
Clinical Outcome of Class I and II Restorations with and without an Intermediary Layer of a Flowable Composite after 24 Months: A Prospective, Randomized, Split-Mouth-Designed, Controlled and Single-Blinded Clinical Trial




Abstract
1. Introduction
- The main objective of this study was to investigate the impact of an additional use of a flowable composite layer (Grandio®SO Heavy Flow) in combination with a nano-hybrid composite (Grandio®SO) on the clinical success of Class I and II restorations.
- The differences in different criteria (secondary caries, tooth vitality, postoperative sensitivity, filling integrity/fracture, proximal contact, surface roughness, marginal adaption, marginal discoloration, and color match) should be identified.
- Is the dentin-bonding system Futurabond® DC (VOCO GmbH, Cuxhaven, Germany) used in the self-etch modus capable of ensuring a long-lasting seal of the fillings in the enamel and dentin over time? Can Futurabond® DC effectively prevent postoperative pain?
- How does the nano-hybrid composite Grandio®SO, which has been on the market since 2010, perform in terms of abrasion, shade stability, and surface roughness in occlusal-loaded Class I and II cavities?
2. Materials and Methods
2.1. Study Design
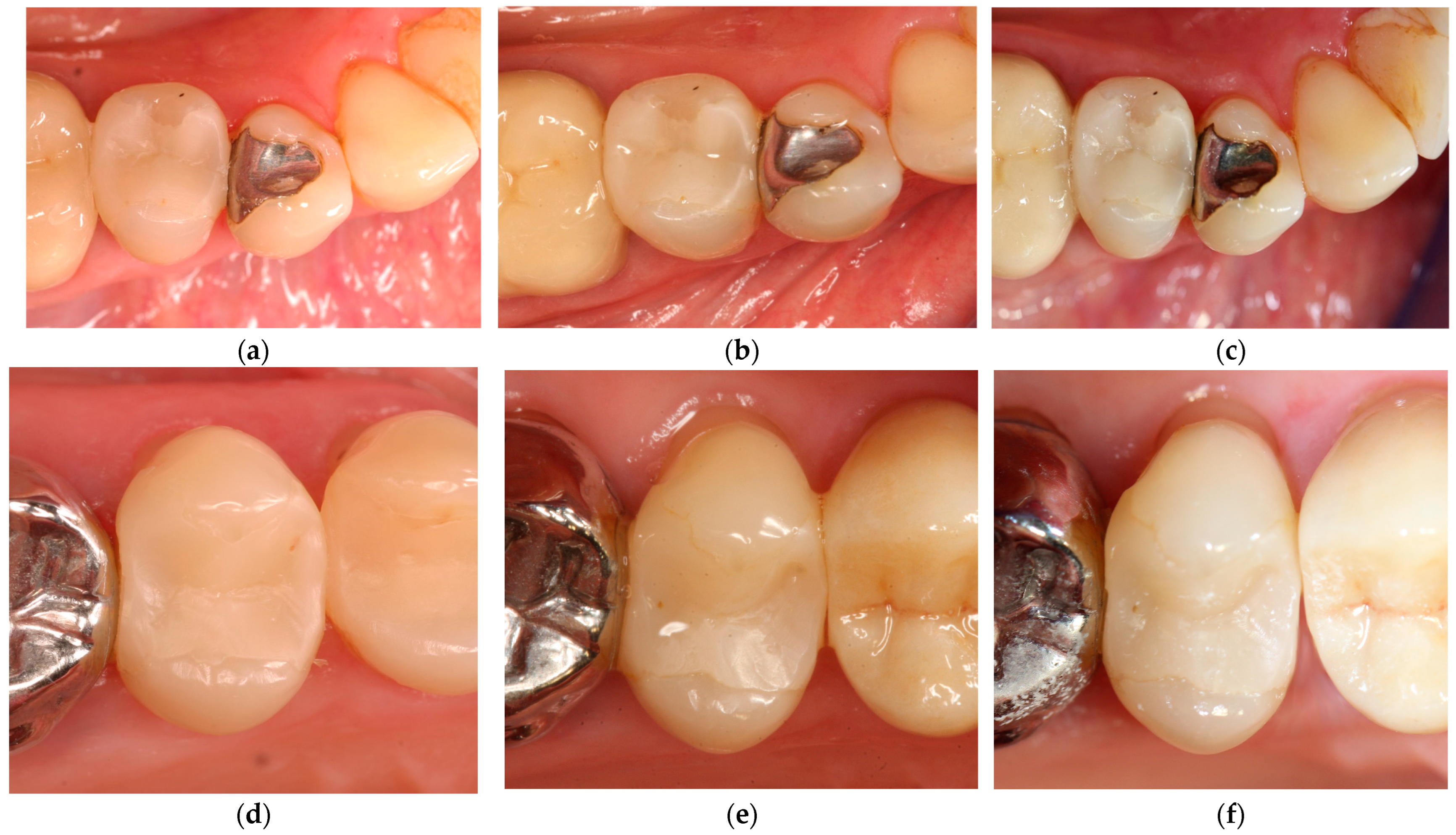
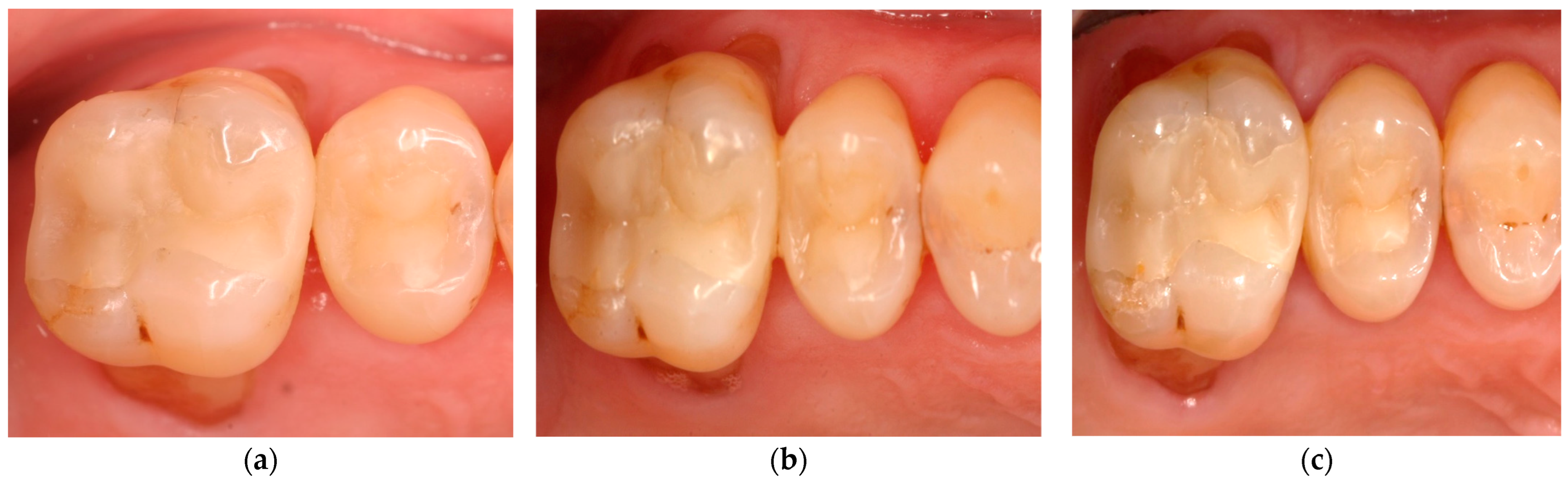
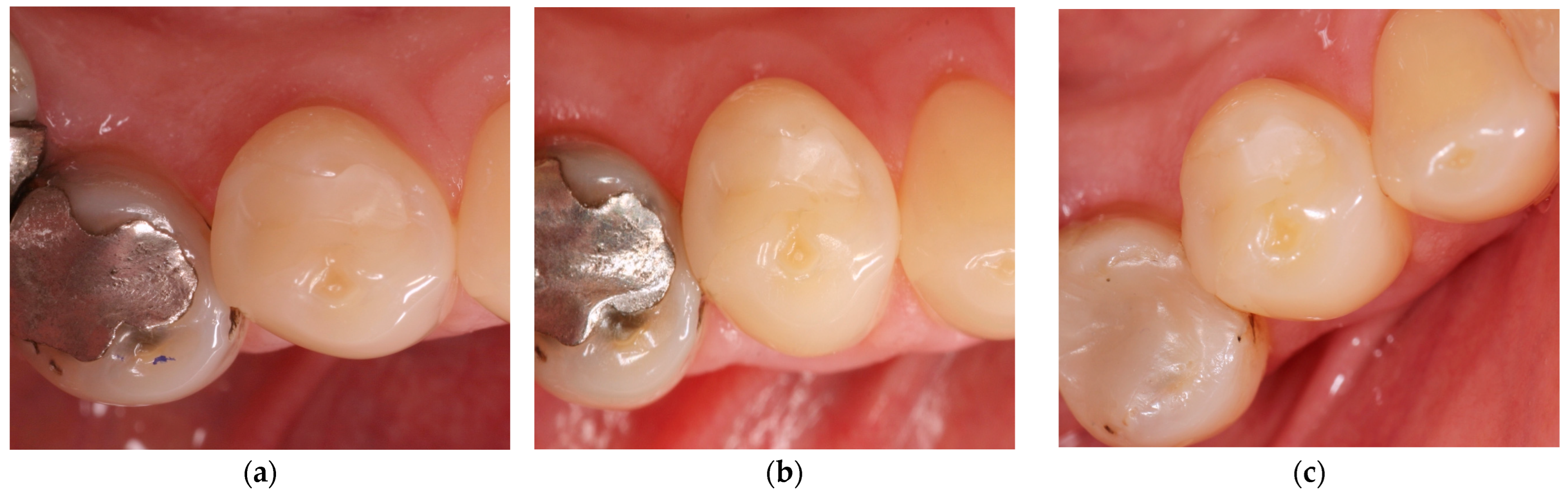
2.2. Clinical Procedure
2.3. Report (Baseline, 6 Months, 12 Months, 24 Months)
2.4. Statistical Analysis
3. Results
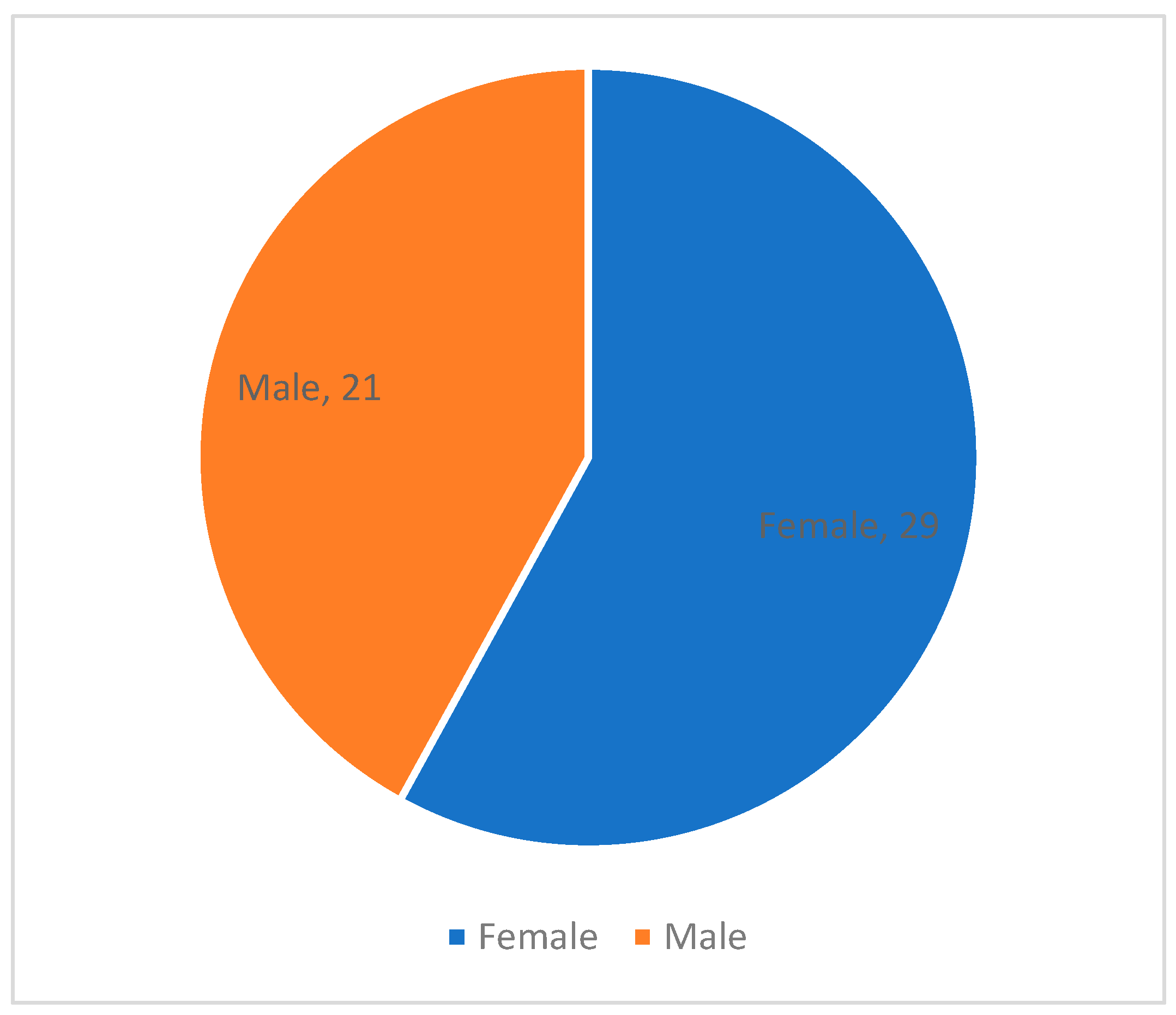
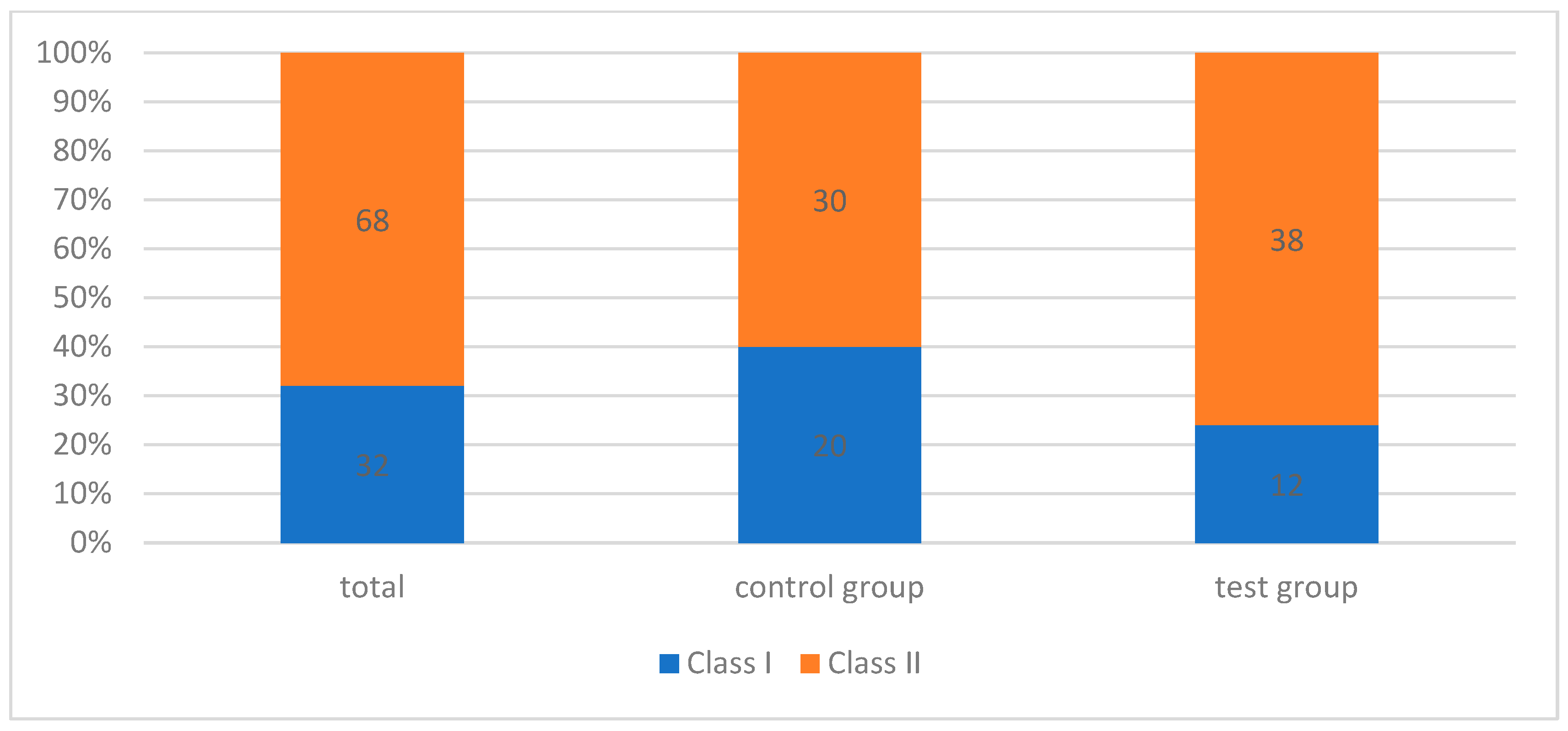
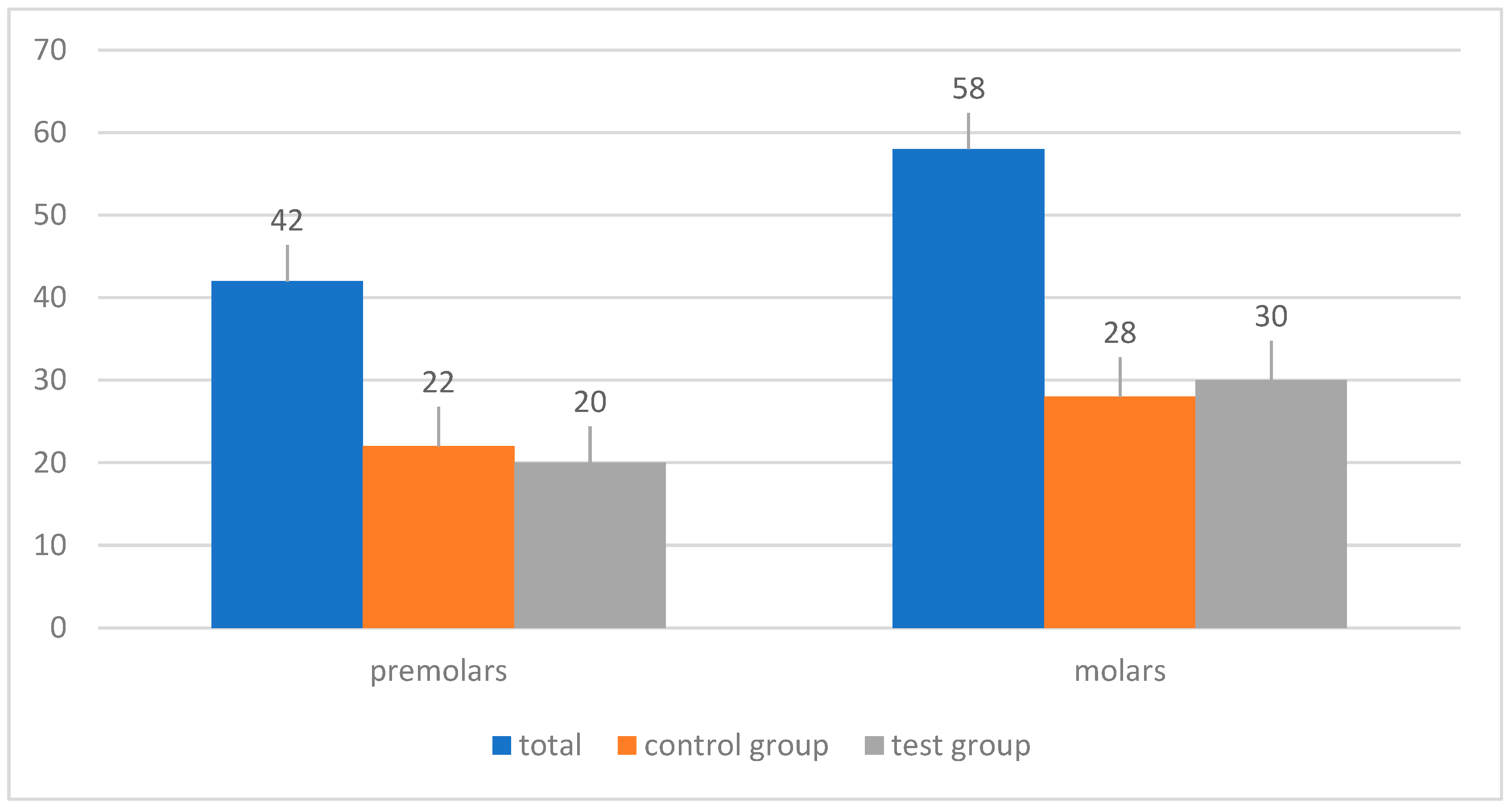
3.1. Study Population
3.2. Success after 24 Months
3.3. Secondary Caries
3.4. Tooth Vitality
3.5. Postoperative Sensitivity
3.6. Filling Integrity/Fracture
3.7. Marginal Discoloration
3.8. Other Parameters
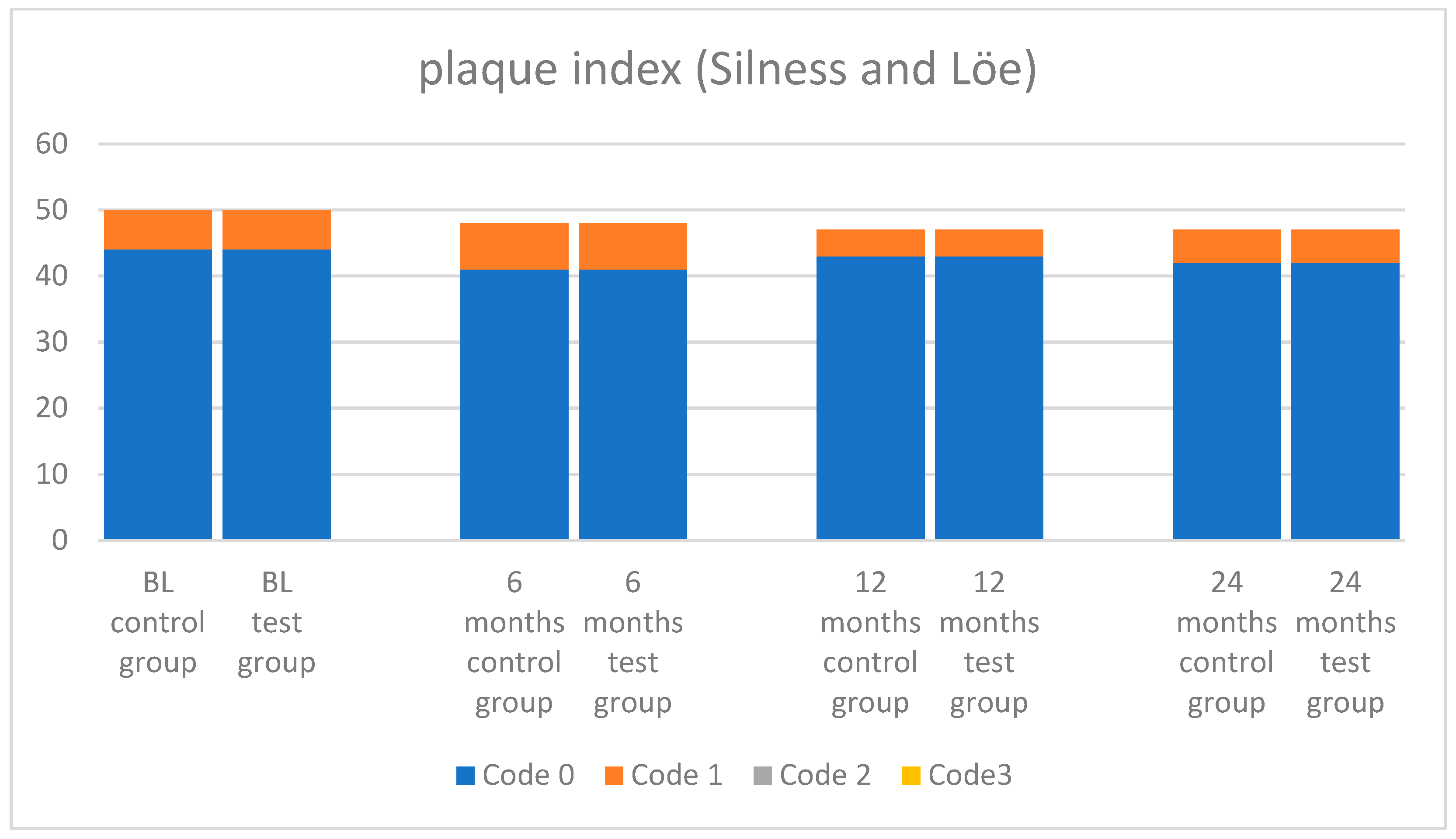
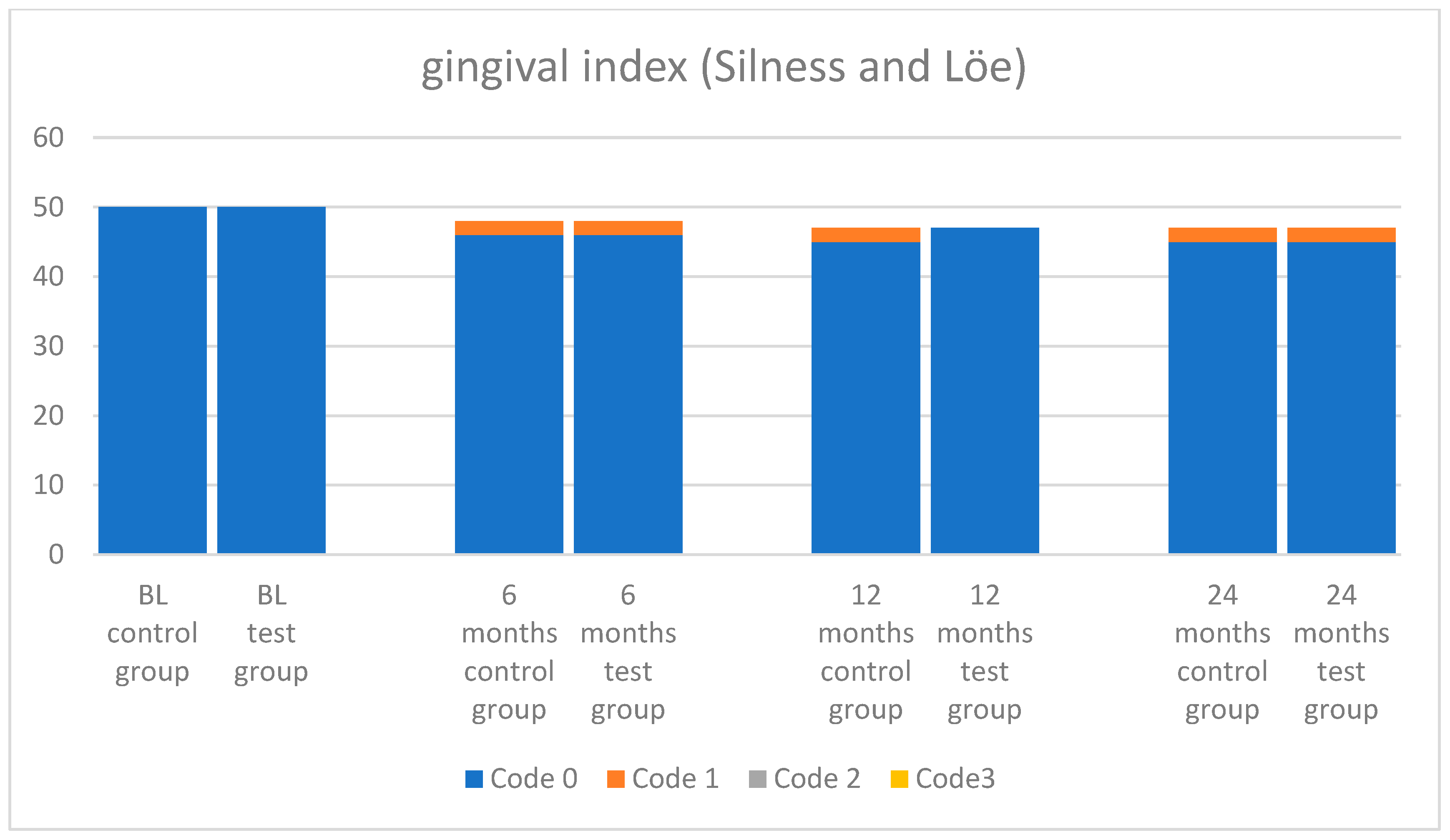
3.9. Plaque and Ginigval Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boeckler, A.; Schaller, H.G.; Gernhardt, C.R. A prospective, double-blind, randomized clinical trial of a one-step, self-etch adhesive with and without an intermediary layer of a flowable composite: A 2-year evaluation. Quintessence Int. 2012, 43, 279–286. [Google Scholar] [PubMed]
- Dietschi, D.; Olsburgh, S.; Krejci, I.; Davidson, C. In vitro evaluation of marginal and internal adaptation after occlusal stressing of indirect class II composite restorations with different resinous bases. Eur. J. Oral Sci. 2003, 111, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Veloso, S.R.M.; Lemos, C.A.A.; de Moraes, S.L.D.; do Egito Vasconcelos, B.C.; Pellizzer, E.P.; de Melo Monteiro, G.Q. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: A systematic review and meta-analysis. Clin. Oral Investig. 2019, 23, 221–233. [Google Scholar] [CrossRef]
- Aggarwal, V.; Singla, M.; Yadav, S.; Yadav, H. Effect of flowable composite liner and glass ionomer liner on class II gingival marginal adaptation of direct composite restorations with different bonding strategies. J. Dent. 2014, 42, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Sarrett, D.C. Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent. Mater. 2005, 21, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Boruziniat, A.; Gharaee, S.; Sarraf Shirazi, A.; Majidinia, S.; Vatanpour, M. Evaluation of the efficacy of flowable composite as lining material on microleakage of composite resin restorations: A systematic review and meta-analysis. Quintessence Int. 2016, 47, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.F.; Liu, J.K.; Chao, C.C.; Liao, F.P.; Chen, Y.H. Effects of flowable composite lining and operator experience on microleakage and internal voids in class II composite restorations. J. Prosthet. Dent. 2001, 85, 177–183. [Google Scholar] [CrossRef]
- Leevailoj, C.; Cochran, M.A.; Matis, B.A.; Moore, B.K.; Platt, J.A. Microleakage of posterior packable resin composites with and without flowable liners. Oper. Dent. 2001, 26, 302–307. [Google Scholar]
- Szesz, A.; Parreiras, S.; Martini, E.; Reis, A.; Loguercio, A. Effect of flowable composites on the clinical performance of non-carious cervical lesions: A systematic review and meta-analysis. J. Dent. 2017, 65, 11–21. [Google Scholar] [CrossRef]
- Sadeghi, M.; Lynch, C.D. The effect of flowable materials on the microleakage of Class II composite restorations that extend apical to the cemento-enamel junction. Oper. Dent. 2009, 34, 306–311. [Google Scholar] [CrossRef]
- Labella, R.; Lambrechts, P.; Van Meerbeek, B.; Vanherle, G. Polymerization shrinkage and elasticity of flowable composites and filled adhesives. Dent. Mater. 1999, 15, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Al Sunbul, H.; Silikas, N.; Watts, D.C. Polymerization shrinkage kinetics and shrinkage-stress in dental resin-composites. Dent. Mater. 2016, 32, 998–1006. [Google Scholar] [CrossRef]
- Korkmaz, Y.; Ozel, E.; Attar, N. Effect of flowable composite lining on microleakage and internal voids in Class II composite restorations. J. Adhes. Dent. 2007, 9, 189–194. [Google Scholar] [PubMed]
- Jager, S.; Balthazard, R.; Dahoun, A.; Mortier, E. Filler Content, Surface Microhardness, and Rheological Properties of Various Flowable Resin Composites. Oper. Dent. 2016, 41, 655–665. [Google Scholar] [CrossRef]
- Geurtsen, W.; Schoeler, U. A 4-year retrospective clinical study of Class I and Class II composite restorations. J. Dent. 1997, 25, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Swift, E.J., Jr.; Ritter, A.V.; Heymann, H.O.; Sturdevant, J.R.; Wilder, A.D., Jr. 36-month clinical evaluation of two adhesives and microhybrid resin composites in Class I restorations. Am. J. Dent. 2008, 21, 148–152. [Google Scholar] [PubMed]
- Sagsoz, O.; Ilday, N.O.; Karatas, O.; Cayabatmaz, M.; Parlak, H.; Olmez, M.H.; Demirbuga, S. The bond strength of highly filled flowable composites placed in two different configuration factors. J. Conserv. Dent. 2016, 19, 21. [Google Scholar] [CrossRef]
- Torres, C.R.G.; Rêgo, H.M.C.; Perote, L.C.C.C.; Santos, L.F.T.F.; Kamozaki, M.B.B.; Gutierrez, N.C.; Di Nicoló, R.; Borges, A.B. A split-mouth randomized clinical trial of conventional and heavy flowable composites in class II restorations. J. Dent. 2014, 42, 793–799. [Google Scholar] [CrossRef]
- Ryge, G. Clinical criteria. Int. Dent. J. 1980, 30, 347–358. [Google Scholar]
- Ryge, G.; Snyder, M. Evaluating the clinical quality of restorations. J. Am. Dent. Assoc. 1973, 87, 369–377. [Google Scholar] [CrossRef]
- Estay, J.; Martín, J.; Vildosola, P.; Mjor, I.A.; Oliveira, O.B., Jr.; Andrade, M.F.; Moncada, G.; Gordan, V.V.; Fernández, E. Effect of Refurbishing Amalgam and Resin Composite Restorations After 12 Years: Controlled Clinical Trial. Oper. Dent. 2017, 42, 587–595. [Google Scholar] [CrossRef]
- Loe, H.; Silness, J. Periodontal Disease in Pregnancy I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef]
- Silness, J.; Loe, H. Periodontal Disease in Pregnancy II. Correlation Between Oral Hygiene and Periodontal Condition. Acta Odontol. Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.G.; Romano, A.R.; Correa, M.B.; Demarco, F.F. Influence of microleakage, surface roughness and biofilm control on secondary caries formation around composite resin restorations: An in situ evaluation. J. Appl. Oral Sci. 2009, 17, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef]
- Hatirli, H.; Yasa, B.; Çelik, E.U. Clinical performance of high-viscosity glass ionomer and resin composite on minimally invasive occlusal restorations performed without rubber-dam isolation: A two-year randomised split-mouth study. Clin. Oral Investig. 2021, 25, 5493–5503. [Google Scholar] [CrossRef] [PubMed]
- Pandis, N.; Walsh, T.; Polychronopoulou, A.; Katsaros, C.; Eliades, T. Split-mouth designs in orthodontics: An overview with applications to orthodontic clinical trials. Eur. J. Orthod. 2013, 35, 783–789. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.M. Randomized controlled trials. Plast. Reconstr. Surg. 2011, 127, 1707–1712. [Google Scholar] [CrossRef]
- Bhide, A.; Shah, P.S.; Acharya, G. A simplified guide to randomized controlled trials. Acta Obstet. Gynecol. Scand. 2018, 97, 380–387. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Curran, A.E.; Voelker, H.T.; Kingman, A. Randomized controlled trials: What are they and who needs them? Periodontol 2000. 2012, 59, 14–31. [Google Scholar] [CrossRef]
- Ernst, C.-P.; Canbek, K.; Aksogan, K.; Willershausen, B. Two-year clinical performance of a packable posterior composite with and without a flowable composite liner. Clin. Oral Investig. 2003, 7, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Szalewski, L.; Szalewska, M.; Jarosz, P.; Woś, M.; Szymańska, J. Temperature Changes in Composite Materials during Photopolymerization. Appl. Sci. 2021, 11, 474. [Google Scholar] [CrossRef]
- Scolavino, S.; Paolone, G.; Orsini, G.; Devoto, W.; Putignano, A. The Simultaneous Modeling Technique: Closing gaps in posteriors. Int. J. Esthet. Dent. 2016, 11, 58–81. [Google Scholar] [PubMed]
- Nair, M.; Gurunathan, D. Clinical and Radiographic Outcomes of Calcium Hydroxide vs Other Agents in Indirect Pulp Capping of Primary Teeth: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2019, 12, 437–444. [Google Scholar] [CrossRef]
- Gyanendra, K.; Dhillon, J.K. Comparative evaluation of clinical outcome of indirect pulp treatment with calcium hydroxide, calcium silicate and Er, Cr: YSGG laser in permanent molars. Laser Ther. 2019, 28, 123–130. [Google Scholar] [CrossRef]
- Berkowitz, G.; Spielman, H.; Matthews, A.; Vena, D.; Craig, R.; Curro, F.; Thompson, V. Postoperative hypersensitivity and its relationship to preparation variables in Class I resin-based composite restorations: Findings from the practitioners engaged in applied research and learning (PEARL) Network. Part 1. Compend. Contin. Educ. Dent. 2013, 34, e44–e52. [Google Scholar] [CrossRef]
- Sancakli, H.S.; Yildiz, E.; Bayrak, I.; Ozel, S. Effect of different adhesive strategies on the post-operative sensitivity of class I composite restorations. Eur. J. Dent. 2014, 8, 15–22. [Google Scholar] [CrossRef]
- Scotti, N.; Bergantin, E.; Giovannini, R.; Delbosco, L.; Breschi, L.; Migliaretti, G.; Pasqualini, D.; Berutti, E. Influence of multi-step etch-and-rinse versus self-etch adhesive systems on the post-operative sensitivity in medium-depth carious lesions: An in vivo study. Am. J. Dent. 2015, 28, 214–218. [Google Scholar]
- Reis, A.; Dourado Loguercio, A.; Schroeder, M.; Luque-Martinez, I.; Masterson, D.; Cople Maia, L. Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations?: A systematic review and meta-analysis. Dent. Mater. 2015, 31, 1052–1067. [Google Scholar] [CrossRef]
- Bekes, K.; Boeckler, L.; Gernhardt, C.R.; Schaller, H.G. Clinical performance of a self-etching and a total-etch adhesive system - 2-year results. J. Oral Rehabil. 2007, 34, 855–861. [Google Scholar] [CrossRef]
- Boeckler, A.; Boeckler, L.; Eppendorf, K.; Schaller, H.G.; Gernhardt, C.R. A prospective, randomized clinical trial of a two-step self-etching vs two-step etch-and-rinse adhesive and SEM margin analysis: Four-year results. J. Adhes. Dent. 2012, 14, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Kotousov, A.; Borkowski, K. Effect of material properties on stresses at the restoration-dentin interface of composite restorations during polymerization. Dent. Mater. 2006, 22, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Bottenberg, P.; Jacquet, W.; Alaerts, M.; Keulemans, F. A prospective randomized clinical trial of one bis-GMA-based and two ormocer-based composite restorative systems in class II cavities: Five-year results. J. Dent. 2009, 37, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Manhart, J.; Chen, H.Y.; Hickel, R. Clinical evaluation of the posterior composite Quixfil in class I and II cavities: 4-year follow-up of a randomized controlled trial. J. Adhes. Dent. 2010, 12, 237–243. [Google Scholar] [CrossRef]
- Armstrong, S.R.; Vargas, M.A.; Chung, I.; Pashley, D.H.; Campbell, J.A.; Laffoon, J.E.; Qian, F. Resin-dentin interfacial ultrastructure and microtensile dentin bond strength after five-year water storage. Oper. Dent. 2004, 29, 705–712. [Google Scholar]
- Efes, B.G.; Dorter, C.; Gomec, Y. Clinical evaluation of an ormocer, a nanofill composite and a hybrid composite at 2 years. Am. J. Dent. 2006, 19, 236–240. [Google Scholar]
- Frankenberger, R.; Tay, F.R. Self-etch vs etch-and-rinse adhesives: Effect of thermo-mechanical fatigue loading on marginal quality of bonded resin composite restorations. Dent. Mater. 2005, 21, 397–412. [Google Scholar] [CrossRef]
- Van Meerbeek, B.; Yoshihara, K.; Yoshida, Y.; Mine, A.; De Munck, J.; Van Landuyt, K.L. State of the art of self-etch adhesives. Dent. Mater. 2011, 27, 17–28. [Google Scholar] [CrossRef]
- Giannini, M.; Makishi, P.; Ayres, A.P.; Vermelho, P.M.; Fronza, B.M.; Nikaido, T.; Tagami, J. Self-etch adhesive systems: A literature review. Braz. Dent. J. 2015, 26, 3–10. [Google Scholar] [CrossRef]
- Worthington, H.V.; Khangura, S.; Seal, K.; Mierzwinski-Urban, M.; Veitz-Keenan, A.; Sahrmann, P.; Schmidlin, P.R.; Davis, D.; Iheozor-Ejiofor, Z.; Rasines Alcaraz, M.G. Direct composite resin fillings versus amalgam fillings for permanent posterior teeth. Cochrane Database Syst. Rev. 2021, 8, CD005620. [Google Scholar] [CrossRef]
- Szalewski, L.; Wójcik, D.; Sofińska-Chmiel, W.; Kuśmierz, M.; Różyło-Kalinowska, I. How the Duration and Mode of Photopolymerization Affect the Mechanical Properties of a Dental Composite Resin. Materials. 2023, 16, 113. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Jepsen, S.; Albers, H.K.; Eberhard, J. Flowable materials as an intermediate layer could improve the marginal and internal adaptation of composite restorations in Class-V-cavities. Dent. Mater. 2006, 22, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Neme, A.M.; Maxson, B.B.; Pink, F.E.; Aksu, M.N. Microleakage of Class II packable resin composites lined with flowables: An in vitro study. Oper. Dent. 2002, 27, 600–605. [Google Scholar]
- Tredwin, C.J.; Stokes, A.; Moles, D.R. Influence of flowable liner and margin location on microleakage of conventional and packable class II resin composites. Oper. Dent. 2005, 30, 32–38. [Google Scholar]
- Shaalan, O.O.; Abou-Auf, E.; El Zoghby, A.F. Clinical evaluation of flowable resin composite versus conventional resin composite in carious and noncarious lesions: Systematic review and meta-analysis. J. Conserv. Dent. 2017, 20, 380–385. [Google Scholar] [CrossRef]
- Badr, C.; Spagnuolo, G.; Amenta, F.; Khairallah, C.; Mahdi, S.S.; Daher, E.; Battineni, G.; Baba, N.Z.; Zogheib, T.; Qasim, S.S.B.; et al. A Two-Year Comparative Evaluation of Clinical Performance of a Nanohybrid Composite Resin to a Flowable Composite Resin. J. Funct. Biomater. 2021, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Diniz, A.C.; Bandeca, M.C.; Pinheiro, L.M.; Dos Santosh Almeida, L.J., Jr.; Torres, C.R.; Borges, A.H.; Pinto, S.C.; Tonetto, M.R.; De Jesus Tavarez, R.R.; Firoozmand, L.M. Influence of Different Etching Modes on Bond Strength to Enamel using Universal Adhesive Systems. J. Contemp. Dent. Pract. 2016, 17, 820–825. [Google Scholar] [CrossRef]
- Rosa, W.L.; Piva, E.; Silva, A.F. Bond strength of universal adhesives: A systematic review and meta-analysis. J. Dent. 2015, 43, 765–776. [Google Scholar] [CrossRef]
- Abdalla, A.I.; El Zohairy, A.A.; Abdel Mohsen, M.M.; Feilzer, A.J. Bond efficacy and interface morphology of self-etching adhesives to ground enamel. J. Adhes. Dent. 2010, 12, 19–25. [Google Scholar] [CrossRef]
- Taneja, S.; Kumari, M.; Bansal, S. Effect of saliva and blood contamination on the shear bond strength of fifth-, seventh-, and eighth-generation bonding agents: An in vitro study. J. Conserv. Dent. 2017, 20, 157–160. [Google Scholar] [CrossRef]
- Ástvaldsdóttir, Á.; Dagerhamn, J.; van Dijken, J.W.V.; Naimi-Akbar, A.; Sandborgh-Englund, G.; Tranæus, S.; Nilsson, M. Longevity of posterior resin composite restorations in adults – A systematic review. J. Dent. 2015, 43, 934–954. [Google Scholar] [CrossRef] [PubMed]
- Ersin, N.K.; Candan, U.; Aykut, A.; önçag, ö.; Eronat, C.; Kose, T. A clinical evaluation of resin-based composite and glass ionomer cement restorations placed in primary teeth using the ART approach: Results at 24 months. J. Am. Dent. Assoc. 2006, 137, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, A.; Hogg, C.H.; Dowling, A.H.; Grufferty, B.F.; Benetti, A.R.; Fleming, G.J.P. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J. Dent. 2012, 40, 500–505. [Google Scholar] [CrossRef] [PubMed]
- van Dijken, J.W.; Pallesen, U. Clinical performance of a hybrid resin composite with and without an intermediate layer of flowable resin composite: A 7-year evaluation. Dent. Mater. 2011, 27, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Gerula-Szymańska, A.; Kaczor, K.; Lewusz-Butkiewicz, K.; Nowicka, A. Marginal integrity of flowable and packable bulk fill materials used for class II restorations -A systematic review and meta-analysis of in vitro studies. Dent. Mater. J. 2020, 39, 335–344. [Google Scholar] [CrossRef]
- Cavalheiro, C.P.; Scherer, H.; Imparato, J.C.P.; Collares, F.M.; Lenzi, T.L. Use of flowable resin composite as an intermediate layer in class II restorations: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 5629–5639. [Google Scholar] [CrossRef]
- Ferracane, J.L.; Lawson, N.C. Probing the hierarchy of evidence to identify the best strategy for placing class II dental composite restorations using current materials. J. Esthet. Restor. Dent. 2021, 33, 39–50. [Google Scholar] [CrossRef]
- Leyton, B.S.; Rached, R.N.; Ignácio, S.A.; Souza, E.M. Fracture strength of extended class I composite restorations with different restorative techniques. Odontology. 2022, 110, 269–277. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Grandio®SO Heavy Flow (VOCO GmbH, Cuxhaven, Germany) | Grandio®SO (VOCO GmbH, Cuxhaven, Germany) |
|---|---|---|
| Main components | Monomers: Bis-GMA, Bis-EMA, TEGDMA | Monomers: Bis-GMA, Bis-EMA, TEGDMA |
| Fillers: glass ceramic, functionalized SiO2 nanoparticles | Fillers: glass ceramic, functionalized SiO2 nanoparticles | |
| Filler degree | 83 wt.% = 68 vol.% | 89 wt.% = 73 vol.% |
| Modulus of elasticity | 11,850 MPa | 16,650 MPa |
| Shrinkage | 2.96 =% | 1.61% |
| Compressive strength | 417 MPa | 439 MPa |
| Flexural strength (3 point) | 159 MPa | 187 MPa |
| Surface hardness | 175 MHV | 211 MHV |
| Curing depth (800 mW/cm2) | >2.5 mm/20 s | >2.8 mm/20 s |
| Modified USPHS/Ryge Criteria | ||
|---|---|---|
| Secondary caries | Alpha | No clinical diagnosis of caries along the margin of the restoration |
| Delta | Clinical diagnosis of caries | |
| Tooth vitality | Alpha | Positive |
| Delta | Negative | |
| Postoperative sensitivity | Alpha | No hypersensitivity |
| Bravo | Complaints only for a short time after placement, no treatment necessary | |
| Charlie | Medium complaints, no treatment necessary | |
| Delta | Permanent complaints, bearable, treatment planned | |
| Filling integrity/fracture | Alpha | No chipping, cracking or wear of the filling material |
| Bravo | Chipping (>100 µm), crack formation, detectable with a probe | |
| Charlie | Continuous crack formation, wear > 200 µm | |
| Delta | Bulk fracture of the restoration | |
| Proximal contact | Alpha | Contact is tight, and it is possible to place one metallic matrix band (50 µm) between the restoration and the adjacent tooth |
| Bravo | Contact is slight, and it is possible to pass two metallic matrix bands (50 µm), or contact is too strong (metallic matrix band cannot be placed) | |
| Charlie | Contact is too slight, but no trauma of the papilla | |
| Delta | Trauma of papilla (Food impaction) | |
| Surface roughness | Alpha | Surface is smooth, and the adjacent tissues showed no irritation |
| Bravo | Surface of the restoration is slightly rough or pitted but can be refinished | |
| Charlie | Surface is deeply pitted or shows irregular grooves, which were not related to the natural anatomy and could not be refinished | |
| Delta | Surface is fractured or flaking | |
| Marginal adaptation | Alpha | No visible evidence of a crevice along the margin into which an explorer will catch |
| Bravo | The explorer catches a crevice along the margin, but there is no exposure of dentin or base | |
| Charlie | Visible evidence of a crevice with exposure of dentin or base | |
| Delta | The restoration is fractured, mobile, or missing | |
| Marginal discoloration | Alpha | No existing marginal discoloration at all |
| Bravo | Presence of discoloration at the margins between the restoration and the tooth structure; discoloration does not penetrate along the margins of the restoration toward the pulp | |
| Charlie | The discoloration penetrated along the margins in a pulpal direction | |
| Color match | Alpha | The restoration cannot be detected with a mirror |
| Bravo | The restoration is visible, but there is no mismatch in color, shade, and/or translucency between the restoration and the adjacent tooth structure | |
| Charlie | There is a mismatch in color, shade, or translucency, but not outside the normal range of tooth color, shade, and/or translucency | |
| Delta | The mismatch is outside the normal range of tooth color, shade, and/or translucency | |
| Grade | Plaque Index | Gingival Index |
|---|---|---|
| 0 | No plaque | No swelling |
| 1 | Thin visible plaque, difficult to identify | Mild swelling, no swelling after gentle probing |
| 2 | Thick visible plaque, easily detected | Moderate to severe gingival swelling, bleeding after air drying |
| 3 | Presence of plaque filling the interproximal region | Severe inflammation; redness and edema; ulceration; spontaneous bleeding tendency |
| Parameter | Control Group (n = 47) | Test Group (n = 47) |
|---|---|---|
| Secondary caries | 47 × Code A | 47 × Code A |
| Tooth vitality | 47 × Code A | 44 × Code A; 3 × Code D |
| Postoperative sensitivity | 47 × Code A | 47 × Code A |
| Filling integrity/fracture | 47 × Code A | 45 × Code A; 2 × Code B |
| Proximal contact | 47 × Code A | 47 × Code A |
| Surface roughness | 47 × Code A | 47 × Code A |
| Marginal adaption | 47 × Code A | 46 × Code A; 1 × Code B |
| Marginal discoloration | 45 × Code A; 2 × Code B | 44 × Code A; 3 × Code B |
| Color match | 47 × Code A | 47 × Code A |
| Plaque index | 42 × Index 0; 5 × Index 1 | 42 × Index 0; 5 × Index 1 |
| Gingival index | 45 × Index 0; 2 × Index 1 | 45 × Index 0; 2 × Index 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gernhardt, C.R.; Nguyen, A.D.; Michaelis, M.; Pütz, N. Clinical Outcome of Class I and II Restorations with and without an Intermediary Layer of a Flowable Composite after 24 Months: A Prospective, Randomized, Split-Mouth-Designed, Controlled and Single-Blinded Clinical Trial. Appl. Sci. 2023, 13, 4224. https://doi.org/10.3390/app13074224
Gernhardt CR, Nguyen AD, Michaelis M, Pütz N. Clinical Outcome of Class I and II Restorations with and without an Intermediary Layer of a Flowable Composite after 24 Months: A Prospective, Randomized, Split-Mouth-Designed, Controlled and Single-Blinded Clinical Trial. Applied Sciences. 2023; 13(7):4224. https://doi.org/10.3390/app13074224
Chicago/Turabian StyleGernhardt, Christian Ralf, Anh Duc Nguyen, Mary Michaelis, and Natalie Pütz. 2023. "Clinical Outcome of Class I and II Restorations with and without an Intermediary Layer of a Flowable Composite after 24 Months: A Prospective, Randomized, Split-Mouth-Designed, Controlled and Single-Blinded Clinical Trial" Applied Sciences 13, no. 7: 4224. https://doi.org/10.3390/app13074224
APA StyleGernhardt, C. R., Nguyen, A. D., Michaelis, M., & Pütz, N. (2023). Clinical Outcome of Class I and II Restorations with and without an Intermediary Layer of a Flowable Composite after 24 Months: A Prospective, Randomized, Split-Mouth-Designed, Controlled and Single-Blinded Clinical Trial. Applied Sciences, 13(7), 4224. https://doi.org/10.3390/app13074224