
Association of Oxidative-Stress-Related Gene Polymorphisms with Pain-Related Temporomandibular Disorders and Oral Behavioural Habits

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Diagnosis of Temporomandibular Disorders—Clinical Examination
2.2. Assessment of Psychosocial and Psychosomatic Characteristics
2.3. Assessment of Oral Behavioural Habits
2.4. Participant Groups
2.5. Extraction of DNA and Genotyping
2.6. Selection of SNPs
2.7. Statistical Analysis
3. Results
Characteristics of Participants
4. Participants’ Genotype
5. Psychological and Psychosomatic Traits with Respect to a Specific Genotype
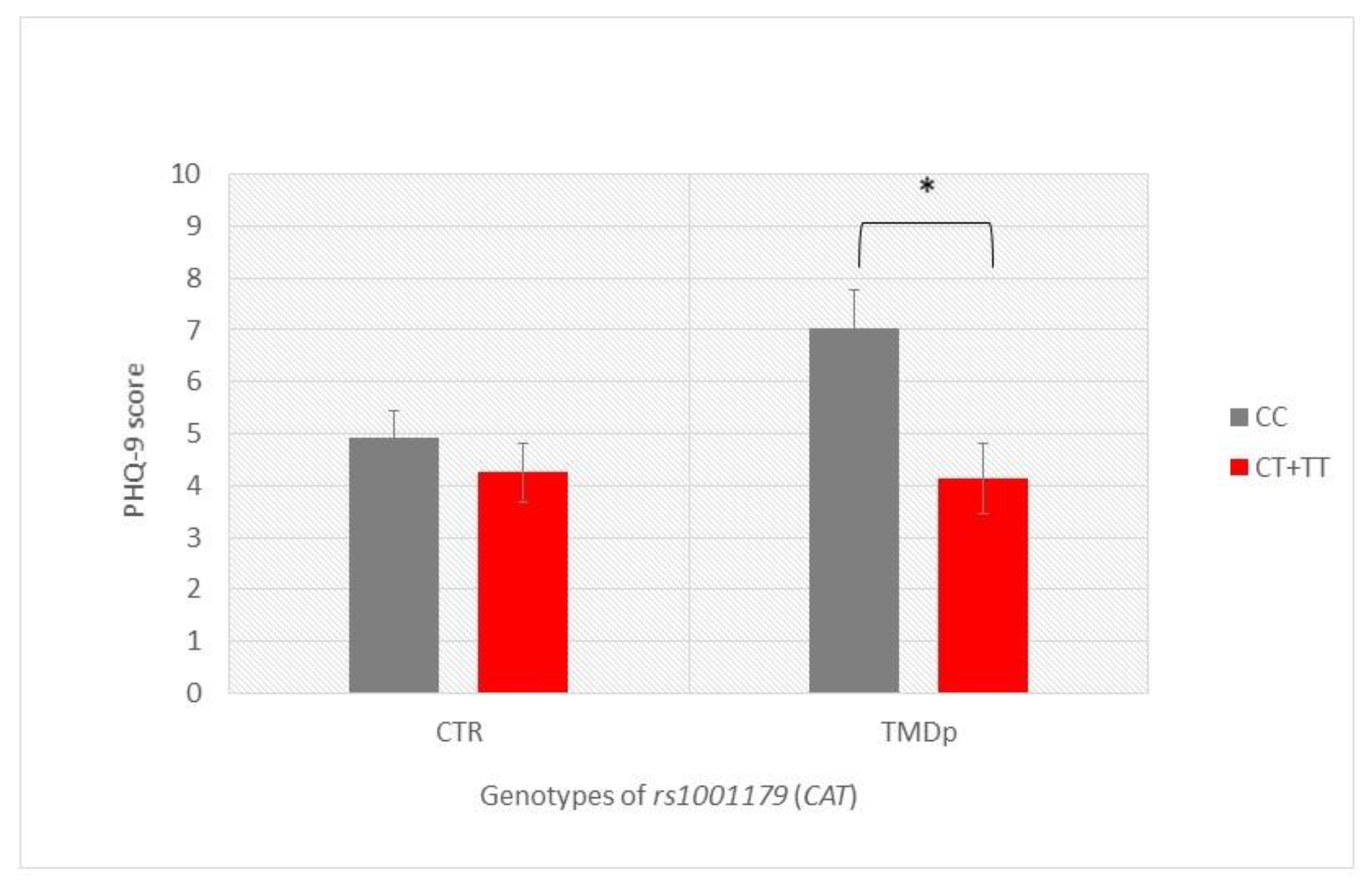
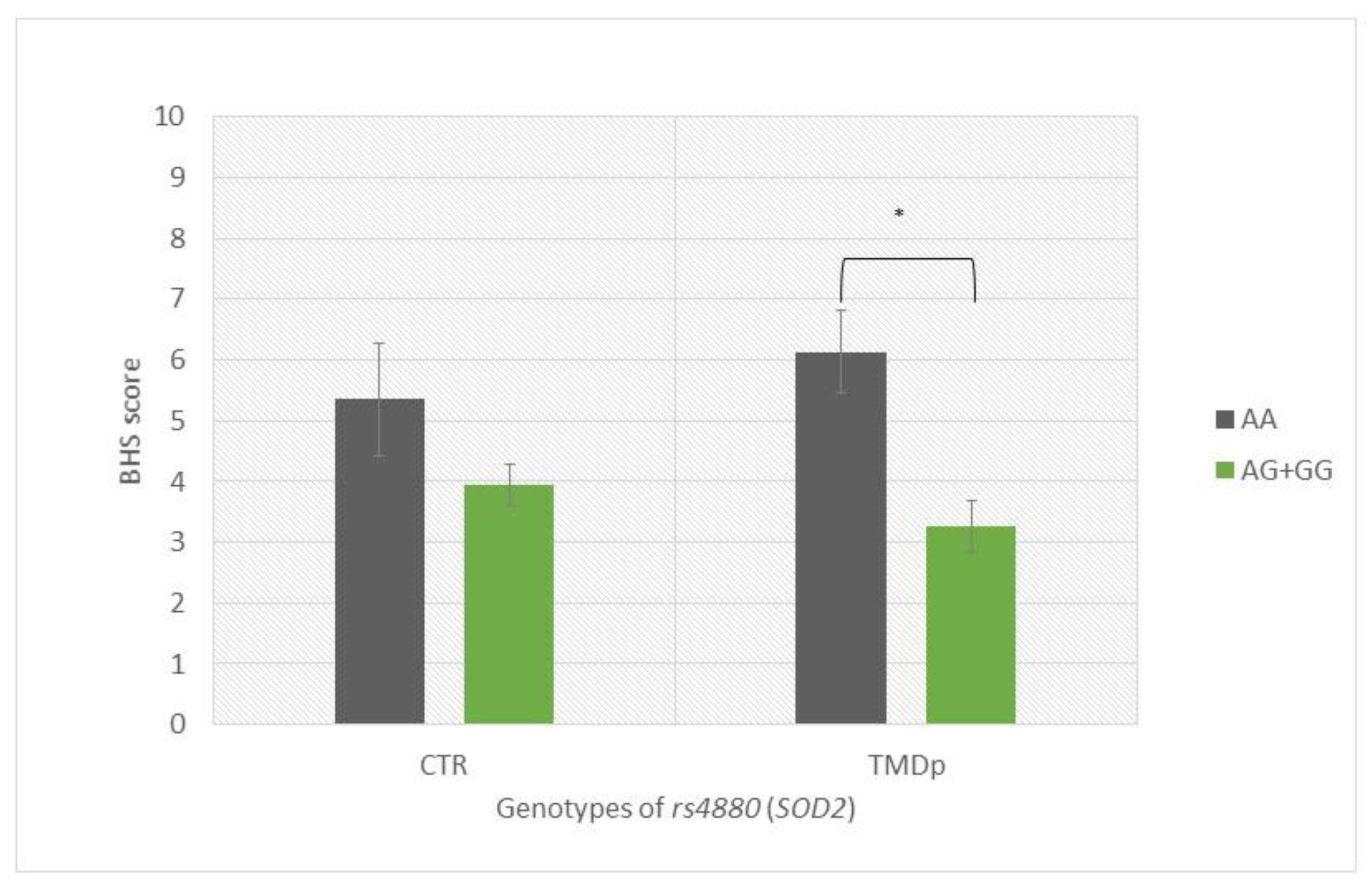
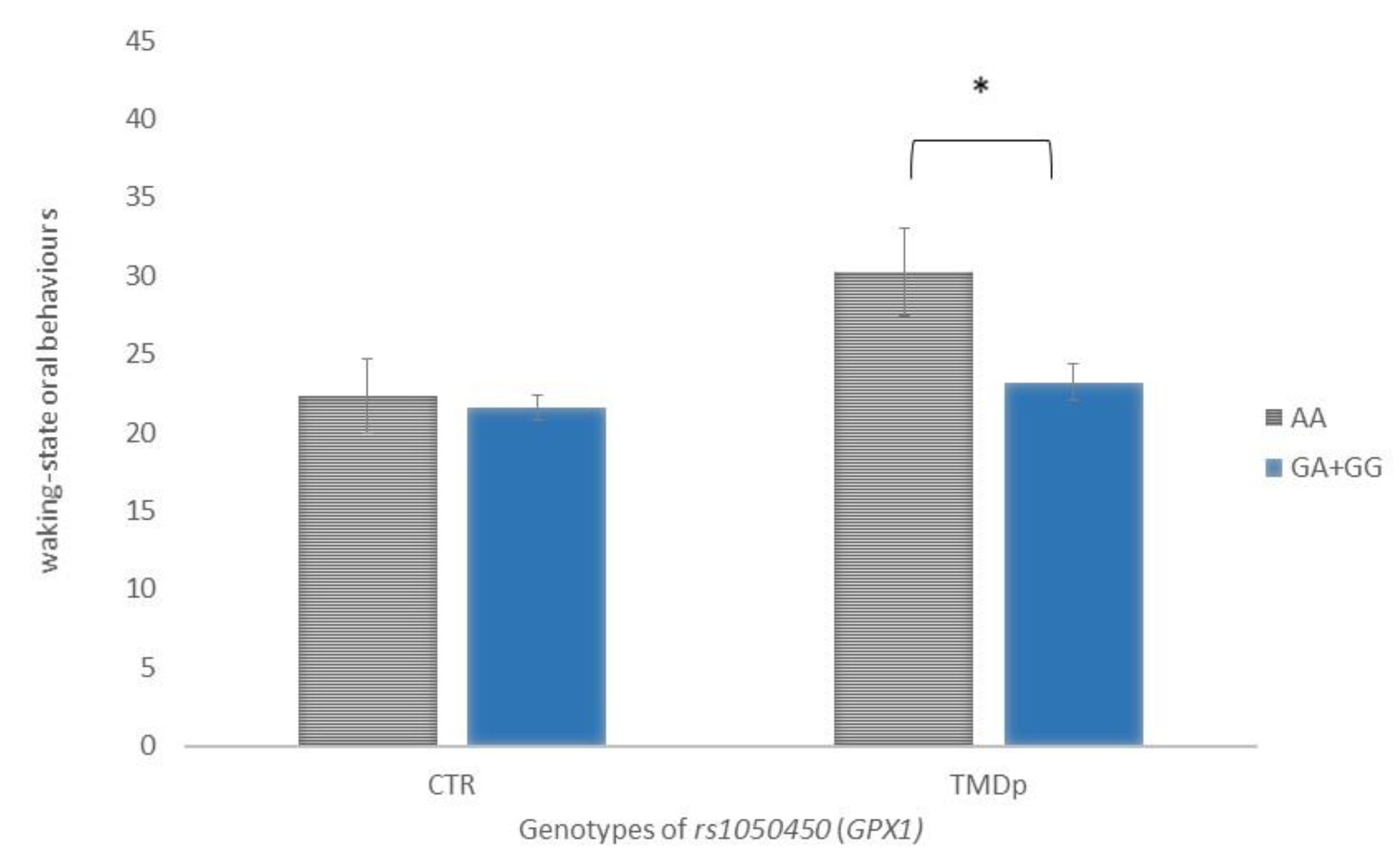
5.1. Analysis with Respect to the Presence of Pain (TMDp/CTR)
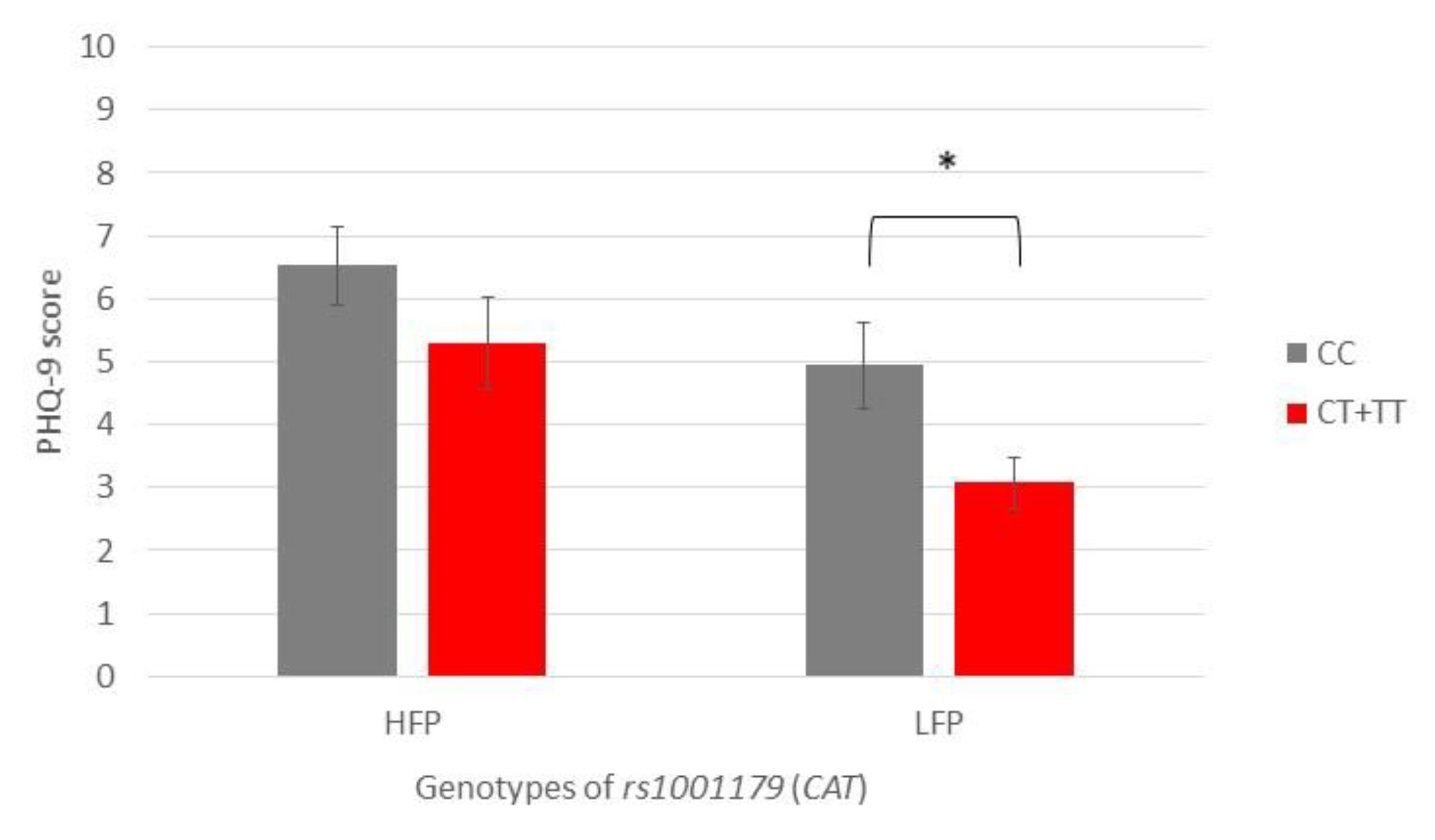
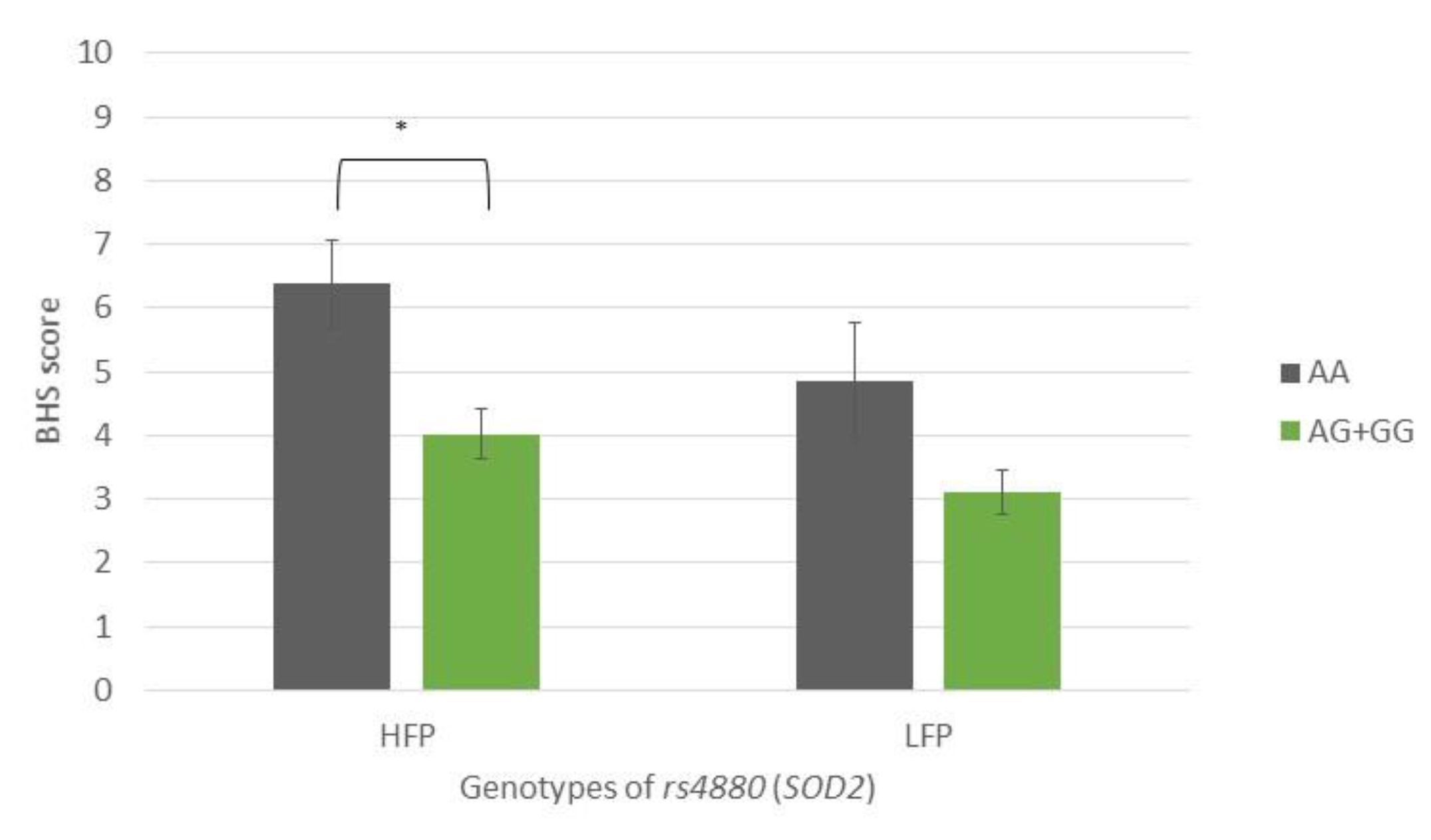
5.2. Analysis with Respect to Oral Behaviour Frequency (HFP/LFP)
6. Risk Factors Associated with Pain-Related TMD
7. Risk Factors Associated with Oral Behaviour Frequency
7.1. Risk Factors Associated with Waking-State Oral Behaviours
7.2. Risk Factors Associated with Sleep-Related Oral Behaviours
8. Discussion
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Maixner, W.; Diatchenko, L.; Dubner, R.; Fillingim, R.B.; Greenspan, J.D.; Knott, C.; Ohrbach, R.; Weir, B.; Slade, G.D. Orofacial pain prospective evaluation and risk assessment study—The OPPERA study. J. Pain 2011, 12, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Bair, E.; Greenspan, J.D.; Dubner, R.; Fillingim, R.B.; Diatchenko, L.; Maixner, W.; Knott, C.; Ohrbach, R. Signs and symptoms of first onset TMD and sociodemographic predictors of its development: The OPPERA prospective cohort study. J. Pain 2013, 14, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Adèrn, B.; Stenvinkel, C.; Sahlqvist, L.; Tegelberg, Å. Prevalence of temporomandibular dysfunction and pain in adult general practice patients. Acta Odontol. Scand. 2014, 72, 585–590. [Google Scholar] [CrossRef]
- Ferrillo, M.; Giudice, A.; Marotta, N.; Fortunato, F.; Di Venere, D.; Ammendolia, A.; Fiore, P.; de Sire, A. Pain Management and Rehabilitation for Central Sensitization in Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 12164. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. International RDC/TMD Consortium Network, International association for Dental Research; Orofacial Pain Special Interest Group, International Association for the Study of Pain. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network * and Orofacial Pain Special Interest Group †. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar]
- Ohrbach, R.; Michelotti, A. The Role of Stress in the Etiology of Oral Parafunction and Myofascial Pain. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 369–379. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Lobbezoo, F. Bruxism definition: Past, present, and future-What should a prosthodontist know? J. Prosthet. Dent. 2022, 128, 905–912. [Google Scholar] [CrossRef]
- Kara, M.I.; Yanık, S.; Keskinruzgar, A.; Taysi, S.; Copoglu, S.; Orkmez, M.; Nalcaci, R. Oxidative imbalance and anxiety in patients with sleep bruxism. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 604–609. [Google Scholar] [CrossRef]
- Iodice, G.; Cimino, R.; Vollaro, S.; Lobbezoo, F.; Michelotti, A. Prevalence of temporomandibular disorder pain, jaw noises and oral behaviours in an adult Italian population sample. J. Oral Rehabil. 2019, 46, 691–698. [Google Scholar] [CrossRef]
- Braz, M.A.; Freitas Portella, F.; Seehaber, K.A.; Bavaresco, C.S.; Rivaldo, E.G. Association between oxidative stress and temporomandibular joint dysfunction: A narrative review. J. Oral Rehabil. 2020, 47, 536–546. [Google Scholar] [CrossRef]
- Masahiro, I.; Shinya, A.; Nagata, S.; Miyata, M.; Hiroshi, K. Relationships between perceived workload, stress and oxidative DNA damage. Int. Arch. Occup. Environ. Health 2001, 74, 153–157. [Google Scholar]
- Soliman, M.M.; Aldhahrani, A.; Althobaiti, F.; Ahmed, M.M.; Sayed, S.; Alotaibi, S.; Shukry, M.; El-Shehawi, A.M. Characterization of the Impacts of Living at High Altitude in Taif: Oxidative Stress Biomarker Alterations and Immunohistochemical Changes. Curr. Issues Mol. Biol. 2022, 44, 1610–1625. [Google Scholar] [CrossRef]
- Crawford, A.; Fassett, R.G.; Geraghty, D.P.; Kunde, D.A.; Ball, M.J.; Robertson, I.K.; Coombes, J.S. Relationships between single nucleotide polymorphisms of antioxidant enzymes and disease. Gene 2012, 501, 89–103. [Google Scholar] [CrossRef]
- Assavarittirong, C.; Samborski, W.; Grygiel-Górniak, B. Oxidative Stress in Fibromyalgia: From Pathology to Treatment. Oxid. Med. Cell. Longev. 2022, 2022, 1582432. [Google Scholar] [CrossRef]
- Geyik, S.; Altunısık, E.; Neyal, A.M.; Taysi, S. Oxidative stress and DNA damage in patients with migraine. J. Headache Pain 2016, 17, 10. [Google Scholar] [CrossRef]
- de Almeida, C.; Amenábar, J.M. Changes in the salivary oxidative status in individuals with temporomandibular disorders and pain. J. Oral Biol. Craniofacial Res. 2016, 6, S1–S4. [Google Scholar] [CrossRef]
- Rodríguez de Sotillo, D.; Velly, A.M.; Hadley, M.; Fricton, J.R. Evidence of oxidative stress in temporomandibular disorders: A pilot study. J. Oral Rehabil. 2011, 38, 722–728. [Google Scholar] [CrossRef]
- Cai, H.X.; Luo, J.M.; Long, X.; Li, X.D.; Cheng, Y. Free-radical oxidation and superoxide dismutase activity in synovial fluid of patients with temporomandibular disorders. J. Orofac. Pain 2006, 20, 53–58. [Google Scholar]
- Vrbanović, E.; Alajbeg, I.Z.; Vuletić, L.; Lapić, I.; Rogić, D.; Andabak Rogulj, A.; Illeš, D.; Knezović Zlatarić, D.; Badel, T.; Alajbeg, I. Salivary Oxidant/Antioxidant Status in Chronic Temporomandibular Disorders Is Dependent on Source and Intensity of Pain -A Pilot Study. Front. Physiol. 2018, 9, 1405. [Google Scholar] [CrossRef]
- Bouayed, J.; Rammal, H.; Soulimani, R. Oxidative stress and anxiety: Relationship and cellular pathways. Oxid. Med. Cell. Longev. 2009, 2, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Rus, A.; Robles-Fernandez, I.; Martinez-Gonzalez, L.J.; Carmona, R.; Alvarez-Cubero, M.J. Influence of Oxidative Stress-Related Genes on Susceptibility to Fibromyalgia. Nurs. Res. 2021, 70, 44–50. [Google Scholar] [CrossRef]
- Pourvali, K.; Abbasi, M.; Mottaghi, A. Role of Superoxide Dismutase 2 Gene Ala16Val Polymorphism and Total Antioxidant Capacity in Diabetes and its Complications. Avicenna J. Med. Biotechnol. 2016, 8, 48–56. [Google Scholar] [PubMed]
- Djokic, M.; Radic, T.; Santric, V.; Dragicevic, D.; Suvakov, S.; Mihailovic, S.; Stankovic, V.; Cekerevac, M.; Simic, T.; Nikitovic, M.; et al. The Association of Polymorphisms in Genes Encoding Antioxidant Enzymes GPX1 (rs1050450), SOD2 (rs4880) and Transcriptional Factor Nrf2 (rs6721961) with the Risk and Development of Prostate Cancer. Medicina 2022, 58, 1414. [Google Scholar] [CrossRef] [PubMed]
- Little, J.; Higgins, J.P.; Ioannidis, J.P.; Moher, D.; Gagnon, F.; von Elm, E.; Khoury, M.J.; Cohen, B.; Davey-Smith, G.; Grimshaw, J.; et al. STrengthening the REporting of Genetic Association Studies (STREGA)--An extension of the STROBE statement. Genet. Epidemiol. 2009, 33, 581–598. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Ohrbach, R. Diagnostic Criteria for Temporomandibular Disorders: Assessment Instruments. Version 15 May 2016. [Dijagnostički Kriteriji za Temporomandibularne Poremećaje (DK/TMP) Instrumenti Procjene: Croatian Version 23 March 2021]; Spalj, S., Katic, V., Alajbeg, I., Celebic, A., Eds.; Universities of Rijeka: Osijek and Zagreb, Croatia; Available online: http://www.rdc-tmdinternational.org (accessed on 20 April 2023).
- Beard, C.; Hsu, K.J.; Rifkin, L.S.; Busch, A.B.; Björgvinsson, T. Validation of the PHQ-9 in a psychiatric sample. J. Affect. Disord. 2016, 193, 267–273. [Google Scholar] [CrossRef]
- Mughal, A.Y.; Devadas, J.; Ardman, E.; Levis, B.; Go, V.F.; Gaynes, B.N. A systematic review of validated screening tools for anxiety disorders and PTSD in low to middle income countries. BMC Psychiatry 2020, 20, 338. [Google Scholar] [CrossRef]
- Barsky, A.J.; Goodson, J.D.; Lane, R.S.; Cleary, P.D. The amplification of somatic symptoms. Psychosom Med. 1988, 50, 510–519. [Google Scholar] [CrossRef]
- Bernstein, R.E.; Delker, B.C.; Knight, J.A.; Freyd, J.J. Hypervigilance in college students: Associations with betrayal and dissociation and psychometric properties in a Brief Hypervigilance Scale. Psychol. Trauma 2015, 7, 448–455. [Google Scholar] [CrossRef]
- Vrbanović, E.; Zlendić, M.; Alajbeg, I.Z. Association of oral behaviours frequency with psychological profile, somatosensory amplification, presence of pain and self-reported pain intensity. Acta Odontol. Scand. 2022, 80, 522–528. [Google Scholar] [CrossRef]
- Zlendić, M.; Vrbanović, E.; Tomljanović, M.; Gall Trošelj, K.; Đerfi, K.V.; Alajbeg, I.Z. Association of oral behaviours and psychological factors with selected genotypes in pain-related TMD. Oral Dis. 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Hu, J.; Zhou, G.W.; Wang, N.; Wang, Y.J. GPX1 Pro198Leu polymorphism and breast cancer risk: A meta-analysis. Breast Cancer Res. Treat. 2010, 124, 425–431. [Google Scholar] [CrossRef]
- Palmirotta, R.; Barbanti, P.; De Marchis, M.L.; Egeo, G.; Aurilia, C.; Fofi, L.; Ialongo, C.; Valente, M.G.; Ferroni, P.; Della-Morte, D.; et al. Is SOD2 Ala16Val polymorphism associated with migraine with aura phenotype? Antioxid. Redox Signal. 2015, 22, 275–279. [Google Scholar] [CrossRef]
- Hong, E.P.; Park, J.W. Sample size and statistical power calculation in genetic association studies. Genom. Inform. 2012, 10, 117–122. [Google Scholar] [CrossRef]
- Levartovsky, S.; Msarwa, S.; Reiter, S.; Eli, I.; Winocur, E.; Sarig, R. The Association between Emotional Stress, Sleep, and Awake Bruxism among Dental Students: A Sex Comparison. J Clin Med. 2021, 11, 10. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Grychowska, N.; Wojciechowski, K.; Pelc, A.; Augustyniak, M.; Sleboda, A.; Zietek, M. Prevalence and correlation between TMD based on RDC/TMD diagnoses, oral parafunctions and psychoemotional stress in Polish university students. Biomed Res. Int. 2014, 2014, 472346. [Google Scholar] [CrossRef]
- Mirhashemi, A.; Khami, M.R.; Kharazifard, M.; Bahrami, R. The Evaluation of the Relationship Between Oral Habits Prevalence and COVID-19 Pandemic in Adults and Adolescents: A Systematic Review. Front. Public Health 2022, 10, 860185. [Google Scholar] [CrossRef]
- Winocur-Arias, O.; Winocur, E.; Shalev-Antsel, T.; Reiter, S.; Levartovsky, S.; Emodi-Perlman, A.; Friedman-Rubin, P. Painful Temporomandibular Disorders, Bruxism and Oral Parafunctions before and during the COVID-19 Pandemic Era: A Sex Comparison among Dental Patients. J. Clin. Med. 2022, 11, 589. [Google Scholar] [CrossRef]
- Alajbeg, I.Z.; Vrbanović, E.; Lapić, I.; Alajbeg, I.; Vuletić, L. Effect of occlusal splint on oxidative stress markers and psychological aspects of chronic temporomandibular pain: A randomized controlled trial. Sci. Rep. 2020, 10, 10981. [Google Scholar] [CrossRef]
- Rajaraman, P.; Hutchinson, A.; Rothman, N.; Black, P.M.; Fine, H.A.; Loeffler, J.S.; Selker, R.G.; Shapiro, W.R.; Linet, M.S.; Inskip, P.D. Oxidative response gene polymorphisms and risk of adult brain tumors. Neuro Oncol. 2008, 10, 709–715. [Google Scholar] [CrossRef]
- Galasso, M.; Dalla Pozza, E.; Chignola, R.; Gambino, S.; Cavallini, C.; Quaglia, F.M.; Lovato, O.; Dando, I.; Malpeli, G.; Krampera, M.; et al. The rs1001179 SNP and CpG methylation regulate catalase expression in chronic lymphocytic leukemia. Cell. Mol. Life Sci. 2022, 79, 521. [Google Scholar] [CrossRef] [PubMed]
- Kido, T.; Sikora-Wohlfeld, W.; Kawashima, M.; Kikuchi, S.; Kamatani, N.; Patwardhan, A.; Chen, R.; Sirota, M.; Kodama, K.; Hadley, D.; et al. Are minor alleles more likely to be risk alleles? BMC Med. Genom. 2018, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Papasavva, M.; Vikelis, M.; Siokas, V.; Katsarou, M.S.; Dermitzakis, E.V.; Raptis, A.; Kalliantasi, A.; Dardiotis, E.; Drakoulis, N. Variability in oxidative stress-related genes (SOD2, CAT, GPX1, GSTP1, NOS3, NFE2L2, and UCP2) and susceptibility to migraine clinical phenotypes and features. Front. Neurol. 2023, 13, 1054333. [Google Scholar] [CrossRef]
- Gentile, G.; Negro, A.; D’Alonzo, L.; Aimati, L.; Simmaco, M.; Martelletti, P.; Borro, M. Lack of association between oxidative stress-related gene polymorphisms and chronic migraine in an Italian population. Expert Rev. Neurother. 2015, 15, 215–225. [Google Scholar] [CrossRef] [PubMed]
- da Rocha, T.J.; Silva Alves, M.; Guisso, C.C.; de Andrade, F.M.; Camozzato, A.; de Oliveira, A.A.; Fiegenbaum, M. Association of GPX1 and GPX4 polymorphisms with episodic memory and Alzheimer’s disease. Neurosci. Lett. 2018, 666, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Teimoori, B.; Moradi-Shahrebabak, M.; Razavi, M.; Rezaei, M.; Harati-Sadegh, M.; Salimi, S. The effect of GPx-1 rs1050450 and MnSOD rs4880 polymorphisms on PE susceptibility: A case-control study. Mol. Biol. Rep. 2019, 46, 6099–6104. [Google Scholar] [CrossRef]
- Ayuso, P.; García-Martín, E.; Agúndez, J.A.G. Variability of the genes involved in the cellular redox status and their implication in drug hypersensitivity reactions. Antioxidants 2021, 10, 294. [Google Scholar] [CrossRef]
- Tang, T.S.; Prior, S.L.; Li, K.W.; Ireland, H.A.; Bain, S.C.; Hurel, S.J.; Cooper, J.A.; Humphries, S.E.; Stephens, J.W. Association between the rs1050450 glutathione peroxidase-1 (C > T) gene variant and peripheral neuropathy in two independent samples of subjects with diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 417–425. [Google Scholar] [CrossRef]
- Charniot, J.C.; Sutton, A.; Bonnefont-Rousselot, D.; Cosson, C.; Khani-Bittar, R.; Giral, P.; Charnaux, N.; Albertini, J.P. Manganese superoxide dismutase dimorphism relationship with severity and prognosis in cardiogenic shock due to dilated cardiomyopathy. Free Radic. Res. 2011, 45, 379–388. [Google Scholar] [CrossRef]
- Khawaja, S.N.; Nickel, J.C.; Iwasaki, L.R.; Crow, H.C.; Gonzalez, Y. Association between waking-state oral parafunctional behaviours and bio-psychosocial characteristics. J. Oral Rehabil. 2015, 42, 651–656. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Pain Presence | Oral Behaviours Frequency | ||||
|---|---|---|---|---|---|---|
| CTR (n = 85) | TMDp (n = 85) | LFP (n = 72) | HFP (n = 98) | |||
| Gender | Female, n (%) | 62 (72.9%) | 76 (89.4%) | 53 (73.6%) | 85 (86.7%) | |
| Male, n (%) | 23 (27.1%) | 9 (10.6%) | 19 (26.4%) | 13 (13.3%) | ||
| p b | 0.006 | 0.031 | ||||
| Age | Female | Mean (SD) | 26.15 (7.71) | 29.51 (11.01) | 29.51 (10.45) | 27.06 (9.27) |
| p a | 0.067 | 0.083 | ||||
| Male | Mean (SD) | 26.52 (7.91) | 33.78 (12.22) | 30.63 (10.96) | 25.54 (6.79) | |
| p a | 0.064 | 0.077 | ||||
| Education level | Elementary school, n (%) | / | 6 (7%) | 1 (1.4%) | 5 (5.1%) | |
| High school, n (%) | / | 24 (28%) | 15 (20.8%) | 9 (9.2%) | ||
| Student, n (%) | 58 (68%) | 23 (27%) | 31 (43.1%) | 50 (51%) | ||
| College Degree, n (%) | 20 (24%) | 25 (30%) | 18 (25%) | 27 (27.6%) | ||
| Master’s Degree, n (%) | 7 (8%) | 7 (8%) | 7 (9.7/%) | 7 (7.1%) | ||
| p b | 0.676 | 0.804 | ||||
| Somatosensory amplification (SSAS) (0–40) | Mean (SD) | 14.09 (5.07) | 14.43 (6.44) | 12.19 (5.03) | 15.79 (5.85) | |
| p a | 0.998 | <0.001 | ||||
| Anxiety symptom severity (GAD-7) (0–21) | Mean (SD) | 4.06 (3.49) | 4.65 (3.99) | 3.42 (2.77) | 5.05 (4.22) | |
| p a | 0.427 | 0.020 | ||||
| Hypervigilance (BHS) (0–20) | Mean (SD) | 4.24 (3.08) | 4.00 (3.49) | 3.47 (2.89) | 4.59 (3.48) | |
| p a | 0.362 | 0.046 | ||||
| Depression symptom severity (PHQ-9) (0–27) | Mean (SD) | 4.60 (3.59) | 5.63 (4.82) | 3.90 (3.30) | 6.01 (4.68) | |
| p a | 0.329 | 0.001 | ||||
| Variable | CTR (n = 85) | TMDp (n = 85) | |
|---|---|---|---|
| Oral Behaviours Checklist (OBC) total score (0–84) | Mean (SD) | 25.92 (7.26) | 29.05 (10.75) |
| p a | 0.161 | ||
| .Sleep-related oral behaviours (0–8) | Mean (SD) | 4.34 (1.76) | 5.21 (2.23) |
| p a | 0.007 | ||
| Waking-state oral behaviours (0–76) | Mean (SD) | 21.63 (6.85) | 24.09 (10.12) |
| p a | 0.235 | ||
| TMDp (n = 85) | CTR (n = 85) | LFP (n = 72) | HFP (n = 98) | |||||
|---|---|---|---|---|---|---|---|---|
| rs1001179 (CAT) n (%) p | TT | CT + CC | TT | CT + CC | TT | CT + CC | TT | CT + CC |
| 6 (7.1%) | 79 (92.9%) | 7 (8.2%) | 78 (91.8%) | 4 (5.6%) | 68 (94.4%) | 9 (9.2%) | 89 (90.8%) | |
| 0.773 | 0.379 | |||||||
| rs4880 (SOD2) n (%) p | GG | AG + AA | GG | AG + AA | GG | AG + AA | GG | AG + AA |
| 16 (18.8%) | 69 (81.2%) | 18 (21.2%) | 67 (78.8%) | 14 (19.4%) | 58 (80.6%) | 20 (20.4%) | 78 (79.6%) | |
| 0.701 | 0.877 | |||||||
| rs1050450 (GPX1) n (%) p | AA | GA + GG | AA | GA + GG | AA | GA + GG | AA | GA + GG |
| 11 (12.9%) | 74 (87.1%) | 6 (7.1%) | 79 (92.9%) | 3 (4.2%) | 69 (95.8%) | 14 (14.3%) | 84 (85.7%) | |
| 0.201 | 0.030 | |||||||
| rs689452 (NQO1) n (%) p | CC | CG + GG | CC | CG + GG | CC | CG + GG | CC | CG + GG |
| 0 (0%) | 85 (100%) | 0 (0%) | 85 (100%) | 0 (0%) | 72 (100%) | 0 (0%) | 98 (100%) | |
| a | a | |||||||
| TMDp (n = 85) | CTR (n = 85) | LFP (n = 72) | HFP (n = 98) | |||||
|---|---|---|---|---|---|---|---|---|
| rs1001179 (CAT) n (%) p | CC | CT + TT | CC | CT + TT | CC | CT + TT | CC | CT + TT |
| 44 (51.8%) | 41 (48.2%) | 45 (52.9%) | 40 (47.1%) | 32 (44.4%) | 40 (55.6%) | 57 (58.2%) | 41 (41.8%) | |
| 0.878 | 0.077 | |||||||
| rs4880 (SOD2) n (%) p | AA | AG + GG | AA | AG + GG | AA | AG + GG | AA | AG + GG |
| 22 (25.9%) | 63 (74.1%) | 17 (20%) | 68 (80%) | 15 (20.8%) | 57 (79.2%) | 24 (24.5%) | 74 (75.5%) | |
| 0.362 | 0.575 | |||||||
| rs1050450 (GPX1) n (%) p | GG | GA + AA | GG | GA + AA | GG | GA + AA | GG | GA + AA |
| 42 (49.4%) | 43 (50.6%) | 35 (41.2%) | 50 (58.8%) | 35 (48.6%) | 37 (51.4%) | 42 (42.9%) | 56 (57.1%) | |
| 0.281 | 0.456 | |||||||
| rs689452 (NQO1) n (%) p | GG | CG + CC | GG | CG + CC | GG | CG + CC | GG | CG + CC |
| 63 (74.1%) | 22 (25.9%) | 66 (77.6%) | 19 (22.4) | 56 (77.8%) | 16 (22.2%) | 73 (74.5%) | 25 (25.5%) | |
| 0.591 | 0.620 | |||||||
| B | SE | p | OR | 95% CI | |
|---|---|---|---|---|---|
| Sleep-related oral behaviours | 0.180 | 0.082 | 0.028 * | 1.198 | 1.020–1.406 |
| Sex (male_0; female_1) | 1.160 | 0.447 | 0.009 * | 3.190 | 1.329–7.654 |
| Age | 0.040 | 0.018 | 0.025 * | 1.041 | 1.005–1.078 |
| B | SE | β | p | |
|---|---|---|---|---|
| rs1050450 (GPX1) (Heterozygous GA + GG_0; -homozygous AA_1) | 1.370 | 0.683 | 0.142 | 0.047 * |
| PHQ-9 score | 0.724 | 0.142 | 0.356 | <0.001 * |
| Sex (male_0; female_1) | 3.934 | 1.555 | 0.177 | 0.012 * |
| Age | −0.110 | 0.063 | −0.123 | 0.083 |
| rs1050450 (GPX1) (Heterozygous GA + GG_0; -homozygous AA_1) | 1.422 | 0.696 | 0.148 | 0.043 * |
| GAD-7 score | 0.721 | 0.165 | 0.311 | <0.001 * |
| Sex (male_0; female_1) | 3.331 | 1.590 | 0.150 | 0.038 * |
| Age | −0.087 | 0.064 | −0.097 | 0.177 |
| rs1050450 (GPX1) (Heterozygous GA + GG_0; -homozygous AA_1) | 1.166 | 0.670 | 0.121 | 0.084 |
| Somatosensory amplification score | 0.604 | 0.104 | 0.402 | <0.001 * |
| Sex (male_0; female_1) | 2.858 | 1.534 | 0.129 | 0.064 |
| Age | −0.098 | 0.062 | −0.110 | 0.114 |
| rs1050450 (GPX1) (Heterozygous GA + GG_0; -homozygous AA_1) | 1.290 | 0.714 | 0.134 | 0.073 |
| Hypervigilance score | 0.619 | 0.196 | 0.234 | 0.002 * |
| Sex (male_0; female_1) | 4.076 | 1.625 | 0.184 | 0.013 * |
| Age | −0.061 | 0.067 | −0.068 | 0.362 |
| B | SE | β | p | |
|---|---|---|---|---|
| PHQ-9 score | 0.091 | 0.036 | 0.189 | 0.012 * |
| TMDp (no_0; yes_1) | 0.636 | 0.318 | 0.155 | 0.048 * |
| Sex (male_0; female_1) | 0.299 | 0.379 | 0.057 | 0.452 |
| Age | 0.025 | 0.016 | 0.117 | 0.123 |
| GAD-7 score | 0.089 | 0.041 | 0.163 | 0.030 * |
| TMDp (no_0; yes_1) | 0.681 | 0.319 | 0.167 | 0.034 * |
| Sex (male_0; female_1) | 0.214 | 0.400 | 0.041 | 0.594 |
| Age | 0.027 | 0.016 | 0.128 | 0.094 |
| Somatosensory amplification score | 0.055 | 0.027 | 0.156 | 0.040 * |
| TMDp (no_0; yes_1) | 0.728 | 0.318 | 0.178 | 0.023 * |
| Sex (male_0; female_1) | 0.171 | 0.403 | 0.033 | 0.671 |
| Age | 0.026 | 0.016 | 0.121 | 0.112 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vrbanović, E.; Zlendić, M.; Trošelj, K.G.; Tomljanović, M.; Vuković Đerfi, K.; Alajbeg, I.Z. Association of Oxidative-Stress-Related Gene Polymorphisms with Pain-Related Temporomandibular Disorders and Oral Behavioural Habits. Antioxidants 2023, 12, 1195. https://doi.org/10.3390/antiox12061195
Vrbanović E, Zlendić M, Trošelj KG, Tomljanović M, Vuković Đerfi K, Alajbeg IZ. Association of Oxidative-Stress-Related Gene Polymorphisms with Pain-Related Temporomandibular Disorders and Oral Behavioural Habits. Antioxidants. 2023; 12(6):1195. https://doi.org/10.3390/antiox12061195
Chicago/Turabian StyleVrbanović, Ema, Marko Zlendić, Koraljka Gall Trošelj, Marko Tomljanović, Kristina Vuković Đerfi, and Iva Z. Alajbeg. 2023. "Association of Oxidative-Stress-Related Gene Polymorphisms with Pain-Related Temporomandibular Disorders and Oral Behavioural Habits" Antioxidants 12, no. 6: 1195. https://doi.org/10.3390/antiox12061195
APA StyleVrbanović, E., Zlendić, M., Trošelj, K. G., Tomljanović, M., Vuković Đerfi, K., & Alajbeg, I. Z. (2023). Association of Oxidative-Stress-Related Gene Polymorphisms with Pain-Related Temporomandibular Disorders and Oral Behavioural Habits. Antioxidants, 12(6), 1195. https://doi.org/10.3390/antiox12061195