
Oral Mesenchymal Stromal Cells in Systemic Sclerosis: Characterization and Response to a Hyaluronic-Acid-Based Biomaterial

 ,
,  ,
,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Mesenchymal Stem Cell (MSCs) Isolation and Characterization
2.2.1. Isolation of MSCs
2.2.2. Immunophenotype Characterization of MSCs
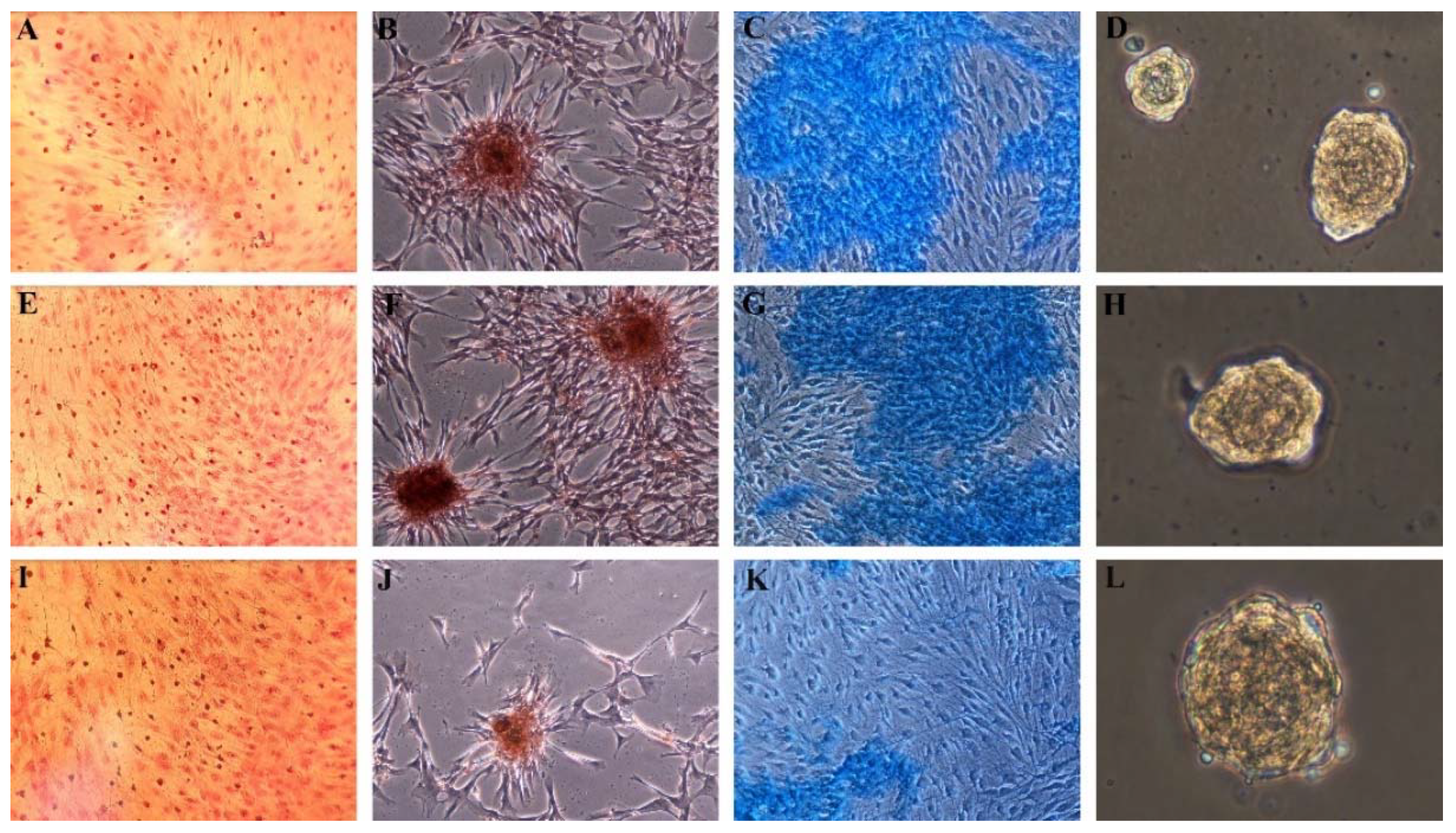
2.2.3. Trilineage Differentiation Assay and Cytochemical Staining
2.2.4. Adipocyte Differentiation
2.2.5. Osteogenic Differentiation
2.2.6. Chondrogenic Differentiation
2.3. Preparation of Experimental Culture Media
2.4. Generation of Aggregates—Spheroids
2.5. Functionality Tests
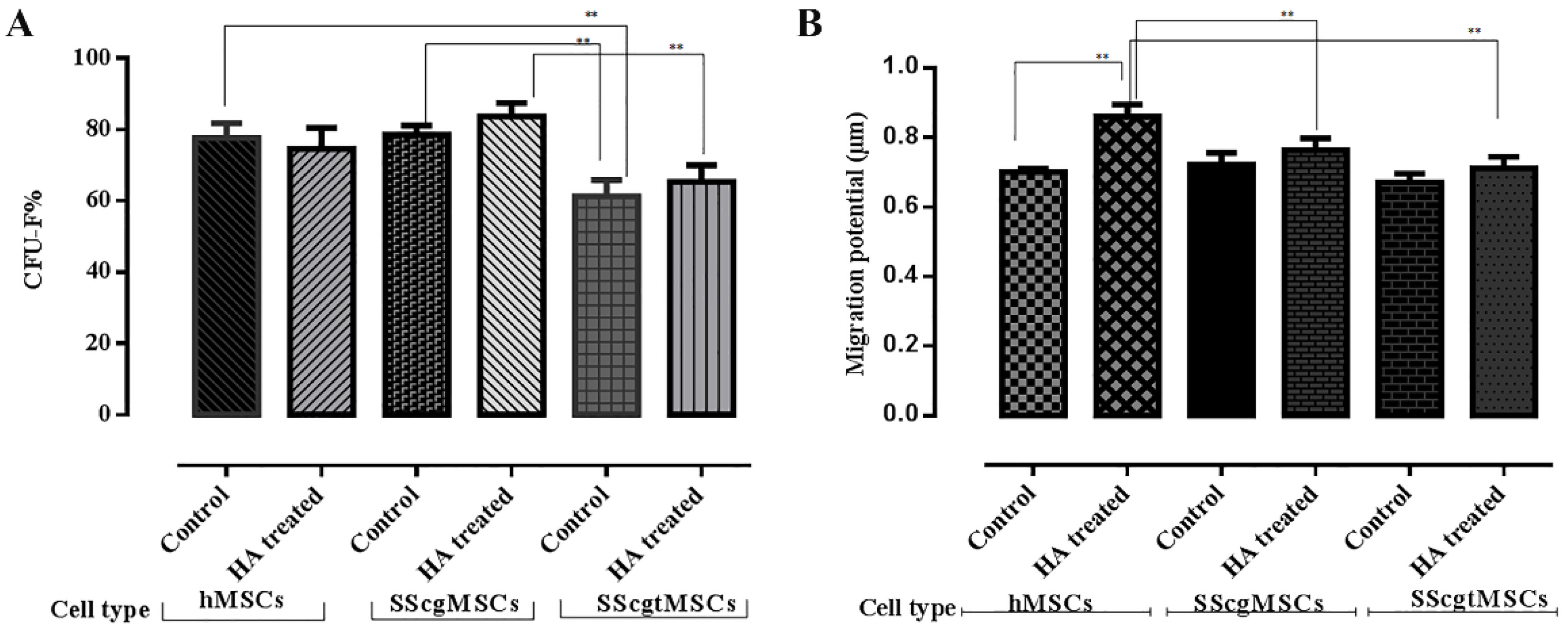
2.5.1. Colony-Forming Unit-Fibroblast (CFU-F) Assay
2.5.2. Migration Potential
2.6. Statistical Analysis
3. Results
3.1. Characterization of MSCs
3.1.1. Surface Markers of MSCs
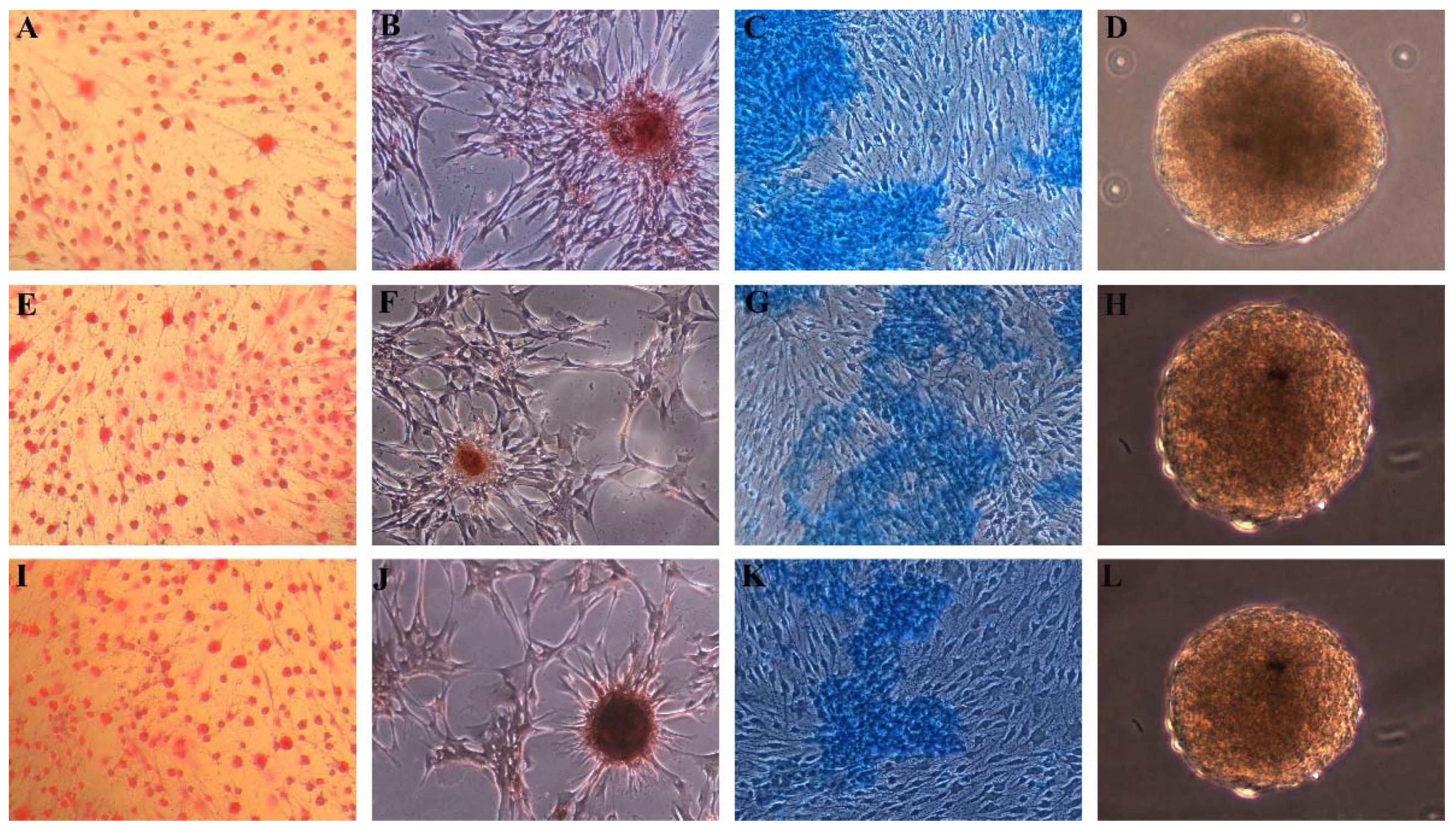
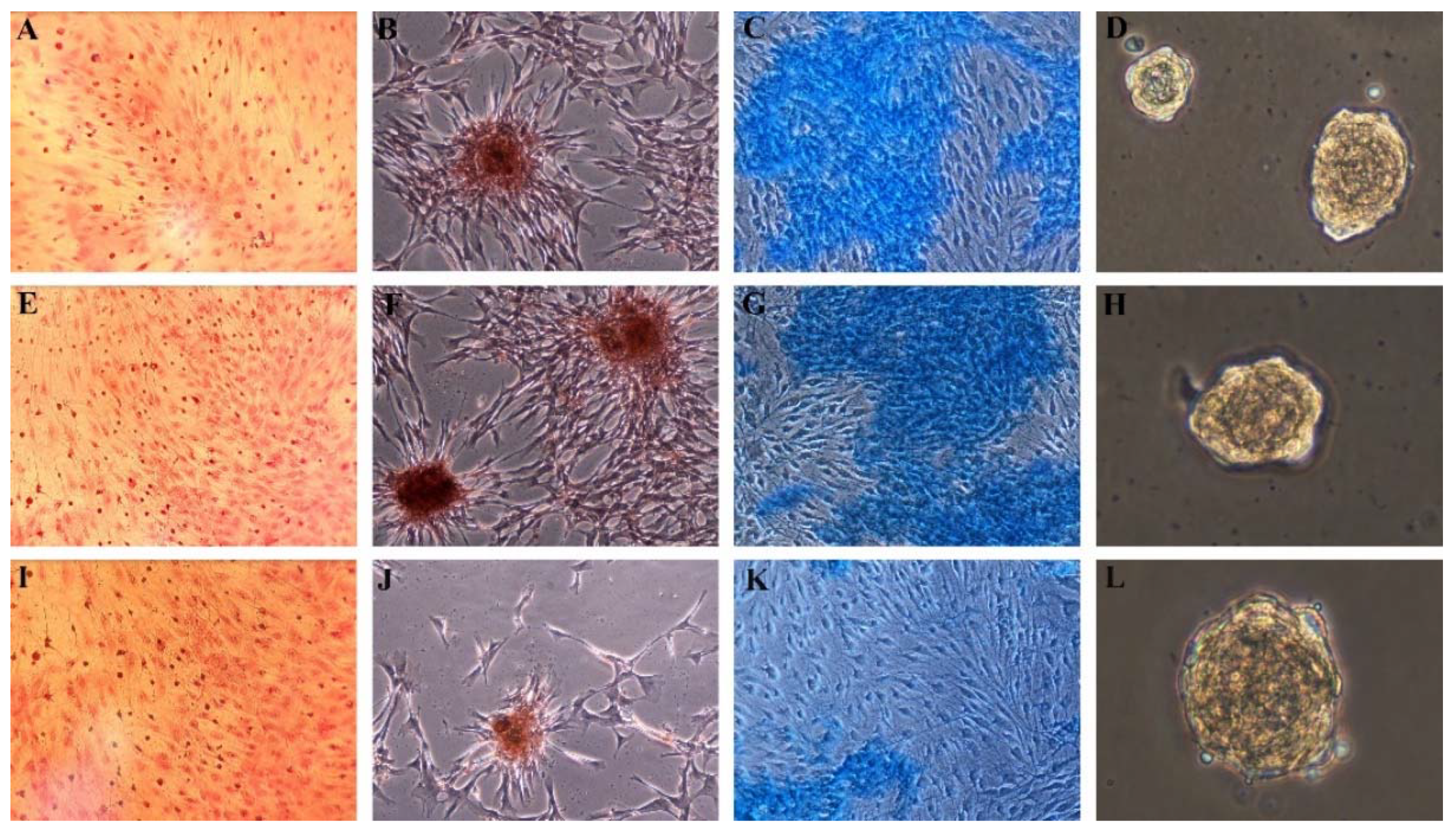
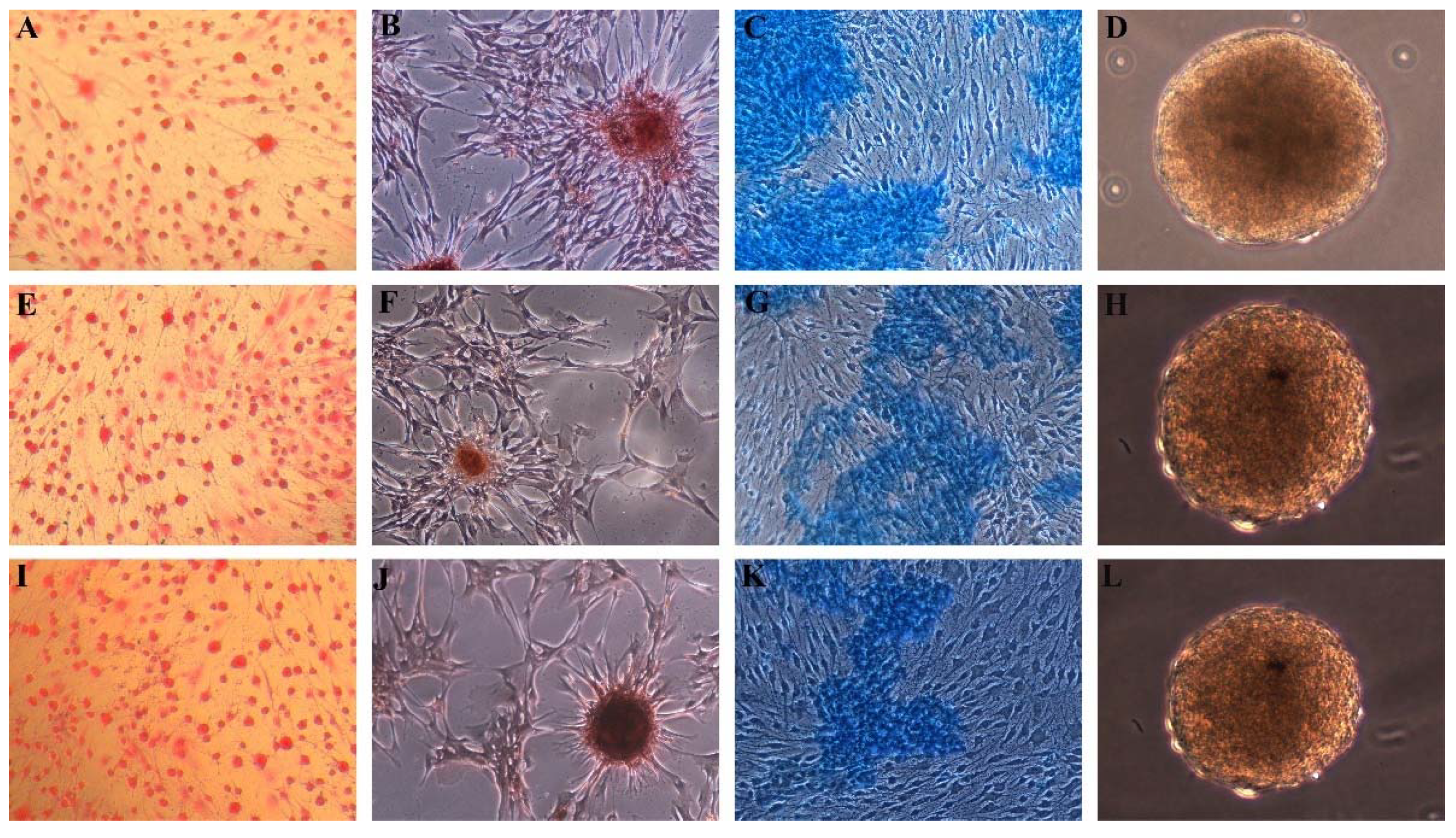
3.1.2. Trilineage Differentiation and Embryonic Body Formation
3.2. Functionality Tests
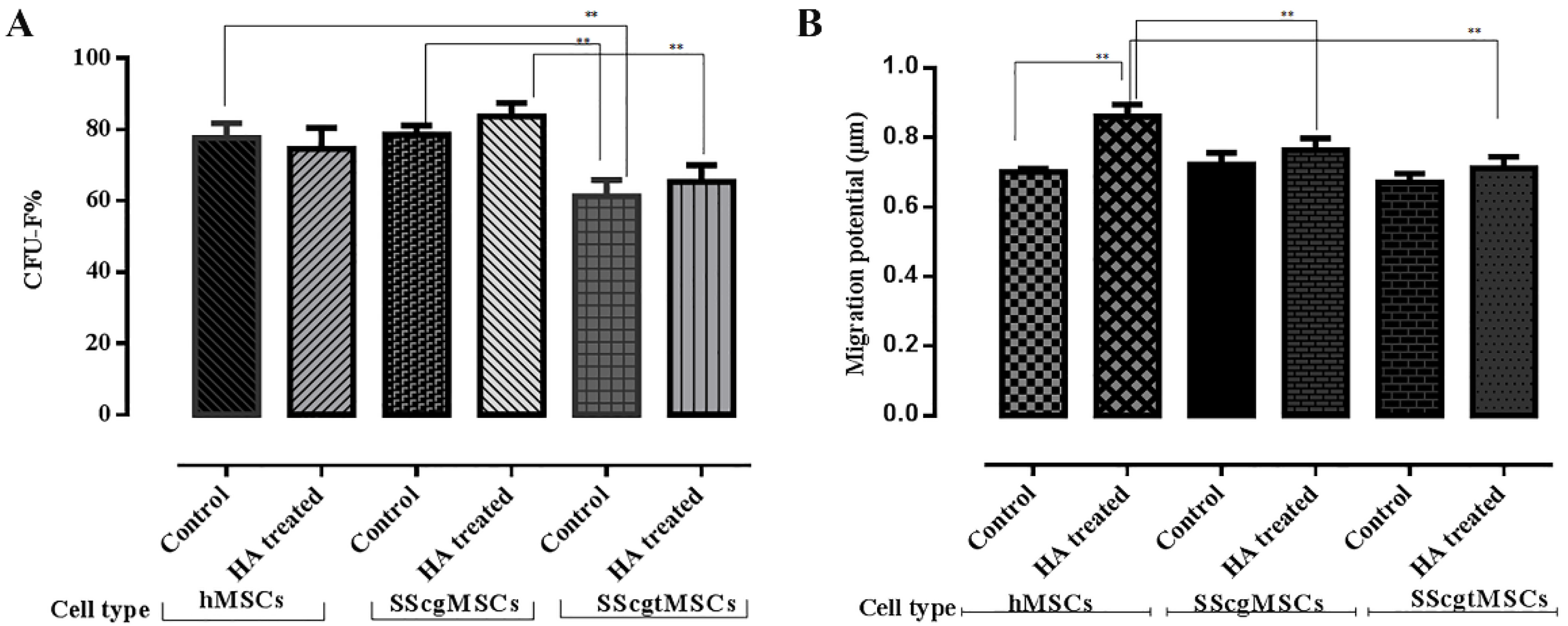
3.2.1. Colony-Forming Unit-Fibroblast (CFU-F) Assay
3.2.2. Migration Potential
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFU-F | Colony-Forming Unit-Fibroblast |
| SSc | Systemic sclerosis |
| SScgMSCs | Gingival MSCs from a SSc patient |
| SScgtMSCs | Granulation tissue MSCs from an SSc patient |
| hMSCs | MSCs from a healthy individual |
| HA | Hyaluronic acid |
| MSCs | Mesenchymal stromal cell |
References
- Jimenez, S.A.; Derk, C.T. Following the Molecular Pathways toward an Understanding of the Pathogenesis of Systemic Sclerosis. Ann. Intern. Med. 2004, 140, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Servettaz, A.; Agard, C.; Tamby, M.C.; Guilpain, P.; Guillevin, L.; Mouthon, L. Systemic sclerosis: Pathophysiology of a multifaceted disease. Presse Med. 2006, 35, 1903–1915. [Google Scholar] [CrossRef]
- Mouthon, L.; Rannou, F.; Bérezné, A.; Pagnoux, C.; Arène, J.-P.; Foïs, E.; Cabane, J.; Guillevin, L.; Revel, M.; Fermanian, J.; et al. Development and Validation of a Scale for Mouth Handicap in Systemic Sclerosis: The Mouth Handicap in Systemic Sclerosis Scale. Ann. Rheum. Dis. 2007, 66, 1651–1655. [Google Scholar] [CrossRef] [Green Version]
- Elimelech, R.; Mayer, Y.; Braun-Moscovici, Y.; Machtei, E.E.; Balbir-Gurman, A. Periodontal Conditions and Tumor Necrosis Factor-Alpha Level in Gingival Crevicular Fluid of Scleroderma Patients. Isr. Med. Assoc. J. IMAJ 2015, 17, 549–553. [Google Scholar]
- Leung, W.K.; Chu, C.H.; Mok, M.Y.; Yeung, K.S.; Ng, S.K. Periodontal Status of Adults with Systemic Sclerosis: Case-Control Study. J. Periodontol. 2011, 82, 1140–1145. [Google Scholar] [CrossRef]
- Pischon, N.; Hoedke, D.; Kurth, S.; Lee, P.; Dommisch, H.; Steinbrecher, A.; Pischon, T.; Burmester, G.R.; Buttgereit, F.; Detert, J.; et al. Increased Periodontal Attachment Loss in Patients with Systemic Sclerosis. J. Periodontol. 2016, 87, 763–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veale, B.J.; Jablonski, R.Y.; Frech, T.M.; Pauling, J. Orofacial manifestations of systemic sclerosis. Br. Dent. J. 2016, 221, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Martin, T.; Schmittbuhl, M.; Huck, O. The spectrum of orofacial manifestations in systemic sclerosis: A challenging management. Oral Dis. 2017, 23, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Scardina, G.; Pizzigatti, M.; Messina, P. Periodontal Microcirculatory Abnormalities in Patients with Systemic Sclerosis. J. Periodontol. 2005, 76, 1991–1995. [Google Scholar] [CrossRef] [PubMed]
- Duscher, D.; Barrera, J.F.; Wong, V.W.; Maan, Z.; Whittam, A.J.; Januszyk, M.; Gurtner, G.C. Stem Cells in Wound Healing: The Future of Regenerative Medicine? A Mini-Review. Gerontology 2015, 62, 216–225. [Google Scholar] [CrossRef]
- Del Papa, N.; Quirici, N.; Soligo, D.; Scavullo, C.; Cortiana, M.; Borsotti, C.; Maglione, W.; Comina, D.P.; Vitali, C.; Fraticelli, P.; et al. Bone marrow endothelial progenitors are defective in systemic sclerosis. Arthritis Rheum. 2006, 54, 2605–2615. [Google Scholar] [CrossRef] [Green Version]
- Di Benedetto, P.; Panzera, N.; Cipriani, P.; Mastroiaco, V.; Tessitore, A.; Liakouli, V.; Ruscitti, P.; Berardicurti, O.; Carubbi, F.; Guggino, G.; et al. Mesenchymal stem cells of Systemic Sclerosis patients, derived from different sources, show a profibrotic microRNA profiling. Sci. Rep. 2019, 9, 7144. [Google Scholar] [CrossRef]
- Larghero, J.; Farge, D.; Braccini, A.; Lecourt, S.; Scherberich, A.; Foïs, E.; Verrecchia, F.; Daikeler, T.; Gluckman, E.; Tyndall, A.; et al. Phenotypical and functional characteristics of in vitro expanded bone marrow mesenchymal stem cells from patients with systemic sclerosis. Ann. Rheum. Dis. 2007, 67, 443–449. [Google Scholar] [CrossRef]
- Scuderi, N.; Ceccarelli, S.; Onesti, M.G.; Fioramonti, P.; Guidi, C.; Romano, F.; Frati, L.; Angeloni, A.; Marchese, C. Human Adipose-Derived Stromal Cells for Cell-Based Therapies in the Treatment of Systemic Sclerosis. Cell Transplant. 2013, 22, 779–795. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.R.E.; Laurent, T.C.; Laurent, U.B.G. Hyaluronan: Its nature, distribution, functions and turnover. J. Intern. Med. 1997, 242, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Bertl, K.; Bruckmann, C.; Isberg, P.-E.; Klinge, B.; Gotfredsen, K.; Stavropoulos, A. Hyaluronan in non-surgical and surgical periodontal therapy: A systematic review. J. Clin. Periodontol. 2015, 42, 236–246. [Google Scholar] [CrossRef]
- Carlson, G.A.; Dragoo, J.L.; Samimi, B.; Bruckner, D.A.; Bernard, G.W.; Hedrick, M.; Benhaim, P. Bacteriostatic properties of biomatrices against common orthopaedic pathogens. Biochem. Biophys. Res. Commun. 2004, 321, 472–478. [Google Scholar] [CrossRef]
- Kang, J.-H.; Kim, Y.-Y.; Chang, J.-Y.; Kho, H.-S. Influences of hyaluronic acid on the anticandidal activities of lysozyme and the peroxidase system. Oral Dis. 2011, 17, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Laurent, T.C.; Laurent, U.B.; Fraser, J.R. Functions of hyaluronan. Ann. Rheum. Dis. 1995, 54, 429–432. [Google Scholar] [CrossRef] [Green Version]
- de Brito Bezerra, B.; Mendes Brazão, M.A.; de Campos, M.L.G.; Casati, M.Z.; Sallum, E.A.; Sallum, A.W. Association of Hyaluronic Acid with a Collagen Scaffold May Improve Bone Healing in Critical-Size Bone Defects. Clin. Oral Implant. Res. 2011, 23, 938–942. [Google Scholar] [CrossRef]
- Mendes, R.M.; Silva, G.A.; Caliari, M.V.; Silva, E.E.; Ladeira, L.O.; Ferreira, A.J. Effects of single wall carbon nanotubes and its functionalization with sodium hyaluronate on bone repair. Life Sci. 2010, 87, 215–222. [Google Scholar] [CrossRef]
- Deed, R.; Rooney, P.; Kumar, P.; Norton, J.D.; Smith, J.; Freemont, A.J.; Kumar, S. Early-response gene signalling is induced by angiogenic oligosaccharides of hyaluronan in endothelial cells. Inhibition by non-angiogenic, high-molecular-weight hyaluronan. Int. J. Cancer 1997, 71, 251–256. [Google Scholar] [CrossRef]
- Chen, W.Y.J.; Abatangelo, G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999, 7, 79–89. [Google Scholar] [CrossRef]
- Jentsch, H.; Pomowski, R.; Kundt, G.; Göcke, R. Treatment of gingivitis with hyaluronan. J. Clin. Periodontol. 2003, 30, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Soancă, A.; Lupse, M.; Moldovan, M.; Pall, E.; Cenariu, M.C.; Roman, A.; Tudoran, O.; Surlin, P.; Șorițău, O. Applications of inflammation-derived gingival stem cells for testing the biocompatibility of dental restorative biomaterials. Ann. Anat.-Anat. Anz. 2018, 218, 28–39. [Google Scholar] [CrossRef]
- Pall, E.; Cenariu, M.; Kasaj, A.; Florea, A.; Soancă, A.; Roman, A.; Georgiu, C. New insights into the cellular makeup and progenitor potential of palatal connective tissues. Microsc. Res. Tech. 2017, 80, 1270–1282. [Google Scholar] [CrossRef] [PubMed]
- Doetschman, T.C.; Eistetter, H.; Katz, M.; Schmidt, W.; Kemler, R. The in vitro development of blastocyst-derived embryonic stem cell lines: Formation of visceral yolk sac, blood islands and myocardium. J. Embryol. Exp. Morphol. 1985, 87, 27–45. [Google Scholar]
- Castro-Malaspina, H.; Gay, R.E.; Resnick, G.; Kapoor, N.; Meyers, P.; Chiarieri, D.; McKenzie, S.; Broxmeyer, H.E.; Moore, M.A. Characterization of Human Bone Marrow Fibroblast Colony-Forming Cells (CFU-F) and Their Progeny. Blood 1980, 56, 289–301. [Google Scholar] [CrossRef] [Green Version]
- Crincoli, V.; Fatone, L.; Fanelli, M.; Rotolo, R.P.; Chialà, A.; Favia, G.; Lapadula, G. Orofacial Manifestations and Temporomandibular Disorders of Systemic Scleroderma: An Observational Study. Int. J. Mol. Sci. 2016, 17, 1189. [Google Scholar] [CrossRef] [Green Version]
- Cipriani, P.; Di Benedetto, P.; Liakouli, V.; Del Papa, B.; DI Padova, M.; Di Ianni, M.; Marrelli, A.; Alesse, E.; Giacomelli, R. Mesenchymal stem cells (MSCs) from scleroderma patients (SSc) preserve their immunomodulatory properties although senescent and normally induce T regulatory cells (Tregs) with a functional phenotype: Implications for cellular-based therapy. Clin. Exp. Immunol. 2013, 173, 195–206. [Google Scholar] [CrossRef]
- Cipriani, P.; Di Benedetto, P.; Ruscitti, P.; Campese, A.F.; Liakouli, V.; Carubbi, F.; Pantano, I.; Berardicurt, O.; Screpanti, I.; Giacomelli, R. Impaired Endothelium-Mesenchymal Stem Cells Cross-talk in Systemic Sclerosis: A Link Between Vascular and Fibrotic Features. Arthritis Res. Ther. 2014, 16, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roman, A.; Şoancă, A.; Florea, A.; Páll, E. In Vitro Characterization of Multipotent Mesenchymal Stromal Cells Isolated from Palatal Subepithelial Tissue Grafts. Microsc. Microanal. 2013, 19, 370–380. [Google Scholar] [CrossRef]
- Páll, E.; Florea, A.; Soriţău, O.; Cenariu, M.; Petruţiu, A.S.; Roman, A. Comparative Assessment of Oral Mesenchymal Stem Cells Isolated from Healthy and Diseased Tissues. Microsc. Microanal. 2015, 21, 1249–1263. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Marino, V.; Gronthos, S.; Bartold, P.M. Location of putative stem cells in human periodontal ligament. J. Periodontal Res. 2006, 41, 547–553. [Google Scholar] [CrossRef]
- Park, J.-C.; Kim, J.-M.; Jung, I.-H.; Kim, J.C.; Choi, S.-H.; Cho, K.S.; Kim, C.-S. Isolation and characterization of human periodontal ligament (PDL) stem cells (PDLSCs) from the inflamed PDL tissue: In vitro and in vivo evaluations. J. Clin. Periodontol. 2011, 38, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Yazid, F.B.; Gnanasegaran, N.; Kunasekaran, W.; Govindasamy, V.; Musa, S. Comparison of immunodulatory properties of dental pulp stem cells derived from healthy and inflamed teeth. Clin. Oral Investig. 2014, 18, 2103–2112. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.-N.; Xia, Y.; Yu, Y.; Wu, R.-X.; Gao, L.-N.; Chen, F.-M. Stem cells derived from “inflamed” and healthy periodontal ligament tissues and their sheet functionalities: A patient-matched comparison. J. Clin. Periodontol. 2015, 43, 72–84. [Google Scholar] [CrossRef]
- Morine, K.J.; Paruchuri, V.; Qiao, X.; Aronovitz, M.; Huggins, G.S.; Denofrio, D.; Kiernan, M.S.; Karas, R.H.; Kapur, N.K. Endoglin selectively modulates transient receptor potential channel expression in left and right heart failure. Cardiovasc. Pathol. 2016, 25, 478–482. [Google Scholar] [CrossRef] [Green Version]
- Rege, T.A.; Hagood, J.S. Thy-1 as a regulator of cell-cell and cell-matrix interactions in axon regeneration, apoptosis, adhesion, migration, cancer, and fibrosis. FASEB J. 2006, 20, 1045–1054. [Google Scholar] [CrossRef]
- de Carvalho, L.A.C.; Dos Santos, S.L.T.; Sacramento, L.V.; de Almeida Júnior, V.R.; de Aquino Xavier, F.C.; Dos Santos, J.N.; Leitão, Á.C.G.H. Mesenchymal stem cell markers in periodontal tissues and periapical lesions. Acta Histochem. 2020, 122, 151636. [Google Scholar] [CrossRef]
- Rozier, P.; Maria, A.; Goulabchand, R.; Jorgensen, C.; Guilpain, P.; Noël, D. Mesenchymal Stem Cells in Systemic Sclerosis: Allogenic or Autologous Approaches for Therapeutic Use? Front. Immunol. 2018, 9, 2938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurosawa, H. Methods for inducing embryoid body formation: In vitro differentiation system of embryonic stem cells. J. Biosci. Bioeng. 2007, 103, 389–398. [Google Scholar] [CrossRef]
- Cipriani, P.; Guiducci, S.; Miniati, I.; Cinelli, M.; Urbani, S.; Marrelli, A.; Dolo, V.; Pavan, A.; Saccardi, R.; Tyndall, A.; et al. Impairment of endothelial cell differentiation from bone marrow–derived mesenchymal stem cells: New insight into the pathogenesis of systemic sclerosis. Arthritis Rheum. 2007, 56, 1994–2004. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.L.; Johansson, C.B.; Wilbertz, J.; Veress, B.; Nilsson, E.; Karlström, H.; Lendahl, U.; Frisén, J. Generalized Potential of Adult Neural Stem Cells. Science 2000, 288, 1660–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, B.; Weiss, S. Generation of neurons and astrocytes from isolated cells of the adult mammalian central nervous system. Science 1992, 255, 1707–1710. [Google Scholar] [CrossRef] [Green Version]
- Rietze, R.L.; Valcanis, H.; Brooker, G.F.; Thomas, T.; Voss, A.K.; Bartlett, P.F. Purification of a pluripotent neural stem cell from the adult mouse brain. Nature 2001, 412, 736–739. [Google Scholar] [CrossRef]
- Bocelli-Tyndall, C.; Bracci, L.; Spagnoli, G.; Braccini, A.; Bouchenaki, M.; Ceredig, R.; Pistoia, V.; Martin, I.; Tyndall, A. Bone marrow mesenchymal stromal cells (BM-MSCs) from healthy donors and auto-immune disease patients reduce the proliferation of autologous- and allogeneic-stimulated lymphocytes in vitro. Rheumatology 2006, 46, 403–408. [Google Scholar] [CrossRef] [Green Version]
- Alongi, D.J.; Yamaza, T.; Song, Y.; Fouad, A.F.; Romberg, E.E.; Shi, S.; Tuan, R.S.; Huang, G.T.-J. Stem/progenitor cells from inflamed human dental pulp retain tissue regeneration potential. Regen. Med. 2010, 5, 617–631. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.; Al Shahrani, M.; Al-Habib, M.; Tanaka, T.; Huang, G.T.-J. Cells Isolated from Inflamed Periapical Tissue Express Mesenchymal Stem Cell Markers and Are Highly Osteogenic. J. Endod. 2011, 37, 1217–1224. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.; Zhang, X.; Li, X. Exosomes Derived from Mesenchymal Stem Cells. Int. J. Mol. Sci. 2014, 15, 4142–4157. [Google Scholar] [CrossRef] [Green Version]
- Vanneaux, V.; Farge-Bancel, D.; Lecourt, S.; Baraut, J.; Cras, A.; Jean-Louis, F.; Brun, C.; Verrecchia, F.; Larghero, J.; Michel, L. Expression of transforming growth factor β receptor II in mesenchymal stem cells from systemic sclerosis patients. BMJ Open 2013, 3, e001890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guiducci, S.; Manetti, M.; Romano, E.; Mazzanti, B.; Ceccarelli, C.; Pozzo, S.D.; Milia, A.F.; Bellando-Randone, S.; Fiori, G.; Conforti, M.L.; et al. Bone marrow-derived mesenchymal stem cells from early diffuse systemic sclerosis exhibit a paracrine machinery and stimulate angiogenesis in vitro. Ann. Rheum. Dis. 2011, 70, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- Maria, A.T.J.; Maumus, M.; Le Quellec, A.; Jorgensen, C.; Noël, D.; Guilpain, P. Adipose-Derived Mesenchymal Stem Cells in Autoimmune Disorders: State of the Art and Perspectives for Systemic Sclerosis. Clin. Rev. Allergy Immunol. 2016, 52, 234–259. [Google Scholar] [CrossRef]
- Rosa, I.; Romano, E.; Fioretto, B.S.; Matucci-Cerinic, M.; Manetti, M. Adipose-derived stem cells: Pathophysiologic implications vs therapeutic potential in systemic sclerosis. World J. Stem Cells 2021, 13, 30–48. [Google Scholar] [CrossRef] [PubMed]
- Manetti, M.; Romano, E.; Rosa, I.; Fioretto, B.S.; Praino, E.; Guiducci, S.; Iannone, F.; Ibba-Manneschi, L.; Matucci-Cerinic, M. Systemic Sclerosis Serum Steers the Differentiation of Adipose-Derived Stem Cells Toward Profibrotic Myofibroblasts: Pathophysiologic Implications. J. Clin. Med. 2019, 8, 1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marangoni, R.G.; Varga, J.; Tourtellotte, W.G. Animal models of scleroderma: Recent progress. Curr. Opin. Rheumatol. 2016, 28, 561–570. [Google Scholar] [CrossRef]
- Abedi, M.; Alavi-Moghadam, S.; Payab, M.; Goodarzi, P.; Mohamadi-Jahani, F.; Sayahpour, F.A.; Larijani, B.; Arjmand, B. Mesenchymal stem cell as a novel approach to systemic sclerosis; current status and future perspectives. Cell Regen. 2020, 9, 20. [Google Scholar]
- Pittenger, M.F.; Discher, D.E.; Péault, B.M.; Phinney, D.G.; Hare, J.M.; Caplan, A.I. Mesenchymal stem cell perspective: Cell biology to clinical progress. npj Regen. Med. 2019, 4, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.; Reese, C.; Carmen-Lopez, G.; Perry, B.; Bonner, M.; Zemskova, M.; Wilson, C.L.; Helke, K.L.; Silver, R.M.; Hoffman, S.; et al. Deficient Adipogenesis of Scleroderma Patient and Healthy African American Monocytes. Front. Pharmacol. 2017, 8, 174. [Google Scholar] [CrossRef] [Green Version]
- Lopes, B.; Sousa, P.; Alvites, R.; Branquinho, M.; Sousa, A.; Mendonça, C.; Atayde, L.; Maurício, A. The Application of Mesenchymal Stem Cells on Wound Repair and Regeneration. Appl. Sci. 2021, 11, 3000. [Google Scholar] [CrossRef]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal Regeneration—Intrabony Defects: A Systematic Review From the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S77–S104. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Chappuis, V.; Stähli, A.; Buser, D.; Sculean, A. Role of hyaluronan in regulating self-renewal and osteogenic differentiation of mesenchymal stromal cells and pre-osteoblasts. Clin. Oral Investig. 2020, 24, 3923–3937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamalik, N.; Kilinc, K.; Caglayan, F.; Eratalay, K.; Caglayan, G. Molecular size distribution analysis of human gingival proteoglycans and glycosaminoglycans in specific periodontal diseases. J. Clin. Periodontol. 1998, 25, 145–152. [Google Scholar] [CrossRef]
- Aya, K.L.; Stern, R. Hyaluronan in wound healing: Rediscovering a major player. Wound Repair Regen. 2014, 22, 579–593. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, L.; Hällgren, R.; Venge, P. Regulation of granulocyte function by hyaluronic acid. In vitro and in vivo effects on phagocytosis, locomotion, and metabolism. J. Clin. Investig. 1980, 66, 298–305. [Google Scholar] [CrossRef] [Green Version]
- Powell, J.D.; Horton, M.R. Threat Matrix: Low-Molecular-Weight Hyaluronan (HA) as a Danger Signal. Immunol. Res. 2005, 31, 207–218. [Google Scholar] [CrossRef]
- Johannsen, A.; Tellefsen, M.; Wikesjö, U.; Johannsen, G. Local Delivery of Hyaluronan as an Adjunct to Scaling and Root Planing in the Treatment of Chronic Periodontitis. J. Periodontol. 2009, 80, 1493–1497. [Google Scholar] [CrossRef]
- El-Sayed, K.M.F.; Dahaba, M.A.; Aboul-Ela, S.; Darhous, M.S. Local application of hyaluronan gel in conjunction with periodontal surgery: A randomized controlled trial. Clin. Oral Investig. 2011, 16, 1229–1236. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Antigen (%) | CD73 | CD90 | CD105 | CD44 | CD79a | CD34 | CD45 | HLA-DR | CD14 |
|---|---|---|---|---|---|---|---|---|---|
| Cell Line | |||||||||
| hMSCs | 100 | 99.7 | 99.8 | 97.5 | 0.2 | 0 | 0.1 | 0.1 | 0.1 |
| SScgMSCss | 95.7 | 90.9 | 89.2 | 97.3 | 0 | 0 | 0 | 0 | 0 |
| SScgtMSCs | 86.4 | 95 | 85 | 85.2 | 1.3 | 0.3 | 0.5 | 2.1 | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanomir, A.; Mihu, C.M.; Rednic, S.; Pamfil, C.; Roman, A.; Soancă, A.; Micu, I.C.; Bulboacă, A.E.; Stratul, Ș.I.; Popa-Wagner, A.; et al. Oral Mesenchymal Stromal Cells in Systemic Sclerosis: Characterization and Response to a Hyaluronic-Acid-Based Biomaterial. Appl. Sci. 2021, 11, 8101. https://doi.org/10.3390/app11178101
Stanomir A, Mihu CM, Rednic S, Pamfil C, Roman A, Soancă A, Micu IC, Bulboacă AE, Stratul ȘI, Popa-Wagner A, et al. Oral Mesenchymal Stromal Cells in Systemic Sclerosis: Characterization and Response to a Hyaluronic-Acid-Based Biomaterial. Applied Sciences. 2021; 11(17):8101. https://doi.org/10.3390/app11178101
Chicago/Turabian StyleStanomir, Alina, Carmen Mihaela Mihu, Simona Rednic, Cristina Pamfil, Alexandra Roman, Andrada Soancă, Iulia Cristina Micu, Adriana Elena Bulboacă, Ștefan Ioan Stratul, Aurel Popa-Wagner, and et al. 2021. "Oral Mesenchymal Stromal Cells in Systemic Sclerosis: Characterization and Response to a Hyaluronic-Acid-Based Biomaterial" Applied Sciences 11, no. 17: 8101. https://doi.org/10.3390/app11178101
APA StyleStanomir, A., Mihu, C. M., Rednic, S., Pamfil, C., Roman, A., Soancă, A., Micu, I. C., Bulboacă, A. E., Stratul, Ș. I., Popa-Wagner, A., & Pall, E. (2021). Oral Mesenchymal Stromal Cells in Systemic Sclerosis: Characterization and Response to a Hyaluronic-Acid-Based Biomaterial. Applied Sciences, 11(17), 8101. https://doi.org/10.3390/app11178101