Abstract
Objective: The study investigated the preoperative anatomical variables that affect the outcome of surgical correction in patients with Class III facial asymmetry. Methods: The study recruited 37 consecutive patients with facial asymmetry who had 2-jaw orthognathic surgery. They were divided into two groups based on the surgical outcome: symmetrical (S group) or asymmetrical (A group), according to the asymmetry index. The CBCT images were obtained before surgery (T0) and after debond (T1). The 3D dentofacial measurements were compared between groups S and A by the Mann–Whitney test. Spearman correlation analysis was performed to examine the relationship of all dentoskeletal variables in T0 with the facial symmetry outcome. Results: Significant between-group differences were observed in preoperative time, including maxillary anterior occlusal canting, maxillary posterior occlusal canting, the gonion–Frankfort horizontal plane (FHP) distance, the mandibular ramus axis–FHP distances, and sagittal and transverse of condyle position. Conclusions: For patients with severe skeletal Class III asymmetry, preoperative anatomical variables, particularly preoperative “roll” and “yaw” discrepancies and anatomical limitations of the mandible, should be considered for favorable asymmetry correction. Based on the anatomic variables that affect the outcomes of facial asymmetry correction, prognosis and treatment limitation could be predicted before treatment.
1. Introduction
Patients with Class III malocclusion with mandibular prognathism have a high prevalence of facial asymmetry [1,2,3,4]. The prevalence of skeletal Class III face asymmetry has been reported to range from 47.9% to as high as 85% in Asian cohorts [3,4]. The lower face, particularly the chin, deviates more frequently than the upper face [2,3]. The occurrence of facial skeleton asymmetry may result from variations in the morphology of bony structures and the positional deviation of the maxillomandibular complex, or only the mandible [5,6].
For patients with severe skeletal jaw discrepancy and facial asymmetry, a combination of orthodontic treatment and orthognathic surgery (OgS) is considered the only viable treatment option for improving facial appearance and restoring normal occlusal function [5]. The goal of 2-jaw OgS is to correct the overall dentofacial asymmetry regarding dental occlusion, align maxillary midline and chin to the facial midline, level the oral commissure and occlusal plane cant, and correct vertical and sagittal discrepancy [6]. Adjunctive surgeries or treatments, such as bone shaving, bone grafting, and soft tissue grafting, can improve contour asymmetry and enhance harmony of the face form [7,8]. With the development of 3D images, cone-beam computed tomography (CBCT), and computer-assisted surgical simulation, 2-jaw OgS can be precisely planned, assisting surgeons to achieve similar treatment outcomes to correct facial asymmetry [9,10,11].
In many cases, however, residual asymmetry persists postoperatively [12]. Lin et al. reported that mandibular asymmetry persisted in 45 patients with facial asymmetry undergoing OgS, even though the center point of the mandible was well aligned with the facial midline [13]. According to the previous study from our team, Lin et al. analyzed 24 patients with skeletal Class III malocclusion with double-jaw OgS, who were classified according to the outcome of subjective visual perception scores [14]. The findings demonstrated that midline parameter deviation, shape of the mandibular border, and contour of menton morphology influenced the visual perception of postoperative asymmetry.
Chen et al. categorized mandibular asymmetry into three groups according to the amount and direction of ramus asymmetry relative to menton deviation in 3D-CBCT analysis [15,16]. They concluded that ramus asymmetry was less predictable. However, no specific factors were found to contribute to residual facial asymmetry.
The study aims to explore the preoperative anatomical variables affecting the outcome of surgical correction in facial asymmetry in patients with skeletal Class III malocclusion. The null hypothesis was that the anatomical factors are not different between the surgical outcome of good facial symmetry and residual asymmetry.
2. Materials and Methods
2.1. Patients
This retrospective study evaluated 37 consecutive adult Taiwanese patients with skeletal Class III facial asymmetry, who received bimaxillary OgS from 2014 to 2016 at the Chang Gung Memorial Hospital, Taipei, Taiwan.
The inclusion criteria were as follows: (1) having skeletal Class III dentofacial deformities with preoperative menton deviation >4 mm from the midsagittal plane (MSP); (2) undergoing bimaxillary OgS (Le Fort I osteotomy and BSSO); (3) having complete preoperative and posttreatment CBCT data; and (4) receiving treatment from the same orthodontist and the same group of surgeons.
The exclusion criteria of the subjects were: (1) craniofacial anomalies, such as cleft lip and palate, hemifacial microsomia; (2) craniofacial trauma; and (3) untreated temporomandibular joint disorder.
The sample size was calculated using G*Power (version 3.1.9.4; Universität Kiel, Kiel, Germany) [17]. On the basis of the difference in Go to FHP, significance of 95%, and power of 80%, the minimum sample size required for the two-sample t-test was 36.
This study followed the guidelines of the Declaration of Helsinki. The research protocol was approved by the Institutional Review Board and medical ethics committee of the Chang Gung Memorial Hospital.
2.2. Data Collection
The patients’ 3D craniofacial images were taken in the natural head position with maximum intercuspation, by using an i-CAT scanner (Image Sciences International, Hatfield, PA), with the following settings: 120 kVp; 36.9 mA; field of view, 22 × 16 cm; scanning time, 40 s; and voxel size, 0.4 × 0.4 × 0.4 mm. All data were obtained 1 month before surgery (T0) and on completion of orthodontic treatment (T1).
The DICOM format from the CBCT scanner was imported into the Simplant O&O software (Materialise Dental NV, Leuven, Belgium) to reconstruct the 3D skull models, including the cranium with maxilla and mandible. Maxillary and mandibular dental casts were digitized by a 3D scanner (3Shape, Copenhagen, Denmark) and integrated into the CBCT model by surface matching.
2.3. Presurgical 3D Surgical Simulation
The guidelines and procedures for 3D surgical simulation were reported in a previous study [11]. Both clinical facial and 3D cephalometric measurements were incorporated into the development of the 3D surgical plan.
The surgical stent for the 2-jaw OgS was fabricated according to the surgical occlusion setup in the maxillary and mandibular dental casts. An intermediate stent was fabricated with a 3D-printed technique to guide the surgery.
2.4. Surgical Technique
All patients underwent double-jaw OgS. The maxillo-mandibular complex (MMC) was completely mobilized with LeFort I osteotomy and BSSO. The sequence of surgery was based on the designated intermediate stent. The final 2-jaw movement was guided by the final occlusion stent with temporary intermaxillary fixation during surgery. The surgeons finalized the MMC pitch rotation according to the 3D surgical simulation and final assessment of the facial symmetry and profile. Next, the MMC was fixed to the maxillary base and mandibular proximal segments with rigid fixation. Genioplasty surgeries were conducted to enhance the chin contour as a last step if required.
The BSSO technique conducted at our center was modified from the Hunsuck technique, with a more anteriorly extended anterior osteotomy cut [18,19]. This technique facilitates later intraoral placement of the plates and screws, and allows for a greater amount of mandibular repositioning with good long-term stability.
For Asian women, simultaneous mandibular angle contouring is a common adjunct procedure to improve the “square face” [20]. The medial cortex of the mandibular angle on the proximal segment can be harvested for a high-quality bone graft, if necessary [21].
2.5. 3D Dentoskeletal Measurements
The 3D skull models at T0 and T1 were superimposed on the anterior cranial base, and frontal and periorbital surface. The deviation values were calculated, and a value of 0.5 mm was considered acceptable to ensure that the corresponding reference areas had the highest possible accuracy.
The 3D reference planes were constructed using the landmarks identified on the preoperative objects (Figure 1). Table 1 lists the definition of the 3D landmarks, and depicts the linear and angular measurements of each landmark relative to the reference planes (Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7). The deviated side was defined as the side of the face, including the skeletal menton, and the opposite side was the contralateral half (Figure 2). All landmarks were identified by the same investigator.
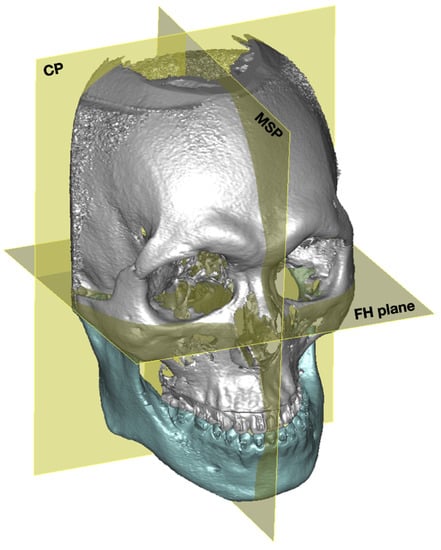
Figure 1.
Three reference planes for 3D analysis. The 3D reference planes were constructed by the landmarks identified on the preoperative objects. The Frankfort horizontal plane (FHP) was determined by the bilateral orbitale and the midpoint of the bilateral porion. The midsagittal plane (MSP) was defined as the plane perpendicular to the FHP and passing through the nasion. The coronal plane (CP) was the plane perpendicular to the FHP and the MSP, and passing through the basion.

Table 1.
Definition of 3D dentoskeletal landmarks and variables for measurement.
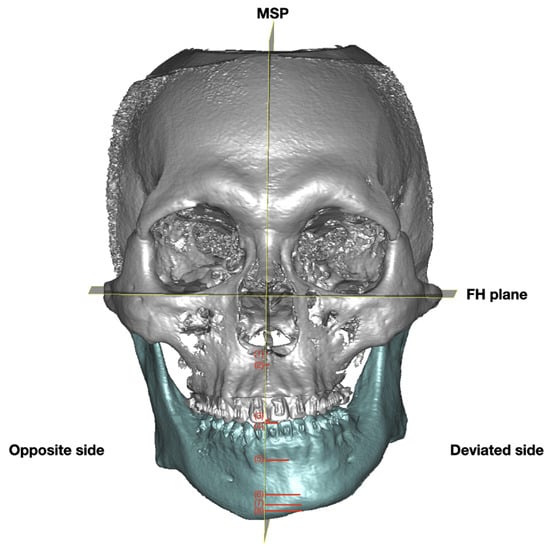
Figure 2.
Midline measurements in the frontal view. The MSP separated the face into deviated and opposite sides. The deviated side was defined as the side of the face, including the skeletal menton, and the opposite side was the contralateral half. (1) ANS to MSP, (2) A point to MSP, (3) U1 to MSP, (4) L1 to MSP, (5) B point to MSP, (6) Pog to MSP, (7) Gn to MSP, (8) Me to MSP.
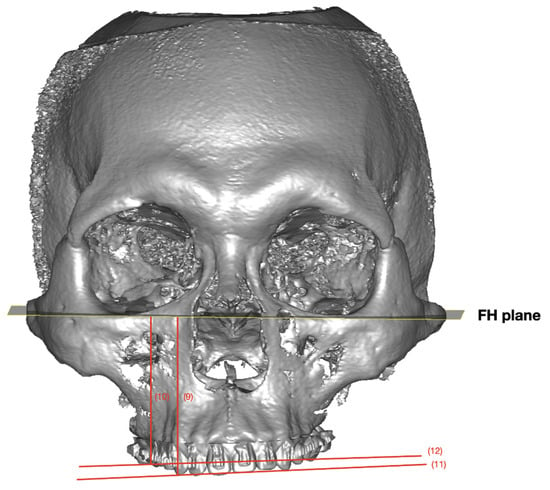
Figure 3.
Maxillary bilateral variables. (9) U3 to the FHP, (10) U6 to the FHP, (11) maxillary anterior canting (ΔU3 to FHP), (12) maxillary posterior canting (ΔU6 to FHP).
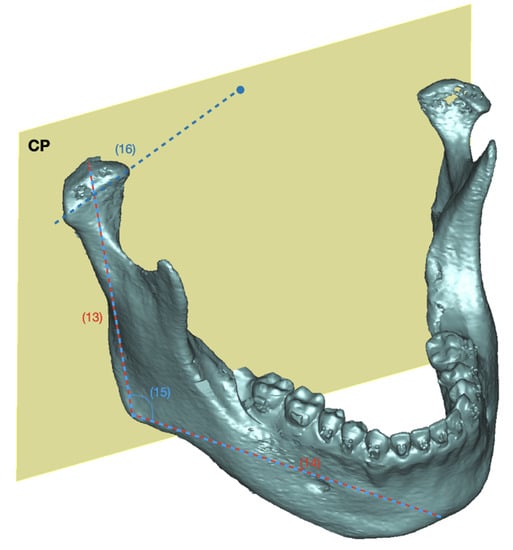
Figure 4.
Mandibular linear and angular measurements. (13) Ramus height, (14) body length, (15) gonial angle, (16) condyle axis to CP.
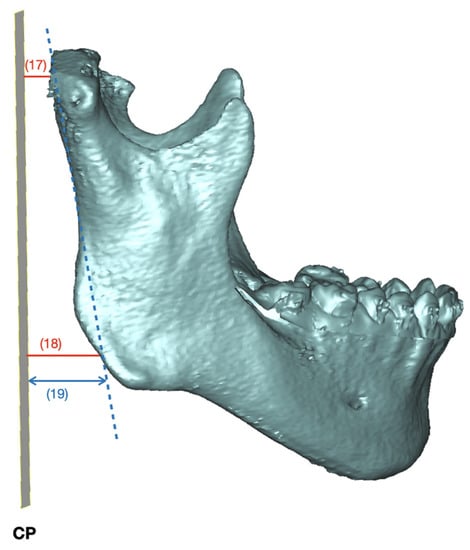
Figure 5.
Mandibular measurements in sagittal view. (17) Co to CP, (18) Go to CP, (19) ramus axis to CP.
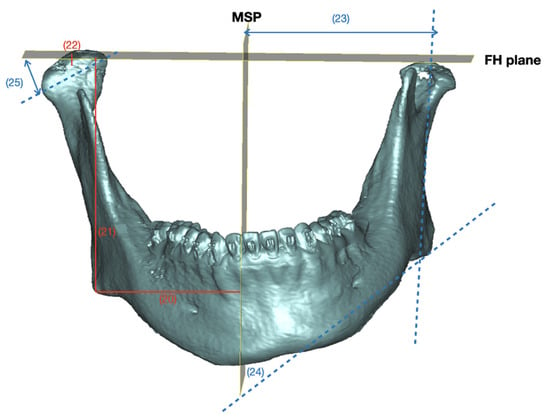
Figure 6.
Mandibular measurements in frontal view. (20) Go to MSP, (21) Go to the FHP, (22) Co to the FHP, (23) Ramus axis to MSP, (24) Md axis to MSP, (25) condyle axis to the FHP.
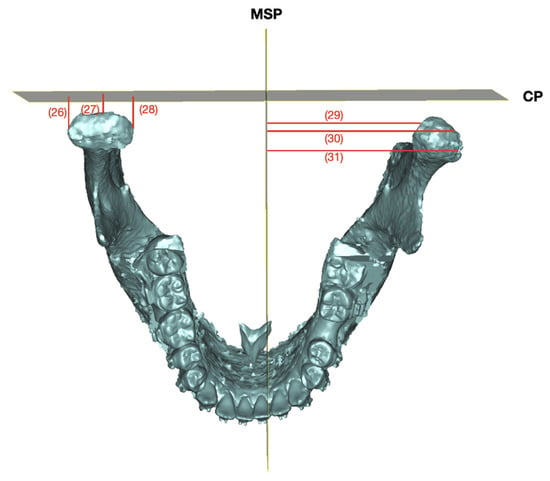
Figure 7.
Mandibular condyle position measurements. (26) Medial condylar pole to CP, (27) Co to CP, (28) lateral condylar pole to CP, (29) medial condylar pole to MSP, (30) Co to MSP, (31) lateral condylar pole to MSP.
2.6. Classification of Patients after Treatment Completion (T1)
The distances from each landmark to the three reference planes were measured and used to calculate the asymmetry index: dx, dy, and dz represent the distance from the landmark to the MSP, FHP, and CP, respectively.
For bilateral asymmetry index, asymmetry index = √((d_d x − [d_o x)]^2 + (d_d y − [d_o y)]^2 + (d_d z − [d_o z)]^2),
where ddx, ddy and ddz represent the distance from the landmark on the deviated side to the MSP and dox, doy and doz represent the distance from the landmark on the opposite side to the MSP.
According to the asymmetry index after treatment completion, patients were categorized into the relative symmetry outcome group (group S) and the relative asymmetry outcome group (group A). One median was excluded, and each group had 18 patients. Figure 8 illustrates the study flowchart.
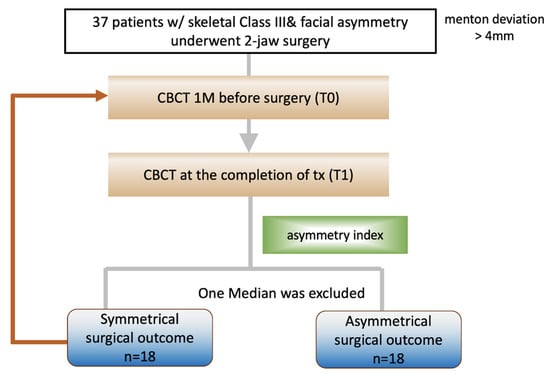
Figure 8.
Flow chart for research design.
2.7. Statistical Analyses
The Mann–Whitney U test was used to compare the between-group differences in preoperative anatomical variables. p < 0.05 was set as statistically significant. Spearman correlation analysis was performed to examine the relationship of all dentoskeletal variables in T0 with the facial symmetry outcome—asymmetry index (T1)—for all patients.
For error study, 10 randomly selected cases were re-landmarked and measured within 3 weeks. The intraexaminer reliability test was conducted using intraclass correlation (ICC) [22] and Dahlberg’s formula [23].
3. Results
We enrolled 37 consecutive patients (21 women and 16 men), with an average age of 23.6 years (18.0–33.0 years, SD 4.6 years). Among them, 27 (72.9%) and 10 (27%) had preoperative chin deviation toward the left and right sides, respectively. Table 2 presents the descriptive data for the patients in the two groups.
Table 2.
Descriptive data of the two groups of patients.
3.1. Error Study
The ICC for linear measurements was 0.91, and the measurement error determined using Dahlberg’s formula was 0.21 mm. Both results indicate excellent intraexaminer reliability.
3.2. Comparison of Preoperative 3D Measurements between Groups S and A
For all midline variables, the amount of the ANS, A, U1, L1, B, Pog, Me, and Gn deviation from the MSP exhibited more discrepancy in group A than in group S, but none of these parameters indicated a significant between-group difference before surgery (Table 3).
Table 3.
Comparison of 3D preoperative (T0) measurements of midline variables between groups S and A.
A significant between-group difference was detected in maxillary anterior canting and maxillary posterior canting before surgery (Table 4). The extent of anterior and posterior canting was significantly larger in group A.
Table 4.
Comparison of 3D preoperative (T0) measurements of bilateral variables between symmetry and asymmetry outcome groups.
In the mandible, the Go–FHP distance exhibited a discrepancy between the two sides (ΔGo to the FHP), which was 1.88 ± 1.77 mm in group S and 5.25 ± 4.51 mm in group A (p = 0.015). The discrepancy in the axis of the mandibular border to FH was also significantly different between the two groups (p = 0.05) (Table 4).
A significant difference was detected in five mandible variables at the deviated side in the distance between the coronal plane and the gonion, condyle, medial condylar pole, lateral condylar pole, and glenoid fossa (Table 5).
Table 5.
Comparison of 3D preoperative (T0) measurements of bilateral variables between groups S and A (deviated side).
A significant difference was observed in two opposite-side mandible variables, in the distances between the MSP and lateral condylar pole (p = 0.012) and medial condylar pole (p = 0.043) (Table 6).
Table 6.
Comparison of 3D preoperative (T0) measurements of bilateral variables between groups S and A (opposite side).
3.3. Correlation of the Asymmetry Index with Presurgical Variables
The asymmetry index had positive low-to-moderate correlations with the six preoperative variables: ΔU3 to the FHP (r = 0.340), ΔU6 to the FHP (0.348), Δmandibular border axis to the FHP (r = 0.332), CoL (r = 0.422)/CoM (r = 0.342) of the opposite side to MSP, and ΔGo to the FHP (r = 0.409) (Figure 9). The asymmetry index was negatively correlated with five preoperative variables: Co (r = −0.476), CoM (r = −0.546), CoL (r = −0.358), GF (r = −0.471), and Go of the deviated side to CP (r = −0.396). It showed that the distance of the deviated-side variables to the coronal plane in group A was negatively correlated with the asymmetry index, while the distance of the opposite side variables to the MSP was positively correlated with the asymmetry index. The bilateral discrepancies demonstrated a positive correlation with the asymmetry index.
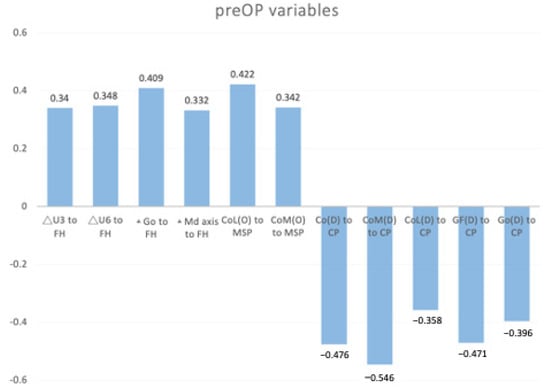
Figure 9.
Significant correlation of the asymmetry index with preoperative variables. Spearman correlation was used for statistical analysis. The asymmetry index was positively correlated with the six preoperative variables and negatively correlated with five preoperative variables.
4. Discussion
This study used 3D linear and angular measurements to clarify the preoperative anatomical variables affecting the outcome of surgical correction in Class III facial asymmetry.
Patients with skeletal Class III malocclusion and facial asymmetry, with a menton deviation greater than 4 mm, were included in this study. According to Kwon et al., the perception of asymmetry of a chin deviation of 2 mm to the right and 4 mm to the left is not detected clinically [24]. Alongside that, most individuals, whether dental professionals or laymen, can notice a chin deviation of more than 4 mm [25]. Thus, it is acceptable to define 4 mm of menton deviation relative to MSP as facial asymmetry. The mean preoperative menton deviation in the two groups was 6.52 ± 5.36 mm in group S and 8.15 ± 4.19 mm in Group A (Table 3). The patients included in our study showed a severe deviation of menton, indicating a greater severity of facial asymmetry.
After treatment completion, facial asymmetry significantly improved in all patients, but did not completely resolve. Lin et al. reported that preoperative 3D dentoskeletal variables were not related to subjective visual perceptions of postoperative asymmetry [14]. In the present study, we used a more objective method to define postoperative asymmetry. However, the menton deviation decreased significantly after treatment, and the difference in midline deviation was not appropriate for defining postoperative symmetry and asymmetry. Currently, there is no objective 3D index to represent the degree of facial asymmetry. Therefore, we used the asymmetry index at treatment completion to classify patients into two groups and evaluate the preoperative variables.
We observed that only bilateral variables, and not midline variables, significantly affected the surgical outcomes. This may be because midline deviation is already corrected by surgeons with the aid of 3D surgical simulation [10,11]. For bilateral discrepancy, four variables were observed to significantly affect the surgical outcome: (1) maxillary anterior occlusal canting, (2) maxillary posterior occlusal canting, (3) ΔGo to the FHP, and (4) Δmandibular axis to the FHP. These variables indicate the “roll asymmetry” of the maxilla and mandible.
For maxillary occlusal canting, the greater the preoperative discrepancy, the higher the possibility of residual asymmetry. However, maxillary occlusal canting was corrected well in both groups. Thiesen et al. found that the odds of presenting with mandibular asymmetry were significantly higher in the presence of maxillary asymmetry [26]. The mandible is often associated with craniofacial asymmetries, with maxillary asymmetries often secondary to asymmetrical mandibular growth [27]. Severe maxillary canting might indicate more severe deviation of the mandible and more severe asymmetry of the whole face. The occlusal plane canting was usually the result of compensating growth to mandibular asymmetry. The reasons underlying the correlations are not certain and deserve future investigation.
Correction of bilateral gonion contour discrepancy is more difficult and relies more on the surgeon’s decision-making during surgery. Trimming or contouring the gonion angle or adaptation of the proximal and distal segments all affect the surgical outcome. Presurgical ΔGo to MSP did not affect the surgical outcome, but ΔGo to the FHP and Go of the deviated side to CP showed a significant between-group difference. This might indicate that the preoperative roll (ΔGo to the FHP) and yaw (Go of the deviated side to CP) mandibular asymmetry affects the outcome. In Asia, most patients request mandibular angle reduction during surgery due to the preference for a slim and oval face [20]. Thus, the 3D gonion point would be altered after surgical contouring of the mandibular angle.
In mandibular variables on the deviated side, a significant difference was observed in the distances between the bilateral gonion, glenoid fossa, condyle, and medial and lateral condylar poles and the coronal plane between groups A and S. The distance of the deviated side variables to the coronal plane was smaller in group A than in group S. On the opposite side, the distances between the bilateral medial and lateral condylar poles to the MSP were significantly different between the two groups. The distance in group A is greater than that in group S. The different results between the deviated and opposite side variables indicate that the preoperative condyle position in the sagittal and transverse directions might relate to a higher asymmetry index after surgery. One reason is that the condyle and glenoid fossa might be anatomical limitations, because we could not move or change their original position during surgery. This should be considered during 3D planning. In clinical situations, when the distance of the CoL–MSP is greater in the opposite side than in the deviated side, the ramus axis is affected, causing facial asymmetry, even when the midline landmarks are perfectly aligned. In such cases, the patient should be informed preoperatively of a greater chance of residual asymmetry. The mandible border contouring or fat transplantation are choices for further asymmetry correction [8].
Some studies have discussed different surgical techniques to improve the outcome of ramus symmetry. The greatest advantage of intraoral vertical ramus osteotomy (IVRO) over BSSO is a lower incidence of injury to the inferior alveolar nerve [28,29]. Other advantages of IVRO include technical simplicity, shorter operation time, and less adverse effects related to the temporomandibular joint [30]. However, BSSO provides better bony interface with proximal and distal segments, and easier use of rigid fixation, thus minimizing the need for intermaxillary fixation [31]. Therefore, there is larger interference between the proximal and distal segments in IVRO during mandibular setback, resulting in a more significant increase of the total ramus angle, compared with that in BSSO [32]. However, Lee et al. had a different opinion: they reported a series of three cases with severe rotational asymmetry, using unilateral IVRO on the shorter side combined with sagittal split ramus osteotomies on the contralateral side for a greater setback [33]. They proposed that IVRO causes less rotational displacement of the proximal segment on the deviated side. The condylar segments that were displaced or rotated during surgery might return to their original physiologic position. The outcome and stability of the two different combined osteotomies on the mandible, in correction of face asymmetry, require further investigation.
Many factors are related to residual facial asymmetry, such as anatomical factors, surgical factors, surgical relapse, soft tissue response and adaptation, and asymmetric dynamic facial movement. However, in this study, we only discussed anatomical factors. This study also had the following limitations: first, we only discussed skeletal and dental variables, while the information of real facial soft tissue appearance was lacking. Second, the 3D reference planes were designed by skeletal landmarks; the setting of the 3D reference plane may be different from real patients. In clinical situations, the whole face, including eyes and ears, should be considered when deciding the reference plane. Finally, considerable interindividual variation may exist in the etiology of facial asymmetry, and thus, variables accounting for each type of asymmetry classification. Further investigations might be needed to develop different surgical consideration and modification for outcome improvement in correction of facial asymmetry. Additionally, a larger sample size and soft tissue evaluation could provide more informative outcome assessment in the future study.
5. Conclusions
- Patients with severe skeletal Class III asymmetry, preoperative anatomical variables of the maxillary occlusal plane cant, bilateral gonion discrepancy to the FHP, bilateral mandibular axis discrepancy to the FHP, and sagittal and transverse of condyle position, were related to an achievement of favorable outcomes in asymmetry correction.
- In sagittal mandible dimension, a significant between-group difference was noted in in the distances from the condyle, medial and lateral condylar poles, glenoid fossa, and gonion of the deviated side, to the coronal plane.
- In the transverse dimension, a significant between-group difference was noted in the distances from the medial and lateral condylar poles of the opposite side, to the MSP. In surgical correction of face asymmetry, “roll” and “yaw” discrepancies and anatomical limitations are critical factors affecting treatment outcomes.
Author Contributions
Conceptualization, E.W.-C.K. and Y.-T.L.; methodology, E.W.-C.K. and Y.-T.L.; software, E.W.-C.K.; validation, E.W.-C.K., C.-H.L., Y.-A.C.; formal analysis, Y.-T.L.; investigation, C.-H.L.; resources, Y.-A.C.; data curation, Y.-T.L.; writing—original draft preparation, Y.-T.L.; writing—review and editing, E.W.-C.K.; visualization, Y.-T.L.; supervision, E.W.-C.K.; project administration, Y.-T.L.; funding acquisition, E.W.-C.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Chang Gung Memorial Hospital (No. 202000813B0).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Please contact the corresponding author to request the data of this study.
Acknowledgments
We acknowledge the support of the Craniofacial Research Center, Chang Gung Memorial Hospital, Linkuo, Taiwan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Peck, S.; Peck, L.; Kataja, M. Skeletal asymmetry in esthetically pleasing faces. Angle Orthod. 1991, 61, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Severt, T.R.; Proffit, W.R. The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int. J. Adult Orthodon. Orthognath. Surg. 1997, 12, 171–176. [Google Scholar]
- Haraguchi, S.; Takada, K.; Yasuda, Y. Facial asymmetry in subjects with skeletal Class III deformity. Angle Orthod. 2002, 72, 28–35. [Google Scholar] [CrossRef]
- Chew, M.T. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle Orthod. 2006, 76, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Bell, W.H.; Creekmore, T.D. Surgical-orthodontic correction of mandibular prognathism. Am. J. Orthod. 1973, 63, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Ko, E.W.-C.; Huang, C.S.; Chen, Y.R. Characteristics and Corrective Outcome of Face Asymmetry by Orthognathic Surgery. J. Oral Maxillofac. Surg. 2009, 67, 2201–2209. [Google Scholar] [CrossRef] [PubMed]
- Cheong, Y.W.; Lo, L.J. Facial asymmetry: Etiology, evaluation, and management. Chang. Gung Med. J. 2011, 34, 341–351. [Google Scholar]
- Wang, Y.-C.; Wallace, C.G.; Pai, B.C.-J.; Chen, H.-L.; Lee, Y.-T.; Hsiao, Y.-C.; Chang, C.-S.; Liao, Y.-F.; Chen, P.K.-T.; Chen, Y.-R. Orthognathic Surgery with Simultaneous Autologous Fat Transfer for Correction of Facial Asymmetry. Plast. Reconstr. Surg. 2017, 139, 693–700. [Google Scholar] [CrossRef]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F. New Clinical Protocol to Evaluate Craniomaxillofacial Deformity and Plan Surgical Correction. J. Oral Maxillofac. Surg. 2009, 67, 2093–2106. [Google Scholar] [CrossRef]
- Udomlarptham, N.; Lin, C.-H.; Wang, Y.-C.; Ko, E.-C. Does two-dimensional vs. three-dimensional surgical simulation produce better surgical outcomes among patients with class III facial asymmetry? Int. J. Oral Maxillofac. Surg. 2018, 47, 1022–1031. [Google Scholar] [CrossRef]
- Ko, E.W.-C.; Lin, C.-H.; Chen, Y.-A.; Chen, Y.-R. Enhanced Surgical Outcomes in Patients With Skeletal Class III Facial Asymmetry by 3-Dimensional Surgical Simulation. J. Oral Maxillofac. Surg. 2018, 76, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Suzuki-Okamura, E.; Higashihori, N.; Kawamoto, T.; Moriyama, K. Three-dimensional analysis of hard and soft tissue changes in patients with facial asymmetry undergoing 2-jaw surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhu, P.; Lin, Q.; Huang, X.; Xu, Y.; Yang, X. Comprehensive Analysis of Mandibular Residual Asymmetry after Bilateral Sagittal Split Ramus Osteotomy Correction of Menton Point Deviation. PLoS ONE 2016, 11, e0161601. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-W.; Wang, Y.-C.; Chen, Y.-H.; Ko, E.-C. Dentoskeletal parameters related to visual perception of facial asymmetry in patients with skeletal class III malocclusion after orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2018, 47, 48–56. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Yao, C.-C.; Chang, Z.-C.; Lai, H.-H.; Lu, S.-C.; Kok, S.-H. A new classification of mandibular asymmetry and evaluation of surgical-orthodontic treatment outcomes in Class III malocclusion. J. Cranio-Maxillofacial Surg. 2016, 44, 676–683. [Google Scholar] [CrossRef]
- Chen, Y.J.; Yao, C.C.; Chang, Z.C.; Lai, H.H.; Yeh, K.J.; Kok, S.H. Characterization of facial asymmetry in skeletal Class III malocclusion and its implications for treatment. Int. J. Oral Maxillofac. Surg. 2019, 48, 1533–1541. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hunsuck, E.E. A modified intraoral sagittal splitting technic for correction of mandibular prognathism. J. Oral Surg. 1968, 26, 49–52. [Google Scholar]
- Chu, Y.-M.; Bergeron, L.; Chen, Y.-R. Bimaxillary protrusion: An overview of the surgical-orthodontic treatment. In Seminars in Plastic Surgery, 32; Thieme Medical Publishers: New York, NY, USA, 2009. [Google Scholar] [CrossRef]
- Morris, D.E.; Moaveni, Z.; Lo, L.-J. Aesthetic Facial Skeletal Contouring in the Asian Patient. Clin. Plast. Surg. 2007, 34, 547–556. [Google Scholar] [CrossRef]
- Honda, T.; Lin, C.-H.; Yu, C.-C.; Heller, F.; Chen, Y.-R. The Medial Surface of the Mandible as an Alternative Source of Bone Grafts in Orthognathic Surgery. J. Craniofacial Surg. 2005, 16, 123–128. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, G. Statistical methods for medical and biological students. Br. Med. J. 1940, 14, 358–359. [Google Scholar]
- Kwon, T.-G.; Park, H.-S.; Ryoo, H.-M.; Lee, S.-H. A comparison of craniofacial morphology in patients with and without facial asymmetry—A three-dimensional analysis with computed tomography. Int. J. Oral Maxillofac. Surg. 2006, 35, 43–48. [Google Scholar] [CrossRef]
- Van Keulen, C.; Martens, G.; Dermaut, L. Unilateral posterior crossbite and chin deviation: Is there a correlation? Eur. J. Orthod. 2004, 26, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Thiesen, G.; Gribel, B.F.; Freitas, M.P.M.; Oliver, D.R.; Kim, K.B. Mandibular asymmetries and associated factors in orthodontic and orthognathic surgery patients. Angle Orthod. 2018, 88, 545–551. [Google Scholar] [CrossRef]
- Thiesen, G.; Gribel, B.F.; Freitas, M.P. Facial asymmetry: A current review. Dent. Press J. Orthod. 2015, 20, 110–125. [Google Scholar] [CrossRef]
- Walter, J.M., Jr.; Gregg, J.M. Analysis of postsurgical neurologic alteration in the trigeminal nerve. Oral Surg. 1979, 37, 410–414. [Google Scholar]
- Westermark, A.; Bystedt, H.; Konow, L.V. Patients’ evaluation of the final result of sagittal split osteotomy: Is it influenced by impaired sensitivity of the lower lip and chin? Orthodon. Orthognath. Surg. 1999, 14, 135–139. [Google Scholar]
- Ghali, G.; Sikes, J. Intraoral vertical ramus osteotomy as the preferred treatment for mandibular prognathism. J. Oral Maxillofac. Surg. 2000, 58, 313–315. [Google Scholar] [CrossRef]
- Wolford, L.M. The sagittal split ramus osteotomy as the preferred treatment for mandibular prognathism. J. Oral Maxillofac. Surg. 2000, 58, 310–312. [Google Scholar] [CrossRef]
- Pan, J.-H.; Lee, J.-J.; Lin, H.-Y.; Chen, Y.-J.; Yao, C.-C.J.; Kok, S.-H. Transverse and sagittal angulations of proximal segment after sagittal split and vertical ramus osteotomies and their influence on the stability of distal segment. J. Formos. Med. Assoc. 2013, 112, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Park, T.-J.; Jeon, J.-H. Unilateral intraoral vertical ramus osteotomy and sagittal split ramus osteotomy for the treatment of asymmetric mandibles. J. Korean Assoc. Oral Maxillofac. Surg. 2015, 41, 102–108. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).