 67.4 | 0.060 | 393.2 ± 194.5 | 478.4 ± 203.2 | 0.009 | |
| Anti-N IgG antibodies | Positive N (%) | 98 (48.5) | 68 (33.7) | 27 (13.4) | 6 (3.0) | 3 (1.5%) | 0.032 | 28 (13.9) | 76 (37.6) | 0.012 |
| Titer U/mL Mean ± SD | 8.3 ± 7.5 | 9.4 ± 7.2 | 12.5 ± 6.0 | 14.0 ± 3.4 | 14.1 ± 1.4 | 0.015 | 8.5 ± 5.9 | 11.3 ± 7.1 | 0.007 | |
| Hybrid | Vaccine Only | p Value | ||
|---|---|---|---|---|
| All samples | Number | 123 | 141 | |
| Anti-S IgG mean ± SD | 448.04 ± 204.72 | 395.88 ± 218.99 | 0.048 | |
| Anti-N IgG mean ± SD | 10.55 ± 6.88 | 8.32 ± 7.52 | 0.014 | |
| Sinopharm | Number | 45 | 49 | |
| Anti-S IgG mean ± SD | 351.21 ± 206.94 | 307.68 ± 209.84 | 0.299 | |
| Anti-N IgG mean ± SD | 11.86 ± 5.44 | 10.44 ± 7.16 | 0.349 | |
| Pfizer | Number | 57 | 70 | |
| Anti-S IgG mean ± SD | 515.82 ± 175.19 | 449.92 ± 214.85 | 0.069 | |
| Anti-N IgG mean ± SD | 9.97 ± 7.23 | 7.66 ± 7.37 | 0.075 | |
| AstraZeneca | Number | 8 | 4 | |
| Anti-S IgG mean ± SD | 487.63 ± 202.26 | 392.82 ± 232.81 | 0.445 | |
| Anti-N IgG mean ± SD | 10.11 ± 8.34 | 5.68 ± 10.87 | 0.314 | |
| Mixed vaccines | Number | 12 | 19 | |
| Anti-S IgG mean ± SD | 488.63 ± 193.51 | 411.38 ± 201.16 | 0.302 | |
| Anti-N IgG mean ± SD | 9.44 ± 8.77 | 5.44 ± 7.30 | 0.131 |
| Categories | Anti-S IgG | Anti-S IgG Titer | ||||
|---|---|---|---|---|---|---|
| Positive N (%) | Negative N (%) | p Value | Mean ± SD | p Value | ||
| Age | 0–20 21–40 41–60 Above 60 | 11 (4.3) 95 (37.0) 101 (39.3) 50 (19.5) | 0 (0) 0 (0) 5 (71.4) 2 (28.6) | 0.177 | 454.3 ± 219.4 414.3 ± 196.8 389.7 ± 210.2 485.7 ± 238.6 | 0.059 |
| Gender | Male Female | 116 (45.1) 141 (54.4) | 3 (42.9) 4 (57.1) | 1.000 | 436.2 ± 216.6 406.9 ± 210.9 | 0.269 |
| BMI | Underweight < 18.5 Normal 18.5–24.9 Overweight 25–29.9 Obese ≥ 30 | 9 (3.5) 78 (30.4) 100 (38.9) 70 (27.2) | 0 (0) 2 (28.6) 1 (14.3) 4 (57.1) | 0.320 | 525.8 ± 184.6 425.6 ± 204.8 409.2 ± 215.5 416.2 ± 223.7 | 0.470 |
| Smoking | Yes No | 89 (34.6) 168 (65.4) | 4 (57.1) 3 (42.9) | 0.247 | 386.4 ± 197.5 438.5 ± 220.3 | 0.058 |
| Chronic diseases | Yes No | 148 (57.6) 109 (42.4) | 7 (100.0) 0 (0) | 0.044 | 420.7 ± 226.0 419.3 ± 195.7 | 0.957 |
| Anti-N IgG | Anti-N IgG titer | |||||
| Categories | Positive N (%) | Negative N (%) | p Value | Mean ± SD | p Value | |
| Age | 0–20 21–40 41–60 Above 60 | 10 (5.0) 65 (32.2) 80 (39.6) 47 (23.3) | 1 (1.8) 27 (48.2) 23 (41.1) 5 (8.9) | 0.034 | 7.2 ± 6.6 8.5 ± 7.3 8.9 ± 6.9 12.0 ± 7.6 | 0.027 |
| Gender | Male Female | 94 (46.5) 108 (53.5) | 25 (44.6) 31 (55.4) | 0.802 | 9.5 ± 7.7 9.2 ± 6.9 | 0.734 |
| BMI | Underweight < 18.5 Normal 18.5–24.9 Overweight 25–29.9 Obese ≥ 30 | 8 (4.0%) 57 (28.2) 78 (38.6) 59 (29.2) | 1 (1.8) 20 (35.7) 20 (35.7) 15 (26.8) | 0.658 | 10.3 ± 7.0 8.5 ± 7.1 9.6 ± 7.5 9.6 ± 7.2 | 0.726 |
| Smoking | Yes No | 64 (31.7) 138 (68.3) | 29 (51.8) 27 (48.2) | 0.006 | 8.3 ± 7.5 9.9 ± 7.1 | 0.100 |
| Chronic diseases | Yes No | 124 (61.4) 78 (38.6) | 30 (53.6) 26 (46.4) | 0.291 | 9.9 ± 7.5 8.4 ± 6.9 | 0.094 |
| Anti-S IgG | ||||
|---|---|---|---|---|
| Sinopharm | Pfizer | |||
| Positivity (p value) | Titer (p value) | Positivity (p value) | Titer (p value) | |
| Age | 0.330 | 0.091 | 0.533 | 0.268 |
| Gender | 0.391 | 0.099 | 0.498 | 0.205 |
| BMI | 0.748 | 0.083 | 0.597 | 0.904 |
| Smoking | 0.169 | 0.075 | 1.00 | 0.468 |
| Chronic diseases | 0.079 | 0.253 | 0.505 | 0.445 |
| Anti-N IgG | ||||
| Sinopharm | Pfizer | |||
| Positivity (p value) | Titer (p value) | Positivity (p value) | Titer (p value) | |
| Age | 0.759 | 0.682 | 0.009 | 0.035 |
| Gender | 0.715 | 0.912 | 0.310 | 0.394 |
| BMI | 0.867 | 0.485 | 0.850 | 0.721 |
| Smoking | 0.104 | 0.968 | 0.096 | 0.383 |
| Chronic diseases | 1.00 | 0.465 | 0.148 | 0.072 |
| Country | Study Type | Study Population and Number | COVID-19 Vaccine Type | Study Goal | Major Conclusions | Citation |
|---|---|---|---|---|---|---|
| Qatar | Cross-sectional | Male participants of manual and craft worker population n = 300 | Pfizer–BioNTech Moderna AstraZeneca Sinopharm Janssen Covaxin | Long-term anti-S and anti-N IgG antibodies titers | Participants vaccinated with mRNA vaccines had higher median anti-S IgG antibody titers. The median time to reach the lowest quartile was 3.53 months and 7.63 months for the non-mRNA vaccine recipients and Pfizer vaccine recipients, respectively. | [30] |
| UAE | Retrospective | Male expatriate workers n = 952 | Sinopharm Sputnik V Pfizer–BioNTech | Anti-S, anti-N, and neutralizing IgG antibodies, and T-cell response | Priming or boosting with mRNA-based vaccines and with two or more doses was more potent for inducing high levels of humoral response | [31] |
| Iran | Cross-sectional | Healthcare workers n = 174 | Oxford/AstraZeneca COVAXIN Sinopharm Sputnik V | To evaluate anti SARS-CoV-2 antibody response after the second dose of COVID-19 vaccine. | Anti-N and S antibodies mean levels were higher in adenoviral-vectored vaccines compared to inactivated virus vaccines. All antibody levels were significantly higher in those with a past COVID-19 infection | [32] |
| Jordan | Prospective observational | Random Jordanian adults n = 288 | Sinopharm Pfizer–BioNTech | To compare anti-S antibodies in subjects vaccinated with Pfizer–BioNTech or Sinopharm vaccine | Fully vaccinated recipients of the Pfizer–BioNTech vaccine had superior quantitative efficiency compared to Sinopharm recipients | [33] |
| Jordan | Prospective observational | Random Jordanian adults n = 299 | Sinopharm Pfizer–BioNTech | To compare the anti-N antibody levels in people vaccinated with Sinopharm or Pfizer’s or naturally infected unvaccinated adults | Inactivated virus vaccine, Sinopharm, induces an anti-N response that can boost that of natural infection or vice versa. On the other hand, the Pfizer mRNA-based vaccine induces a significantly stronger anti-S Ab response. | [34] |
| Morocco | Cross-sectional | Healthcare workers n = 82 | AstraZeneca Sinopharm | To determine anti-S IgG levels five months after the second vaccination dose | No significant difference between the positivity rates of the vaccinated individuals for gender, age or vaccine type. Longevity of the anti-SARS-CoV-2 IgG antibodies at least five months after vaccination. | [35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Shudifat, A.-E.; Al-Tamimi, M.; Dawoud, R.; Alkhateeb, M.; Mryyian, A.; Alahmad, A.; Abbas, M.M.; Qaqish, A. Anti-S and Anti-N Antibody Responses of COVID-19 Vaccine Recipients. Vaccines 2023, 11, 1398. https://doi.org/10.3390/vaccines11091398
Al-Shudifat A-E, Al-Tamimi M, Dawoud R, Alkhateeb M, Mryyian A, Alahmad A, Abbas MM, Qaqish A. Anti-S and Anti-N Antibody Responses of COVID-19 Vaccine Recipients. Vaccines. 2023; 11(9):1398. https://doi.org/10.3390/vaccines11091398
Chicago/Turabian StyleAl-Shudifat, Abdel-Ellah, Mohammad Al-Tamimi, Rand Dawoud, Mohammad Alkhateeb, Amel Mryyian, Anas Alahmad, Manal M Abbas, and Arwa Qaqish. 2023. "Anti-S and Anti-N Antibody Responses of COVID-19 Vaccine Recipients" Vaccines 11, no. 9: 1398. https://doi.org/10.3390/vaccines11091398
APA StyleAl-Shudifat, A.-E., Al-Tamimi, M., Dawoud, R., Alkhateeb, M., Mryyian, A., Alahmad, A., Abbas, M. M., & Qaqish, A. (2023). Anti-S and Anti-N Antibody Responses of COVID-19 Vaccine Recipients. Vaccines, 11(9), 1398. https://doi.org/10.3390/vaccines11091398