1. Introduction
Spinal cord injury (SCI) affects approximately 250,000 to 500,000 individuals every year, with violence and motor vehicular crashes (MVCs) as the main causes of this condition; however, nontraumatic etiologies are still relevant, such as neurodegenerative and malignant conditions [
1]. Recovering and assessing SCI patients is challenging, owing to the heterogeneity of etiology, severity (level lesion, partial or complete), and population affected [
2,
3]. SCI affects young adults (less than 30 years old) the most and has a strong lifetime economic impact of between
$2 and 4 billion [
4]. Current treatments focus on reducing the impact of physical and neurological disabilities with limited functional recovery in most patients [
5]. This condition not only causes physical disability but also negatively affects patients’ self-esteem, increasing the risk of psychiatric conditions, mortality rate, and the costs of health care for family members and the public system [
6,
7]. For this reason, understanding the neurophysiological mechanisms and neuroplasticity changes after SCI could help the development of more accurate neurological tests and improve the treatment options in the physical medicine and rehabilitation field.
After an injury to the central or peripheral nervous system, the brain is naturally designed to adapt by strengthening or weakening connections between certain groups of neurons. This adaptive process helps preserve functionality and maintain homeostasis within the nervous system [
8]. However, traumatic and nontraumatic injuries can affect these compensatory mechanisms by disrupting the motor and somatosensory systems [
9]. SCI triggers inflammatory responses, including apoptosis and necrosis, acute axonal degeneration, axonal remodeling, demyelination, and glial scar formation [
6]. Owing to the complexity of this condition, previous researchers have investigated the use of neurophysiological tests, such as electroencephalogram (EEG), transcranial magnetic stimulation (TMS), and conditioned pain modulation (CPM), to identify potential biomarkers for neuroplasticity and imbalanced cerebral activities in patients with functional disabilities [
10].
EEG is extensively used in medicine to diagnose epilepsy and sleep disturbances, and its applications have been explored to help patients with many other neuropsychiatric conditions and disabilities [
11]. Vuckovic et al. [
12] observed significant differences in alpha power between different groups of patients with spinal cord injury and neuropathic pain, with patients who developed pain presenting a reduced alpha power resting state in the parietal region compared to those who did not develop pain. Moreover, Wang et al. [
13] demonstrated lower alpha power in SCI patients with neuropathic pain than in a group with only numbness, but this difference was identified across multiple brain regions, such as the frontal, motor, and parietal regions. Furthermore, Wang et al. [
13] demonstrated that SCI could lead to functional sensory and metabolic changes in the frontal, premotor, and thalamic regions.
Some authors hypothesize that SCI induces a shift in spectral oscillations towards low-frequency bands (such as theta oscillations) caused by a thalamocortical dysrhythmia (TDC) [
14,
15,
16]. Additional findings included the observation of reduced alpha and increased beta power in SCI patients [
17,
18]. In our studies involving patients with SCI, we observed a reduction in alpha and theta activity in patients with neuropathic pain and SCI compared to healthy controls during the EEG resting state, and the alpha/theta ratio is a potential surrogate of functional recovery during rehabilitation [
19,
20]. In our EEG studies in stroke, knee osteoarthritis, and fibromyalgia patients, we observed higher theta activity as a potential compensatory mechanism of pain and functional recovery, which brings attention to TDC in those populations as well [
21,
22,
23,
24]. In addition, frontal asymmetry in alpha and low-frequency bands, such as delta and theta bands, has been studied as a metric of emotion, motivation, and psychiatric conditions in both resting-state and task conditions [
25,
26].
However, other investigations showed an increase in EEG resting-state theta and alpha power in SCI patients [
27,
28]. The role of EEG oscillations in SCI recovery and the mechanism of neuroplasticity after the lesion is not completely clear. Given these mixed results regarding neural oscillations and their relationship with SCI, our cohort combined EEG measures with assessments of clinical improvement to investigate potential biomarkers of neuroplasticity. Additionally, while CPM assesses pain processing and the descending pain inhibitory system, TMS provides critical parameters of cortical excitability, including motor threshold (MT), motor-evoked potential (MEP), intracortical inhibition (ICI), and intracortical facilitation (ICF), thereby enhancing neurophysiological test interpretation when combined with EEG signals [
21].
Based on the evidence in the literature and the nature of this exploratory cross-sectional study, we hypothesized that EEG oscillations such as delta, theta, and alpha bands are associated with clinical and other neurophysiological variables in patients with SCI. Low-frequency EEG oscillations are potential biomarkers of motor recovery and psychological status, indicating a potential salutogenic compensatory mechanism in the central nervous system. These associations involve factors such as cognitive–emotional status, neurological impairment, lesion duration and level, conditioning pain tests, and cortical excitability parameters. Unfortunately, there is a lack of neurophysiological tests available to assess motor recovery in SCI in clinical practice, but EEG has potential applications that need to be explored in the physical rehabilitation field.
3. Results
3.1. Demographic and Clinical Variables
One hundred and two patients with SCI were included in this study, with a mean age of 41 years (SD: 16), eighty males (87.9%) and eleven females (12.1%), forty-one were white (45.1%), ten were black (11%), thirty-nine were of mixed race (42.9%), and one was indigenous (1.0%). Participants who self-reported as “pardo” in Portuguese were included in the “mixed race” category. In addition, we observed that the lesion levels of our participants were forty-eight cervical (47.06%), forty-one thoracic (40.21%), twelve lumbar (11.76), and one sacral (1.0%); forty-five had tetraplegia (44.12%), and fifty-seven paraplegia (55.88%).
Additional demographic and clinical data are shown in
Table 1. Continuous variables are presented with their mean and SD, while categorical or binary variables are presented with their
n and percentage.
3.2. Neurophysiological Findings
EEG data were recorded from 86 subjects, and the average of their relative power was represented as the mean and SD in each ROI and separated in the right and left brain hemispheres, as displayed in
Table 2 and
Table 3.
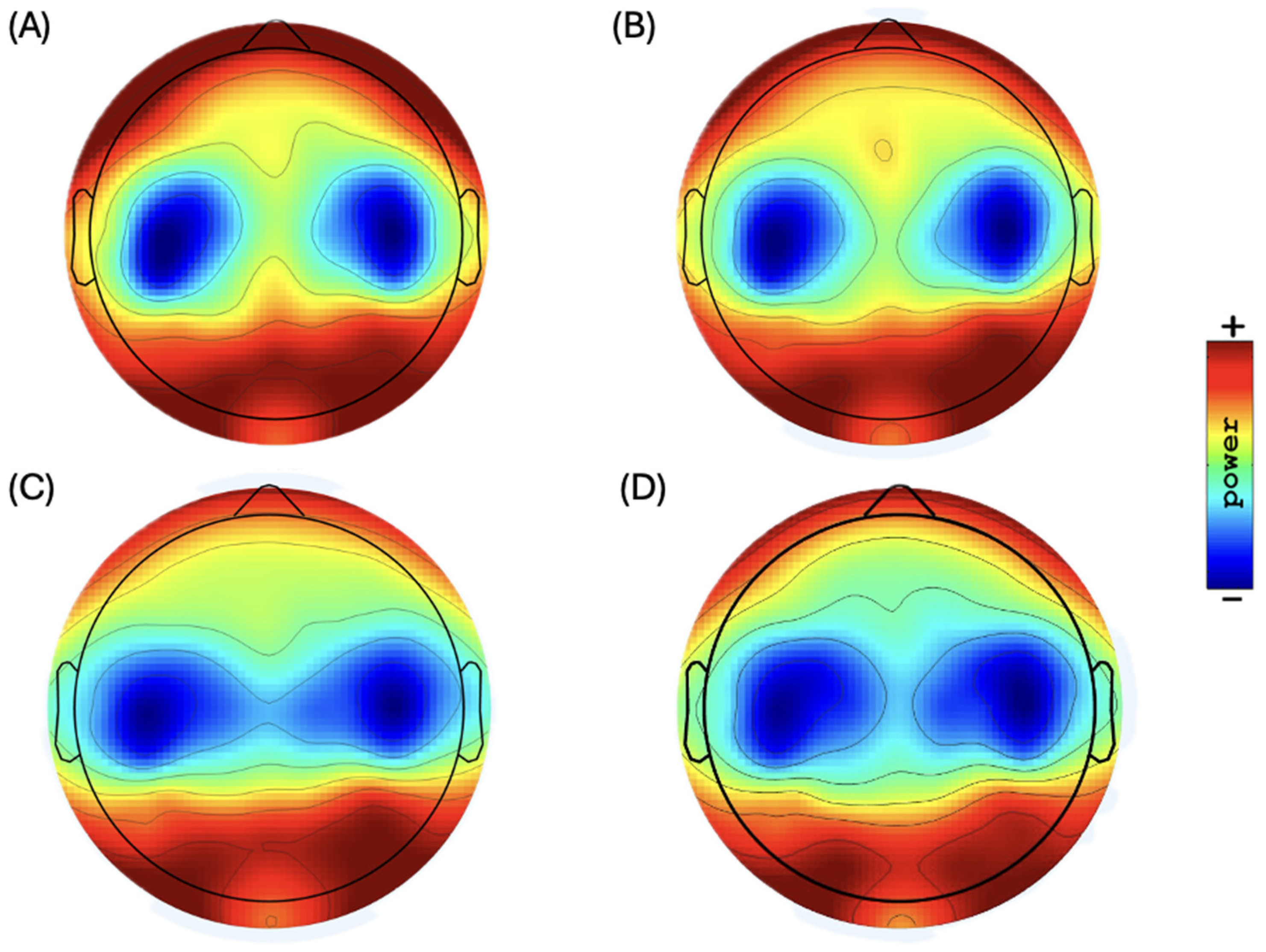
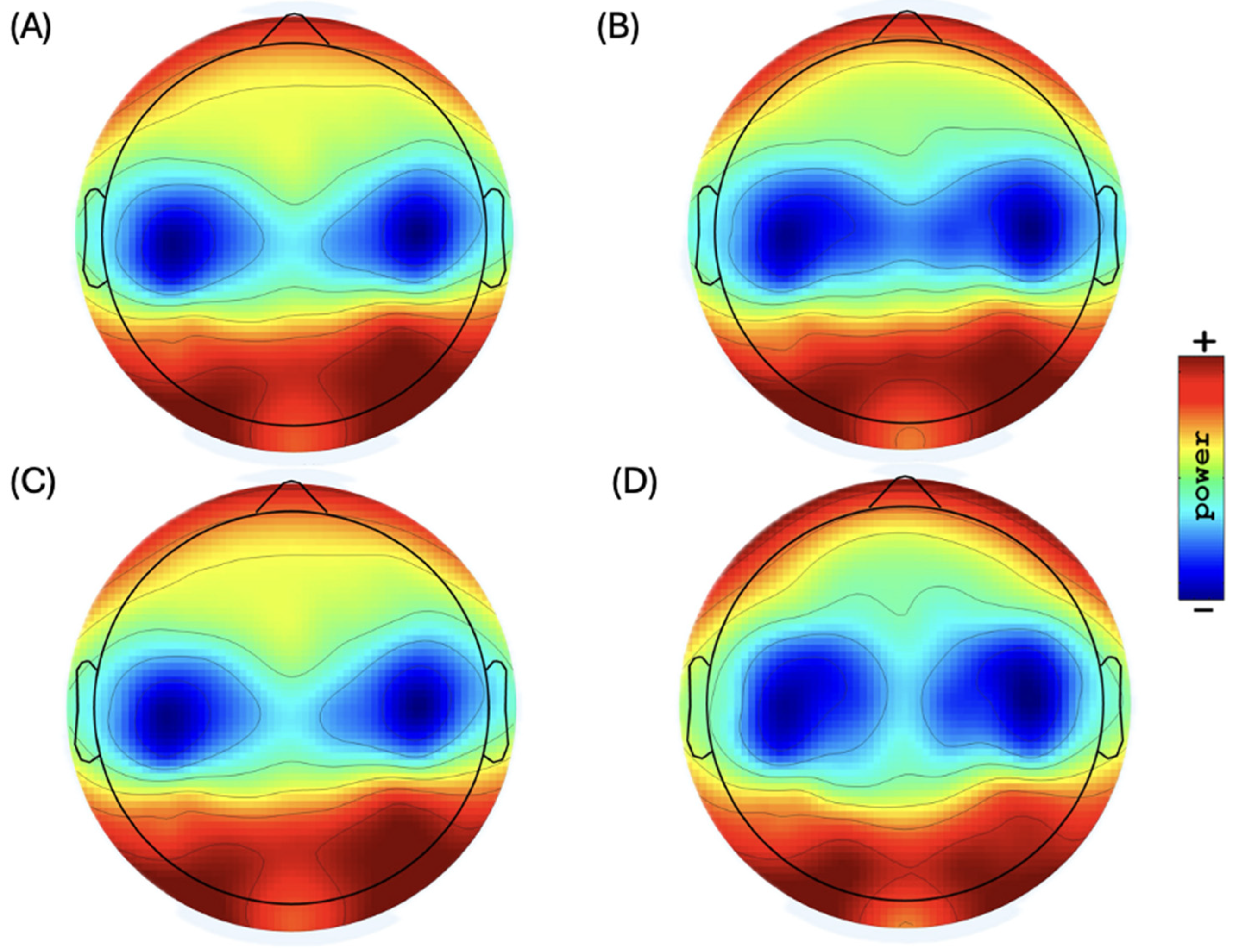
Figure 1 shows the topographic distribution of scalp plots in the resting-state EEG.
3.3. Univariate Analysis
Delta oscillations in the frontal regions demonstrated a negative association with depression symptoms (β-coef.: −0.05,
p-value: 0.032, 95% CI: −0.01 to 0.00) and a frontal delta asymmetry showed a negative association (towards the right hemisphere) with depression symptoms (β-coef.: −0.11,
p-value: 0.033, 95% CI: 0.00 to 0.02), demonstrating a reduction of delta frontal activity and a shift towards the right hemisphere as the depression symptoms worsen. A scatter plot of the regression lines is shown in
Figure 2.
Theta oscillations demonstrated significant or almost significant negative association with MEP in all ROIs: (i) frontal: β-coef.: −0.04, p-value: 0.068, 95% CI: −0.08 to 0.00; (ii) central: β-coef.: −0.03, p-value: 0.083, 95% CI: −0.07 to 0.00; (iii) parietal: β-coef.: −0.05, p-value: 0.027, 95% CI: −0.09 to −0.01. In contrast, alpha oscillations showed a positive correlation with MEP in all ROIs: (i) frontal: β-coef.: 0.102, p-value: 0.002, 95% CI: 0.04 to 0.16; (ii) central: β-coef.: 0.08, p-value: 0.008, 95% CI: 0.02 to 0.15; (iii) parietal: β-coef.: 0.106, p-value: 0.002, 95% CI: 0.04 to 0.17. These results show an interesting behavior of more activity towards higher frequency bands as the MEP also increases, indicating a potential compensatory mechanism involving theta and alpha oscillations and cortical excitability in patients with SCI.
In addition, we observed a negative association between frontal alpha and sleepiness (Î
2-coef.: −0.01,
p-value: 0.048, 95% CI: −0.01 to 0.00), as the alpha band is often associated with relaxed wakefulness and inhibitory control in the CNS. Frontal alpha asymmetry demonstrated a negative correlation (towards the left hemisphere) with anxiety symptoms (β-coef.: −0.01,
p-value: 0.014, 95% CI: −0.01 to −0.00), showing an association between greater alpha activity in the left frontal hemisphere and more severe depression symptoms. Scatter plots are shown in
Figure 3.
High alpha oscillations showed a negative relationship with CPM in the right hand in the frontal and parietal regions, with (i) β-coef.: −0.01, p = 0.087, 95% CI: −0.02, 0.00 and (ii) β-coef.: −0.01, p = 0.044, 95% CI: −0.03, 0.00, respectively, indicating that high alpha oscillations in those regions could be linked to a reduced ability to modulate pain. No significant results were observed for beta oscillations.
3.4. Multivariate Analysis
Delta-oscillation models reveal distinct regional effects influenced by various factors. The corresponding model explained the variance with an R-square of 0.25 in the frontal region, with depression showing a negative association with delta-band activity (β-coef.: 0.01,
p-value: 0.036) and age having a positive and significant relationship (β-coef.: 0.001,
p-value: 0.035). Other variables, such as the level of lesion, MOCA scores, and years of education, were included to control for their potential impacts on cognition and mental health. In the parietal region, where the model presented an R-square of 0.205, the ICI mean was a significant positive predictor of delta-band activity (β-coefficient: 0.010,
p-value: 0.022), while age, sex, level of lesion, and lesion time were included to control for their potential impact on neurological impairment.
Table 4 presents the delta multivariate models.
Theta-oscillation models showed a significant negative correlation with MEP and an R-square of 0.32, 0.29, and 0.40, respectively, in the frontal (β-coef.: −0.062,
p-value: 0.034), central (β-coef.: −0.057,
p-value: 0.049), and parietal (β-coef.: −0.063,
p-value: 0.021) regions. Age also had a significant negative relationship in the frontal and central areas (β-coef.: −0.105,
p-value: 0.008). Variables such as biological sex, lesion level, and AIS score were included to control for their potential influence on neurological impairment.
Table 5 presents the theta multivariate models.
Alpha-oscillation models showed a significant positive correlation with MEP and R-squares of 0.21, 0.14, and 0.23, respectively, in the frontal (β-coef.: 0.111,
p = 0.008), central (β-coef.: 0.087,
p = 0.040), and parietal (β-coef.: 0.110,
p = 0.010) regions, with age showing a trend toward a negative association in the parietal area (β-coef.: −0.106,
p = 0.075). Variables such as biological sex, age, lesion level, and lesion time were included to control for their potential influence on neurological impairment. Additionally, the SEPW total scale had a significant negative association with alpha-band activity in the parietal region (β-coefficient: −0.008,
p = 0.017), and age was a significant negative predictor (β-coefficient: −0.136,
p-value: 0.012) in this context. Multivariate alpha models are presented in
Table 6.
High alpha-oscillation models showed a significant negative correlation with CPM in the right hand, with R-squares of 0.13 and 0.18, respectively, in the frontal (β-coef.: −0.012,
p-value: 0.049) and parietal (β-coef.: −0.016,
p = 0.018) regions, and with age also showing a significant negative relationship in the parietal area (β-coef.: −0.148,
p-value: 0.033). Variables such as sex and lesion level were included to control for their potential influence on brain function. The high alpha multivariate models are presented in
Table 7.
Frontal-asymmetry models showed a significant association in the delta band with depression symptoms and lesion time, with an R-square of 0.13, with depression showing a positive relationship with the right hemisphere (β-coef.: 0.010,
p = 0.036) and lesion time showing a negative relationship (β-coef.: −0.002,
p = 0.040). The frontal alpha-asymmetry model, with an R-square of 0.13, was negatively correlated with anxiety symptoms (β-coefficient: −0.006,
p = 0.034) and asymmetry towards the left hemisphere. Variables, such as age, lesion time, and lesion level, were included to control for their potential influence on brain function. Multivariate frontal asymmetry models are presented in
Table 8.
A summary of the main results and correlation directions is presented in
Table 9. No model was found to be significantly related to beta oscillations.
4. Discussion
Our multivariate model results are consistent with those of previous studies, reinforcing the association between EEG oscillations and psychological and other neurophysiological variables. Frontal delta oscillations and asymmetry in the delta and alpha bands are linked to the severity of depression and anxiety symptoms. A reduction in alpha bands and an increase in low-frequency bands in the right hemisphere are often associated with worse psychiatric symptoms. Another interpretation of our results is that the reduction in MEP correlates with higher theta and lower alpha activity across all ROIs. Patients with SCI often present a reduction in their MEP metrics due to impaired motor pathways; therefore, a shift of higher frequency bands to lower frequency bands could result in intrinsic compensatory mechanisms in the cortical–spinal pathway [
21]. These results converge with previous findings in the literature that found that the shift towards theta could indicate TDC in this population [
14,
15,
16]. Finally, increased alpha activity in the frontal and parietal regions was associated with a less effective descending inhibitory pain process, as measured in the right hand. However, this relationship was not statistically significant when compared with the left hand.
Anxiety and depression symptoms are prevalent among patients with spinal cord injury (SCI) due to significant functional limitations and a profound impact on quality of life. Beyond these factors, the presence of spinal cord lesions can disrupt compensatory mechanisms in the brain, which may increase the risk of developing mental health issues [
9]. The increase in delta activity in the frontal region may be explained by a compensatory mechanism in patients with more depressive symptoms. Low-frequency bands, such as delta oscillations, are associated with homeostatic processes in the cortical and subcortical circuits [
35,
36]. A recent investigation demonstrated that reduced delta baseline activity is correlated with enhanced efficacy of cognitive behavioral therapy in depression [
37]. Moreover, we observed a pattern of frontal delta asymmetry in depression and frontal alpha asymmetry in anxiety (
Figure 2). Delta oscillations shift from the left toward the right hemisphere, while alpha oscillations shift from the right toward the left hemisphere as the symptoms worsen, crossing the “x” axis approximately at score five. A closer examination of the behavior of both frequency bands suggests that the reorganization of frontal circuits towards lower frequency bands in the right hemisphere is associated with a greater prevalence of mental health issues.
Other neuroimaging studies have also investigated the use of frontal asymmetry as a biomarker for cognition and psychiatric conditions [
38,
39,
40]. EEG frontal asymmetry scores hold significant potential as tools for understanding cortical activity across various neuropsychiatric conditions in mental health and rehabilitation; however, further research is essential to fully elucidate their role and effectiveness in these contexts. Expanding the evidence will help clarify how these asymmetry scores can be used for diagnosis and treatment in clinical settings, contributing to more targeted and effective interventions.
The reduction of MEP in patients with SCI is expected, as MEP reflects the integrity of descending corticospinal-tract fibers, which are often impaired in patients with SCI [
41]. While conditions such as stroke and traumatic brain injury directly affect the cortical substrate, the cortical and subcortical regions remain intact in SCI. Therefore, an injury to the spinal cord triggers cortical reorganization in the brain areas associated with the affected limbs, activating mechanisms of cortical plasticity to promote functional recovery [
42]. Cortical reorganization can be attributed to intrinsic connections and inhibitory GABAergic activation, resulting in the plasticity of cortical networks and ICI [
43]. The observed negative association between theta oscillations and MEPs and the positive correlation between alpha oscillations and MEP support the theory presented in the literature [
21,
42,
43,
44]. This indicates a compensatory mechanism within the CNS, such as changes in theta and alpha oscillations, in an attempt to reorganize and restore function despite the disruption caused by SCI.
Theta oscillations appear to play a compensatory role in response to motor injuries, as demonstrated in previous studies [
23,
45]. In contrast, alpha oscillations may reflect a more relaxed and salutogenic state, particularly in relation to cognitive functions, such as attention and memory. These distinct patterns of neural activity suggest that different oscillations may indicate various aspects of recovery and brain function post-injury [
46]. These associations with MEP are linked to the modulation of the cortical–spinal pathway, while the negative correlation between delta and ICI is explained by an increase in cortical inhibition in the parietal regions, which are involved in cognitive tasks [
47,
48].
Interestingly, our findings indicate that high alpha oscillations are linked to a lower CPM response, with statistical significance only on the right-hand side. This relationship can be explained by the role of alpha oscillations in modulating cortical excitability and sensory processing, which are essential for the brain’s ability to regulate and inhibit pain; as shown in our CPM metric, a reduced CPM means a worse response to pain [
10,
49,
50]. Additionally, the negative association between the alpha band in the parietal region and sleepiness illustrates the role of alpha activity in cognitive function, fatigue, and attention levels, as described previously in our study [
24]. EEG signals and CPM are potential biomarkers for understanding the neurophysiological mechanisms underlying pain modulation, particularly in the spinal cord injury (SCI) population where CPM is frequently impaired.
The strengths of this study are the sample size, the standardized recruitment and data collection protocols, and the use of well-known validated tools. The limitations are related to the cross-sectional design, which restricts the possibility of establishing causality between variables. Also, the absence of a control group limits the capacity to compare our findings with those of healthy subjects, reducing the generalizability of the results. However, our findings could identify associations and contribute to hypothesis generation for future studies. To address these limitations, longitudinal studies with a control group are necessary to provide more robust evidence regarding the temporal relationships between variables and to establish causality over time.

 ,
, 



{kind=link}
{kind=link}
{kind=link}