

Vaccination Knowledge, Attitudes, Perceptions, and Educational Needs of Pharmacists in Singapore: A Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Pharmacists’ Participation in Survey
3.2. Demographics of Pharmacists
3.3. Pharmacists’ Vaccination Knowledge
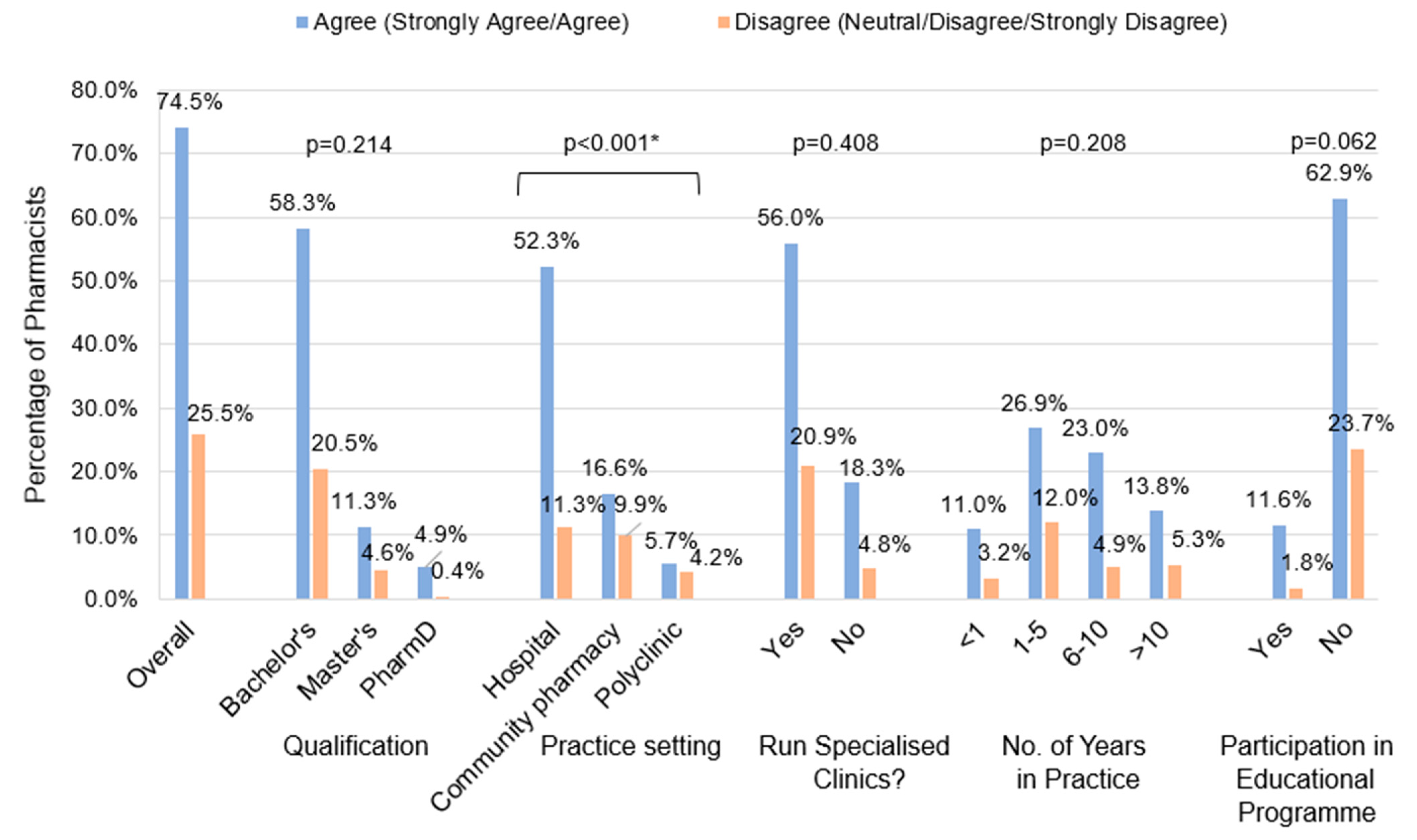
3.4. Confidence in and Perception of Pharmacist’s Role in Providing Vaccination Services
3.5. Practice Behaviour of Pharmacists
3.6. Willingness to Serve as Vaccine Providers
3.7. Barriers to Pharmacist-Led Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| 1 | Please indicate your gender:
|
| 2 | Please indicate your age:
|
| 3 | Please indicate your race:
|
| 4 | Please indicate the vaccinations that you have received (Please select all that apply):
|
| 5 | Please indicate your highest academic qualification:
|
| 6 | Please indicate the status of your Practising Certificate: [SKIP TO Q9 if “Inactive status” is selected]
|
| 7 | Please indicate your current practice setting: For locum pharmacists, please select others and indicate your practice setting
|
| 8 | Are you currently running any clinics or specialised services?
|
| 9 | Please indicate your number of years in practice:
|
| Knowledge | |
| 10 | Have you participated in any educational programs (modules, workshops, etc.) regarding vaccinations?
|
| 11 | Please select the information sources that you usually consult to obtain information about vaccination (Please select all that apply)
|
| 12 | Please answer the following questions to the best of your ability. |
| 12a | It is recommended to avoid giving live and inactivated vaccinations simultaneously.
|
| 12b | To administer an intramuscular injection, pinch the skin and insert the needle at a 45° angle.
|
| 12c | Apart from the usual symptoms of anaphylaxis, requests for water and thirst shortly after vaccination can hint that anaphylaxis is under way.
|
| 12d | The quadrivalent influenza vaccine covers against one influenza A H1N1 virus, one influenza A H7N9 virus and two influenza B viruses.
|
| 12e | For the hepatitis B vaccine, an interruption in the vaccination schedule (missed dose) does not call for extra doses or restarting the entire series of vaccination.
|
| 12f | The recommended vaccinations for patients <65 years old with chronic liver disease include the influenza vaccine and both pneumococcal vaccines (PCV13 and PPSV23).
|
| Attitude and Perception | |
| 13 | I believe that Pharmacists have an important role to play in providing vaccination services.
|
| 14 | Please rate your confidence level in providing the following vaccination services: Very confident: I have the skills and knowledge to provide the service for all adult vaccines and I am able to train others to provide the service. Confident: I have the skills and knowledge required to provide the service for all adult vaccines. Moderately confident: I have adequate skills and knowledge required to provide the service in my current practice setting. Slightly confident: I have some level of the skills and knowledge required to provide the service but am uncertain at times. Not confident: I lack the skills and knowledge required to provide the service. |
| 14a | Educating patients about adult vaccinations
|
| 14b | Recommending vaccinations for adult patients (directly to patients/through other healthcare professionals)
|
| 14c | Administering vaccines to adult patients
|
| 15 | Please rate how frequent you provide the following vaccination services Always: I provide the service at least once a week. Often: I provide the service at least once a month. Sometimes: I have provided the service at least once in the past 3 months. Rarely: I have provided the service at least once during practice. Never: I have never provided the service. |
| 15a | Educating patients about adult vaccinations
|
| 15b | Recommending vaccination for adult patients (directly to patients/through other healthcare professionals)
|
| 16 | If given the opportunity, I would like to be able to provide direct administration of vaccines to patients. Please elaborate on why you have chosen the option.
|
| 17 | Which adult vaccines do you think should be directly offered by Pharmacists? (Please select all that apply)
|
| 18 | Please rank the top 3 potential barriers for Pharmacists to implement direct administration of vaccines.
|
| Knowledge | |
| 19 | Are you interested in future education programs on vaccination? [SKIP questions 20 and 21 if “No” was selected]
|
| 20 | What are some areas regarding vaccination that you are interested to find out more about? (Please select all that apply)
|
| 21 | Which of the following is your preferred type of education program on vaccination? (Please select all that apply)
|
| Characteristics | N = 283 |
|---|---|
| Gender | |
| Male | 199 (70.3%) |
| Female | 84 (29.7%) |
| Age in years | |
| 20–29 | 143 (50.5%) |
| 30–39 | 110 (38.9%) |
| 40–49 | 22 (7.8%) |
| 50–59 | 6 (2.1%) |
| ≥ 60 | 2 (0.7%) |
| Ethnicity | |
| Chinese | 270 (95.4%) |
| Malay | 3 (1.1%) |
| Indian | 7 (2.5%) |
| Others—2 Vietnamese, 1 Filipino | 3 (1.0%) |
| Vaccinations received | |
| Hepatitis B | 252 (89.0%) |
| Influenza | 244 (86.2%) |
| Measles-Mumps-Rubella (MMR) | 256 (90.5%) |
| Varicella | 144 (50.9%) |
| Tetanus, Diptheria & Acellular Pertussis (TdAP) | 245 (86.6%) |
| Highest qualifications | |
| Bachelor of Science/Pharmacy | 223 (78.8%) |
| Masters | 45 (15.9%) |
| PharmD | 15 (5.3%) |
| Status of Practising Certificate | |
| Pre-registration/Conditional registration | 21 (7.4%) |
| Active status | 262 (92.6%) |
| Inactive | 0 (0.0%) |
| Practice setting | |
| Hospital | 180 (63.6%) |
| Community Pharmacy | 68 (24.0%) |
| Locum Community Pharmacy | 7 (2.5%) |
| Polyclinic | 28 (9.9%) |
| Others | 0 (0.0%) |
| Running any specialised clinics? (N = 268) | |
| Yes | 62 (23.1%) |
| No | 206 (76.9%) |
| Number of years in practice | |
| <1 | 40 (14.1%) |
| 1–5 | 110 (38.9%) |
| 6–10 | 79 (27.9%) |
| 11–20 | 40 (14.1%) |
| 21–30 | 10 (3.5%) |
| >30 | 4 (1.4%) |
| Participation in education programme | |
| Yes | 38 (13.4%) |
| No | 245 (86.6%) |
| Sources of information | |
| Local vaccination guidelines | 248 (87.6%) |
| International guidelines | 220 (77.7%) |
| Medical/Scientific resources | 176 (62.2%) |
| Educational programs | 24 (8.5%) |
| Mass media/Internet | 7 (2.5%) |
| Healthcare Professionals | 126 (44.5%) |
| Knowledge | |
| It is recommended to avoid giving live and inactivated vaccinations simultaneously. | |
| True | 65 (23.0%) |
| False (correct) | 154 (54.4%) |
| Not sure | 64 (22.6%) |
| To administer an intramuscular injection, pinch the skin and insert the needle at a 45° angle. | |
| True | 35 (12.4%) |
| False (correct) | 211 (74.5%) |
| Not sure | 37 (13.1%) |
| Apart from the usual symptoms of anaphylaxis, requests for water and thirst shortly after vaccination can hint that anaphylaxis is under way. | |
| True (correct) | 39 (13.8%) |
| False | 89 (31.4%) |
| Not sure | 155 (54.8%) |
| The quadrivalent influenza vaccine covers against one influenza A H1N1 virus, one influenza A H7N9 virus and two influenza B viruses. | |
| True | 84 (29.7%) |
| False (correct) | 68 (24.0%) |
| Not sure | 131 (46.3%) |
| For the hepatitis B vaccine, an interruption in the vaccination schedule (missed dose) does not call for extra doses or restarting the entire series of vaccination. | |
| True (correct) | 114 (40.3%) |
| False | 91 (32.2%) |
| Not sure | 78 (27.5%) |
| The recommended vaccinations for patients <65 years old with chronic liver disease include the influenza vaccine and both pneumococcal vaccines (PCV13 and PPSV23). | |
| True | 138 (48.8%) |
| False (correct) | 90 (31.8%) |
| Not sure | 55 (19.4%) |
| Perceived knowledge | |
| Confidence in educating adult patients | |
| Very Confident | 7 (2.5%) |
| Confident | 48 (17.0%) |
| Moderately Confident | 81 (28.6%) |
| Slightly Confident | 95 (33.5%) |
| Not Confident | 52 (18.4%) |
| Confidence in recommending vaccinations for adult patients | |
| Very Confident | 8 (2.8%) |
| Confident | 55 (19.5%) |
| Moderately Confident | 82 (29.0%) |
| Slightly Confident | 87 (30.7%) |
| Not Confident | 51 (18.0%) |
| Confidence in administering vaccinations to adult patients | |
| Very Confident | 5 (1.8%) |
| Confident | 6 (2.1%) |
| Moderately Confident | 13 (4.6%) |
| Slightly Confident | 22 (7.8%) |
| Not Confident | 237 (83.7%) |
| Attitude and Perception | |
| I believe that Pharmacists have an important role to play in providing vaccination services. | |
| Strongly Agree | 81 (28.6%) |
| Agree | 130 (45.9%) |
| Neither Agree nor Disagree | 59 (20.9%) |
| Disagree | 12 (4.2%) |
| Strongly Disagree | 1 (0.4%) |
| If given the opportunity, I would like to be able to provide direct administration of vaccines to patients. | |
| Strongly Agree | 33 (11.7%) |
| Agree | 67 (23.7%) |
| Neither Agree nor Disagree | 85 (30.0%) |
| Disagree | 70 (24.7%) |
| Strongly Disagree | 28 (9.9%) |
| Frequency of educating adult patients | |
| Always | 11 (3.9%) |
| Often | 23 (8.1%) |
| Sometimes | 57 (20.1%) |
| Rarely | 112 (39.6%) |
| Never | 80 (28.3%) |
| Frequency of recommending vaccinations for adult patients | |
| Always | 19 (6.7%) |
| Often | 32 (11.3%) |
| Sometimes | 55 (19.4%) |
| Rarely | 99 (35.0%) |
| Never | 78 (27.6%) |
| Vaccinations that should be administered by pharmacists (n = 283) | |
| Influenza | 245 (86.6%) |
| Pneomococcal | 149 (52.7%) |
| Potential COVID-19 vaccine | 102 (36.0%) |
| Hepatitis B | 77 (27.2%) |
| Varicella | 61 (21.6%) |
| Zoster | 54 (19.1%) |
| TdAP | 49 (17.3%) |
| Tetanus Post exposure | 42 (14.8%) |
| Hepatitis A | 36 (12.7%) |
| Measles-Mumps-Rubella | 34 (12.0%) |
| Haemophilus Influenza Type B | 27 (9.5%) |
| Polio | 25 (8.8%) |
| Typhoid | 24 (8.5%) |
| Yellow Fever | 23 (8.1%) |
| Rabies | 15 (5.3%) |
| Cholera | 13 (4.6%) |
| Japanese Encephalitis | 1 (0.4%) |
| Others—2 Human Papillomavirus, 1 Dengue | 3 (1.1%) |
| Barriers | |
| Uncomfortable with injections | 198 (70.0%) |
| Ranked 1st | 103 (36.4%) |
| Ranked 2nd | 51 (18.0%) |
| Ranked 3rd | 44 (15.5%) |
| Lack of knowledge/skills | 200 (70.7%) |
| Ranked 1st | 79 (27.9%) |
| Ranked 2nd | 78 (27.6%) |
| Ranked 3rd | 43 (15.2%) |
| Lack of time | 120 (42.4%) |
| Ranked 1st | 40 (14.1%) |
| Ranked 2nd | 30 (10.6%) |
| Ranked 3rd | 50 (17.7%) |
| Lack of space | 83 (29.3%) |
| Ranked 1st | 18 (6.4%) |
| Ranked 2nd | 32 (11.3%) |
| Ranked 3rd | 33 (11.7%) |
| Lack of support from patients | 110 (38.9%) |
| Ranked 1st | 17 (6.0%) |
| Ranked 2nd | 51 (18.0%) |
| Ranked 3rd | 42 (14.8%) |
| Lack of support from other HCP | 101 (35.7%) |
| Ranked 1st | 14 (4.9%) |
| Ranked 2nd | 32 (11.3%) |
| Ranked 3rd | 55 (19.4%) |
| Others | 16 (5.7%) |
| Ranked 1st | 5 (1.8%) |
| Ranked 2nd | 2 (0.7%) |
| Ranked 3rd | 9 (3.2%) |
| Ranked 1st (n = 283) | |
| Uncomfortable with injections | 109 (38.5%) |
| Lack of knowledge/skills | 80 (28.3%) |
| Lack of time | 41 (14.5%) |
| Lack of space | 18 (6.4%) |
| Lack of support from patients | 17 (6.0%) |
| Lack of support from other HCP | 13 (4.6%) |
| Others | 5 (1.8%) |
| Educational Needs | |
| Interest in educational programmes | |
| Yes | 247 (87.3%) |
| No | 36 (12.7%) |
| Areas of interest (n = 247) | |
| Indication and contraindication | 219 (88.7%) |
| Dose of vaccine, number and freq of doses | 207 (83.8%) |
| Administration techniques | 194 (78.5%) |
| Management of SE and adverse reactions | 184 (74.5%) |
| Patient counselling | 180 (72.9%) |
| Others (sieved) | 4 (1.6%) |
| Type of programme (n = 247) | |
| Large group lecture/talks | 89 (36.0%) |
| Small group seminar | 87 (35.2%) |
| Hands-on workshop | 172 (69.6%) |
| Web-lecture (webinar) | 163 (66.0%) |
| Modules | 168 (68.0%) |
| Reading materials | 138 (55.9%) |
References
- World Health Organization. Health Topics: Vaccines and Immunization. Available online: https://www.who.int/topics/immunization/en/ (accessed on 17 July 2024).
- Ministry of Health. Communicable Disease Surveillance: Singapore 2018 Report. 2019. Available online: https://www.moh.gov.sg/docs/librariesprovider5/diseases-updates/communicable-diseases-surveillance-in-singapore-2018210c9a3beaa94db49299c2da53322dce.pdf (accessed on 17 July 2024).
- Chua, A. MOH introduces new list of recommended vaccine jabs for adults. Today. 21 October 2017. Available online: https://www.todayonline.com/singapore/moh-introduces-new-list-recommended-vaccine-jabs-adults (accessed on 17 July 2024).
- Hsu, L.Y.; Cook, A.R. Commentary: Why is Singapore vaccination rate so low? Today. 18 August 2019. Available online: https://www.todayonline.com/commentary/why-singapores-adult-vaccination-rate-so-low (accessed on 17 July 2024).
- Kaur, A. Parliament: Subsidised vaccines for children and adults at all Chas GP clinics and polyclinics. The Straits Times. 5 March 2020. Available online: https://www.straitstimes.com/politics/parliament-subsidised-vaccines-for-children-and-adults-at-all-chas-gp-and-polyclinics (accessed on 17 July 2024).
- Ministry of Health. News Highlights: Adult Immunisation Vaccinations Take-Up Rates. 3 February 2020. Available online: https://www.moh.gov.sg/news-highlights/details/adult-immunisation-vaccinations-take-up-rate (accessed on 17 July 2024).
- Teo, L.M.; Smith, H.E.; Lwin, M.O.; Tang, W.E. Attitudes and perception of influenza vaccines among older people in Singapore: A qualitative study. Vaccine 2019, 37, 6665–6672. [Google Scholar] [CrossRef] [PubMed]
- Rahim, M.H.A.; Dom, S.H.M.; Hamzah, M.S.R.; Azman, S.H.; Zaharuddin, Z.; Fahrni, M.L. Impact of pharmacist interventions on immunisation uptake: A systematic review and meta-analysis. J. Pharm. Policy Pract. 2023, 17, 2285955. [Google Scholar] [CrossRef] [PubMed]
- Eldooma, I.; Maatoug, M.; Yousif, M. Outcomes of Pharmacist-Led Pharmaceutical Care Interventions Within Community Pharmacies: Narrative Review. Integr. Pharm. Res. Pract. 2023, 12, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Ecarnot, F.; Crepaldi, G.; Juvin, P.; Grabenstein, J.; Del Giudice, G.; Tan, L.; O’Dwyer, S.; Esposito, S.; Bosch, X.; Gavazzi, G.; et al. Pharmacy-based interventions to increase vaccine uptake: Report of a multidisciplinary stakeholders meeting. BMC Public Health 2019, 19, 1698. [Google Scholar] [CrossRef]
- Goad, J.A.; Taitel, M.S.; Fensterheim, L.E.; Cannon, A.E. Vaccinations administered during off-clinic hours at a national community pharmacy: Implications for increasing patient access and convenience. Ann. Fam. Med. 2013, 11, 429–436. [Google Scholar] [CrossRef]
- Gerges, S.; Peter, E.; Bowles, S.K.; Diamond, S.; Bucci, L.M.; Resnick, A.; Taddio, A. Pharmacists as vaccinators: An analysis of their experiences and perceptions of their new role. Hum. Vaccines Immunother. 2018, 14, 471–477. [Google Scholar] [CrossRef]
- Papastergiou, J.; Folkins, C.; Li, W.; Zervas, J. Community pharmacist-administered influenza immunization improves patient access to vaccination. Can. Pharm. J. 2014, 147, 359–365. [Google Scholar] [CrossRef]
- Merks, P.; Kowalczuk, A.; Wong, A.; Chung, K.; Religioni, U.; Świetlik, D.; Rotmans-Plagens, K.; Cameron, J.; Sola, K.F.; Kazmierczak, J.; et al. Patient Satisfaction with Pharmacist-Administered COVID-19 Vaccines in Poland: A Survey Study in the Vaccination Centres Context. BMC Health Serv. Res. 2022, 22, 1339. [Google Scholar] [CrossRef]
- Rubin, S.E.; Schulman, R.M.; Roszak, A.R.; Herrmann, J.; Patel, A.; Koonin, L.M. Leveraging partnerships among community pharmacists, pharmacies, and health departments to improve pandemic influenza response. Biosecur. Bioterror. 2014, 12, 76–84. [Google Scholar] [CrossRef]
- American Pharmacists Association. APhA Pharmacy-Based Immunisation Delivery: A National Certificate Training Program; American Pharmacists Association: Washington, DC, USA, 2017. [Google Scholar]
- Grzegorczyk-Karolak, I.; Zglińska-Pietrzak, A.; Weremczuk-Jeżyna, I.; Kałucka, S. Evaluation of Patient Experiences Regarding Pharmacist-Administrated Vaccination and Attitude Towards Future Additional Pharmacy Services in Poland. Vaccines 2022, 10, 1479. [Google Scholar] [CrossRef]
- Paudyal, V.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Cadogan, C.; Da Costa, F.A.; Galfrascoli, E.; Pudritz, Y.M.; et al. Pharmacists’ Involvement in COVID-19 Vaccination Across Europe: A Situational Analysis of Current Practice and Policy. Int. J. Clin. Pharm. 2021, 43, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Grabenstein, J.D. Essential Services: Quantifying the Contributions of America’s Pharmacists in COVID-19 Clinical Interventions. J. Am. Pharm. Assoc. 2022, 62, 1929–1945. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, N.; Duckett, K.; Chee, F.Y.; Koh, C.T.; Sidharta, S.; Venkatachalam, I.; Chow, A.; Yoong, J. “I wouldn’t really believe statistics”—Challenges with influenza vaccine acceptance among healthcare workers in Singapore. Vaccine 2018, 36, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.M.; Khan, A.U.; Ali, I.; Wu, D.B. Knowledge, attitude and awareness among healthcare professionals about influenza vaccination in Peshawar, Pakistan. Vaccine 2016, 34, 1393–1398. [Google Scholar] [CrossRef]
- Tolentino, V.; Unni, E.; Montuoro, J.; Bezzant-Ogborn, D.; Kepka, D. Utah pharmacists’ knowledge, attitudes, and barriers regarding human papillomavirus vaccine recommendation. J. Am. Pharm. Assoc. 2018, 58, S16–S23. [Google Scholar] [CrossRef]
- Chumnumwat, S.; Montakantikul, P.; Wongpakwat, J.; Siriwannapha, N.; Pitaknitinun, K. An Analysis of Attitudes, Knowledge, and Willingness of Thai Pharmacists as Vaccinators: A Nationwide Survey Study. J. Am. Coll. Clin. Pharm. 2023, 7, 376–383. [Google Scholar] [CrossRef]
- Della Polla, G.; Napolitano, F.; Pelullo, C.P.; De Simone, C.; Lambiase, C.; Angelillo, I.F. Investigating knowledge, attitudes, and practices regarding vaccinations of community pharmacists in Italy. Hum. Vaccines Immunother. 2020, 16, 2422–2428. [Google Scholar] [CrossRef]
- Youssef, D.; Abou-Abbas, L.; Farhat, S.; Hassan, H. Pharmacists as immunizers in Lebanon: A national survey of community pharmacists’ willingness and readiness to administer adult immunization. Hum. Resour. Health 2021, 19, 131. [Google Scholar] [CrossRef]
- Tak, C.R.; Marciniak, M.W.; Savage, A.; Ozawa, S. The essential role of pharmacists facilitating vaccination in older adults: The case of Herpes Zoster. Hum. Vaccines Immunother. 2020, 16, 70–75. [Google Scholar] [CrossRef]
- Gajdács, M.; Paulik, E.; Szabó, A. Knowledge, Attitude and Practice of Community Pharmacists Regarding Antibiotic Use and Infectious Diseases: A Cross-Sectional Survey in Hungary (KAPPhA-HU). Antibiotics 2020, 9, 41. [Google Scholar] [CrossRef]
- Qamar, M.; Koh, C.M.; Choi, J.H.; Mazlan, N.A. Community pharmacist’s knowledge towards the vaccination and their willingness to implement the community-based vaccination service in Malaysia. J. Appl. Pharm. Sci. 2022, 12, 128–139. [Google Scholar] [CrossRef]
- Tadele, S.; Demissie, B.N.; Tamiru, M.T.; Tadesse, T.A. Knowledge and attitudes of community pharmacists on vaccination, barriers and willingness to implement community pharmacy-based vaccination services in Ethiopia. Hum. Vaccines Immunother. 2023, 19, 2291243. [Google Scholar] [CrossRef] [PubMed]
- Poudel, A.; Lau, E.T.L.; Deldot, M.; Campbell, C.; Waite, N.M.; Nissen, L.M. Pharmacist role in vaccination: Evidence and challenges. Vaccine 2019, 37, 5939–5945. [Google Scholar] [CrossRef]
- Merks, P.; Religioni, U.; Bilmin, K.; Lewicki, J.; Jakubowska, M.; Waksmundzka-Walczuk, M.; Czerw, A.; Barańska, A.; Bogusz, J.; Plagens-Rotman, K.; et al. Readiness and Willingness to Provide Immunization Services After Pilot Vaccination Training: A Survey Among Community Pharmacists Trained and Not Trained in Immunization During the COVID-19 Pandemic in Poland. Int. J. Environ. Res. Public Health 2021, 18, 599. [Google Scholar] [CrossRef] [PubMed]
- Capurso, K.A.; Powers, M.F. Barriers to Implementing a Pharmacist-Run Immunization Service, as Perceived by Pharmacists, in a Community Pharmacy Chain. J. Pharm. Technol. 2006, 22, 91–94. [Google Scholar] [CrossRef]
- MacDougallm, D.; Halperin, B.A.; Isenor, J.; MacKinnon-Cameron, D.; Li, L.; McNeil, S.A.; Langley, J.M.; Halperin, S.A. Routine immunization of adults by pharmacists: Attitudes and beliefs of the Canadian public and health care providers. Hum. Vaccines Immunother. 2016, 12, 623–631. [Google Scholar] [CrossRef]
- Edwards, N.; Corsten, E.G.; Kiberd, M.; Bowles, S.; Isenor, J.; Slayter, K.; McNeil, S. Pharmacists as immunizers: A survey of community pharmacists’ willingness to administer adult immunizations. Int. J. Clin. Pharm. 2015, 37, 292–295. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Global Health; Forum on Microbial Threats; Nicholson, A.; Minicucci, C.; Liao, J. (Eds.) Improving Access and Closing the Global Immunization Gap. In The Critical Public Health Value of Vaccines: Tackling Issues of Access and Hesitancy: Proceedings of a Workshop; National Academies Press: Washington, DC, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572615/ (accessed on 17 July 2024).
- International Pharmaceutical Federation (FIP). An Overview of Pharmacy’s Impact on Immunisation Coverage: A Global Survey. 2020. Available online: https://www.fip.org/file/4751 (accessed on 17 July 2024).
- Deslandes, R.; Evans, A.; Baker, S.; Hodson, K.; Mantzourani, E.; Price, K.; Way, C.; Hughes, L. Community pharmacists at the heart of public health: A longitudinal evaluation of the community pharmacy influenza vaccination service. Res. Soc. Adm. Pharm. 2020, 16, 497–502. [Google Scholar] [CrossRef]
- Lum, Z.K.; Nguyen, A.D.; Szeto, J.; Goode, J.K.R.; Han, Z.; Lee, J.Y. Spinning the globe from west to east: A mixed-method study to examine the impact of pharmacists on immunization advocacy and delivery in Asia Pacific. J. Am. Pharm. Assoc. 2021, 61, 605–613. [Google Scholar] [CrossRef]




| Characteristics | All Pharmacists N = 283 N (%) | Hospital Pharmacists (HPs) N = 180 N (%) | Community Pharmacists (CPs) N = 75 N (%) | Polyclinic Pharmacists (PPs) N = 28 N (%) |
|---|---|---|---|---|
| Gender | ||||
| Male | 84 (29.7%) | 54 (30.0%) | 24 (32.0%) | 6 (21.4%) |
| Female | 199 (70.3%) | 126 (70.0%) | 51 (68.0%) | 22 (78.6%) |
| Age | ||||
| 20–29 | 143 (50.5%) | 93 (51.6%) | 35 (46.7%) | 15 (53.6%) |
| 30–39 | 110 (38.9%) | 72 (40.0%) | 27 (36.0%) | 11 (39.3%) |
| 40–49 | 22 (7.8%) | 12 (6.7%) | 8 (10.7%) | 2 (7.1%) |
| 50–59 | 6 (2.1%) | 2 (1.1%) | 4 (5.3%) | 0 (0.0%) |
| ≥60 | 2 (0.7%) | 1 (0.6%) | 1 (1.3%) | 0 (0.0%) |
| Race | ||||
| Chinese | 270 (95.4%) | 175 (97.2%) | 68 (90.6%) | 27 (96.4%) |
| Malay | 3 (1.1%) | 1 (0.6%) | 2 (2.7%) | 0 (0.0%) |
| Indian | 7 (2.5%) | 4 (2.2%) | 2 (2.7%) | 1 (3.6%) |
| Others: 2 Vietnamese, 1 Filipino | 3 (1.1%) | 0 (0.0%) | 3 (4.0%) | 0 (0.0%) |
| Number of vaccinations received (out of 5) | ||||
| Received 0 | 2 (0.7%) | 1 (0.6%) | 1 (1.3%) | 0 (0.0%) |
| Received 1 | 7 (2.5%) | 3 (1.6%) | 4 (5.3%) | 0 (0.0%) |
| Received 2 | 18 (6.4%) | 12 (6.7%) | 6 (8.0%) | 0 (0.0%) |
| Received 3 | 40 (14.1%) | 18 (10.0%) | 21 (28.0%) | 1 (3.6%) |
| Received 4 | 102 (36.0%) | 66 (36.7%) | 26 (34.7%) | 10 (35.7%) |
| Received 5 | 114 (40.3%) | 80 (44.4%) | 17 (22.7%) | 17 (60.7%) |
| Vaccinations received | ||||
| Measles–Mumps– Rubella (MMR) | 256 (90.5%) | 161 (89.4%) | 67 (89.3%) | 28 (100.0%) |
| Hepatitis B | 252 (89.0%) | 161 (89.4%) | 64 (85.3%) | 27 (96.4%) |
| Tetanus, Diphtheria, & Acellular Pertussis (TdAP) | 245 (86.6%) | 157 (87.2%) | 61 (81.3%) | 27 (96.4%) |
| Influenza | 244 (86.2%) | 171 (95.0%) | 46 (61.3%) | 27 (96.4%) |
| Varicella | 144 (50.9%) | 95 (52.8%) | 30 (40.0%) | 19 (67.9%) |
| Qualifications | ||||
| Bachelor of Science/Pharmacy | 223 (78.8%) | 138 (76.7%) | 62 (82.7%) | 23 (82.1%) |
| Master’s | 45 (15.9%) | 28 (15.5%) | 13 (17.3%) | 4 (14.3%) |
| PharmD | 15 (5.3%) | 14 (7.8%) | 0 (0.0%) | 1 (3.6%) |
| Status of Practising Certificate | ||||
| Pre-registration/conditional registration | 21 (7.4%) | 19 (10.6%) | 1 (1.3%) | 1 (3.6%) |
| Active status | 262 (92.6%) | 161 (89.4%) | 74 (98.7%) | 27 (96.4%) |
| Practice Setting | ||||
| Hospital | 180 (63.6%) | - | - | - |
| Community pharmacy | 75 (26.5%) | - | - | - |
| Polyclinic | 28 (9.9%) | - | - | - |
| Running any specialised clinics? * | ||||
| Yes | 62 (23.1%) | 22.8 (23.8%) | 4 (5.9%) | 17 (60.7%) |
| No | 206 (76.9%) | 72.8 (76.2%) | 64 (94.1%) | 11 (39.3%) |
| Number of years in practice | ||||
| <1 year | 40 (14.1%) | 31 (17.2%) | 5 (6.7%) | 4 (14.3%) |
| 1–5 years | 110 (38.9%) | 63 (35.0%) | 36 (48.0%) | 11 (39.3%) |
| 6–10 years | 79 (27.9%) | 53 (29.4%) | 18 (24.0%) | 8 (28.5%) |
| >10 years | 54 (19.1%) | 33 (18.4%) | 16 (21.3%) | 5 (17.9%) |
| Participation in educational programme | ||||
| Yes | 38 (13.4%) | 17 (9.4%) | 15 (20.0%) | 6 (21.4%) |
| No | 245 (86.6%) | 163 (90.6%) | 60 (80.0%) | 22 (78.6%) |
| Number of Responses | Quotes | |
|---|---|---|
| List of themes for pharmacists who are willing to serve as vaccine advocates | ||
| Pharmacists have the capacity to provide the vaccination service if trained - pharmacist-led vaccination services have been implemented overseas | 17 | “If we are capable of screening, we should be able to administer too. Pharmacists in other countries are trained to administer vaccine.” “As a(n) active team member of collaborative practice with Doctors, Pharmacists should be given the opportunity to learn how to administer vaccines.” |
| Beneficial to patients - convenience, shortened waiting time, providing one-stop vaccination services (counsel, recommend, administer) | 13 | “Avoid unnecessary visit to clinics which can free up slots for other patients.” “It minimizes the number of touch points for patient hence improving care and efficiency.” |
| List of themes for pharmacists who are unwilling to serve as vaccine advocates | ||
| There are other healthcare professionals available to provide the service - structure of healthcare system | 25 | “No need to take on this role in the hospital setting when we have nurses able to do it. Even the doctors are not administering them.” “I think it is a good opportunity to learn something new, but I cannot see this service being time-efficient for pharmacist at the current moment (due to strong competition with other HCP for such service).” |
| Lack confidence and familiarity with handling injections | 20 | “Would need skills and practice before I am comfortable in doing it” “Not confident to do so due to lack of training and experience” |
| Lack of training and competency | 15 | “Lack of training. No competency in administration.” “Not trained in injection techniques” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Au, A.L.; Chia, D.M.; Ong, P.-S. Vaccination Knowledge, Attitudes, Perceptions, and Educational Needs of Pharmacists in Singapore: A Cross-Sectional Study. Vaccines 2024, 12, 1219. https://doi.org/10.3390/vaccines12111219
Au AL, Chia DM, Ong P-S. Vaccination Knowledge, Attitudes, Perceptions, and Educational Needs of Pharmacists in Singapore: A Cross-Sectional Study. Vaccines. 2024; 12(11):1219. https://doi.org/10.3390/vaccines12111219
Chicago/Turabian StyleAu, Ally L., Deborah M. Chia, and Pei-Shi Ong. 2024. "Vaccination Knowledge, Attitudes, Perceptions, and Educational Needs of Pharmacists in Singapore: A Cross-Sectional Study" Vaccines 12, no. 11: 1219. https://doi.org/10.3390/vaccines12111219
APA StyleAu, A. L., Chia, D. M., & Ong, P.-S. (2024). Vaccination Knowledge, Attitudes, Perceptions, and Educational Needs of Pharmacists in Singapore: A Cross-Sectional Study. Vaccines, 12(11), 1219. https://doi.org/10.3390/vaccines12111219