
Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS)

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Laboratory Measurements
2.3. Clinical Data
2.4. Statistical Methods
3. Results
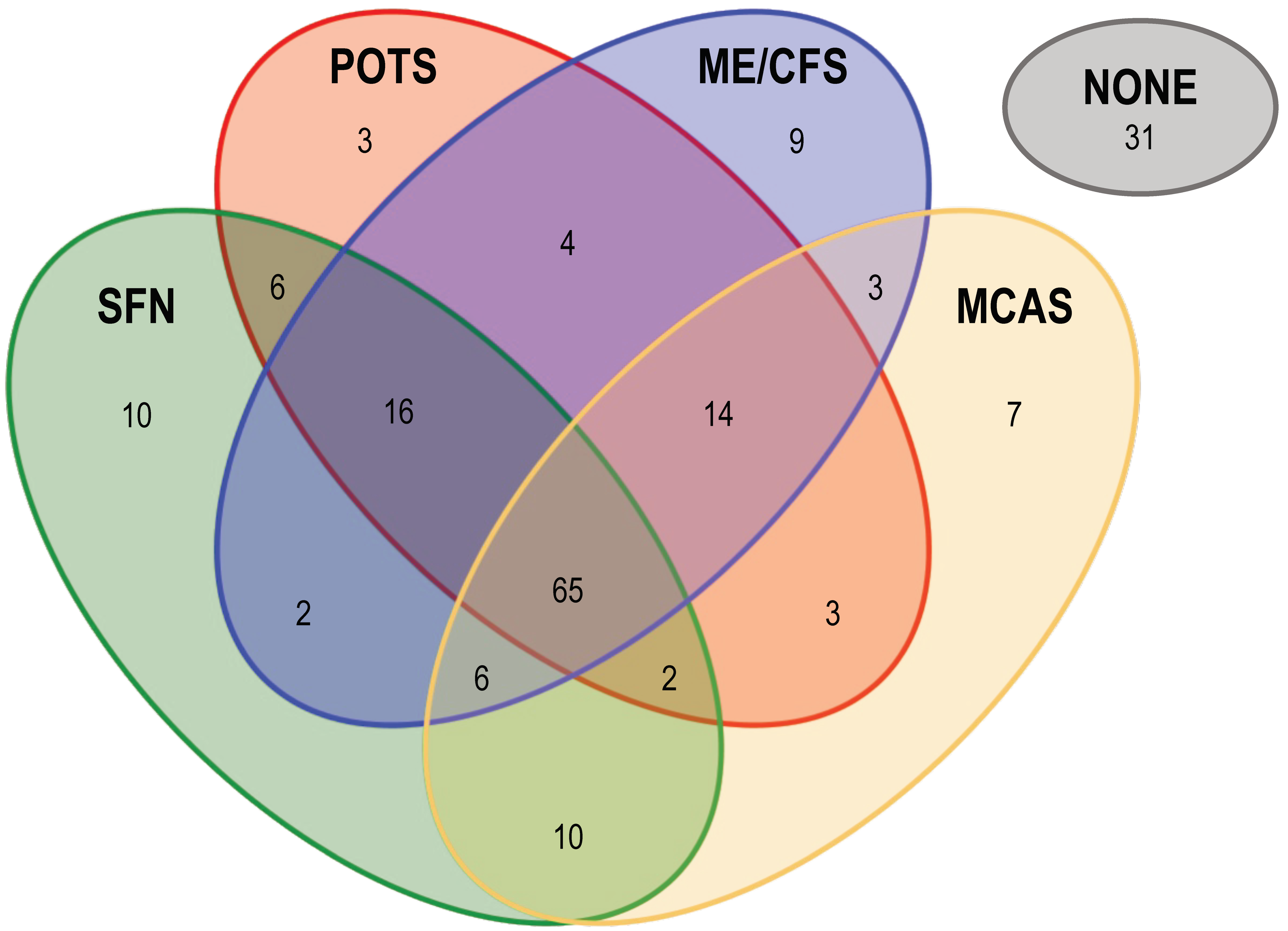
3.1. Prevalence of ME/CFS-, POTS-, SFN- and MCAS-Associated Symptoms in PACVS
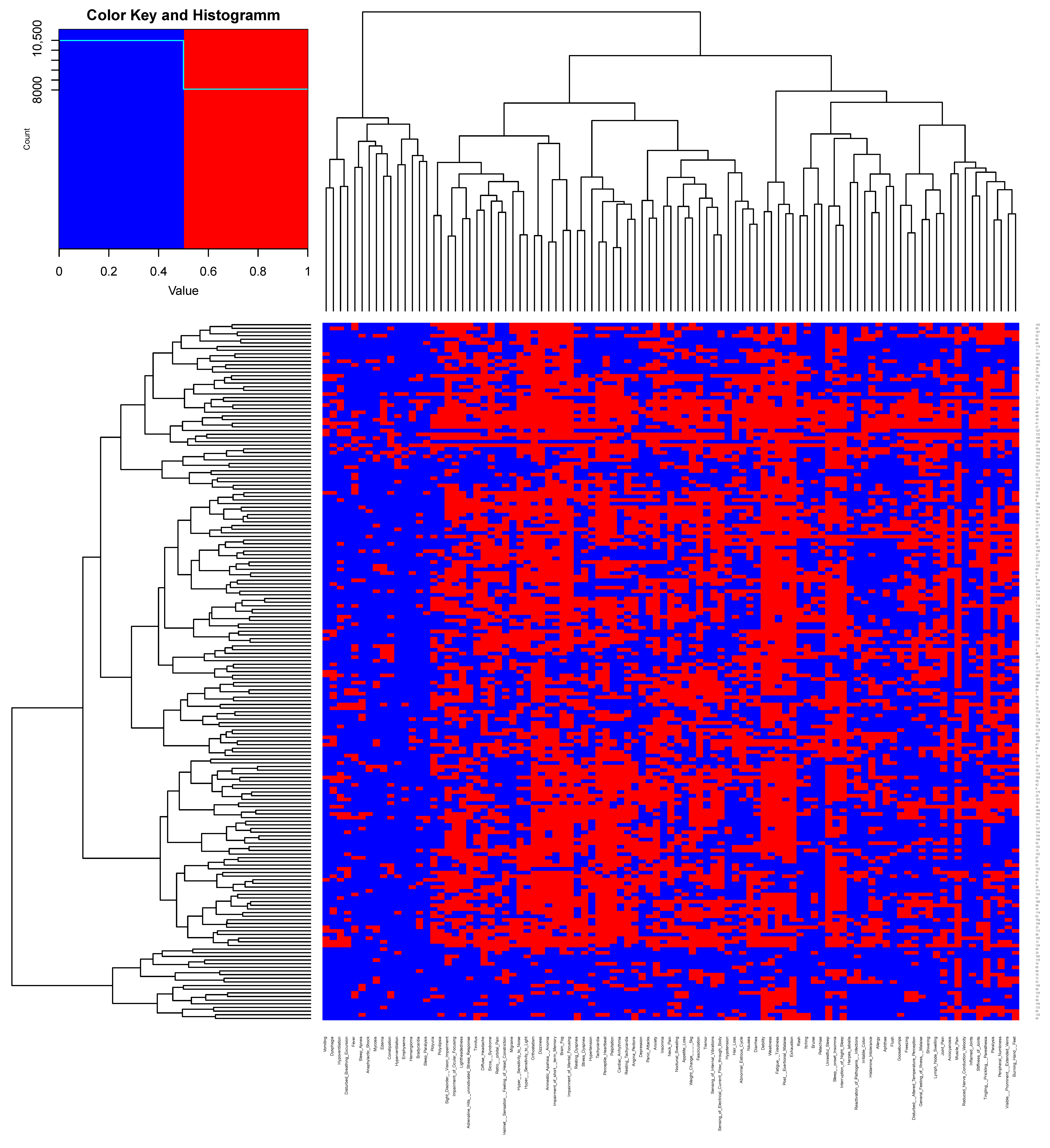
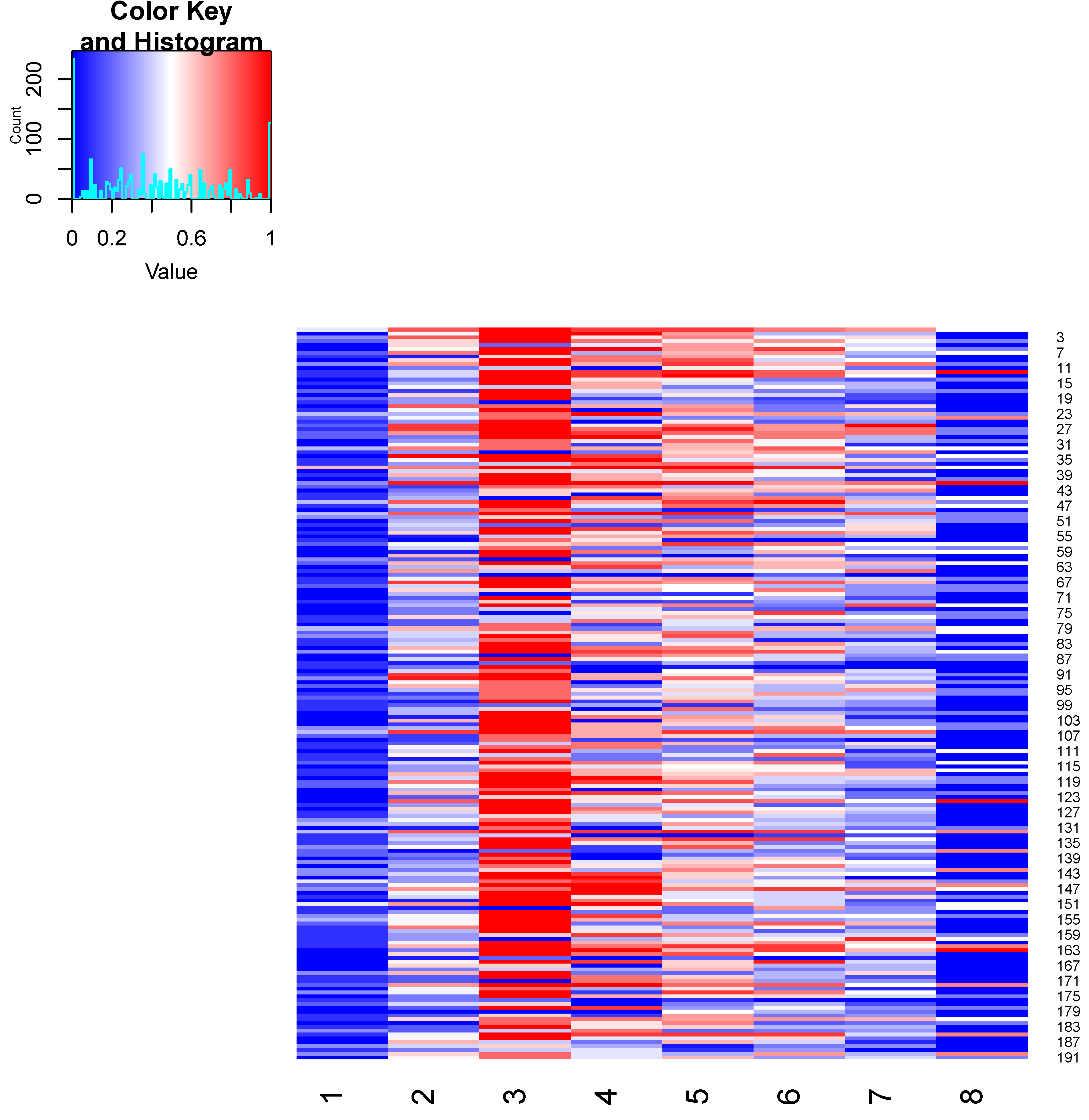
3.2. Unbiased Clustering of PACVS-Associated Symptoms
3.3. Prevalence of Major PACVS-Associated Symptoms
3.4. Abnormalities of Blood Markers in PACVS
4. Discussion
4.1. Comparison of the Clinical Phenotypes of PACVS and ME/CFS
4.2. Comparison with Other Sequelae of SARS-CoV-2 Vaccination
4.3. PACVS-Associated Alterations of Diagnostic Markers
4.3.1. Increased eGFR
4.3.2. Low fT3
4.3.3. Disturbance of Iron Storage
4.3.4. Increase in Serum Neurofilament Light Chain (sNFL)
4.3.5. IgG Subclass Imbalances
4.3.6. Systemic Inflammation
4.3.7. Lipids
4.4. Pathogen Reactivation
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CRP | C-reactive protein |
| eGFR | Estimate of glomerular filtration rate based on serum creatinine or cystatin C |
| fT3 | Free tri-iodine thyroxine |
| fT4 | Free tetra-iodine thyroxine |
| GBS | Guillain-Barré syndrome |
| HDL | High-density lipoptotein |
| LDL | Low-density lipoptotein |
| MCAS | Mast cell activation syndrome |
| ME/CFS | Myalgic encephalomyelitis/chronic fatigue syndrome |
| NAB | PanIg reactivity against SARS-CoV-1 nucleocapsid protein |
| panIg | Immunoglobulins of all classes (A, D, G, E, M) |
| pBNP | Pro-brain natriuretic peptide |
| PEM | Post exertional malaise |
| POTS | Postural tachycardia syndrome |
| PACS | Post-acute COVID-19 syndrome |
| PACVS | Post-acute COVID-19 vaccination syndrome |
| ROC | Receiver-operator characteristics |
| SAB | PanIg reactivity against SARS-CoV-2 spike S1 protein |
| SFN | Small fiber neuropathy |
| sNFL | Serum neurofilament light chain |
| TPO | Thyroid peroxidase |
| TSH | Thyroid-stimulating hormone |
| TSH-R | Receptor for thyroid-stimulating hormone |
References
- Scholkmann, F.; May, C.-A. COVID-19, post-acute COVID-19 syndrome (PACS, “long COVID”) and post-COVID-19 vaccination syndrome (PCVS, “post-COVIDvacsyndrome”):Similarities and differences. Pathol. -Res. Prcatice 2023, 246, 154497. [Google Scholar] [CrossRef] [PubMed]
- Semmler, A.; Mundorf, A.K.; Kuechler, A.S.; Schulze-Bosse, K.; Heidecke, H.; Schulze-Forster, K.; Schott, M.; Uhrberg, M.; Weinhold, S.; Lackner, K.J.; et al. Chronic Fatigue and Dysautonomia following COVID-19 Vaccination Is Distinguished from Normal Vaccination Response by Altered Blood Markers. Vaccines 2023, 11, 1642. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.J.; Son, C.G. Review of case definitions for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2020, 18, 289. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A. Postural orthostatic tachycardia syndrome: Clinical presentation, aetiology and management. J. Intern. Med. 2019, 285, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Tavee, J.; Zhou, L. Small fiber neuropathy: A burning problem. Clevel. Clin. J. Med. 2009, 76, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Hartmann, K.; Bonadonna, P.; Niedoszytko, M.; Triggiani, M.; Arock, M.; Brockow, K. Mast Cell Activation Syndromes: Collegium Internationale Allergologicum Update 2022. Int. Arch. Allergy Immunol. 2022, 183, 693–705. [Google Scholar] [CrossRef]
- Patterson, B.; Francisco, E.; Yogendra, R.; Long, E.; Pise, A.; Beaty, C.; Osgood, E.; Bream, J.; Kreimer, M.; Heide, R.V.; et al. SARS-CoV-2 S1 Protein Persistence in SARS-CoV-2 Negative Post-Vaccination Individuals with Long COVID/PASC-like Symptoms. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Patterson, B.K.; Francisco, E.B.; Yogendra, R.; Long, E.; Pise, A.; Rodrigues, H.; Hall, E.; Herrera, M.; Parikh, P.; Guevara-Coto, J.; et al. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front. Immunol. 2021, 12, 746021. [Google Scholar] [CrossRef]
- Kuechler, A.S.; Weinhold, S.; Boege, F.; Adams, O.; Muller, L.; Babor, F.; Bennstein, S.B.; Pham, T.U.; Hejazi, M.; Reusing, S.B.; et al. A Diagnostic Strategy for Gauging Individual Humoral Ex Vivo Immune Responsiveness Following COVID-19 Vaccination. Vaccines 2022, 10, 1044. [Google Scholar] [CrossRef] [PubMed]
- Benkert, P.; Meier, S.; Schaedelin, S.; Manouchehrinia, A.; Yaldizli, O.; Maceski, A.; Oechtering, J.; Achtnichts, L.; Conen, D.; Derfuss, T.; et al. Serum neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: A retrospective modelling and validation study. Lancet Neurol. 2022, 21, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Reinsberg, J.; Dembinski, J.; Dorn, C.; Behrendt, D.; Bartmann, P.; van Der Ven, H. Determination of total interleukin-8 in whole blood after cell lysis. Clin. Chem. 2000, 46, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Cancarevic, I.; Nassar, M.; Medina, L.; Sanchez, A.; Parikh, A.; Hosna, A.; Devanabanda, B.; Vest, M.; Ayotunde, F.; Ghallab, M.; et al. Nephrotic Syndrome in Adult Patients With COVID-19 Infection or Post COVID-19 Vaccine: A Systematic Review. Cureus 2022, 14, e29613. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Finterer, J.; Scorza, F.A. A retrospective analysis of clinically confirmed long post-COVID vaccination syndrome. J. Clin. Transl. Res. 2022, 8, 506–508. [Google Scholar] [PubMed]
- Finsterer, J.; Scorza, F.A.; Scorza, C.A. Post SARS-CoV-2 vaccination Guillain-Barre syndrome in 19 patients. Clinics 2021, 76, e3286. [Google Scholar] [CrossRef] [PubMed]
- Abolmaali, M.; Rezania, F.; Behnagh, A.K.; Hamidabad, N.M.; Gorji, A.; Mirzaasgari, Z. Guillain-Barré syndrome in association with COVID-19 vaccination: A systematic review. Immunol. Res. 2022, 70, 752–764. [Google Scholar] [CrossRef]
- Finsterer, J. Exacerbating Guillain-Barre Syndrome Eight Days after Vector-Based COVID-19 Vaccination. Case Rep. Infect. Dis. 2021, 2021, 3619131. [Google Scholar] [CrossRef]
- Murvelashvili, N.; Tessnow, A. A Case of Hypophysitis Following Immunization With the mRNA-1273 SARS-CoV-2 Vaccine. J. Investig. Med. High Impact Case Rep. 2021, 9, 23247096211043386. [Google Scholar] [CrossRef] [PubMed]
- Ankireddypalli, A.R.; Chow, L.S.; Radulescu, A.; Kawakami, Y.; Araki, T. A Case of Hypophysitis Associated With SARS-CoV-2 Vaccination. AACE Clin. Case Rep. 2022, 8, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Bouca, B.; Roldao, M.; Bogalho, P.; Cerqueira, L.; Silva-Nunes, J. Central Diabetes Insipidus Following Immunization With BNT162b2 mRNA COVID-19 Vaccine: A Case Report. Front. Endocrinol. 2022, 13, 889074. [Google Scholar] [CrossRef] [PubMed]
- Moura Neto, A.; Zantut-Wittmann, D.E. Abnormalities of Thyroid Hormone Metabolism during Systemic Illness: The Low T3 Syndrome in Different Clinical Settings. Int. J. Endocrinol. 2016, 2016, 2157583. [Google Scholar] [CrossRef] [PubMed]
- Suriawinata, E.; Mehta, K.J. Iron and iron-related proteins in COVID-19. Clin. Exp. Med. 2022, 23, 969–991. [Google Scholar] [CrossRef] [PubMed]
- Legler, F.; Meyer-Arndt, L.; Mödl, L.; Kedor, C.; Freitag, H.; Stein, E.; Hoppmann, U.; Rust, R.; Wittke, K.; Siebert, N.; et al. Long-term symptom severity and clinical biomarkers in post-COVID-19/chronic fatigue syndrome: Results from a prospective observational cohort. eClinicalMedicine 2023, 63, 102146. [Google Scholar] [CrossRef]
- Lutz, L.; Rohrhofer, J.; Zehetmayer, S.; Stingl, M.; Untersmayr, E. Evaluation of Immune Dysregulation in an Austrian Patient Cohort Suffering from Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Biomolecules 2021, 11, 1359. [Google Scholar] [CrossRef] [PubMed]
- Guenther, S.; Loebel, M.; Mooslechner, A.A.; Knops, M.; Hanitsch, L.G.; Grabowski, P.; Wittke, K.; Meisel, C.; Unterwalder, N.; Volk, H.D.; et al. Frequent IgG subclass and mannose binding lectin deficiency in patients with chronic fatigue syndrome. Hum. Immunol. 2015, 76, 729–735. [Google Scholar] [CrossRef]
- Gordon, C.L.; Johnson, P.D.; Permezel, M.; Holmes, N.E.; Gutteridge, G.; McDonald, C.F.; Eisen, D.P.; Stewardson, A.J.; Edington, J.; Charles, P.G.; et al. Association between severe pandemic 2009 influenza A (H1N1) virus infection and immunoglobulin G(2) subclass deficiency. Clin. Infect. Dis. 2010, 50, 672–678. [Google Scholar] [CrossRef]
- Yates, J.L.; Ehrbar, D.J.; Hunt, D.T.; Girardin, R.C.; Dupuis, A.P., 2nd; Payne, A.F.; Sowizral, M.; Varney, S.; Kulas, K.E.; Demarest, V.L.; et al. Serological analysis reveals an imbalanced IgG subclass composition associated with COVID-19 disease severity. Cell Rep. Med. 2021, 2, 100329. [Google Scholar] [CrossRef]
- Schultheiss, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; Girndt, M.; et al. Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19. J. Med. Virol. 2023, 95, e28364. [Google Scholar] [CrossRef] [PubMed]
- Cervia-Hasler, C.; Bruningk, S.C.; Hoch, T.; Fan, B.; Muzio, G.; Thompson, R.C.; Ceglarek, L.; Meledin, R.; Westermann, P.; Emmenegger, M.; et al. Persistent complement dysregulation with signs of thromboinflammation in active Long Covid. Science 2024, 383, eadg7942. [Google Scholar] [CrossRef] [PubMed]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.; Wittke, K.; Hanitsch, L.G.; Zoller, T.; Steinbeis, F.; Haffke, M.; Rudolf, G.; Heidecker, B.; et al. A prospective observational study of post-COVID-19 chronic fatigue syndrome following the first pandemic wave in Germany and biomarkers associated with symptom severity. Nat. Commun. 2022, 13, 5104. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Symptom/Diagnosis 1 | Prevalence (%) | Syndrome Assoc. 2,3 |
|---|---|---|
| Exhaustion | 84.82 | ME/CFS, POTS |
| Debility | 83.77 | ME/CFS, POTS |
| Muscle Pain | 80.63 | ME/CFS, POTS, SFN |
| Unrestful Sleep | 80.63 | ME/CFS |
| Dizziness | 80.10 | ME/CFS, POTS, SFN |
| Tingling/Prickling/Paresthesia | 79.58 | SFN |
| Impairment of Mental Focusing | 78.53 | ME/CFS, POTS |
| Fatigue/Tiredness | 76.96 | ME/CFS, POTS |
| Orthostatism | 76.44 | ME/CFS, POTS, SFN |
| Brain Fog | 76.44 | ME/CFS, POTS |
| Interruption of Night Sleep | 74.87 | ME/CFS, POTS |
| Weakness | 74.35 | ME/CFS, POTS |
| Perceptible Heartbeat | 72.77 | ME/CFS, POTS, SFN |
| Post-Exertional Malaise | 70.68 | ME/CFS |
| Fasciculation | 70.68 | ME/CFS, POTS, SFN |
| Anxiety | 69.11 | ME/CFS, POTS |
| Injury from Immunization | 67.54 | |
| Tachycardia | 65.97 | ME/CFS, POST, SFN |
| Impairment of Short-term Memory | 65.45 | ME/CFS, POTS |
| Hyper-Sensitivity to Noise | 64.92 | ME/CFS, POTS |
| Sleep-onset Insomnia | 64.40 | ME/CFS, POTS |
| Neck Pain | 64.40 | |
| Diffuse Headache | 63.35 | ME/CFS, POTS, MCAS |
| Peripheral Numbness | 62.83 | SFN |
| Amnestic Aphasia/Anomia | 60.73 | ME/CFS, POTS |
| Joint Pain | 60.73 | ME/CFS |
| Sight Disorder/Vision Impairment | 60.21 | ME/CFS |
| Stress Dyspnea | 59.69 | ME/CFS, MCAS |
| Palpitation | 58.64 | ME/CFS, POTS, SFN |
| Sensing of Internal Vibrations | 58.12 | SFN |
| Lightheadedness | 57.59 | ME/CFS, POTS |
| Resting Tachycardia | 57.07 | ME/CFS, POTS, SFN |
| Sensing Electr. Current Flow through Body | 56.02 | SFN |
| Impairment of Ocular Focusing | 56.02 | ME/CFS |
| Hyper-Sensitivity to Light | 55.50 | ME/CFS, POTS |
| Weight Change ≥/≤ 5 kg | 53.93 | ME/CFS, POTS |
| Nausea | 52.36 | ME/CFS, POTS, MCAS |
| Sicca Syndrome | 49.74 | ME/CFS, SFN |
| Tinnitus | 48.17 | |
| Post-Vaccine Syndrome | 47.64 | |
| Nocturnal Sweating | 47.12 | |
| Angina Pectoris | 46.40 | |
| Burning Hand/Feet | 46.07 | SFN |
| Histamine Intolerance | 44.50 | ME/CFS |
| Retro-orbital Pain | 43.98 | ME/CFS, POTS |
| Appetite Loss | 43.46 | |
| Panic Attacks | 43.46 | |
| Cardiac Arrhythmia | 42.93 | ME/CFS, POTS, SFN |
| Abnormal Estrous Cycle | 42.93 | |
| Disturbed/Altered Temp Perception | 40.84 | SFN |
| Freezing | 40.31 | |
| Diarrhea | 40.31 | POTS, MCAS |
| General Feeling of Illness/Malaise | 39.27 | ME/CFS |
| Resting Dyspnea | 39.27 | MCAS |
| Adrenal Hits/Unmotiv. Stress-Response | 39.27 | |
| Helmet Sensation/Head Constriction | 39.27 | ME/CFS, POTS, MCAS |
| Lymph Node Swelling | 38.74 | ME/CFS |
| Visible/Prominent/Extended Veins | 37.70 | |
| Polyuria | 37.17 | ME/CFS, POTS, SFN |
| Hair Loss/Alopecia | 37.17 | |
| Insomnia | 36.13 | ME/CFS, POTS |
| Long COVID without COVID Infection | 36.13 | |
| Hypertension | 34.55 | |
| Tremor | 34.55 | SFN |
| Depression | 32.98 | ME/CFS |
| Shivering | 32.46 | |
| Polydipsia | 31.94 | |
| ME/CFS | 31.94 | |
| Paralysis | 31.41 | SFN |
| Migraine | 30.37 | ME/CFS, POTS |
| Allergy | 29.84 | ME/CFS |
| Stiffness of Joints | 29.32 | |
| Itching | 29.32 | MCAS |
| Irritable Colon | 28.27 | ME/CFS |
| Spont. Bruising (unrelated to trauma) | 27.75 | |
| Reactivation of Pathogens/Infections | 26.70 | |
| Hypotension | 26.18 | ME/CFS, SFN, MCAS |
| Rash | 26.18 | POTS |
| Aphthae | 24.61 | |
| Goosebumps | 24.08 | |
| Vaccine-Induced Inflamm. Response | 24.08 | |
| Petechiae | 23.04 | |
| Hypoventilation | 21.99 | |
| Hyper-Inflammation | 21.99 | POTS |
| Herpes labialis | 21.47 | |
| POTS | 20.94 | |
| Inflamed Joints | 20.42 | |
| Flush | 20.42 | MCAS |
| Fever | 19.90 | |
| Acrocyanosis | 19.90 | POTS |
| Reduced Nerve Conduction Velocity | 19.90 | POTS, MCAS |
| Dysphagia | 19.90 | POTS |
| MCAS | 19.37 | |
| Myocarditis/Pericarditis | 18.85 | |
| Fibromyalgia | 17.80 | |
| SFN | 17.80 | |
| Constipation | 17.28 | |
| Edema | 14.14 | MCAS |
| Bradycardia | 13.61 | POTS, SFN |
| Disturbed Breathing Excursion | 13.61 | |
| Mycosis | 12.57 | |
| Vomiting | 12.57 | |
| Sleep Apnea | 12.04 | MCAS |
| Sleep Paralysis | 7.85 | |
| Hyperventilation | 7.85 | |
| Hemangioma | 7.33 | POTS |
| Thrombosis | 6.81 | |
| Anaphylactic Shock | 5.76 | MCAS |
| Shingles | 5.76 | |
| Guillain-Barré Syndrome | 4.71 | |
| Emphysema | 3.66 | |
| Facial Nerve Paresis | 3.14 |
Cluster 1: General Unwellness
|
Cluster 2: Peripheral Nerve Dysfunction, Dysesthesia, Paralysis, Pain, Vasomotor Dysfunction
|
Cluster 3: Chronic Fatigue, Malaise
|
Cluster 4: Cardiovascular Impairment
|
Cluster 5: Cognitive Impairment, Headache, visual and acoustic Dysfunctions
|
Cluster 6: Psychomotoric Dysfunction, Anxiety, Disturbed Body Perception, Gastrointestinal Dysfunction
|
Cluster 7: Sleep Disturbance, Cutaneous Symptoms
|
Cluster 8: Dyspagia, Breathing Impairment
|
| Normal Range (n.r.) 1 [Dimension] | Below n.r. 2 n (%) | Above n.r. 2 n (%) | Remarks | |
|---|---|---|---|---|
| Kidney | GFR > 120 always associated with urea <18 | |||
| eGFR (CAPA) | 60–120 [mL/min/1.73 m2] | 14 (7) | 33 (17) | |
| eGFR (CKD-EPI) | 60–120 [mL/min/1.73 m2] | 1 (1) | 30 (16) | |
| Urea | ♀ 21–43, ♂ 18–55 [mg/dL] | 70 (37) | 1 (1) | |
| Thyroid | All other fT3-values in lower half of n.r. | |||
| TSH | 0.27–4.2 [µIU/mL] | 4 (2) | 4 (2) | |
| fT3 | ♀ 2.6–5, ♂ 2–4.4 [ng/mL] | 65 (34) | - | |
| fT4 | ♀ 9.8–16.3, ♂ 9.3–17.1 [pg/mL] | 14 (7) | 7 (4) | |
| anti-TPO | ≤34 [IU/mL) | - | 18 (9) | |
| anti-TSH-R | ≤1.7 [IU/L] | - | 1 (1) | |
| Cardiac markers | ||||
| ProBNP | ≤125 [pg/mL] | - | ||
| hsTroponin T | ♀ ≤ 14, ♂ ≤ 11 [ng/L] | 1 (1) | ||
| Liver | AST/ALT ≤ 1 in all cases No value > 2 | |||
| AST | ♀ ≤ 3, ♂ ≤ 35 [U/L] | 20 (10) | ||
| ALT | ♀ ≤ 35, ♂ ≤ 45 [U/L] | 11 (6) | ||
| ALP | ♀ ≤ 104, ♂ ≤ 129 [U/L] | 1 (1) | ||
| gammaGT | ♀ ≤ 38, ♂ ≤ 55 [U/L] | 7 (4) | ||
| Bilirubin | ≤1.2 [mg/dL] | 8 (4) | ||
| Lipids | Fasting state not assured | |||
| Cholesterol | ≤200 [mg/dL] | 61 (32) | ||
| Trigliceride | ≤150 [mg/dL] | 39 (20) | ||
| LDL | ≤160 [mg/dL] | 10 (5) | ||
| HDL | ≥40 [mg/dL] | 32 (17) | ||
| LDL/HDL | 2.5–3.5 | 117 (62) | 4 (2) | |
| Inflammation | IL-6 up to 50,000 IL-8 up to 2,000,000 | |||
| Il-6 | ≤7 [pg/mL] | - | 115 (60) | |
| Il-8 | ≤62 [pg/mL] | - | 172 (90) | |
| CRP | ≤0.5 [mg/dL] | - | 13 (7) | |
| IgG subclasses | ||||
| total | 700–1600 [mg/dL] | 19 (10) | 3 (2) | |
| IgG1 | 280–800 [mg/dL] | 1 (1) | 18 (9) | |
| IgG2 | 115–570 [mg/dL] | 2 (1) | 5 (3) | |
| IgG3 | 24–125 [mg/dL] | 88 (46) | 17 (9) | |
| IgG4 | 5.2–125 [mg/dL] | 12 (6) | 21 (11) | |
| Iron metabolism | ||||
| Fe | ♀ 37–165, ♂ 40–155 [µg/dL] | 9 (5) | 20 (10) | |
| Ferritin | ♀ 13–150, ♂ 30–400 [µg/L] | 11 (6) | 3 (2) | |
| Transferrin | 200–360 [mg/dL] | 34 (18) | 3 (2) | |
| Transf. Saturation | 16–45 [%] | 27 (14) | 20 (10) | |
| Sol Transf. Recept. | 0.81–1.75 [mg/L] | 36 (19) | 4 (2) | |
| Ferritin Index | 0.63–2.2 | 117 (61) | 2 (1) | |
| Neurodegeneration | Adjusted for age, BMI, GFR according to ref. [12] | |||
| sNFL | <1.5 (zScore) | 39 (20) | ||
| sNFL | 10–90 (Percentile) | 6 (3) | 52 (27) | |
| BMI | 18.5–30 | 19 (10) | 16 (8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mundorf, A.K.; Semmler, A.; Heidecke, H.; Schott, M.; Steffen, F.; Bittner, S.; Lackner, K.J.; Schulze-Bosse, K.; Pawlitzki, M.; Meuth, S.G.; et al. Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS). Vaccines 2024, 12, 790. https://doi.org/10.3390/vaccines12070790
Mundorf AK, Semmler A, Heidecke H, Schott M, Steffen F, Bittner S, Lackner KJ, Schulze-Bosse K, Pawlitzki M, Meuth SG, et al. Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS). Vaccines. 2024; 12(7):790. https://doi.org/10.3390/vaccines12070790
Chicago/Turabian StyleMundorf, Anna Katharina, Amelie Semmler, Harald Heidecke, Matthias Schott, Falk Steffen, Stefan Bittner, Karl J. Lackner, Karin Schulze-Bosse, Marc Pawlitzki, Sven Guenther Meuth, and et al. 2024. "Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS)" Vaccines 12, no. 7: 790. https://doi.org/10.3390/vaccines12070790
APA StyleMundorf, A. K., Semmler, A., Heidecke, H., Schott, M., Steffen, F., Bittner, S., Lackner, K. J., Schulze-Bosse, K., Pawlitzki, M., Meuth, S. G., Klawonn, F., Ruhrländer, J., & Boege, F. (2024). Clinical and Diagnostic Features of Post-Acute COVID-19 Vaccination Syndrome (PACVS). Vaccines, 12(7), 790. https://doi.org/10.3390/vaccines12070790