
Is Panoramic Radiography Really a Key Examination before Chemo-Radiotherapy Treatment for Oropharyngeal Cancer?

 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
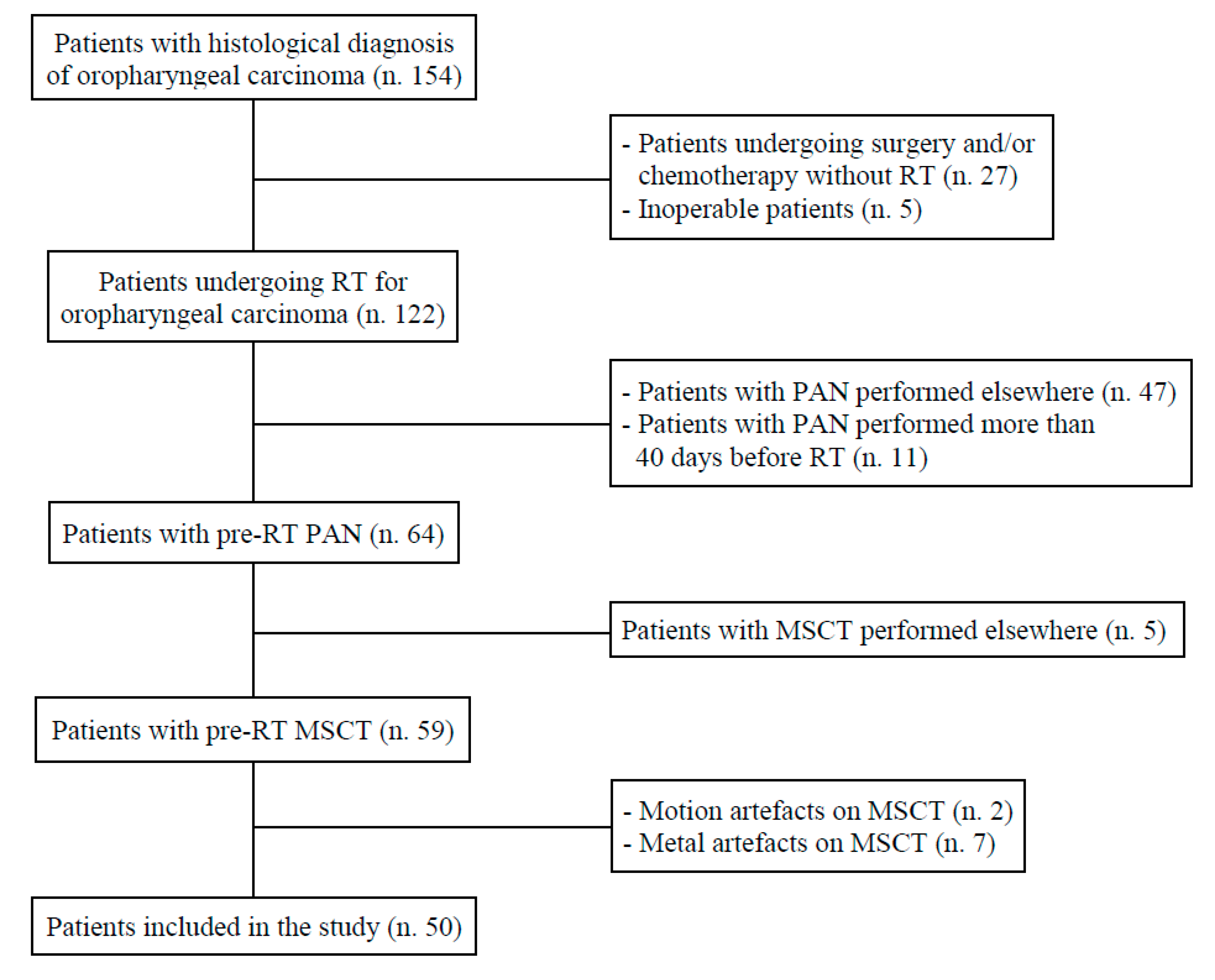
2.1. Patients and Devices
- Underage patient (<18 years);
- No histological diagnosis of OPC;
- No RT;
- No pre-RT PAN examination;
- PAN has not been performed during the 40 days prior to MSCT examination;
- No pre-RT MSCT examination;
- Poor MSCT image quality due to motion and/or metal artefacts.
- Adult patient (≥18 years);
- Histological diagnosis of OPC;
- RT for OPC;
- Pre-RT MSCT examination;
- PAN carried out during the earlier 40 days to MSCT examination;
- Absence of motion and/or metal artefacts.
2.2. Assessment of Infectious Foci and Outline of the Study
- Deep caries, defined as a loss of dental crown extending beyond half the thickness of the dentin with possible involvement of the pulp chamber [14];
- Root remnants, where there is loss of at least 75% of the crown [15];
- Stage III periodontal disease, determined by loss of bone extending to the middle third of the root or beyond [16];
2.3. Readers and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Who.int. Global Health Observatory Data Repository. Incidence (World) by Cancer Site. 2020. Available online: https://gco.iarc.fr (accessed on 28 July 2021).
- Timbang, M.R.; Sim, M.W.; Bewley, A.F.; Farwell, D.G.; Mantravadi, A.; Moore, M.G. HPV-related oropharyngeal cancer: A review on burden of the disease and opportunities for prevention and early detection. Hum. Vaccin. Immunother. 2019, 15, 1920–1928. [Google Scholar] [CrossRef] [PubMed]
- Jamal, Z.; Anjum, F. Oropharyngeal Squamous Cell Carcinoma. StatPearls 2021. Available online: https://www.statpearls.com (accessed on 18 August 2021).
- Huber, M.A.; Tantiwongkosi, B. Oral and oropharyngeal cancer. Med. Clin. N. Am. 2014, 98, 1299–1321. [Google Scholar] [CrossRef]
- Hamilton, D.; Khan, M.K.; O’hara, J.; Paleri, V. The changing landscape of oropharyngeal cancer management. J. Laryngol. Otol. 2017, 131, 3–7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- You, E.L.; Henry, M.; Zeitouni, A.G. Human papillomavirus-associated oropharyngeal cancer: Review of current evidence and management. Curr. Oncol. 2019, 26, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Evans, M.; Beasley, M.; Chatterjee, S.; Dilkes, M.; Homer, J.; O’hara, J.; Robinson, M.; Shaw, R.; Sloan, P. Oropharyngeal cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130 (Suppl. S2), S90–S96. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.; Dijkstra, P.U.; Vissink, A.; Spijkervet, F.K. Evidence supporting pre-radiation elimination of oral foci of infection in head and neck cancer patients to prevent oral sequelae: A systematic review. Oral Oncol. 2015, 51, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Nardi, C.; Calistri, L.; Grazzini, G.; Desideri, I.; Lorini, C.; Occhipinti, M.; Mungai, F.; Colagrande, S. Is Panoramic Radiography an Accurate Imaging Technique for the Detection of Endodontically Treated Asymptomatic Apical Periodontitis? J. Endod. 2018, 44, 1500–1508. [Google Scholar] [CrossRef]
- Mostafapoor, M.; Hemmatian, S. Evaluation of the accuracy values of cone-beam CT regarding apical periodontitis: A systematic review and meta-analysis. Oral Radiol. 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Lin, A. Radiation Therapy for Oral Cavity and Oropharyngeal Cancers. Dent. Clin. N. Am. 2018, 62, 99–109. [Google Scholar] [CrossRef]
- Sulaiman, F.; Huryn, J.M.; Zlotolow, I.M. Dental extractions in the irradiated head and neck patient: A retrospective analysis of MemorialSloan—Kettering Cancer Center protocols, criteria, and end results. J. Oral Maxillofac. Surg. 2003, 61, 1123–1131. [Google Scholar] [CrossRef]
- Beech, N.; Robinson, S.; Porceddu, S.; Batstone, M. Dental management of patients irradiated for head and neck cancer. Aust. Dent. J. 2014, 59, 20–28. [Google Scholar] [CrossRef]
- Anusavice, K.J. Present and future approaches for the control of caries. J. Dent. Educ. 2005, 69, 538–554. [Google Scholar] [CrossRef] [PubMed]
- Ada.org. Glossary of Dental Clinical and Administrative Terms by American Dental Association. Available online: https://www.ada.org/en/publications/cdt/glossary-of-dental-clinical-and-administrative-terms (accessed on 28 July 2021).
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S1–S8. [Google Scholar] [CrossRef]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef] [PubMed]
- Uraba, S.; Ebihara, A.; Komatsu, K.; Ohbayashi, N.; Okiji, T. Ability of cone-beam computed tomography to detect periapical lesions that were not detected by periapical radiography: A retrospective assessment according to tooth group. J. Endod. 2016, 42, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Nardi, C.; Calistri, L.; Pietragalla, M.; Vignoli, C.; Lorini, C.; Berti, V.; Mungai, F.; Colagrande, S. Electronic processing of digital panoramic radiography for the detection of apical periodontitis. Radiol. Med. 2020, 125, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Bender, I.B.; Seltzer, S. Roentgenographic and direct observation of experimental lesions in bone: I. 1961. J. Endod. 2003, 29, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Cotton, T.P.; Geisler, T.M.; Holden, D.T.; Schwartz, S.A.; Schindler, W.G. Endodontic applications of cone-beam volumetric tomography. J. Endod. 2007, 33, 1121–1132. [Google Scholar] [CrossRef]
- Liang, X.; Jacobs, R.; Hassan, B.; Li, L.; Pauwels, R.; Corpas, L.; Souza, P.C.; Martens, W.; Shahbazian, M.; Alonso, A.; et al. A comparative evaluation of cone beam computed tomography, (CBCT); multi-slice CT (MSCT) Part I. On subjective image quality. Eur. J. Radiol. 2010, 75, 265–269. [Google Scholar] [CrossRef]
- Estrela, C.; Bueno, M.R.; Leles, C.R.; Azevedo, B.; Azevedo, J.R. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J. Endod. 2008, 34, 273–279. [Google Scholar] [CrossRef]
- Nardi, C.; Calistri, L.; Pradella, S.; Desideri, I.; Lorini, C.; Colagrande, S. Accuracy of Orthopantomography for Apical Periodontitis without Endodontic Treatment. J. Endod. 2017, 43, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Santos, J.V.; Ridao-Sacie, C.; Bullón, P.; Fernández-Palacín, A.; Segura-Egea, J.J. Assessment of periapical status: A comparative study using film-based periapical radiographs and digital panoramic images. Med. Oral Patol. Oral Cir. Bucal. 2010, 15, e952–e956. [Google Scholar] [CrossRef] [PubMed]
- Lechuga, L.; Weidlich, G.A. Cone Beam CT vs. Fan Beam CT: A Comparison of Image Quality and Dose Delivered Between Two Differing CT Imaging Modalities. Cureus 2016, 8, e778. [Google Scholar] [CrossRef] [PubMed]
- Spin-Neto, R.; Costa, C.; Salgado, D.M.; Zambrana, N.R.; Gotfredsen, E.; Wenzel, A. Patient movement characteristics and the impact on CBCT image quality and interpretability. Dentomaxillofac. Radiol. 2018, 47, 20170216. [Google Scholar] [CrossRef] [PubMed]
- Nardi, C.; Molteni, R.; Lorini, C.; Taliani, G.G.; Matteuzzi, B.; Mazzoni, E.; Colagrande, S. Motion artefacts in cone beam CT: An in vitro study about the effects on the images. Br. J. Radiol. 2016, 89, 20150687. [Google Scholar] [CrossRef]
- Nardi, C.; Talamonti, C.; Pallotta, S.; Saletti, P.; Calistri, L.; Cordopatri, C.; Colagrande, S. Head and neck effective dose and quantitative assessment of image quality: A study to compare cone beam CT and multislice spiral CT. Dentomaxillofac. Radiol. 2017, 46, 20170030. [Google Scholar] [CrossRef]
- Pistorius, A.; Patrosio, C.; Willershausen, B.; Mildenberger, P.; Rippen, G. Periodontal probing in comparison to diagnosis by CT-scan. Int. Dent. J. 2001, 51, 339–347. [Google Scholar] [CrossRef]
- Mardini, S.; Gohel, A. Imaging of Odontogenic Infections. Radiol. Clin. N. Am. 2018, 56, 31–44. [Google Scholar] [CrossRef]
- Jasmer, K.J.; Gilman, K.E.; Muñoz Forti, K.; Weisman, G.A.; Limesand, K.H. Radiation-Induced Salivary Gland Dysfunction: Mechanisms, Therapeutics and Future Directions. J. Clin. Med. 2020, 9, 4095. [Google Scholar] [CrossRef]
- Brook, I. Late side effects of radiation treatment for head and neck cancer. Radiat. Oncol. J. 2020, 38, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Hancock, P.J.; Epstein, J.B.; Sadler, G.R. Oral and dental management related to radiation therapy for head and neck cancer. J. Can. Dent. Assoc. 2003, 69, 585–590. [Google Scholar] [PubMed]
- Irie, M.S.; Mendes, E.M.; Borges, J.S.; Osuna, L.G.; Rabelo, G.D.; Soares, P.B. Periodontal therapy for patients before and after radiotherapy: A review of the literature and topics of interest for clinicians. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e524–e530. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.W.K.; Jacobs, R.; Bornstein, M.M. Novel low-dose protocols using cone beam computed tomography in dental medicine: A review focusing on indications, limitations, and future possibilities. Clin. Oral Investig. 2019, 23, 2573–2581. [Google Scholar] [CrossRef]
- Geibel, M.A.; Schreiber, E.S.; Bracher, A.K.; Hell, E.; Ulrici, J.; Sailer, L.K.; Ozpeynirci, Y.; Rasche, V. Assessment of apical periodontitis by MRI: A feasibility study. Rofo 2015, 187, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Juerchott, A.; Sohani, M.; Schwindling, F.S.; Jende, J.M.; Kurz, F.T.; Rammelsberg, P.; Heiland, S.; Bendszus, M.; Hilgenfeld, T. Comparison of non-contrast-enhanced dental magnetic resonance imaging and cone-beam computed tomography in assessing the horizontal and vertical components of furcation defects in maxillary molars: An in vivo feasibility study. J. Clin. Periodontol. 2020, 47, 1485–1495. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PAN | Multi Slice CT | ||
|---|---|---|---|
| Diseased | Healthy | Total | |
| Deep caries | |||
| Positive | 65 (100%) | 0 | 65 |
| Negative | 0 | 65 (100%) | 65 |
| Total | 65 | 65 | 130 |
| Root remnants | |||
| Positive | 37 (100%) | 0 | 37 |
| Negative | 0 | 37 (100%) | 37 |
| Total | 37 | 37 | 74 |
| Stage III periodontal disease | |||
| Positive | 143 (100%) | 0 | 143 |
| Negative | 0 | 143 (100%) | 143 |
| Total | 143 | 143 | 286 |
| Apical periodontitis | |||
| Positive | 36 (46.8%) | 2 (2.6%) | 38 |
| Negative | 41 (53.2%) | 75 (97.4%) | 116 |
| Total | 77 | 77 | 154 |
| Parameter | SEN | SPE | PPV | NPV | ACC | K |
|---|---|---|---|---|---|---|
| Deep caries | 100% | 100% | 100% | 100% | 100% | 0.96 |
| Root remnants | 100% | 100% | 100% | 100% | 100% | 0.94 |
| Stage III periodontal disease | 100% | 100% | 100% | 100% | 100% | 0.93 |
| Apical periodontitis | 46.8% | 97.4% | 94.7% | 64.7% | 72.1% | 0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bosoni, C.; Pietragalla, M.; Maraghelli, D.; Rastrelli, V.; Locatello, L.G.; Desideri, I.; Giuntini, V.; Franchi, L.; Nardi, C. Is Panoramic Radiography Really a Key Examination before Chemo-Radiotherapy Treatment for Oropharyngeal Cancer? Appl. Sci. 2021, 11, 7965. https://doi.org/10.3390/app11177965
Bosoni C, Pietragalla M, Maraghelli D, Rastrelli V, Locatello LG, Desideri I, Giuntini V, Franchi L, Nardi C. Is Panoramic Radiography Really a Key Examination before Chemo-Radiotherapy Treatment for Oropharyngeal Cancer? Applied Sciences. 2021; 11(17):7965. https://doi.org/10.3390/app11177965
Chicago/Turabian StyleBosoni, Carlo, Michele Pietragalla, Davide Maraghelli, Vieri Rastrelli, Luca Giovanni Locatello, Isacco Desideri, Veronica Giuntini, Lorenzo Franchi, and Cosimo Nardi. 2021. "Is Panoramic Radiography Really a Key Examination before Chemo-Radiotherapy Treatment for Oropharyngeal Cancer?" Applied Sciences 11, no. 17: 7965. https://doi.org/10.3390/app11177965
APA StyleBosoni, C., Pietragalla, M., Maraghelli, D., Rastrelli, V., Locatello, L. G., Desideri, I., Giuntini, V., Franchi, L., & Nardi, C. (2021). Is Panoramic Radiography Really a Key Examination before Chemo-Radiotherapy Treatment for Oropharyngeal Cancer? Applied Sciences, 11(17), 7965. https://doi.org/10.3390/app11177965