

Perceptions of COVID-19 Vaccines: Protective Shields or Threatening Risks? A Descriptive Exploratory Study among the Italian Population


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measurements
2.3. Statistical Analyses
3. Results
3.1. Prevalence of Themes in the Total Sample
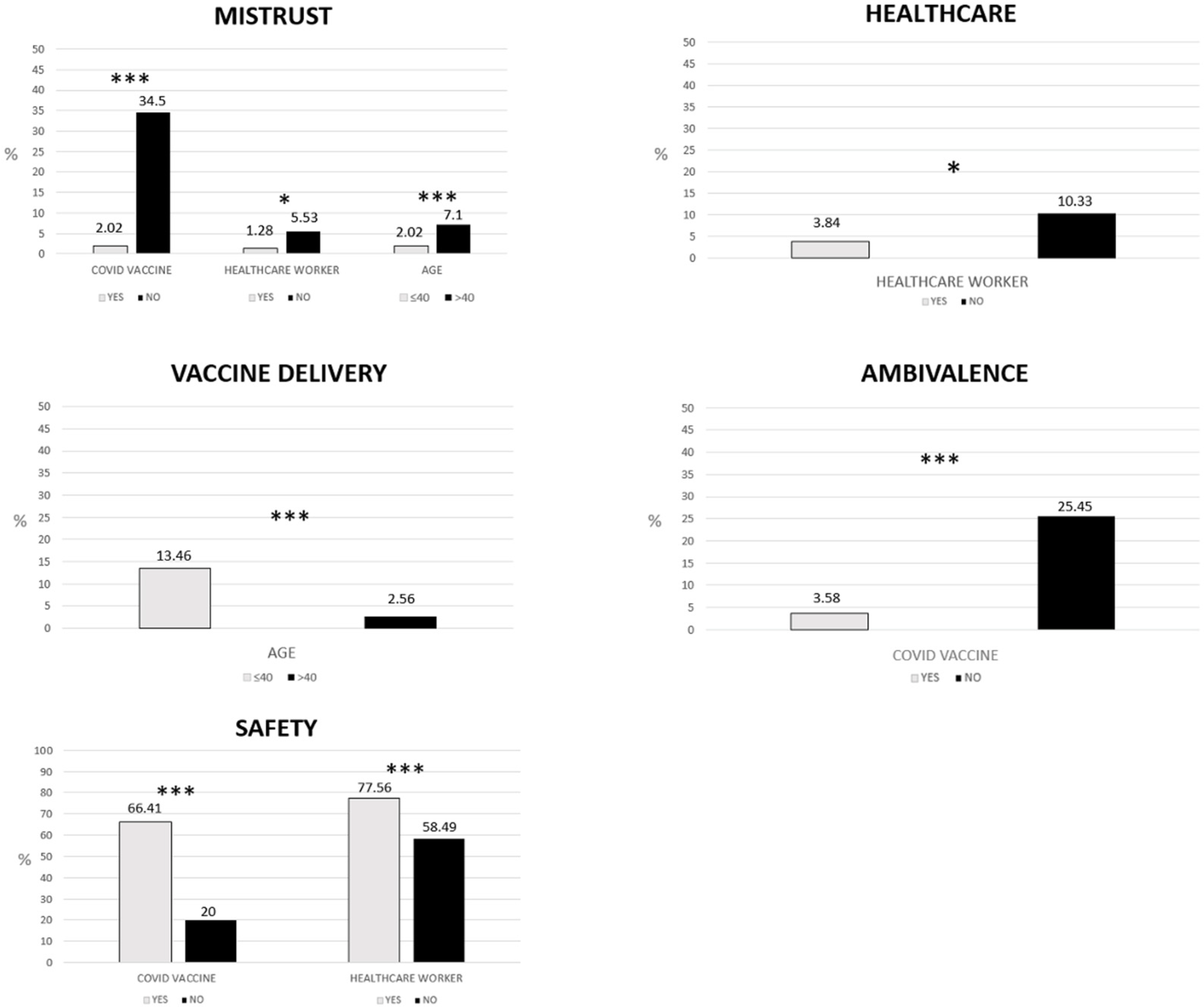
3.2. Differences in the Prevalence of Themes between COVID-19-Vaccinated and Unvaccinated Individuals
3.3. Differences in the Prevalence of Themes between Healthcare Workers and Non-Healthcare Workers
3.4. Differences in the Prevalence of Themes between Individuals Aged 40 or Younger and Individuals Aged over 40
3.5. Perception of Risk and Attitudes towards Vaccination: Differences between Vaccinated against COVID-19 and Unvaccinated Individuals
3.5.1. Answers to the Question ‘Why Do you Think Getting Vaccinated May Be Risky?’
3.5.2. Answers to the Question ‘Which of the following Variables Do You Think Impact More on Your Attitudes toward Vaccination?’
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Facciolà, A.; Visalli, G.; Orlando, A.; Bertuccio, M.P.; Spataro, P.; Squeri, R.; Picerno, I.; Pietro, A.D. Vaccine hesitancy: An overview on parents’ opinions about vaccination and possible reasons of vaccine refusal. J. Public Health Res. 2019, 8, 1436. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Qiao, J.; Ming, W.-K.; Wu, Y. Megastudies: A New Approach to Reducing Vaccine Hesitation Worldwide. Vaccines 2023, 11, 133. [Google Scholar] [CrossRef] [PubMed]
- Jee, Y. WHO international health regulations emergency committee for the COVID-19 outbreak. Epidemiol. Health 2020, 42, e2020013. [Google Scholar] [CrossRef] [PubMed]
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 vaccination program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Le, T.T.; Andreadakis, Z.; Kumar, A.; Román, R.G.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine developmentlandscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Roshchina, Y.; Roshchin, S.; Rozhkova, K. Determinants of COVID-19 Vaccine Hesitancy and Resistance In Russia. SSRN Electron. J. 2021, 40, 5739–5747. [Google Scholar] [CrossRef]
- World Health Organization. Ten-Threats-to-Global-Health-in-2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 16 October 2022).
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy–A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccines 2015, 14, 4161–4164. [Google Scholar] [CrossRef]
- Bankamp, B.; Hickman, C.; Icenogle, J.P.; Rota, P.A. Successes and challenges for preventing measles, mumps and rubella by vaccination. Curr. Opin. Virol. 2019, 34, 110–116. [Google Scholar] [CrossRef]
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The state of vaccine confidence 2016: Global insights through a 67-country survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef]
- Reintjes, R.; Das, E.; Klemm, C.; Richardus, J.H.; Keßler, V.; Ahmad, A. “Pandemic public health paradox”: Time series analysis of the 2009/10 influenza A/H1N1 epidemiology, media attention, risk perception and public reactions in 5 European countries. PLoS ONE 2016, 11, e0151258. [Google Scholar] [CrossRef]
- Fu, C.; Wei, Z.; Pei, S.; Li, S.; Sun, X.; Liu, P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). MedRxiv 2020, 2020, 2020-04. [Google Scholar] [CrossRef]
- Khan, Y.H.; Mallhi, T.H.; Alotaibi, N.H.; Alzarea, A.I.; Alanazi, A.S.; Tanveer, N.; Hashmi, F.K. Threat of COVID-19 vaccine hesitancy in Pakistan: The need for measures to neutralize misleading narratives. Am. J. Trop. Med. Hyg. 2020, 103, 603–604. [Google Scholar] [CrossRef]
- Boragno, P.; Fiabane, E.; Colledani, D.; Dalla Gasperina, D.; Setti, I.; Sommovigo, V.; Gabanelli, P. Attitude towards Intranasal Vaccines and Psychological Determinants: Effects on the General Population in Northern Italy. Vaccines 2023, 11, 138. [Google Scholar] [CrossRef]
- Fadda, M.; Suggs, L.S.; Albanese, E. Willingness to vaccinate against COVID-19: A qualitative study involving older adults from Southern Switzerland. Vaccine 2021, 8, 100108. [Google Scholar] [CrossRef]
- Perrone, C.; Fiabane, E.; Maffoni, M.; Pierobon, A.; Setti, I.; Sommovigo, V.; Gabanelli, P. Vaccination hesitancy: To be vaccinated, or not to be vaccinated, that is the question in the era of COVID-19. Public Health Nurs. 2022, 40, 90–96. [Google Scholar] [CrossRef]
- Finney Rutten, L.J.; Zhu, X.; Leppin, A.L.; Ridgeway, J.L.; Swift, M.D.; Griffin, J.M.; Sauver, J.L.S.; Virk, A.; Jacobson, R.M. Evidence-based strategies for clinical organizations to address COVID-19 vaccine hesitancy. Mayo Clin. Proc. 2021, 96, 699–707. [Google Scholar] [CrossRef]
- Bagić, D.; Šuljok, A.; Ančić, B. Determinants and reasons for coronavirus disease 2019 vaccine hesitancy in Croatia. Croat. Med. J. 2022, 28, 89–97. [Google Scholar] [CrossRef]
- Benham, J.L.; Atabati, O.; Oxoby, R.J.; Mourali, M.; Shaffer, B.; Sheikh, H.; Boucher, J.-C.; Constantinescu, C.; Leigh, J.P.; Ivers, N.M.; et al. COVID-19 vaccine-related attitudes and beliefs in Canada: National cross-sectional survey and cluster analysis. JMIR Public Health Surveill. 2021, 7, e30424. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Paoli, S.; Lorini, C.; Puggelli, F.; Sala, A.; Grazzini, M.; Paolini, D.; Bonanni, B.; Bonaccorsi, G. Assessing vaccine hesitancy among healthcare workers: A cross-sectional study at an Italian pediatric hospital and the development of a healthcare worker’s vaccination compliance index. Vaccines 2019, 7, 201. [Google Scholar] [CrossRef] [PubMed]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Wake, A.D. The willingness to receive COVID-19 vaccine and its associated factors: “Vaccination Refusal Could Prolong the War of This Pandemic”-a systematic review. Risk Manag. Health Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Asma, S.; Akan, H.; Uysal, Y.; Poçan, A.G.; Sucakli, M.H.; Yengil, E.; Gereklioğlu, Ç.; Korur, A.; Başhan, I.; Erdogan, A.F.; et al. Factors effecting influenza vaccination uptake among health care workers: A multi-center cross-sectional study. BMC Infect. Dis. 2016, 16, 192. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]
- Joffe, H. Thematic analysis. In Qualitative Research Methods in Mental Health and Psychotherapy: A Guide for Students and Practitioners; John Wiley & Sons: Hoboken, NJ, USA, 2011; pp. 209–223. [Google Scholar]
- Giuliani, M.; Ichino, A.; Bonomi, A.; Martoni, R.; Cammino, S.; Gorini, A. Who Is Willing to Get Vaccinated? A Study into the Psychological, Socio-Demographic, and Cultural Determinants of COVID-19 Vaccination Intentions. Vaccines 2021, 9, 810. [Google Scholar] [CrossRef]
- Wang, J.; Ji, Q.; Dong, S.; Zhao, S.; Li, X.; Zhu, Q.; Long, S.; Zhang, J.; Jin, H. Factors Influencing Vaccine Hesitancy in China: A Qualitative Study. Vaccines 2021, 9, 1291. [Google Scholar] [CrossRef]
- Bond, L.; Nolan, T.; Pattison, P.; Carlin, J. Vaccine preventable diseases and immunisations: A qualitative study of mothers? Perceptions of severity, susceptibility, benefits and barriers. Aust. N. Z. J. Public Health 1998, 22, 441–446. [Google Scholar] [CrossRef]
- Marzo, R.R.; Shrestha, R.; Sapkota, B.; Acharya, S.; Shrestha, N.; Pokharel, M.; Ahmad, A.; Patalinghug, M.E.; Rahman, F.; Su, T.T.; et al. Perception towards vaccine effectiveness in controlling COVID-19 spread in rural and urban communities: A global survey. Front. Public Health 2022, 10, 3103. [Google Scholar] [CrossRef]
- Fieselmann, J.; Annac, K.; Erdsiek, F.; Yilmaz-Aslan, Y.; Brzoska, P. What are the reasons for refusing a COVID-19 vaccine? A qualitative analysis of social media in Germany. BMC Public Health 2022, 22, 846. [Google Scholar] [CrossRef]
- Barattucci, M.; Pagliaro, S.; Ballone, C.; Teresi, M.; Consoli, C.; Garofalo, A.; De Giorgio, A.; Ramaci, T. Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB). Vaccines 2022, 10, 1099. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Stacchini, L.; Stancanelli, E.; Guida, A.; Radi, A.; Morittu, C.; Zimmitti, S.; Alderotti, G.; Del Riccio, M.; et al. Determinants of Actual COVID-19 Vaccine Uptake in a Cohort of Essential Workers: An Area-Based Longitudinal Study in the Province of Prato, Italy. Int. J. Environ. Res. Public Health 2022, 19, 13216. [Google Scholar] [CrossRef]
- Burke, P.F.; Masters, D.; Massey, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef]
- Ledda, C.; Costantino, C.; Cuccia, M.; Maltezou, H.C.; Rapisarda, V. Attitudes of Healthcare Personnel towards Vaccinations before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2703. [Google Scholar] [CrossRef]
- Brannon, S.M.; Gawronski, B. Cognitive consistency in social cognition. In The Oxford Encyclopedia of Social Psychology; Hogg, M., Ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Harmon-Jones, E.; Mills, J. An introduction to cognitive dissonance theory and an overview of current perspectives on the theory. In Cognitive Dissonance: Reexamining a Pivotal Theory in Psychology, 2nd ed.; Harmon-Jones, E., Ed.; American Psychological Association: Washington, DC, USA, 2019; pp. 3–24. [Google Scholar]
- Cristea, D.; Ilie, D.-G.; Constantinescu, C.; Fîrțală, V. Acceptance, Hesitancy, and Refusal in Anti-COVID-19 Vaccination: A Cluster Analysis Aiming at the Typology behind These Three Concepts. Vaccines 2022, 10, 1496. [Google Scholar] [CrossRef]
- Yurttas, B.; Poyraz, B.C.; Sut, N.; Ozdede, A.; Oztas, M.; Uğurlu, S.; Tabak, F.; Hamuryudan, V.; Seyahi, E. Willingness to get the COVID-19 vaccine among patients with rheumatic diseases, healthcare workers and general population in Turkey: A web-based survey. Rheumatol. Int. 2021, 41, 1105–1114. [Google Scholar] [CrossRef]
- Rios-Fetchko, F.; Carson, M.; Gonzalez Ramirez, M.; Butler, J.Z.; Vargas, R.; Cabrera, A.; Gallegos-Castillo, A.; LeSarre, M.; Liao, M.; Fernandez, A.; et al. COVID-19 Vaccination Perceptions among Young Adults of Color in the San Francisco Bay Area. Health Equity 2022, 6, 836–844. [Google Scholar] [CrossRef]
- Davis, T.C.; Fredrickson, D.D.; Arnold, C.L.; Cross, J.T.; Humiston, S.G.; Green, K.W.; Bocchini, J.A., Jr. Childhood vaccine risk/benefit communication in private practice office settings: A national survey. Pediatrics 2001, 107, E17. [Google Scholar] [CrossRef] [PubMed]
- Gust, D.A.; Woodruff, R.; Kennedy, A.; Brown, C.; Sheedy, K.; Hibbs, B. Parental perceptions surrounding risks and benefits of immunization. Semin. Pediatr. Infect. Dis. 2003, 14, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Hidayana, I.; Amir, S.; Pelupessy, D.C.; Rahvenia, Z. Using a health belief model to assess COVID-19 vaccine intention and hesitancy in Jakarta, Indonesia. PLoS Glob. Public Health 2022, 2, e0000934. [Google Scholar] [CrossRef]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Hyland, P.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Wynen, J.; Op de Beeck, S.; Verhoest, K.; Glavina, M.; Six, F.; Van Damme, P.; Beutels, P.; Hendrickx, G.; Pepermans, K. Taking a COVID-19 vaccine or not? Do trust in government and trust in experts help us to understand vaccination intention? Adm. Soc. 2022, 54, 1875–1901. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]


{kind=link}
| Items | Response |
|---|---|
| Socio-Demographic Data | |
| Age | (Number) |
| Gender |
|
| Do you work as a healthcare professional? |
|
| Perception of Vaccines | |
| (a) Which image/word/phrase does come to mind when you think of vaccines? | (Free answer) |
| (b) Why do you think getting vaccinated may be risky? You can select more than one option. |
|
| (c) Which of the following variables do you think impact more on your attitudes toward vaccination? You can select more than one option. |
|
| (d) I have had COVID-19 vaccine. |
|
| Themes | n (%) | Examples |
|---|---|---|
| Safety | 439 (62.7) | ‘Salvation’; ‘Protective Shield’; ‘Needs’ |
| Healthcare | 62 (8.9) | ‘COVID’; ‘Virus’; ‘Doctor’ |
| Vaccine Delivery | 55 (7.9) | ‘Injection’; ‘Syringe’; ‘Needle’ |
| Progress | 42 (6) | ‘Evolution’; ‘Scientific Research’; ‘Future’ |
| Ambivalence | 37 (5.3) | ‘Uncertainty’; ‘Some safe others not’; ‘Fear’ |
| Mistrust | 32 (4.6) | ‘Obligation in the form of blackmail’; ‘Fraud, censorship, truth-hiding and drugs for the healthy’; ‘Gene therapy and genotoxicity’. |
| Ethics | 22 (3.1) | ‘An act of responsibility’; ‘I vaccinate myself to help others’; ’Civic sense’ |
| Unclassifiable | 11 (1.6) | ‘Cow’s milk’; ‘To cows’; ‘Daje’ |
| Vaccinated against COVID-19 | Unvaccinated against COVID-19 | χ2 | p | |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Risk perceptions | ||||
| No risk | 317 (49.15) | 2 (3.64) | 40.50 | <0.001 |
| Negative experience of relatives and/or friends | 55 (8.53) | 26 (47.27) | 70.61 | <0.001 |
| Negative experiences reported by acquaintances | 80 (12.40) | 14 (25.45) | 6.35 | <0.05 |
| Medical opinions | 104 (16.12) | 21 (38.18) | 15.34 | <0.001 |
| Scientific journals | 107 (16.59) | 29 (52.73) | 40.00 | <0.001 |
| Attitudes | ||||
| Vaccine type | 200 (31.01) | 42 (76.36) | 44.11 | <0.001 |
| Trust in pharmaceutical companies | 100 (5.12) | 1 (1.82) | 6.62 | <0.05 |
| Distrust of pharmaceutical companies | 70 (15.52) | 1 (1.82) | 164.77 | <0.001 |
| Trust in healthcare worker and doctors | 258 (40) | 2 (3.64) | 27.17 | <0.001 |
| Mass media, newspapers, magazines | 39 (6.05) | 12 (21.82) | 16.40 | <0.001 |
| Distrust of scientific research | 21 (3.26) | 12 (21.82) | 34.85 | <0.001 |
| Trust in scientific research | 547 (84.81) | 9 (16.36) | 141.13 | <0.001 |
| Distrust of health workers and doctors | 18 (2.79) | 21 (38.18) | 114.02 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boragno, P.; Fiabane, E.; Taino, I.; Maffoni, M.; Sommovigo, V.; Setti, I.; Gabanelli, P. Perceptions of COVID-19 Vaccines: Protective Shields or Threatening Risks? A Descriptive Exploratory Study among the Italian Population. Vaccines 2023, 11, 642. https://doi.org/10.3390/vaccines11030642
Boragno P, Fiabane E, Taino I, Maffoni M, Sommovigo V, Setti I, Gabanelli P. Perceptions of COVID-19 Vaccines: Protective Shields or Threatening Risks? A Descriptive Exploratory Study among the Italian Population. Vaccines. 2023; 11(3):642. https://doi.org/10.3390/vaccines11030642
Chicago/Turabian StyleBoragno, Paola, Elena Fiabane, Irene Taino, Marina Maffoni, Valentina Sommovigo, Ilaria Setti, and Paola Gabanelli. 2023. "Perceptions of COVID-19 Vaccines: Protective Shields or Threatening Risks? A Descriptive Exploratory Study among the Italian Population" Vaccines 11, no. 3: 642. https://doi.org/10.3390/vaccines11030642
APA StyleBoragno, P., Fiabane, E., Taino, I., Maffoni, M., Sommovigo, V., Setti, I., & Gabanelli, P. (2023). Perceptions of COVID-19 Vaccines: Protective Shields or Threatening Risks? A Descriptive Exploratory Study among the Italian Population. Vaccines, 11(3), 642. https://doi.org/10.3390/vaccines11030642